
Abstract
Background
Physician trainees in pulmonary medicine are not provided with supervised practice opportunities to gain confidence and skill in having serious illness conversations in the ambulatory setting.
Objective
We incorporated a palliative medicine attending into an ambulatory pulmonology teaching clinic to provide supervised opportunities for serious illness conversations.
Methods
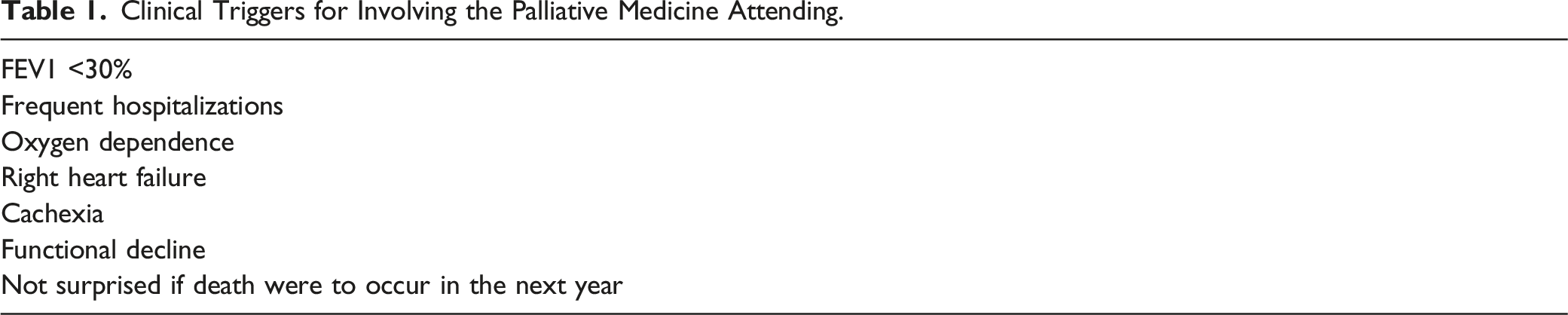
Trainees in a pulmonary medicine teaching clinic requested supervision from a palliative medicine attending based on a set of evidence-based pulmonary-specific triggers that indicate advanced disease. Semi-structured interviews were conducted to determine the trainee’s perceptions of the educational intervention.
Results
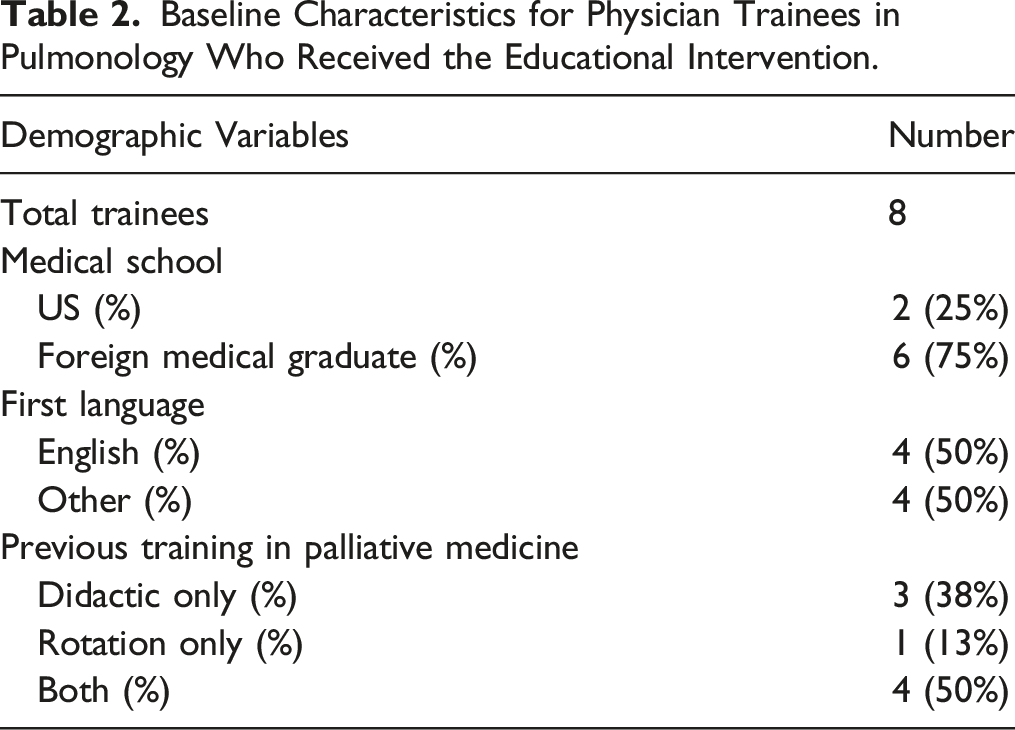
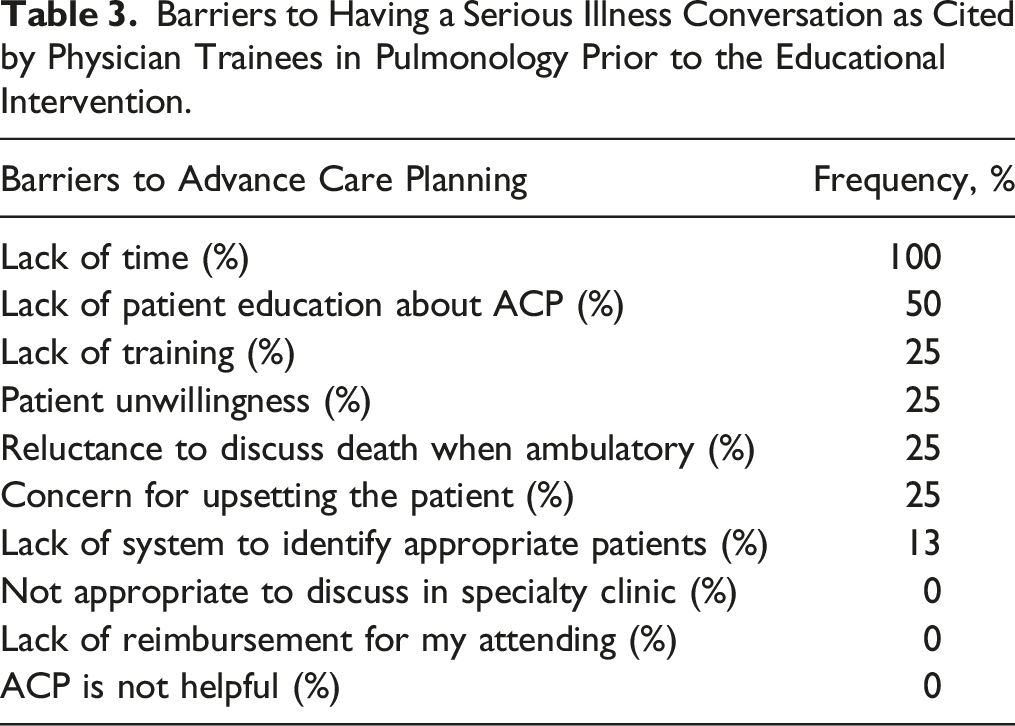
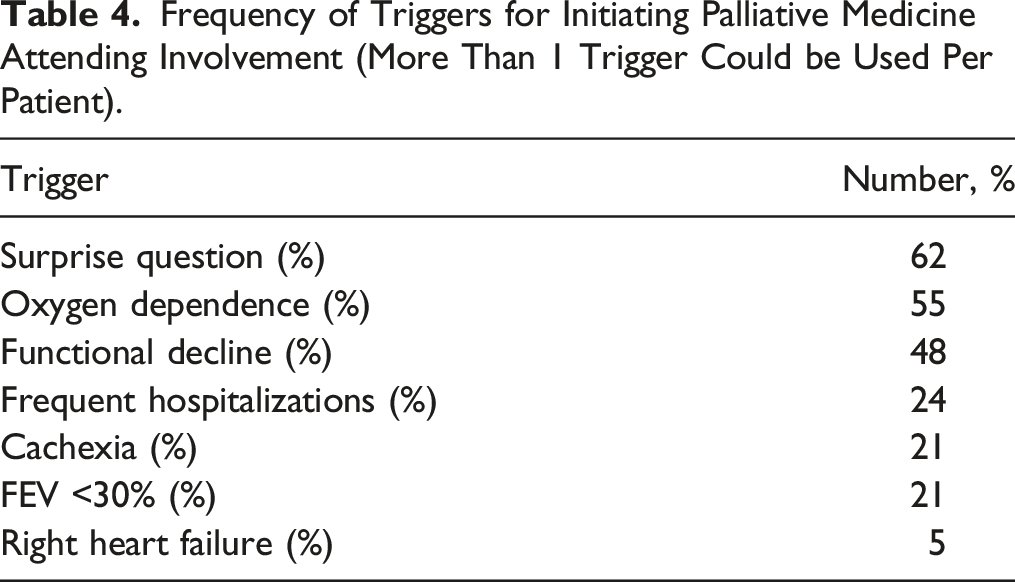
The palliative medicine attending supervised 8 trainees in 58 patient encounters. The most common trigger for palliative medicine supervision was answering “no” to the “surprise question.” At baseline, all trainees cited lack of time as the primary barrier to having serious illness conversations. Themes emerging from post-intervention semi-structured interviews included trainees learning that (1) patients are grateful to have conversations about the severity of their illness, (2) patients do not have a good sense of their prognosis, and (3) with improved skills, these conversations can be conducted efficiently.
Conclusions
Pulmonary medicine trainees were provided practice opportunities for having serious illness conversations under the supervision of the palliative medicine attending. These practice opportunities effected trainee perception on important barriers to further practice.
Keywords
Introduction
Chronic pulmonary diseases are a leading cause of morbidity and mortality worldwide. 1 As a result, it is important that the pulmonologists caring for these patients initiate and navigate conversations that provide prognostic information and align care plans with patient’s expectations, preferences, and concerns – often referred to as serious illness conversations. 2
Most patients with chronic pulmonary disease express a desire to engage in serious illness conversations with their physicians 3 and the American College of Chest Physicians recommends such conversations as an integral part of the management of pulmonary disease. 4 Yet, only a minority of pulmonologists report engaging in these discussions with their patients,5,6 and few patients report that they have had these conversations with their physicians. 7
There are many reasons why physicians do not initiate such conversations, including perceived lack of adequate time, training, and experience; reluctance to discuss death with patients and families; the belief that it is upsetting to patients or will deprive them of hope; the belief that patients should initiate the discussion; and discomfort with communicating a prognosis.8,9 When physicians do start these conversations, they tend to focus on symptoms, prognosis, and biomedical details rather than spiritual and social issues, which tend to be more important to patients. 10
As physicians gain more experience with these conversations, they are more likely to initiate the conversation, feel more comfortable communicating a prognosis, and are less likely to believe that it takes too much time or is upsetting to patients. 11 This suggests that physician trainees require routine opportunities to practice having these conversations in training if they are to be prepared to have these conversations with their future patients. 12 However, few studies have evaluated educational interventions for the physicians caring for patients with chronic pulmonary diseases. 13
This educational intervention aimed to provide pulmonary medicine trainees with supervised practice opportunities for serious illness conversations. We then evaluated this educational intervention to understand what trainees learned from their supervised practice opportunities.
Methods
Clinical Triggers for Involving the Palliative Medicine Attending.
Evaluation Process
We used mixed methods to evaluate the educational intervention. Trainees answered a baseline survey and participated in semi-structured interviews at the end of the intervention period. Interviews began with an open-ended question about the trainee’s experience with the educational intervention and proceeded with the interviewer asking for clarification about information provided. The semi-structured interviews were conducted by 1 of the investigators (LJ) who was not involved in the educational intervention.
Data Analysis
Patient characteristics, palliative activities performed, and type of visit were collected and analyzed descriptively. Trainee survey data was analyzed using descriptive statistics. Two investigators (LJ and MP) independently reviewed de-identified transcripts, used grounded theory to extract themes, assigned codes to the content themes, compared findings, and resolved discrepancies to reach common thematic determinations. Themes were ranked in order of frequency.
Ethical Approval
Our institutional review board approved the evaluation of our educational intervention. Trainee participation in the clinic was required as an educational innovation; the palliative medicine attending was not involved in the academic evaluation of trainees. Patient participation was considered within the standard of care. All trainees provided informed consent to surveys and interviews.
Results
Baseline Characteristics for Physician Trainees in Pulmonology Who Received the Educational Intervention.
Barriers to Having a Serious Illness Conversation as Cited by Physician Trainees in Pulmonology Prior to the Educational Intervention.
Frequency of Triggers for Initiating Palliative Medicine Attending Involvement (More Than 1 Trigger Could be Used Per Patient).
List of Themes Emerging From Semi-Structured Interviews With Pulmonary Medicine Trainees.
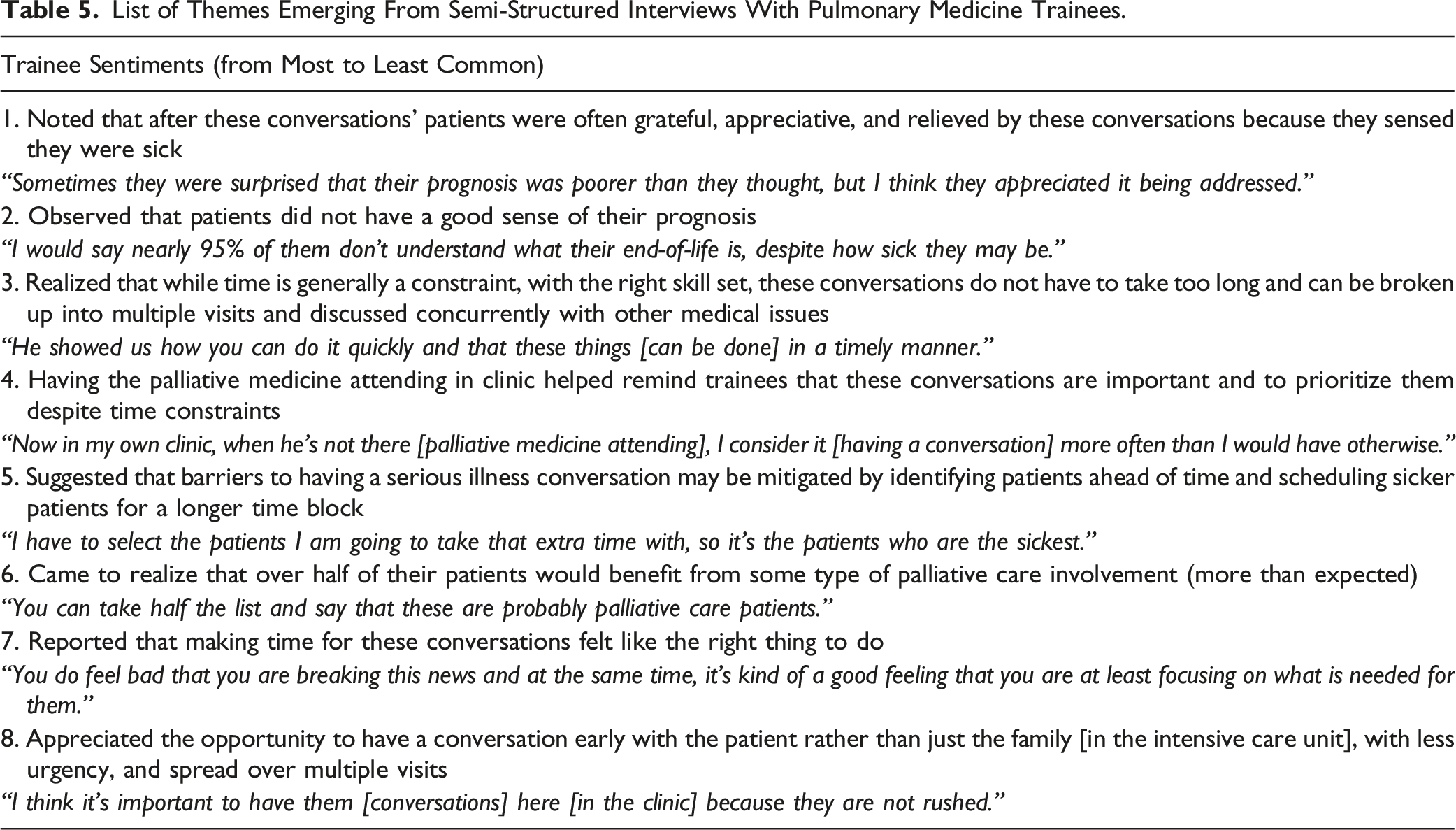
Discussion
Providing pulmonary medicine trainees with supervised practice of serious illness conversations proved to be a useful educational intervention. In semi-structured interviews, trainees consistently reported these conversations did not take as much time as they assumed and realized that they could be spread over multiple encounters (especially when compared to the rushed encounters in the intensive care unit). Even if 1 conversation took more time than usual, the trainees felt these were so important as to justify the additional time. Additionally, trainees learned that rather than patients being unwilling to participate or being fearful, patients seemed grateful and appreciative that their physician was willing to talk about the severity of their illness.
There are several limitations in the evaluation of this educational intervention. We evaluated affective variables, such as trainee perceptions, rather than trainee communication skills. Therefore, we cannot claim that this intervention improved trainee skill. Additionally, our sample size was limited to a small cohort of pulmonary medicine trainees at a single academic institution. While this may have been a small sample size, the themes that emerged in qualitative analysis are concordant with our experience of training multiple cohorts over many years and of implementing and assessing the educational intervention with other trainees. 15
The literature continues to be sparse on effective models for providing trainees with routine practice opportunities to have serious illness conversations. Our model for providing supervision and guidance to practice these important communication skills was feasible and welcomed by the trainees. Two immediate barriers to the universal adoption of such an educational intervention became apparent during the intervention period: limited palliative care staffing and lack of an obvious path for reimbursement if the services of the palliative medicine attending are based on relative value units (RVUs) beyond the advance care planning code. Additionally, our experience suggests that it might be more productive to identify patients with advanced disease prior to clinic, rather than on clinic day. This would prepare the trainee to expect the educational intervention.
We hope that future educational interventions focus on providing physician trainees in pulmonary medicine with sustained supervised practice opportunities. We believe that our evaluation of this educational intervention, along with prior work suggests that sustained opportunity (rather than a single workshop or rotation) is needed to lessen affective barriers and to grow skill in having these important conversations. For our part, we continue to search for ways to incorporate a palliative medicine presence in our pulmonary teaching clinic to provide this important service to our patients, and to train our pulmonary medicine trainees to identify appropriate patients and initiate these important conversations.
Conclusion
Providing pulmonary medicine trainees with serious illness conversation practice opportunities changed trainee perception on important barriers to further practice. Trainees learned that time does not have to be a barrier to these conversations, rather can be improved with skill and that conversations can be conducted over multiple visits. It also taught the trainees that patients desire to have these conversations, do not seem upset by them, and are often waiting for their clinician to initiate them.
Footnotes
Author Contributions
MP, BC, and CW conceived and implemented the educational intervention. MP, AS, and LJ conceived and designed the evaluation. MP and LJ analyzed the results. MP and AS prepared the draft manuscript; all authors reviewed the results and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research ethics
Institutional Review Board approval was obtained for evaluating this educational intervention.
Ethical approval
MedStar Health Research Institute IRB number: 2018-16