
Abstract
Background
Analysis of documented Serious Illness Conversations (SICs) in the inpatient setting can help clinicians align management to address patient and caregiver needs.
Methods
We conducted a mixed methods analysis of the first instance of standardized documentation of a SIC within a structured module among hospitalized general medicine patients from 2018 to 2019. Percentage of documentations that included a description of patient or family understanding of the patient’s medical condition and use of radio buttons to answer the “prognostic information shared,” “hopes,” and “worries” modules are reported. Using grounded theory approach, physicians analyzed free text entries to: “What is important to the patient/family?” and “Recommendations or next steps planned.”
Results
Out of 5142 patients, 59 patients had a documented SIC. Patient or family understanding of the medical condition(s) was reported in 56 (95%). For “prognostic information shared,” the most frequently selected radio buttons were: 49 (83%) incurable disease and 28 (48%) prognosis of weeks to months while those for “hopes” were: 52 (88%) be comfortable and 27 (46%) be at home and for “worries” were: 49 (83%) other physical suffering and 36 (61%) pain. Themes generated from entries to “What’s important to patient/family?” included being with loved ones; comfort; mentally and physically present; and reliable care while those for “Recommendations” were coordinating support services; symptom management; and support and communication.
Conclusions
SIC content indicated concern about pain and reliable care suggesting the complex, intensive nature of caring for seriously ill patients and the need to consider SICs earlier in the life course of patients.
Background
The purpose of conducting Serious Illness Conversations (SICs) is to build prognostic awareness, explore patient hopes and worries and align medical management to reflect each patient’s unique set of goals and priorities. 1 While serious illness communication may happen in the outpatient setting with a trusted provider 1-2 years prior to death, 1 the process is iterative and exists on a continuum. 2 Those conducted during hospitalization can be important for medical care depending on a patient’s acute medical issues and prognosis,3,4 need for prompt medical decision-making or symptom management, presence of prior conversations, 5 caregiver concern and caregiving intensity, 6 availability of palliative care specialists in the outpatient setting,7,8 and other factors. Many older adults with multiple chronic conditions experiencing an acute illness requiring hospitalization face complications including delirium, 9 loss of function, 10 and death 11 requiring multi-disciplinary and more intense and complex decision-making. Conducting SICs during hospitalization for the growing population of older adults with multiple chronic conditions supports patient-centered care, empowers patients, promotes patient dignity, and helps care teams assess and manage more complex needs.
Clinicians, including hospitalists at our institution, have previously received training in conducting SICs12,13 and in documenting these conversations in a standardized manner using an institutionally approved electronic health record (EHR) module.14,15
We present a mixed methods analysis with the aims of better understanding the characteristics of hospitalized patients with a first instance of standardized documentation of a SIC within a structured electronic health record (EHR) module and the content of SICs within this institutionally approved module for patients hospitalized on a general medicine service. We hypothesize that patients with standardized documentation of a SIC have high comorbidity and caregiving needs in addition to high mortality.
Methods
Study Design, Participants, Setting, Data Sources
We conducted retrospective, mixed methods analyses of adult (≥18 years old), general medicine inpatient encounters with a first instance of standardized documentation of a SIC within a structured electronic health record (EHR) module at Brigham and Women’s Faulkner Hospital (BWFH), a community teaching hospital affiliated with Mass General Brigham (MGB), a large integrated health care system in Massachusetts, from October 2018 to August 2019. All data were obtained from the enterprise data warehouse including data from our EHR (Epic Systems, Inc). The MGB institutional review board approved this study.
Quantitative Analyses: Patient Characteristics and Outcomes
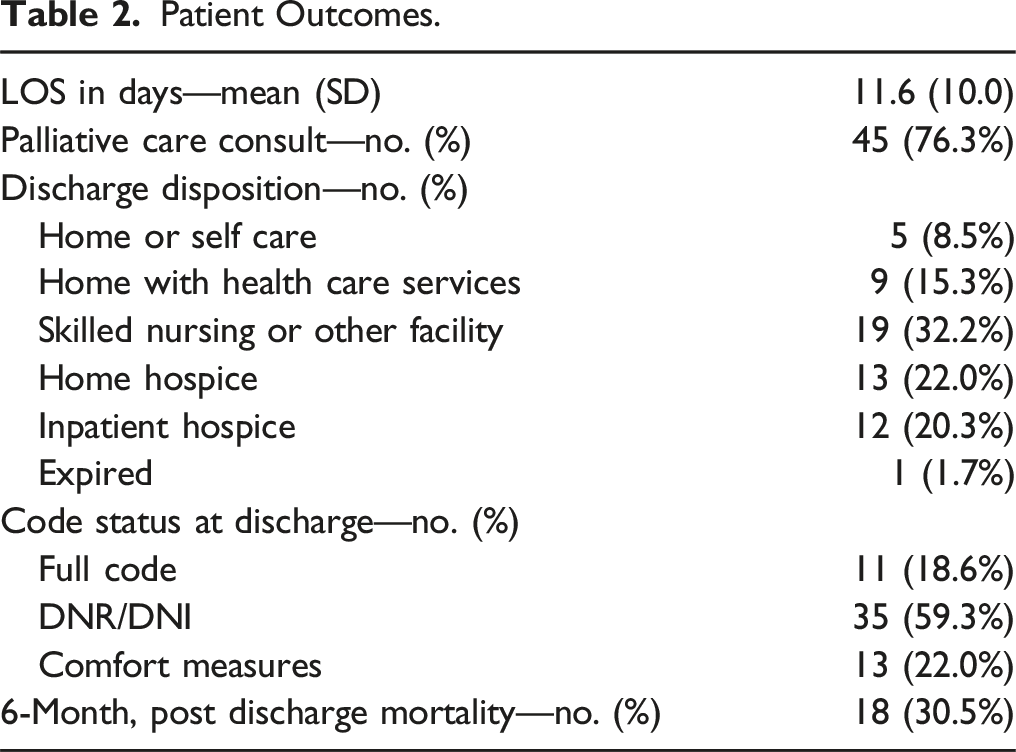
We used descriptive statistics including percentage and mean (standard deviation (SD) to measure and report patient demographics: age, sex, ethnicity, race, primary language, insurance, income, comorbidity measures including Epic’s Risk of Unplanned Readmission (Readmission Risk Score [RRS]), 16 Elixhauser/Van Walraven comorbidity score, 17 and electronic Cardiac Arrest Risk Triage (eCART) (risk of death, cardiac arrest, or ICU transfer) score 18 on admission, diagnosis related group (DRG) weight and hospitalizations in the year prior to index hospitalization. Clinical outcomes included length of stay (LOS), palliative care consult, discharge disposition, code status on discharge, and 6-month post-discharge mortality.
EHR SIC Module
The SIC EHR module is reflective of the key components of SICs 19 and includes structured modules with use of radio buttons that physicians can use to describe clinicians’ “prognostic information shared,” and patient “hopes” and “worries” with the ability to include additional free-text comments. A provider can use more than 1 radio button within each structured module. As an example, a provider can choose ‘be comfortable,’ ‘be at home,’ and ‘achieve life goal’ radio buttons to document the hopes of their patient. The module also contains free-text questions to describe “patient illness understanding,” “What’s important to the patient/family?” and “Recommendations or next steps planned.” Providers in any setting, including the primary inpatient team, palliative care or geriatric consultants, and social workers, can fill out the module partially or in its entirety depending on what parts of the conversation happened during a clinical encounter. Documented modules are stored in a flowsheet data element and can be found quickly by clicking on a patient’s code status in the patient storyboard within the Epic EHR, making review of prior conversations readily accessible to all providers.
Quantitative SIC Module Entry Analysis
The number and percentage of standardized documentations of SICs within the EHR module that included a free text description of patient or family understanding of the patient’s medical condition are reported. The number and percentage of standardized documentations of SICs that used each radio button within the following structured SIC modules are reported: “prognostic information shared,” “hopes,” and “worries.”
Qualitative SIC Module Entry Analysis
Using grounded theory approach, a hospitalist (MKS) and a palliative care physician (JRL) analyzed the free text entries to 2 open-ended questions: “What is important to the patient/family?” and “Recommendations or next steps planned.” An initial coding schema was developed based on previously identified domains of serious illness conversations between patients and providers 13 as well as a priori categories. Coding was performed independently by MKS and then reviewed with JRL. Disagreements were resolved with consensus-based discussion aimed at clarifying and refining the coding scheme. Themes were identified as they emerged. Microsoft Excel 2019 was used for thematic analysis.
Results
Patient Demographics.
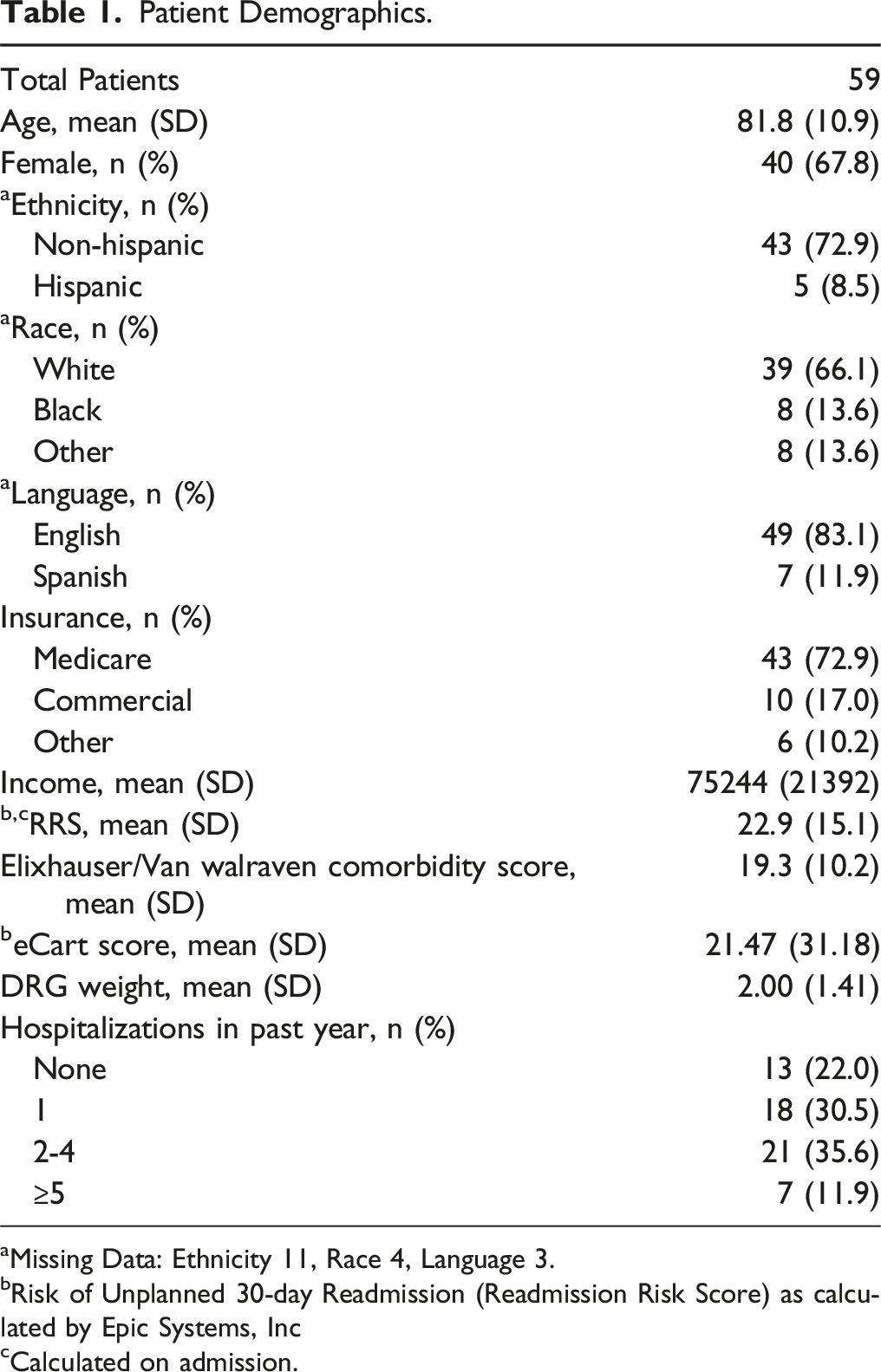
aMissing Data: Ethnicity 11, Race 4, Language 3.
bRisk of Unplanned 30-day Readmission (Readmission Risk Score) as calculated by Epic Systems, Inc
cCalculated on admission.
Patient Outcomes.
Mixed Methods Analysis of Standardized Serious Illness Conversation Documentation.
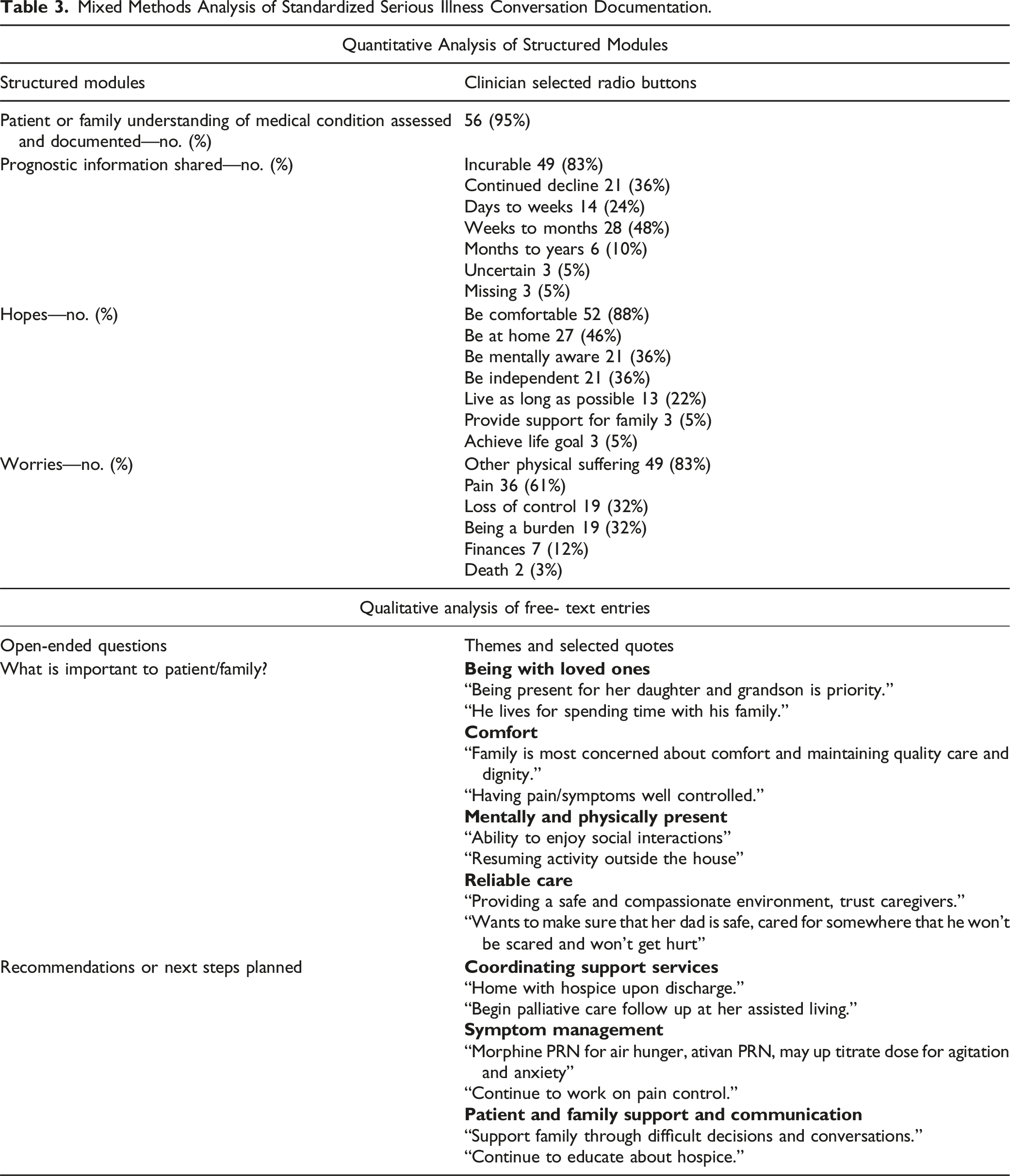
Themes generated from analysis of free-text responses to the open-ended question “What is important to the patient and family?” included being with loved ones; comfort; mentally and physically present; and reliable care. Coordinating support services, symptom management, patient and family support, and communication were themes generated from thematic analysis of free-text responses to the open-ended question “recommendations or next steps planned.” Illustrative quotes are included in Table 3.
Discussion
Unsurprisingly, a first structured standardized documentation of a SIC within an EHR module during hospitalization to a general medicine service occurred late in the life course of patients and frequently by or in conjunction with a palliative care consultation. Patients had elevated comorbidity burden and most had a recent prior hospitalization. Upon discharge, almost all of the patients either required social support through home health care services, skilled nursing or other facility admission or inpatient or home hospice. Approximately 30% of patients died within 6 months of discharge. This is reflected in the poor prognostic information shared by providers to patients: incurable or continued decline, days to weeks or weeks to months to live. The most frequently selected radio buttons for the “hopes” module were to be comfortable and to be at home while those for the “worries” module included other physical suffering and pain. Themes generated from analysis of free-text responses to the “What is important to patient/family?” open-ended question were being with loved ones; comfort; mentally and physically present; and reliable care. Coordinating support services; symptom management; and patient and family support and communication were themes generated from analysis of free text entries to “Recommendations or next steps planned.”
Patients admitted to medical services are among those with the highest mortality, 20 especially among patients aged 70 years or older. 11 Older patients who experience hospitalization often have functional and cognitive decline and require substantial assistance for activities of daily living (ADLs). 21 For these patients especially, it is important to consider SICs in any setting, including during hospitalization, as the patient’s medical status changes, as their caregiving needs rise, and prior to the patient losing capacity, as most patients with serious illness are open and want to have these important conversations.11,22 Prior to death, many patients experience hospitalization or other exposure 23 to providers, marking several opportunities to have a SIC or revisit this conversation with the patient in multiple settings and contexts to understand their priorities and provide goal concordant care. In this unique study, structured SIC documentation made it easy to aggregate results and learn the extent to which patients and their families did not want aggressive care at the end of life. We can assume that these would be the same wishes of many other hospitalized medical patients who did not have the opportunity to participate in an SIC.
The most often selected radio buttons for the “hopes” module closely mirrored many of the themes generated for the “What is important to patient/family?” open-ended question: comfort, being with loved ones, be mentally aware and be independent. These results are not surprising and are reflected in prior research. 24 Having “reliable care” is also important to patients and those closest to them with the ability to place trust in providers in a safe and compassionate environment. 25 This is especially relevant for this vulnerable population at the end of their life course and with high caregiving needs and is likely reflective of the challenges those caring for the patient at home face, including managing symptoms.26,27 End-of-life care is complex and intensive requiring multi-disciplinary teamwork, collaboration and communication with the patient and loved ones, and optimal use of available resources to provide mental, physical and spiritual care of the dying patient.28,29
Themes generated for the “Recommendations or next steps planned” open-ended question, including coordinating support services, symptom management and patient and family support and communication, are reflective of the challenging nature of caring for patients with high comorbidity at the end-of-life, including the difficulty in treating pain and other symptoms. It is helpful to have prior awareness of patient priorities through having SICs prior to this stage so the focus can be on medical management and alignment with these priorities. Talking with those providing care to the patient is important as the caregivers may require substantial support at home. 30 Additionally, most patients had a palliative care consult and these themes are also likely reflective of the additional, expert recommendations from palliative care consultants. This also draws attention to the need to have more training for primary providers to care for patients at the end-of-life.
Limitations of this study include that it is single site, low overall standardized documentation of SICs within the EHR module (thus leading to likely selection bias), and the inability to capture and analyze conversations recorded elsewhere within the EHR. In addition, documentation is only a proxy for the conversation itself and represents the clinician’s interpretation of the conversation. Lastly, the radio buttons, while useful to facilitate conversations, can also influence the choices made and documented.
In conclusion, first standardized documentation of a SIC within a structured module occurred late in the life course of patients admitted to a general medicine service and often by or in conjunction with a palliative care consultant. Analysis of SIC content indicated that most patients and families were concerned about pain or other physical suffering and having reliable care with good communication suggesting the complex and intensive nature of caring for patients with a serious illness and the need to support families and caregivers and provide additional resources and training to primary providers caring for these patients. SICs should be considered in hospitalized older adults with multiple chronic conditions, ideally when patients are still able to express their wishes, to ensure that they receive goal-concordant care. Providers should also be mindful of the burdensome nature of caregiving for a patient at the end-of-life when engaging in conversations about goals and values for seriously ill, hospitalized older adults.
Supplementary Materials: Please direct any questions and requests for data and/or models to the first author.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the a grant from the Controlled Risk Insurance Company (CRICO). CRICO had no role in the design or conduct of the study, the collection, analysis, or interpretation of data, or preparation or review of the manuscript. The conclusions in this report are those of the authors and do not necessarily represent the official position of AHR.