
Abstract
Background:
Screening patients with patient-reported outcome measures allows identification of palliative care concerns. The Integrated Palliative Care Outcome Scale (IPOS) was developed in the United Kingdom for this purpose. Tools developed in another setting might not be readily usable locally. We previously evaluated the validity and reliability of the IPOS in our cardiology setting. However, it remains uncertain what factors would influence the subsequent implementation of IPOS for routine screening of patients with advanced heart failure in future practice.
Objectives:
This study aimed to identify the factors that could affect the IPOS implementation for patients with advanced heart failure.
Design:
This was a qualitative study conducted at the National Heart Centre Singapore.
Methods:
Patients with advanced heart failure who participated in our previous IPOS validation study were purposively recruited for semi-structured interviews. Healthcare workers caring for these patients and involved in the testing of the IPOS tool were also invited for interviews. The interviews were analyzed thematically and mapped to the Consolidated Framework for Implementation Research (CFIR).
Results:
Our analysis identified six potential facilitators and six potential barriers to implementation across five major domains of the CFIR (intervention characteristics, inner setting, outer setting, individual characteristics, and process). Facilitators include: (i) perception of utility, (ii) perception of minimal complexity, (iii) perception of relatability, (iv) conducive culture, (v) dedicated resources, and (vi) advocates for implementation. Barriers include: (i) need for adaptation, (ii) mindsets/role strains, (iii) resource constraints, (iv) cultural concerns, (v) individual needs, and (vi) change process.
Conclusion:
Institutions could focus on cultivating appropriate perceptions and conducive cultures, providing dedicated resources for implementation and introducing facilitators to advocate for implementation. Adaptation of IPOS to suit workflows and individual needs, consideration of change processes, and systemic changes to alleviate cultural, resource, and staff role strains would improve IPOS uptake during actual implementation in clinical services.
Trial registration:
Not applicable.
Introduction
Patients with heart failure have significant physical and psycho-emotional concerns.1,2 However, these concerns are often under-detected and reported.3–5 Palliative care services aim to improve the quality-of-life of patients with serious illnesses. Screening of patients using patient and staff reported tools may prove to be an effective way of identifying those who need palliative care. These patients can then be promptly referred to palliative care by their primary clinicians, allowing them to receive palliative care support, in a timely manner.6–11
The Integrated Palliative Care Outcome Scale (IPOS) is a widely used patient-and-staff-reported outcome measure that could be used to screen patients with serious illnesses.12,13 Developed in the United Kingdom, this brief measure is shown to be clinically meaningful with good psychometric properties in the palliative care setting. 14 However, screening tools developed in another country may not be entirely applicable in a new setting due to differing socio-economic-cultural contexts and disease-specific impacts. 15 It is also unknown whether a tool that was developed in a specialist palliative care setting would be readily usable in a setting where most of the care are provided by cardiac specialists who are non-palliative care specialists (generalists) 16 and specialist palliative care services are only available on a consult basis.
Therefore, our team sought to evaluate the validity and reliability of the IPOS locally17,18 as well as seek factors that would influence subsequent IPOS implementation for routine screening of patients with advanced heart failure in Singapore, in the clinical, non-research setting. In a prior study, 18 we described our results that the IPOS was valid and reliable for screening patients with advanced heart failure in Singapore. In this article, we will describe the factors that could affect implementation of the IPOS for screening for needs of patients with advanced heart failure, who are cared for in a non-palliative care setting. This was done through seeking the view of patients and their healthcare staff who had experience with use of the IPOS screening tool, during the prior research and validation process.
Methods
Study design and setting
This qualitative study is part of a two-phase prospective study that was carried out in the inpatient and outpatient setting of the National Heart Centre Singapore (NHCS). NHCS is a large volume national referral center for heart failure (HF) patients, staffed only by cardiac specialists. 19 Patients with heart failure who have palliative care needs are referred to consult palliative care services in the Singapore General Hospital 20 and the National Cancer Centre Singapore. 21
In the first phase of the project, we validated the IPOS scale (full details are described in the prior published paper). 18 English-speaking patients with heart failure, aged 21 years and above, and who were aware of their diagnosis participated in the study. Patients were given a physical hard copy of the patient IPOS to fill in. For staff participants, nursing and physician staff from the palliative care and heart failure teams who directly cared for the recruited patient participants were asked to fill in a physical hard copy of the staff IPOS for his/her patient. This was done so that each patient’s IPOS would be matched by a staff IPOS. Staff participants were not part of the study team.
In the current study, we purposively invited patient participants who had already completed the IPOS in the first research validation phase for semi-structured interviews. This ensures that they had prior exposure to the IPOS screening tool. We ensured diversity in terms of age, gender, years living with heart failure (for patients) and setting that care was received (inpatient versus outpatient). Patient recruitment was carried out iteratively and stopped when data saturation was achieved. We defined ‘data saturation’ as the point in data collection when no additional insights were identified from our data and data began to repeat, such that further data collection was redundant. Data saturation indicates that an adequate sample size has been reached. 22 We also asked all recruited staff who had previously used the IPOS for the interviews.
A female research coordinator (JT), trained in qualitative research, with no dependent relationship and pre-existing bias with the participants was responsible for recruiting participants. Semi-structured interviews focused on understanding their views toward their healthcare and the implementation and use of IPOS in Singapore. The semi-structured interview guide was developed based on existing literature23–25 (Supplemental Appendix 1).
Conceptual framework
Our study was guided by the Consolidated Framework for Implementation Research (CFIR) 25 – a framework commonly used for assessing context and the potential barriers and facilitators to implementation of an intervention within that context. The CFIR contains five major domains that guide program evaluation and implementation. These are: intervention characteristics, outer setting, inner setting, individual characteristics, and process.
Data collection and analysis
Interviews were conducted in a private setting in the clinic, audio-recorded, and transcribed verbatim with field notes taken when needed. The interviews lasted for maximum 1 h. Transcripts were checked for accuracy before coding. Coding was performed independently by two of the authors (SN and JT). Transcripts were thematically analyzed based on Braun and Clark. 26 The coders familiarized with the data and generate initial codes independently before collecting codes into potential categories and subthemes. The categories and subthemes were constantly reviewed and reclassified. We subsequently mapped the code categories and subthemes to the relevant domains of the CFIR. 25 We resolved discrepancies in coding and theme generation through consecutive rounds of discussion between the two coders. Data were managed with Microsoft Excel and an audit trail was kept. Data collection, analysis, and theme generation were iterative processes. We adhered to the consolidated criteria for reporting qualitative research (COREQ) criteria for qualitative research. 27
Results
Participant characteristics
We conducted interviews with 10 patient participants. The average age of patients was 55.8 years, with an equal number of males and females. Most patients (80%) were Chinese. More than half (60%) had secondary school education and above. Patients had an average length of illness of 5.1 years. Majority (90%) were New York Heart Association functional status 1 and 2. Patients were equally distributed between inpatient and outpatient settings.
Out of 12 healthcare staff participants who participated in the validation phase of the study, 9 healthcare staff (75%) participated in the semi-structured interviews phase. The rest could not participate as they had left the institution. The mean age of staff participants was 32.5 years. There were more female staff (77.8%). Four nurses (44.4%) participated, and the rest (55.5%) were physicians. On average, they had 6.2 years of experience with heart failure patients. More staff (77.8%) had a primary specialty of heart failure compared to palliative care (Table 1).
Participant characteristics.

Mean and standard deviation (SD) for continuous variables, frequency (N) and percent for categorical variables.
IPOS, Integrated Palliative Care Outcome Scale.
Themes
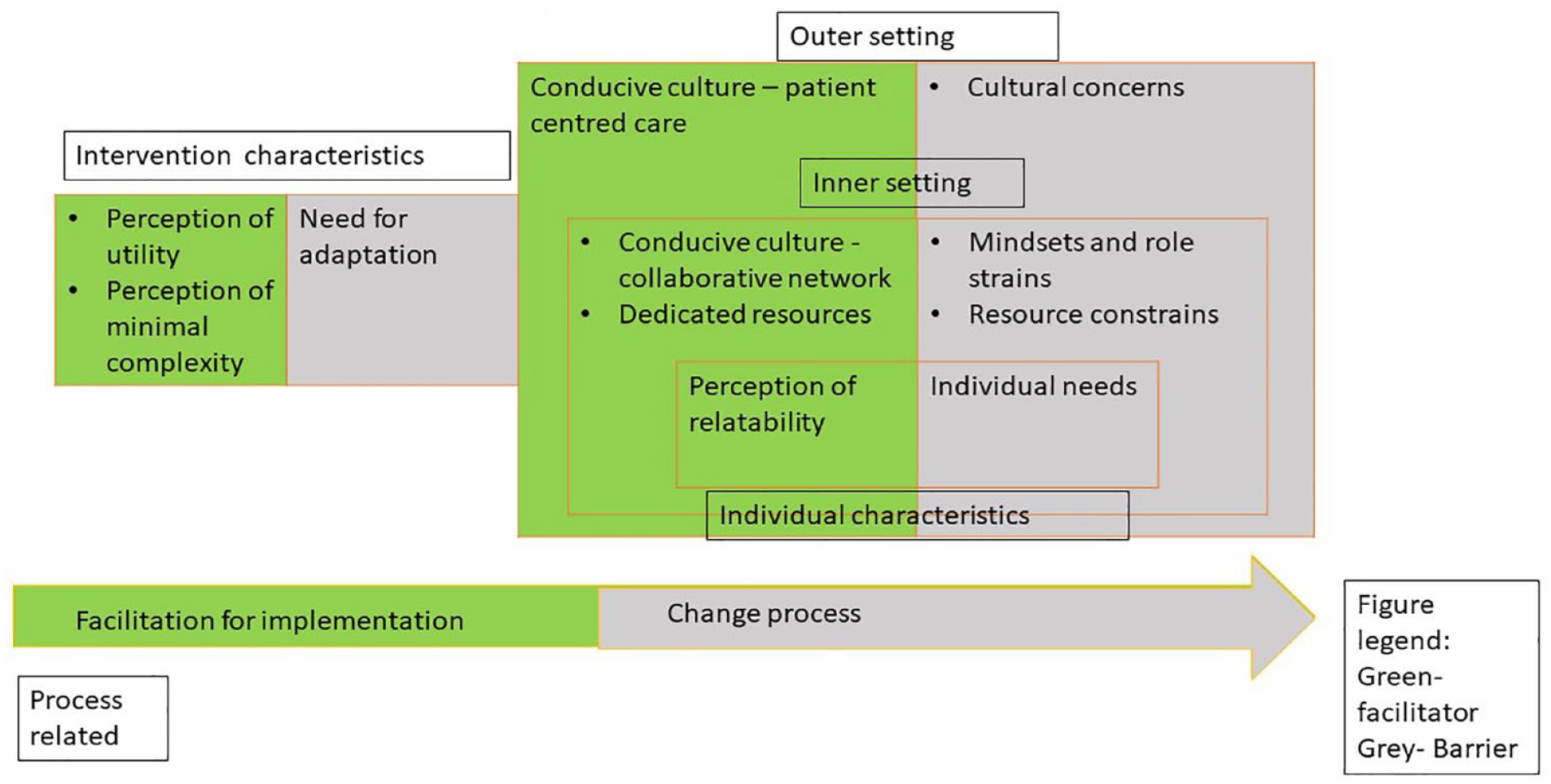
We present two major themes. Theme 1 – Facilitators to implementation – is presented inTable 2 while Theme 2 – Barriers to implementation – is presented in Table 3. Table 4 summarizes how our facilitators and barriers relate to the domains in the Consolidated Framework for Implementation Research (CFIR) and this is also visually presented in Figure 1. A succinct version of quotes from patient (PT) and healthcare worker (HCW) is presented in the text. Views of patients versus staff, as well as views of palliative care staff versus heart failure staff were compared where appropriate.
Theme 1 – Facilitators to implementation of the Integrated Palliative Care Outcome Scale (IPOS).

Theme 2 – Barriers to implementation of the Integrated Palliative Care Outcome Scale (IPOS).

PCOC is an outcome assessment scale that is filled in by palliative care staff, during their reviews of palliative care patients.
Relationship of CFIR domains to factors – ‘facilitators’ and ‘barriers’ that potentially influence IPOS implementation.

CFIR, Consolidated Framework for Implementation Research; IPOS, Integrated Palliative Care Outcome Scale.
Relationship of barriers and facilitators to domains on the Consolidated Framework for Implementation Research.
Theme 1: Facilitators for implementation
Subtheme 1a and 1b: Perceptions of utility and minimal complexity (intervention characteristics)
First, the utility of IPOS was commonly recognized. Both patients and staff brought up myriad examples of how IPOS could be used in the local setting. For example, staff believed that the IPOS could be usefully adopted as a guide in cardiology setting for symptom assessment (‘it is kind of a little guide or consolidated guide to assessing the patient’s symptoms’ – HCW11) and holistic evaluation (‘make sure that our patients are both healthy in body and healthy in mind’ – PT25). They also saw IPOS as facilitating communication (‘IPOS can help us to build better rapport with the patient?’ – HCW07) and early detection of patient’s concerns (‘we may not pick it up during the ward rounds’ – HCW 10); supporting prioritization of problems and triggering follow actions (‘start with a survey (IPOS) and then I think an interview’ – PT25). IPOS was also considered a useful tool for progress monitoring (‘so I can track my own progress also’ – PT26).
In general, healthcare staff and patients did not find it difficult to understand the phrasing of the IPOS items – (‘It’s not confusing’ – HCW05); (‘Easy to understand, instructions also can’ – PT32). The IPOS was also deemed not time-consuming to complete (‘It doesn’t really occupy a lot of time to do this survey’ – HCW07).
Subtheme 1c: Conducive culture (outer setting)
In terms of institutional culture and values, both patients and healthcare staff valued the IPOS and felt that it would serve as a means to achieve patient-centered care (‘I think it will help to assess whether or not we are trying to do what the patient wants actually. . .’ – HCW01). Patient-centered care was recognized as the provision of care that begins by first understanding and subsequently addressing the unique needs of patients and in that respect, the use of IPOS as a patient-reported survey would be very helpful (‘understand what they need. And then have something suited for them’ – PT25). One staff participant further opined that patient-centered care ought to be a core approach to healthcare (‘For patient-centered care, it should be how we approach every patient, regardless of our discipline’ – HCW12). Patients also felt that participating in patient-reported surveys would allow their views to be heard, and their voice to be a catalyst for change (‘Because to me, I want to participate, hope to see changes’ – PT26). This participant also felt that the IPOS was a useful tool, as doctors should have a means to screen for and act on patients’ concerns, even though some of the problems being screened for on the IPOS might not be in the physician’s direct specialty (‘Show some concern. I know you’re not specialised in this, but you can always refer you know’ – PT 26, 50s, Chinese, Female).
Another aspect related to culture that would favorably impact the implementation of IPOS was that of the culture between different clinical teams. One heart failure care staff described a pre-existing strong collaborative culture between the palliative care team and heart failure team to be an advantage (‘it’s always nice to collaborate with the palliative team.’ – HCW09).
Subtheme 1d: Dedicated resources (inner setting)
In terms of facilitation for administration, having dedicated resources such as coordinators to administer the IPOS was seen as important to aid IPOS implementation (‘I think then would be the coordinators to administer this’ – HCW09).
Subtheme 1e: Perception of relatability (individual characteristics)
In addition, the items on the IPOS were relevant to patient participants. For example, one patient said, (‘the symptoms were very relatable’ – PT25).
Subtheme 1f: Advocates for implementation (process)
Participants highlighted the importance of engaging people at various staff levels within the healthcare system. These would include having opinion leaders amongst the multidisciplinary staff. Opinion leaders could help spread the message about the benefits of using IPOS (‘I think it’s a good start for people who are taking care of heart failure patients. . . we’re talking about value-based care’ – HCW 12).
It was also mentioned that patients themselves could be a voice for promoting the value of participating in IPOS to other patients (‘If they (patients) themselves know they will, I tell you they will share with others about this (IPOS). . .’ – PT34).
Theme 2: Barriers to implementation of IPOS
Subtheme 2a: Need for adaptation (intervention characteristics)
Both patients and staff felt that there was still a need for the IPOS to be further modified and adapted prior to a large-scale implementation in clinical setting. For example, staff wanted to be able to elaborate on the issues at hand (‘Giving some free text would be better’ – HCW 01). Patients also felt it important to share on their rationale for their particular response (‘even if I tick, it also doesn’t make sense if it is moderate or slight or what. You want to elaborate’ – PT 26).
One patient expressed the importance of tailoring surveys to specific care settings to adequately address distinct concerns. For example, it was suggested (‘Inpatient should have inpatient survey. Outpatient should have outpatient survey’ – PT 34).
Both patient and staff emphasized the need for adapting to current workflows to seamlessly integrate IPOS (‘If you incorporate into their work, that means you are giving them. . . the assessment form (IPOS).’ – PT48). From a healthcare staff workflow perspective, it was crucial to ensure easy access to IPOS results and their trends (‘something easily retrievable that we can see and compare to the previous IPOS’ – HCW 12).
Subtheme 2b: Cultural concerns (outer setting)
Healthcare staff shared cultural concerns regarding the use of IPOS for screening spiritual concerns. For example, the item of ‘peace’ was seen as subjective (‘It is a bit hard to say if he is feeling at peace or not’ – HCW 01). It was also deemed challenging to ask a patient if one was at peace (‘How to ask her, “are you at peace?”’ – HCW 03). Similarly, another staff raised concerns over a patient’s potential misinterpretation of the ‘peace’ item on IPOS, and if it would be seen as signifying ‘death’ and thus be offensive (‘in an Asian country if you talk about peace, they will relate it to death’ – HCW 05).
One palliative care staff stated that culturally, sharing about psycho-emotional concerns could be seen as a weakness (‘For the physical symptoms I think people are more willing to talk about it, cause it’s like, it’s not perceived so much as being weak you know what I mean?’ – HCW12). Another heart failure staff stated that patients tended to hide their emotions, thus making it hard to screen for psycho-emotional concerns (‘they may be looking very cheerful, but I think, we can see they’re worried.’ – HCW03).
Both healthcare staff and patients also shared concerns regarding language literacy. For example, one healthcare staff verbalized that the IPOS would potentially be more suitable for ‘English-speaking participants’ only (‘is this (IPOS) typically for the English-speaking patients’ – HCW01); (‘Those who are English educated, it should not be an issue.’ – PT48). One participant suggested using pictorial presentations for IPOS items, to allow easier administration for patients who speak minimal English (‘With pictorial it is better, for example, if patient is not local. . . only minimal English.’ – HCW05).
Regarding technological literacy, it was stressed that technological aspects related to the use of IPOS were important, because if left unaddressed, these could pose potential barriers to implementation. For example, healthcare staff felt that IPOS should be administered by electronic means for ease of review and integration into the clinical documentation rather than relying on hard copies and that the IPOS interface should be user-friendly (‘we are in an era of the computer. So, I think if the interface is easy to use. . .’ – HCW 12).
On the other hand, this view was not shared by all patient participants. For example, one patient participant maintained that it was important to consider the technological literacy of different types of patients as it would affect the mode of IPOS administration (‘those people who are, who knows how to go online probably is better. But others who don’t go online then you won’t be able to receive a response from them.’ – PT48).
Subtheme 2c: Mindsets and role strains (inner setting)
Although a collaborative culture between heart failure team and palliative care team was acknowledged as an important facilitator for IPOS implementation, this view was not consistent across staff. For example, a heart failure staff noted that the pre-existing network between the two teams may paradoxically reduce the motivation to implement IPOS in a setting where cardiologists were the primary care providers (‘the referral at National Cancer Centre (palliative care), is there for this reason. But the questionnaire (IPOS) may or may not, be the answer to improve that.’ – HCW 10).
Participants also spoke of the varying degrees of acceptance amongst different disciplines for IPOS implementation. Achieving a balance towards change was, to some extent, related to a mindset towards the acceptability of palliative care (If they are from the department of Palliative Medicine, I would definitely tell them this is a good tool to try first and see. But I think for other departments it is a bit difficult’ – HCW 01).
From the patient perspective, educating patients about palliative care and the benefits of participation in IPOS was an essential first step before the implementation of IPOS (‘I don’t think people might understand exactly what you are trying to achieve. Maybe the best way to get that better is to explain about the concept of “palliative care” first and say this is what we are trying to achieve.’ – PT25).
Lastly, heart failure staff, in particular, experienced role strain with regards to expanding their skillsets and role beyond cardiac care. For example, one staff described how personally it felt awkward asking patients about topics on the IPOS as these topics were beyond their heart-related issues (‘It’s also very awkward to me to ask all those questions, because the patients will also think like “what’s happening now. I just came to get my heart checked”’ – HCW09).
Subtheme 2d: Resource constraints (inner setting)
Although it was described earlier that the time required to complete the IPOS was acceptable by most, there remained considerable time constraints in the clinic. Both staff and patients were concerned if there would be enough time for doing the IPOS assessment or for doctors to respond to the IPOS results (‘So, doing this kind of questionnaire is not going to change that reality, that we only have that X number of minutes for a patient.’ – HCW10); (‘whether they have time to read. Cause the consultations are very tight.’ – PT70). One patient also suggested allowing sufficient time for patients to fill in the IPOS to enhance the validity of their responses (‘this helps when I was at home and when I had more time to. . .think’ – PT14).
Regarding other members of the multidisciplinary team, there were also concerns about the time constraints for nurses to complete the staff version of the IPOS (‘I mean the nurses are all generally busy with their own stuff. So, I think it becomes very difficult to ask them to do this (IPOS) because this is something extra which they have to do.’ – HCW01).
Lastly, a participant described that the lack of a dedicated resource for follow-up of palliative care issues after conducting the IPOS survey was also seen as a potential barrier (‘I don’t know whether you can do this in this survey (IPOS) or not? But I think that that is an important part of palliative care. Because if I got a concern and no one is listening to me at home or anywhere. . . I got nowhere to vent. . .maybe that’s where the solution is at.’ – PT25).
Subtheme 2e: Individual needs (individual characteristics)
From the patient perspective, some patients found it important to have a physical document to review while completing the IPOS. Clinical services should also be attentive to provide support in case of any queries related to filling out the IPOS (‘Some people need to really understand or, you know, if nobody’s there you just do it yourself you just anyhow hamtam, hamtam, (“to guess and randomly put an answer”-in Malay))’ (PT 85, 60s, Indian, Female).
In terms of the compatibility of IPOS for individual patients, views varied. In an earlier section on facilitators to implementation, one heart failure patient described the IPOS as ‘relatable’. However, this view was held differently by healthcare staff. For example, a heart failure healthcare staff described that the IPOS could be more suitable for use only by a subset of patients (‘I guess it’s a selective group of patients that we feel like’ – HCW04).
Subtheme 2f: Change process (process related)
Patients also expressed that individual patients might be at different stages of readiness for adopting IPOS (‘Not everyone will put themselves through this. don’t know’ – PT14). From the healthcare staff perspective, both palliative care staff and heart failure staff tended to agree that there may be less priority for using the IPOS, as other tools were already available for evaluating patients under palliative care or heart failure (‘I mean I wouldn’t mind using IPOS, but I already must fill in PCOC- (Palliative care outcomes collaborative)’ – HCW 12).
Both palliative care and heart failure staff opined that it would be better to have a trial period before full-scale implementation of IPOS (‘I will want to see again for myself and then maybe I will like start using this (IPOS)’ – HCW01).
Relationship to key domains of CFIR
Our analysis revealed that facilitators and barriers to implementation of IPOS spanned all five domains of the CFIR (Table 4). For example, in the ‘outer setting’, cultural factors such as having a ‘conducive culture’ were a facilitator for implementation, yet ‘cultural concerns’ were also a barrier to implementation. This was observed for the other four domains of CFIR – ‘intervention characteristics’, ‘inner setting’, ‘individual characteristics’, and ‘process’. We observed that there were more facilitators to implementation in the ‘intervention characteristics’ as compared to barriers, which would be helpful for advocating for the use of the IPOS screening tool locally. We summarized these findings visually in Figure 1 to illustrate the interactions between different components of the CFIR.
Discussion
Main findings
In this study, we found various factors that could affect the implementation of IPOS. Facilitators include: (i) perception of utility, (ii) perception of minimal complexity, (iii) perception of relatability, (iv)conducive culture, (v) dedicated resources, and (vi) advocates for implementation. Barriers include: (i) need for adaptation, (ii) mindsets/role strains, (iii) resource constraints, (iv) cultural concerns, (v) individual needs, and (vi) change process. Facilitators and barriers cut across all five major domains of the CFIR.
With regard to facilitators, a systematic review in the palliative care setting described the importance of having a coordinator present throughout the implementation process, and that pre-implementation educational component would be crucial. 28 A subsequent systematic review published in 2018 by Foster et al. 29 reviewed factors that would help facilitate the implementation of patient reported surveys in more generic settings. Specifically, the review described that implementation ought to be separated into a ‘designing’ and ‘preparation’ stage. In the preparation stage, steps such as getting an organization and staff ready to use the patient reported survey and having a dedicated implementation lead were described as useful facilitators. This is similar to our findings in a cardiology (and non-palliative care) setting where recognition of IPOS as a valuable tool and allocation of dedicated resources for IPOS administration were identified as important facilitators for successful IPOS implementation.
Regarding barriers, our findings of mindsets, role strains, resource constraints, individual factors, and change process are similar to what was described in a recently published editorial regarding barriers to implementing cardiology-specific-outcome measures. 30 In that editorial, barriers included factors related to staff reluctance, system factors, difficulties in patient completion, and clinician interpretation.
When considering potential improvement of facilitators and possible modification of barriers, altering factors related to the ‘intervention’ of IPOS itself, such as elaboration or rephrasing of IPOS items, may prove challenging. While there was a suggestion by a patient that there should be an ‘inpatient’ version of the IPOS versus an ‘outpatient’ version of the IPOS, we believe that this perceived ‘difference’ is more related to the severity of the palliative care issues rather than a qualitative difference in the type of palliative care concerns detected by IPOS screening. This is corroborated by our own results from the validity phase 18 where the patient and staff IPOS scores were higher in the inpatient setting (indicating more severe concerns). Therefore, rather than delineating specific surveys for different settings, we believe that more attention could be paid to planning out the relevant palliative care responses to match the severity of issues that are detected in different care settings.
Additionally, modifying factors related to the inner culture or the ‘inner setting’ or with regards to ‘mindsets’ would possibly yield more successful implementation of IPOS locally. One example is that of the ‘pre-existing collaborative culture’. Establishing a close network between palliative care team and heart failure team is still more likely than not to foster the integration of palliative care principles into usual cardiac care. A close collaborative network could also facilitate palliative care services in generating a ‘tension for change’ and cultivating a ‘collaborative sharing climate’. This in turn supports co-learning and teaching of principles related to screening of needs for patients potentially requiring palliative care support.31,32
With regard to the inner setting and ‘resource constrains’, ‘time’ has traditionally been a significant issue in Singapore, 33 and most recently exacerbated by the COVID-19 pandemic. 34 With increasing demands on healthcare staff, achieving buy-in for IPOS implementation would almost certainly require significant systemic change related to ‘workflows’, as well as the use of appropriate ‘technological’ support and innovation. 35
Both patients and staff brought up considerations regarding cultural sensitivities ‘literacy’ concerns. Poor technological literacy has been described in local publications.36,37 Cultural views towards palliative care and perceived potential stigma of discussing psycho-emotional issues were also similarly described in our prior work.38,39 Therefore, more efforts would be needed to improve patient engagement regarding the value of patient-reported surveys and how support could be given to individuals who have challenges with palliative specific surveys, before large-scale roll out of IPOS for patients with heart failure in the cardiology setting.
Lastly, process factors such as ‘stage of change’ related well with our prior study on the staff validity of IPOS. 18 We noted that a significant number of staff assessments were incomplete or marked by staff as ‘unable to assess’. These were mainly related to psychosocial issues, such as screening for patient’s anxiety, or screening for practical problems. Having a trial period would facilitate specific support to staff who have challenges regarding screening for subjective psycho-emotional symptoms. Inter-rater differences between patient and staff on outcome measures and surveys have also been reported in other settings. 40 Further work on how best to integrate patient and staff assessments as well as which aspects of palliative care screenings could be done by ‘generalists’ versus ‘specialists’ 16 could be explored. Further studies on how to build up palliative care capacity for generalists could also be explored. 41
Strengths and limitations
This study has a few strengths. First, its recruitment of both patients and staff allowed for comprehensive assessment of the factors influencing the implementation of the IPOS in a multidisciplinary context. Second, beyond assessing validity and reliability of IPOS, we have also evaluated barriers and facilitators to identify real-world factors that would influence implementation of IPOS. Third, this study was performed in a non-palliative care setting, in contrast to other studies where patients were recruited predominantly from palliative care services.12,13 We have illuminated the potential challenges of implementing a palliative care-specific patient screening tool in a non-palliative care setting. Our study is especially relevant amid the changing demographics of physicians and growing numbers of patients who will need palliative care support. There is a strong need to determine which patients would benefit most from specialist palliative care versus those who could receive support from healthcare staff with generalist palliative care skills, such as cardiologists.16,41
A minor limitation of this study was that the IPOS was only validated in English, due to funding constraints on the part of the study team. Therefore, we were unable to recruit Chinese speaking participants in the current study. This may explain why staff participants expressed concerns about the potential limitations of the IPOS, particularly regarding its suitability for ‘non-English-speaking’ patients. However, it should also be noted that the literacy profile of Singaporeans has also improved over time and English is now most frequently spoken at home and thus the IPOS should still be acceptable for use by a significant majority of the patient population. 42 As the IPOS had not been formally implemented in the clinical setting, we did not seek participants’ input on the degree to which they felt the various factors influenced the extent of IPOS implementation.
Another potential limitation of this study is related to the patient sample size. While we did achieve data saturation with 10 patients, and it is worth noting that a prior systematic review indicated that data saturation could be reached with sample sizes of 9–17 patients, 22 We also did not recruit any bereaved caregivers as we did not test the caregiver version of the IPOS in our validation phase. Future studies could consider recruiting Chinese speaking patients as well as caregivers to increase the transferability of our findings.
Third, although CFIR is a widely used framework for assessing intervention implementation, there is a possibility that our mapping of findings to the CFIR may have overlooked some factors that are relevant to other settings. Consequently, our results may not be fully representative of various settings with different healthcare systems. Lastly, the study primarily relied on staff and patient interviews. Inclusion of other methods such as observations or involving other stakeholders such as healthcare leadership may provide more comprehensive understanding of the implementation process.
Conclusion
This study provided important insights into the various facilitators and barriers to implementation for IPOS in patients with heart failure in Singapore. We also presented possible strategies for ensuring a seamless implementation of IPOS for patients with heart failure who are cared for in a setting primarily managed by generalists, with specialist palliative care services accessible only through consult.
Future studies could be performed with non-English-speaking participants to substantiate our findings. The short-term, medium-term, and long-term fidelity, reach, and adoption of the IPOS tool on a larger scale in the cardiology setting should also be evaluated in the future, following formal IPOS implementation locally for clinical assessment. Further studies should also be done on how to effectively build generalist palliative care capacity and engage patients in palliative care discussion in a culturally safe and appropriate manner.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524231214814 – Supplemental material for Facilitators and barriers to implementation of a patient and staff reported measure for screening of palliative concerns of patients with heart failure: a qualitative analysis using the Consolidated Framework for Implementation Research
Supplemental material, sj-docx-1-pcr-10.1177_26323524231214814 for Facilitators and barriers to implementation of a patient and staff reported measure for screening of palliative concerns of patients with heart failure: a qualitative analysis using the Consolidated Framework for Implementation Research by Shirlyn Hui-Shan Neo, Jasmine Yun-Ting Tan, Elaine Swee-Ling Ng and Sungwon Yoon in Palliative Care and Social Practice
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.