
Abstract
Background:
There is a growing need for palliative care for patients near the end of life and their caregivers. Palliative and end-of-life care (EoLC) education are recommended for all health care (e.g., physicians, nurses, and allied health practitioners) and social care professionals (e.g., social workers) to ensure the quality of services. However, less attention has been afforded to generic, in contrast to specialized, EoLC education. This study evaluated the effectiveness of a series of short-term generic EoLC educational programs for health and social care professionals.
Method:
A pre-post survey design was adopted, focusing on different EoLC core competences.
Results:
Significant improvement was observed in all perceived competences after the educational programs, regardless of participants’ occupation or EoLC experience. Perceived competence in self-care was rated significantly higher than all other competences prior to the programs. Healthcare professionals rated significantly higher on competence in symptom management than social workers. Scores on communication skill and self-care competences were significantly higher following longer (i.e., 16-24 hours) than shorter (i.e., 4-8 hours) programs.
Conclusion:
Generalist palliative/EoLC educational programs may enable health and social care professionals to refresh and extend their knowledge and skills and enhance their perceived competence in providing EoLC. Further research on generalist palliative/EoLC education is needed to examine the impact of continuing training on professionals’ actual practice in EoLC and palliative care.
Keywords
Introduction
In 2017, it was estimated that 25.7 million people worldwide required end-of-life palliative care. 1 With an aging population, an increasing number of deaths from non-communicable diseases and chronic diseases, coupled with the recent COVID-19 pandemic, the need for end-of-life care (EoLC) is expected to continue to rise rapidly. Affirming that patients with a life-threatening illness have a human right to palliative care, 2 society has a responsibility to ensure all people living with life-threatening illnesses are provided quality care, regardless of disease, age, or care setting. Since individuals and families affected by end-of-life issues can be found in different settings and in different levels of the health care system, EoLC education should be provided to all health care professionals including physicians, nurses and allied health practitioners, as well as social care professionals such as social workers, and not simply to EoLC/palliative care specialists only, to implement the shared care model. 3 A care model consisting of a primary level of palliative care and a specialized level has been advocated for building a sustainable care model for patients with serious illnesses. 4 Similarly, the World Health Organization has proposed 3 levels of palliative care education to upskill professionals to provide differentiated levels of care: the palliative care approach for all health professionals, generalist palliative care for those who regularly working with patients with advanced illnesses, and specialist palliative care for whom have to manage patients with more complex symptoms.5-7 Although formal education for third-tier palliative care specialists is well developed, general education for health and social care workers is less so.
Continuing education is recognized as essential to ensure that responses to regulatory changes across EoLC and palliative care retain their currency. 8 However, recent research has documented a lack of EoLC and palliative care education among health and social care professionals in non-palliative care settings. 3 An institutional survey in 2019 illustrated that 38% of critical care nurses reported having received no education on palliative care in the previous 2 years. 9 A US study of social workers found similar results, only 45.3% of whom reported that they had attended a conference related to hospice/palliative care. 8 Insufficient education leaves EoLC/palliative care providers feeling less competent, often susceptible to experiencing “burnout” and emotional exhaustion, 10 and higher moral distress. 9 Moreover, a survey of social care workers identified insufficient financial incentives for participating in relevant courses (84%) and time away from work (50%) as the main barriers impeding their participation in further professional development. 8 Thus, introductory and time-limited generic palliative and EoLC learning might provide a practical means of equipping professionals who are new to EoLC with basic competencies, while providing refresher training for professionals with existing knowledge. This study, therefore, focused on short-term palliative and EoLC educational programs.
Previous research has evaluated short-term training (ranging from 3 to 72 hours’ duration) and demonstrated that it may effectively improve physicians’ and/or nurses’ self-efficacy in different domains (e.g., knowledge, advanced care planning, symptom management, and communication skills).11-15 Perceived competence is a psychological construct corresponding to self-efficacy that is characterized as an individual’s self-perception of their capabilities or skills required to perform an action or behavior in a particular situation.16-18 Evidence suggested that perceived competence is causally linked with actual performance as well as psychological strain and job stress, which a strong belief in one’s capabilities could enhance his/her organizational performance, 19 while reduced emotional exhaustion and feelings of depersonalization at work. 20 Nevertheless, most existing studies have focused on health care professionals and have largely overlooked social care professionals.21-24 Studies that have involved both health and social care professionals have focused on interprofessional collaboration or 1 or 2 competences rather than multi-dimensional competency in end-of-life and palliative care.13,25-27 One pilot study reporting on a 9-month interprofessional palliative care curriculum for both health and social care workers targeted specialist palliative care professionals exclusively and involved only a very small sample (n = 24), thus rendering generalization to other tiers of care and rigorous inter-professional comparison difficult. 28 It is also unclear if the length of EoLC teaching and experience makes a difference to the effectiveness of short-term educational programs.
This study fills the void by examining the effectiveness of a series of short-term palliative and EoLC educational programs for health and social care professionals in improving participants’ competences. Specifically, the study differentiated changes between participants from different professional backgrounds, years of experience in EoLC and the length of the programs. It was hypothesized that participants with more EoLC experience would demonstrate a lower level of improvement, participants would demonstrate a higher level of improvement in programs focused on their respective discipline, and longer programs would yield better results.
Method
The Educational Programs
Thirty-four educational programs related to EoLC were organized by the Jockey Club End-of-life Community Care Project in Hong Kong between April 2016 and May 2018, covering the 7 domains in the end-of-life competency framework developed by the Project team at the University of Hong Kong in 2016. 29 The format of delivery combined didactic presentation, small group discussion, case sharing, role-playing scenarios and experiential exercises. The programs ranged in duration from a single session (4 hours) to 6 sessions (24 hours), covering 1 (20 programs) or more domains (14 programs) as shown in Table 1. An average of 12.54 (SD = 5.51) hours of training completed per participant.
The Focus and Length of the Educational Programs (N = 786).
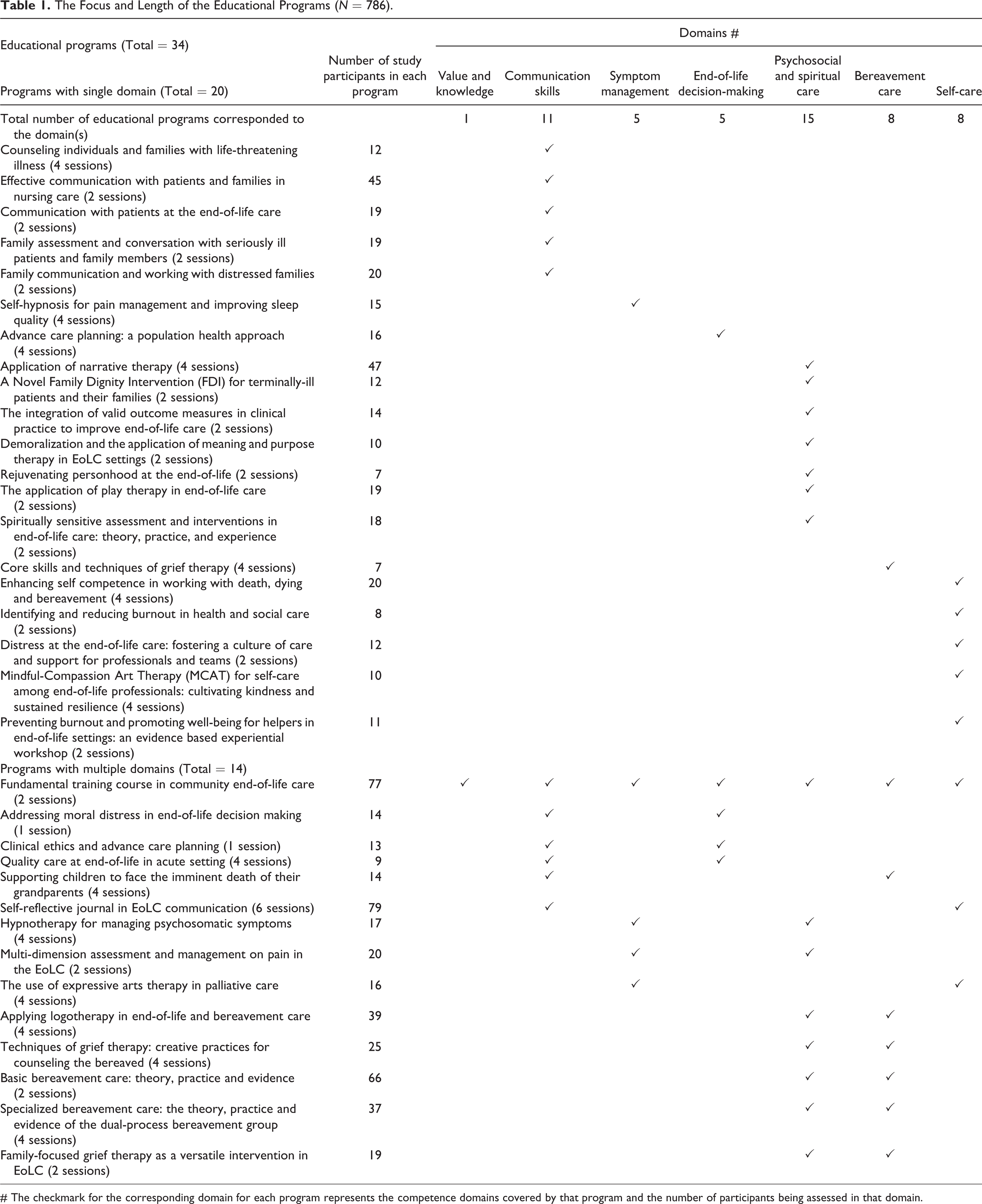
# The checkmark for the corresponding domain for each program represents the competence domains covered by that program and the number of participants being assessed in that domain.
Participants and Procedure
Study participants were health and social care professionals (nurses, social workers, and allied health practitioners) who had attended any of the educational programs. Participants were recruited via bulk mail disseminated by the program organizer to a list of local social and medical service settings. Ethical approval was granted by the Human Research Ethics Committee of the University of Hong Kong (EA1601006). Pre- and post-training questionnaires were distributed by the event organizer at the training venue after obtaining participants’ informed consent. Participation in both the training program and the study was completely voluntary. Records of responses at 2 time-points were matched using the first five-digits of participants’ phone numbers.
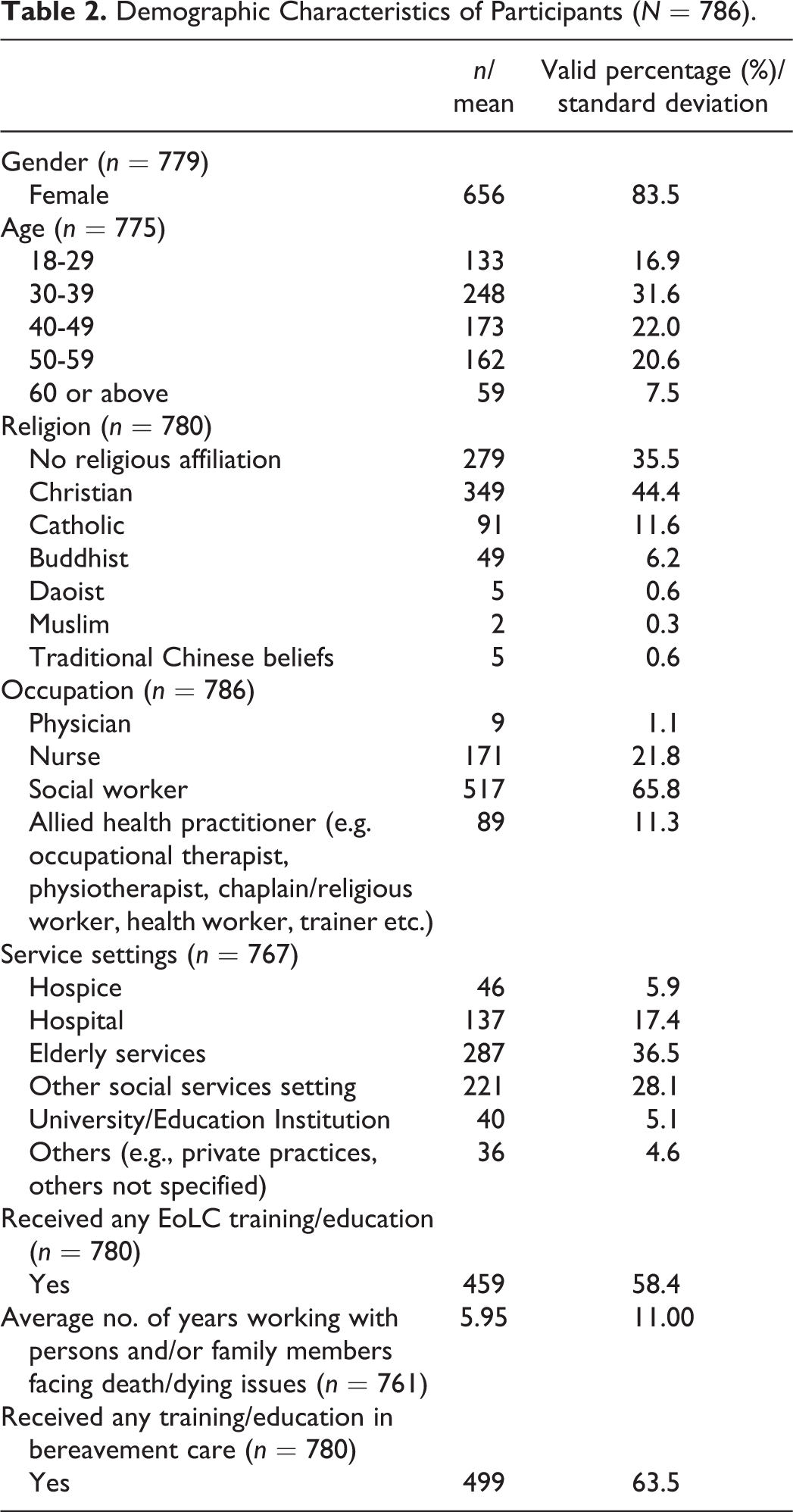
Among 1632 health and social care professionals participated in the training program, 900 and 79 took part in the study; a response rate of 60.0%. Excluding 193 participants who did not complete the post-questionnaire, 786 participants were included in the final analysis. Demographics of the final sample showed no significant differences compared with those who did not complete the post-questionnaire. Detailed demographic characteristics are shown in Table 2.
Demographic Characteristics of Participants (N = 786).
Measures
Information was collected on various demographic variables: gender, age, religion, occupation, service setting, EoLC and bereavement care training/education experience, and the number of years working with persons facing death/dying issues and their family members.
The Comprehensive Competences End-of-Life Scale (CECCS) developed by Xiu, Chow, and Chan, 30 was used to assess participants’ perceptions of their competence in 7 domains of EoLC: overarching values and knowledge (OVK; 3-items), communication skills (5-items), symptom management (4-items), psychosocial and community care (PSCC; 5-items), EoLC decision-making (5-items), bereavement care (2-items), and selfcare (2-items). Each item is rated on a 10-point Likert scale from 1 (not confident at all) to 10 (very confident), and a subscale score for each domain is calculated by taking the mean of all competence items under the domain. Different professionals were using the same scale measuring the level of recognizing and capability in managing, applying the skills as well as offering the care. Participants were asked to complete the subscale(s) of EoLC competence in the CECCS corresponding to the topic of the educational program they completed (see Table 1). The entire inventory and subscales illustrate good internal reliability for health and social care professionals (Cronbach’s α ranging from .87 to .97). 30 The internal consistency of the inventory in this study was acceptable (Cronbach’s α = .63-.97).
Data Analysis
Data were analyzed using SPSS 25.0. A series of paired-sample t tests was conducted to compare pre-to-post changes in different domains for each profession, with a 1-tailed significance level of 0.05. Analysis of Variance (ANOVA) was used to compare participants’ perceptions of their competence levels at baseline (pre-test score). Subsequently, a Bonferroni adjustment for multiple tests was undertaken to compare each p-value to an adjusted significance level in order to reduce Type I error. 31 Repeated measures ANOVA were employed to examine the baseline scores across the 7 domains. We used Mauchly’s test of sphericity to assess whether or not the assumption of sphericity was met, and the Greenhouse-Geisser epsilon where necessary. A 3 (professions: nurses, social workers, and allied health practitioners) x 2 (time: pre- and post-questionnaire) mixed-design ANOVA with repeated measures was run to compare the mean differences between groups in each competence domain. The same analysis was also used to examine whether participants with less EoLC experience (less than 3 years) showed a steeper improvement than those with more experience (3 years or above), and compare the participants’ changes in programs that lasted longer (4-6 sessions) to programs that lasted shorter (1-2 sessions). To reduce self-selection biases, physicians (n = 9) was removed from the analysis in all domains, while allied health practitioners were excluded from the domains of OVK and EoLC decision-making as the number of participants is extremely small (n = 3; n = 8, respectively).
Results
Baseline Scores Across Domains and Professional Groups
The overall baseline scores were significantly differed across 7 competence domains, F(3.09, 231.66) = 78.42, p < .001, η 2 = .38, with a small effect size. Perceived competence on self-care was significantly higher than all other domains (p < .01). Scores on symptom management, however, was the lowest, and apart from self-care, it was also significantly lower than values and knowledge, communication skills, and bereavement care (p < .05). By profession, significant difference was found only in the domain of symptom management with a medium effect size, F(2,175) = 5.65, p = .004, η 2 = .061). Nurses scored significantly higher perceived competence than social workers (p = .004).
Effectiveness of the Training for Different Professions
Table 3 presents the results of the paired-sample t tests among different professions (also see Supplementary Figure 1). Significant improvement was found in all the subscales of perceived competence (p ≤ .001) for nurses, social workers, and allied health practitioners. These improvements were qualified by medium-large effect sizes (r = .60-1.15).
Descriptive Statistics and Results of Paired-Sample t Tests by Professions.
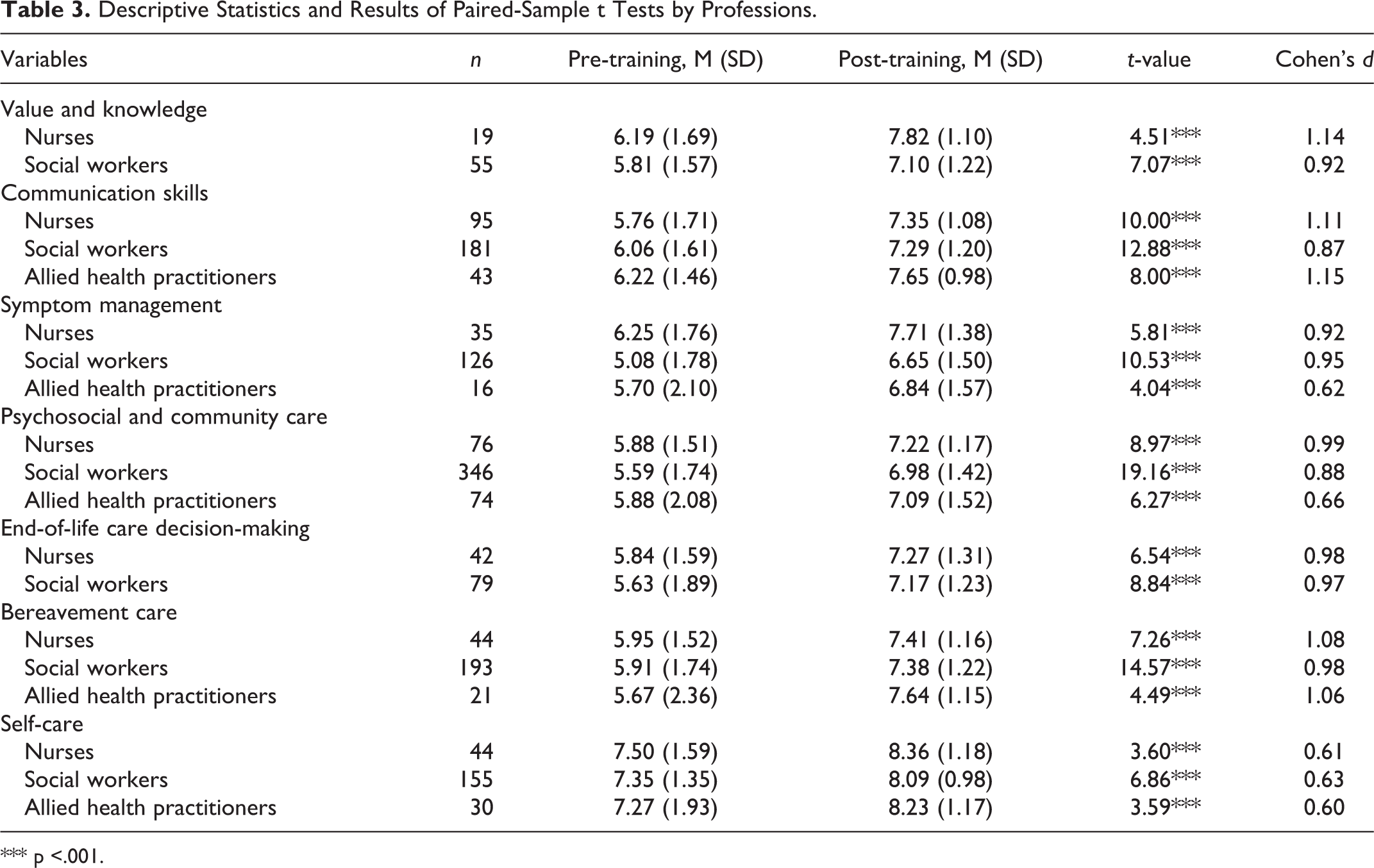
*** p <.001.
The Extent of Benefit Between Different Professional Groups
No significant between-subject main effect for professions was showed (p > .05), but a significant within-subject main effect for time was found in all competence domains (p < .01), suggesting significant improvement in perceived competence at post-training. The interaction between professions and time was non-significant (p > .05), indicating the pre-post difference on perceived competence did not differ across nurses, social workers, and allied health practitioners (see Supplementary Table 1).
Improvement Among Participants With Different Lengths of EoLC Experience
No domain showed significant difference in terms of the experience by time interaction (p > .05). The extent of improvement in perceived competence did not differ between professionals who had more and less than 3 years’ EoLC experience. The results of mixed ANOVA are displayed in Table 4 (also see Supplementary Figure 2).
Descriptive and Inferential Statistics for the 2 × 2 ANOVA (< 3 Years vs. ≥ 3 Years x Pre-Test vs. Post-Test).
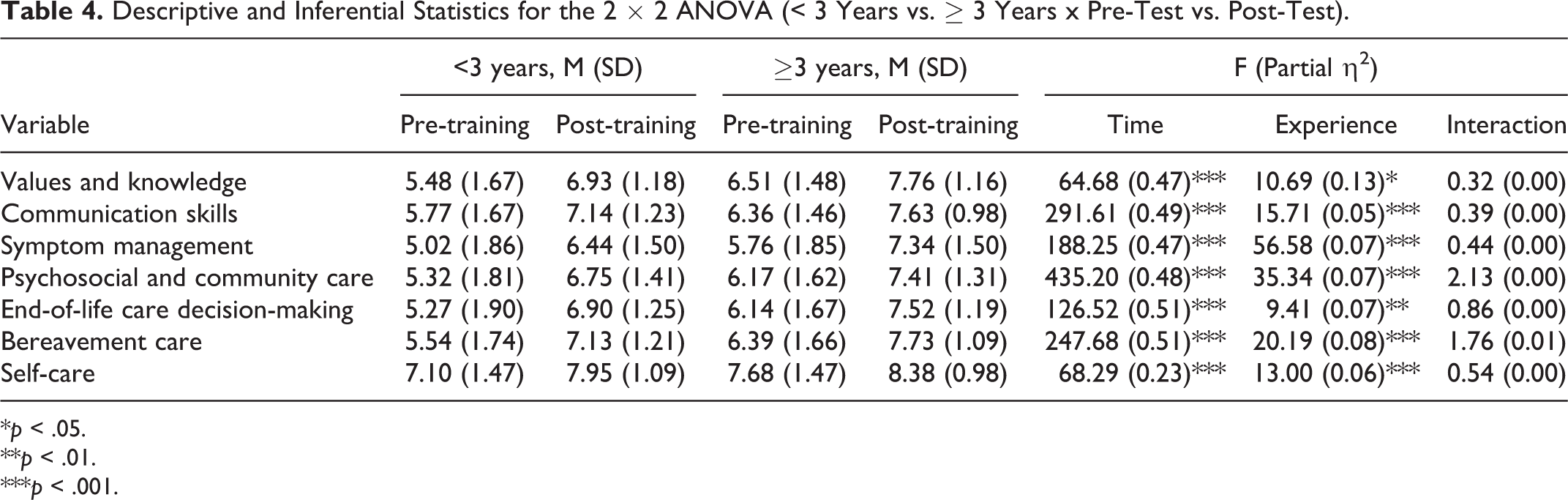
*p < .05.
**p < .01.
***p < .001.
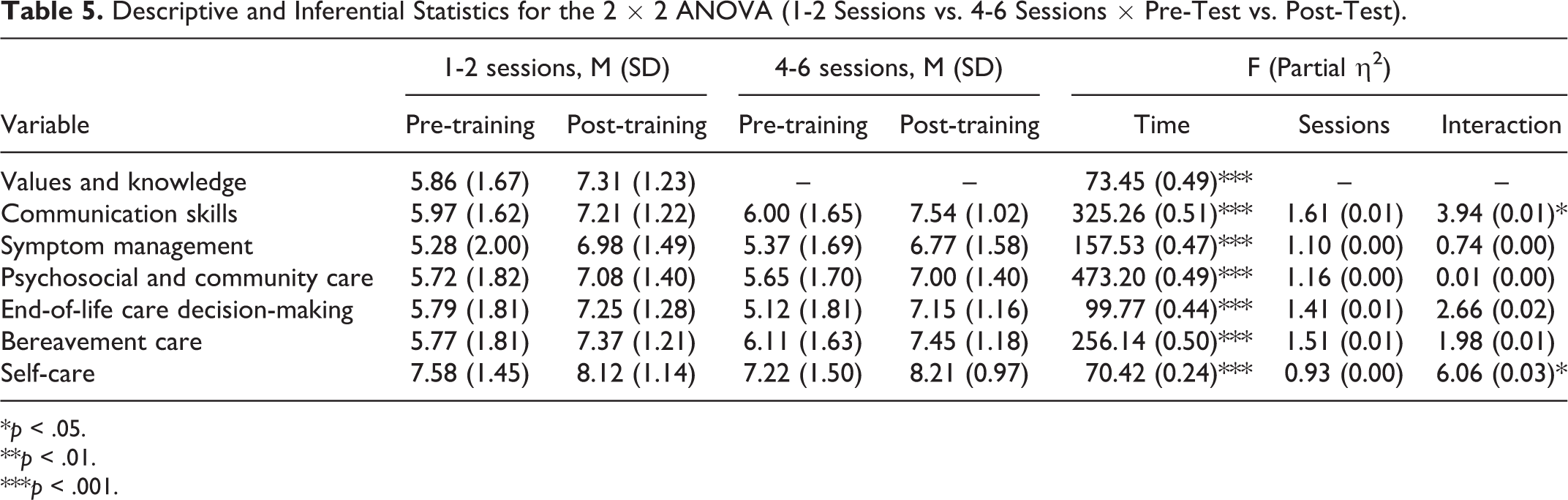
Improvement for Participants in Educational Programs of Different Length
Significant length by time interaction was found in the communication skills and self-care domains. Improvement of competence in both domains was significantly higher in programs of longer duration. Table 5 shows the results of mixed ANOVA (also see Supplementary Figure 3).
Descriptive and Inferential Statistics for the 2 × 2 ANOVA (1-2 Sessions vs. 4-6 Sessions × Pre-Test vs. Post-Test).
*p < .05.
**p < .01.
***p < .001.
Discussion
This study evaluated a series of short-term generic palliative and EoLC educational programs covering 7 core competencies for nurses, social workers and allied health practitioners. Following all programs, both health and social care professionals identified a significant improvement in perceived competence in terms of values and knowledge, communication skills, symptom management, psychosocial care, and self-care. The baseline scores, when compared to those health and social care professionals in the validation study of Xiu, Chow and Chan, 30 were comparatively lower in all domains except self-care. After receiving the educational programs in the present study, their scores increased and higher than their baseline and even the reference score in the validation study. Nevertheless, the changes were at statistically significant level. This further supports that these short-term education programs, ranging from 1 to 4 sessions, are a practical and viable means of enhancing the confidence of health and social care professionals from different backgrounds in providing generic palliative and EoLC services. Most of these programs were offered to a diversified background of health and social care professionals. The absence of significant interaction of group and time effects infers that the level of change after the training are similar between different professionals. Thus, when offering palliative/EoLC training, in particular at generalist level, accepting trainees of different disciplines are acceptable. Similarly, the length of experience in EoLC does not affect the changes. The longer programs on communication skills and self-care domains indicated a larger improvement, thus, a longer length of education is recommended on these topics as these are practice-oriented.
The educational programs effectively improved social workers’ confidence on symptom management (with a large effect size, d = .95), and narrowed the gaps between health and social care professionals. Social workers were less confident in managing symptoms than nurses prior to the education. This is unsurprising since nurses receive specialized training in nursing care related to control of physical symptoms in regular training, 32 while social workers do not. This, however, could not be neglected because social workers are well positioned to provide comprehensive assessments to explore the interconnection of mental and physical symptoms, and should recognize the need for specialist consultation and referral to address patients’ psychosomatic symptoms. 33 The results also suggest that social workers may have greater potential for change following generic training and benefit more than their nursing and allied health peers.
Compared to other competences, perceived competence in self-care was highest for all groups at both baseline and post-training. A higher baseline score in self-care may imply that participants coped relatively well with the stress of death-related work. Two self-competence concepts from the Self-Competency in Death Work Scale (SC-DWS): existential coping and emotional coping, were adopted in the self-care subscales in the CECCS, 34 but may not be representative of overall self-care competence. A recent study has also argued that management of stress (i.e., coping) should not be the only indicator of self-care in EoLC services. 35 The current study draws attention to the pressing need for training on symptom management for social care professionals and highlights the need for further clarity regarding self-care.
Experienced and less experienced professionals showed a similar extent (i.e., approximately 1-point) of increased confidence. However, a further series of independent t-tests revealed that the experienced group had significantly higher scores in all competence domains than less experienced group in both pre- and post-tests (p < .05). Thus, the original difference due to EoLC experience remained even the programs had enhanced both groups to a similar extent. Additionally, no significant difference in terms of the increased confidence between nurses, social workers, and allied health practitioners in all competence domains (i.e., approximately 1-point). The above finding indicates that prior in-depth knowledge and experience in the field is not necessary when participating the generic educational programs. The programs help to improve the confidence of core competences that are needed in palliative/EoLC among health and social care professionals regardless of their occupation and experience in EoLC.
The longer the training programs on communication skills and self-care domains, the larger the change. A longer program may provide more opportunities for experiential activities and followed by debriefing and self-reflection which are paramount in self-care. 36 Short programs of 1 to 2 sessions may be optimal for topic related to value and knowledge, symptom management, psychosocial and community care, end-of-life decision making and bereavement care. As for the program on communication and self-care which is more action and practice-oriented, more time is needed.
This study has several limitations. Firstly, no follow-up tests were undertaken to ascertain the lasting effect of the training on professionals’ perceived competence, and their actual practices in EoLC/palliative care services. Secondly, the measurement of competence is a proxy only. Ideally, direct observational measures or report by supervisors or service recipients on assessing the competence of the professionals will be more reliable. With the time and design constraints, these have not applied in similar studies, but deserve attention. Thirdly, the absence of a control group meant that it was not possible to compare the perceived competence of training program participants and professionals who did not undergo training. Fourthly, the sample was skewed toward females and social workers, which may limit the generalizability of the findings to more diverse health and social care professionals and male professionals. Fifthly, the educational programs evaluated in the study were non-standardized, for which there was no clear delineation of the mechanisms of change, content and pedagogies. Sixthly, the absence of an intention-to-treat analysis for dropouts indicates potential bias in the findings. Lastly, there were not an identified threshold of level of competence. More insights will be gained if a threshold is available. Particularly, the differentiated impacts of the training programs for those below and above threshold. Nevertheless, despite these limitations, various avenues for future research are suggested. Future studies should validate the present findings using a more diverse sample of health and social care professionals, and examine the longer-term effects of generic EoLC training.
This study lends support to the efficacy of short-term generic EoLC education in enhancing perceived competence among health and social care professionals regardless of their experience in EoLC and their occupations. The finding also highlights the importance of generic training on symptom management for both health and social care professionals in order to deliver a comprehensive palliative/EoLC services. A longer education time (4 sessions or above) of generic education is suggested on the topics of communication skills and self-care if greater improvements are aimed at. Further research is necessary to understand if the attained level of perceived competence in short-term education would be sustained and translated to improved practices in the long term. Given that perceived competence is a proxy to actual practice commonly used as an outcome indicator in education research, examining the threshold of perceived competence would help educators assess their training outcomes in terms of practice.
Supplemental Material
Supplemental Material, sj-pdf-1-ajh-10.1177_10499091211038501 - Effectiveness of Educational Programs on Palliative and End-of-life Care in Promoting Perceived Competence Among Health and Social Care Professionals
Supplemental Material, sj-pdf-1-ajh-10.1177_10499091211038501 for Effectiveness of Educational Programs on Palliative and End-of-life Care in Promoting Perceived Competence Among Health and Social Care Professionals by Kelly Tsz Ching Wong, Amy Yin Man Chow and Iris Kwan Ning Chan in American Journal of Hospice and Palliative Medicine®
Footnotes
Acknowledgments
This research was supported by the Hong Kong Jockey Club Charities Trust.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research and publication of this article were supported by the Hong Kong Jockey Club Charities Trust [grant number 2019-0038-007].
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.