
Abstract
Long COVID is a debilitating and persistent illness that affects individuals in multiple and dynamic ways. Because of the significant physical, emotional, and economic impacts long COVID holds on individuals, their families, and society more broadly, it is imperative that a multi-faceted approach is taken to the long COVID research that aims to improve outcomes for those affected. Expertise about the barriers and supports to accessing appropriate, patient-centered care is best provided by those with lived experience. A Patient and Community Engagement Research (PaCER) team of student researchers, all with lived experience of long COVID, conducted a qualitative study to understand barriers and supports to a return to health for those living with long COVID. This online study was informed by Canada-wide participants all living with long COVID. Patient experience and perspective data were collected through peer-to-peer focus groups and semi-structured interviews. The team used a thematic and a thematic and narrative analysis approach to identify six themes: Challenges Within Medical Systems to Keep Pace With Novel Condition, Impact of Long COVID Condition on Mental Well-Being, Money Matters, Managing Personal Energy Capacity, Resources and Supports for Long COVID Care and Recovery, and Disregard Participants Felt Toward Their Health and Well-Being. They identified 21 subthemes. This patient-directed study yielded essential recommendations to supporting a return to health for those living with long COVID to enable them to re-engage with their previous family, social, employment, and other relational activities. In addition to demonstrating more inclusive approaches to including long COVID patients in the research that impacts them, the study results can inform more appropriate person-centered healthcare, planning, and policy for those living with, and for those who will be living with, long COVID going forward.
Keywords
Introduction
Since the beginning of the COVID pandemic in Canada in early 2020, attention has been focused on mortality, critical care, vaccines, and reviving the global economy. As time went on, it became evident that a sizeable number of those living with acute COVID-19 did not recover in the first few weeks after contracting the virus. These individuals, often referred to as “long haulers” (Callard & Perego, 2021), dealt with a collection of wide-ranging persistent symptoms and syndromes that have come to be collectively known as “long COVID” or “post-acute COVID” (Sen-Crowe et al., 2021). A unique group of these individuals subsequently activated themselves, notably through social media, Facebook and Twitter, and moved awareness and discourse about this new condition from a subjective concept to an objective reality (Roth & Gadebusch-Bondio, 2022).
The increasing number of individuals affected by long COVID, globally estimated to be over 65 million, will continue to impact workforces, academic institutions, families, and communities overall (Davis et al., 2023). In a recent study, one in nine Canadians experienced long-term COVID-19 symptoms and of these, one in three reported no change in their symptoms over time (Government of Canada, Statistics Canada, 2023). There are many quantitative studies looking into etiology and treatments of long COVID (Davis et al., 2023; De Mars et al., 2022; Sen-Crowe et al., 2021). However, until now, responses to long COVID concerns have ranged from disregard to utilizing treatment plans or frameworks for existing conditions that might share one or more symptoms that long COVID presents. As a result, many of the treatments put in place for long COVID are neither relevant nor effective in addressing the unique and individual needs of this population, and are in fact sometimes even considered harmful.
There are also concerns about the capacity of health systems to manage post-acute COVID (Sen-Crowe et al., 2021). In addition to research aimed to understand the mechanisms that cause long COVID, qualitative research is needed to understand the patient experience and perspective about the barriers and supports leading to recovery, or at best an acceptable return to health, and to identify gaps in current related resources and services for long COVID patients. This includes identifying and accessing existing and potential rehabilitation treatment options for post-acute COVID patients (long haulers), determining the timing, delivery criteria, and extent of treatment, as well as trying to understand the barriers and facilitators patients might experience to accessing rehabilitation care pathways (Wasilewski et al., 2021). There are some regional qualitative studies (Ontario COVID-19 Science Advisory Table, 2021) about the needs of those living with long COVID, but there is a discernable lack of literature about studies that meaningfully integrate patient lived-experience expertise and insight into research study design, data collection, and analysis (Fazer et al., 2021).
This qualitative study was conducted by a team of six Patient and Community Engagement Research (PaCER) students who had firsthand lived experience of long COVID or were carers for those living with long COVID. These individuals were enrolled in the PaCER certificate program offered through University of Calgary, Continuing Education (PaCER, n.d.). Over the course of 12 months, they received training in participatory health research methodology and skills, and then designed, developed, and carried out this qualitative, peer-to-peer study. They identified best practices and gaps in knowledge about what matters most to those living with long COVID in accessing diagnosis, support, and treatment for a return to health.
Objective
The objective of this study was to explore the lived experiences of those living with long COVID on their journey to return to a level of health that they experienced prior to long COVID, and to provide patient-centered evidence and a set of recommendations for healthcare systems and communities.
Methods
PaCER students are learners from all walks of life who gain training and experience to conduct patient-led, peer-to-peer qualitative research using the innovative participatory PaCER methodology outlined in Grey Matters (Marlett et al., 2014). The PaCER process of SET, COLLECT, and REFLECT ensures that the voices and perspectives of those with lived experience are meaningfully integrated at every phase of the research process from conception to completion. The SET phase engages a group of patient partners with lived experience of the specific health condition being studied to provide input and insights into designing the scope and direction of the study. In the COLLECT phase, data are collected from patient participants through peer-to-peer focus groups and individual semi-structured interviews. Collective and iterative thematic and narrative analysis is used to identify key patterns, themes, and recommendations. In the member-checking REFLECT phase, participants from COLLECT come together again to review and confirm the themes and recommendations for accuracy and intent, and to make suggestions on future research priorities and sharing of results. This project was conducted entirely online using the Zoom platform (Figure 1). PaCER process.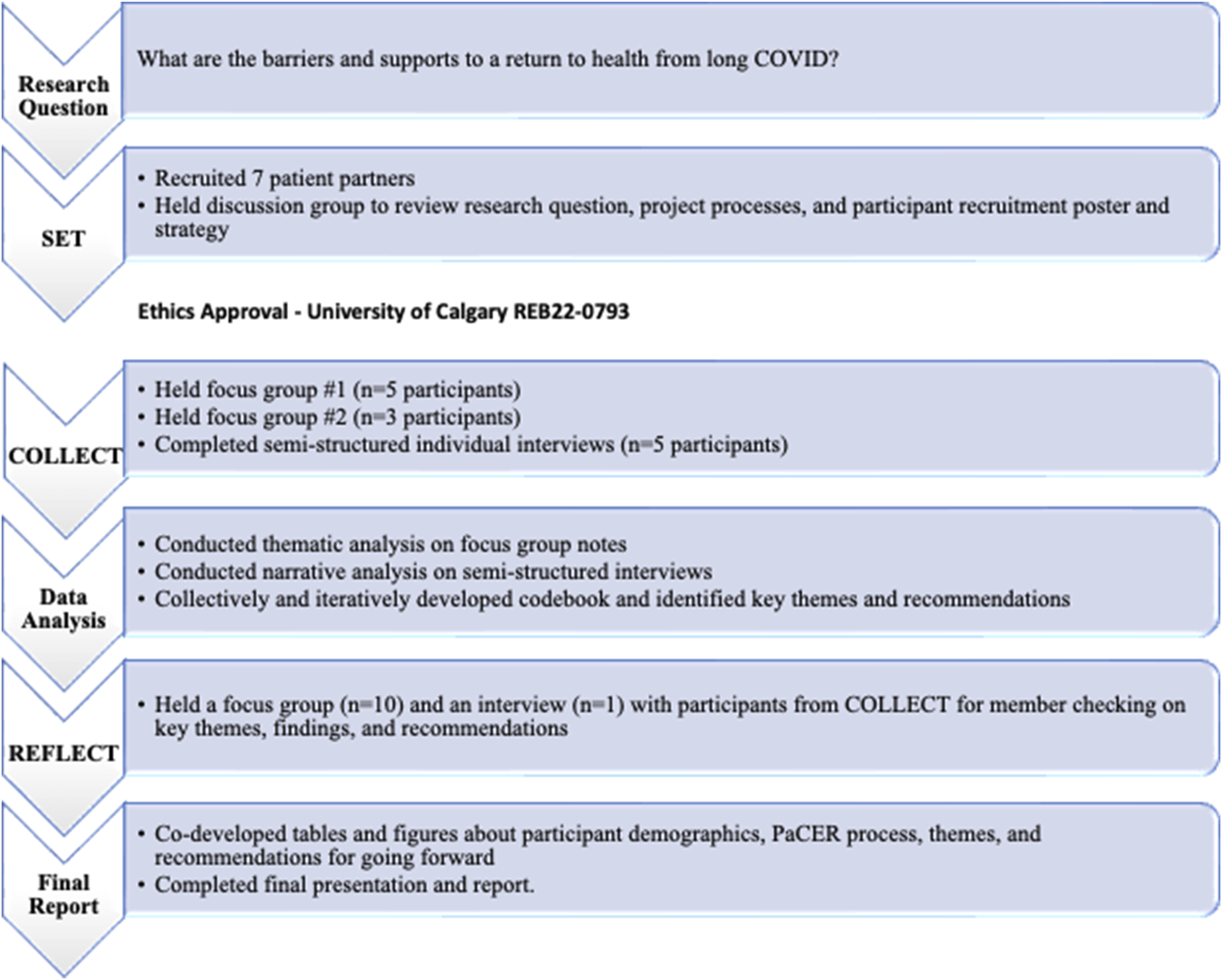
Developing the Research Question
The original research question was, “What are the barriers and facilitators to recovery after long COVID?” Through iterative discussions, the team decided to replace “facilitators” with “supports” to align better with everyday language and encourage broad interpretation. The team also decided to replace the word “recovery” with “return to health” to reflect the reality that those living with long COVID may never fully recover and return to the health that they knew before COVID-19, but many may accept a “new normal.” The research question prior to the SET discussion group was, “What are the barriers and supports to a return to health from long COVID?”
SET
The SET discussion group was held in May 2022. Patient partners were recruited primarily through team members’ social media accounts using a recruitment poster co-designed by the team. Patient partners had to be a resident of Canada; over the age of 18; and living with long COVID for more than three months (see Appendix A for SET recruitment poster). One team member was established as a central contact person to liaise with applicants. Forty people responded to the initial posting of the opportunity. The designated team member followed up with each applicant via phone or email to confirm they met the inclusion criteria; to share expectations; and to confirm availability for the scheduled date. As a result, seven patient partners attended the online SET discussion group; all were women who were living in British Columbia, Alberta, Saskatchewan, or Ontario, and two of whom identified as Indigenous or Black.
SET patient partners indicated strongly that peer-to-peer, qualitative research evidence was essential to offering access to timely care that was more responsive and appropriate to the unique and evolving circumstances of long COVID patients. They agreed with the wording of our research question but suggested some changes to the SET recruitment poster to make it more effective in recruiting COLLECT participants. Suggestions included less text and more inviting, inclusive, and long COVID–appropriate graphics. Based on this feedback, we updated the SET recruitment poster to use for COLLECT participant recruitment incorporating all suggested changes (see Appendix A for COLLECT recruitment poster).
The SET patient partners also identified important and unique challenges that some long COVID focus group and interview participants might experience, particularly about overstimulation. They made recommendations to (1) schedule focus groups and interviews earlier in the day and on weekends to lessen mental strain, (2) limit focus groups to 1.5 hours and interviews to 1 hour and offer body breaks as needed, (3) offer presentation slides in neutral colors with concise information and share these, along with the agenda and question guide in advance of the focus group and interview sessions, and (4) have all team members, except for the facilitator, turn off their video features during focus groups and interviews. These comments and suggestions were incorporated into the research protocol that was subsequently submitted to and approved by the University of Calgary, Conjoint Health Research Ethics Board (CHREB).
COLLECT
Between October and November 2022, the team held two COLLECT focus groups and conducted five semi-structured COLLECT interviews using the CHREB-approved question guides (see Appendix B). All team members attended and held unique roles in the focus groups including facilitator, Zoom host, Chat monitor, process note-taker and two note-takers. Note-takers entered detailed notes of the conversation into secure Excel spreadsheets for future analysis.
Individual semi-structured interviews were offered to participants who were uncomfortable or unable to attend the focus group sessions. Five semi-structured interviews of approximately 1 hour in length each were conducted by two team members. One team member facilitated the interview while the other took detailed notes of the conversation. Team debriefs were held after each focus group and interview for shared reflection, to discuss and confirm notes, and to review any other details.
Participant Sampling Strategy
The team was intentional to recruit participants from across Canada and with diversity of background and lived experience with long COVID. The inclusion criteria included being a Canadian resident, 18+ years of age, and having a minimum of three months lived experience of long COVID.
The COLLECT recruitment poster (see Appendix A) was shared through the Alberta Health Services Patient and Family Advisor networks, team members’ own social media networks, and the Alberta SPOR SUPPORT Unit (AbSPORU) Albertans4HealthResearch.ca network. One team member was designated as the single point of contact for interested participants. After confirming applicants met the inclusion criteria and were available for the scheduled focus group or interview dates, the team member sent eligible applicants an email containing an invitation letter, the consent procedures, and a link to an anonymous demographic survey. Verbal consent to participate was offered as an option, but all focus group participants chose to provide electronic written consent to participate. Interview participants provided verbal consent to participate at the beginning of the interviews. Focus groups and interviews were recorded for note-taking purposes only, and all participants provided consent to record the sessions. Participants were offered the opportunity to keep their video off; however, most participants kept their video on during sessions.
Using the CHREB-approved participant demographic questionnaire, an online survey was created using the University of Calgary Qualtrics platform. An anonymous link to the survey was shared with participants prior to their focus group or interview. Participants were encouraged to complete this survey. As a result, we learned that of the 13 total participants recruited, there was one each from British Columbia, Quebec, and the Yukon, three from Alberta, and five from Ontario. Eleven were female and two identified as male. Participants ranged in age from 18 to 79 years, although they were predominantly in the 30- to 69-year age range. All participants had post-secondary training or education.
All focus group and semi-structured interview participants were asked if they would be interested in being approached for further studies and if they would like to receive a copy of the final report. All were amenable to both.
Data Analysis
The team collectively and iteratively analyzed the focus group data following the six steps of reflexive data analysis described by Braun and Clarke (2022) and using an inductive exploratory approach. Anonymized, detailed notes from the focus groups and interviews were organized into separate pages in an Excel folder. Team members carefully reviewed the data from the first focus group and then began individual coding. They then met and established a “codebook” with codes and descriptions which was then applied to the remaining focus group data, including additional codes added as they emerged. Codes were then sorted, categorized, and themed using a process of discussion, defining, refining, and then describing the emerging themes. Interviews were analyzed by two members each using narrative analysis for additional context. A total of six themes and 21 subthemes emerged as well as six recommendations. These were presented back to COLLECT participants in a REFLECT focus group and interview.
REFLECT
The REFLECT focus group included 10 participants from the COLLECT focus groups and interviews, nine women and one man. In addition, a 1-hour semi-structured REFLECT interview was held for a participant (woman) who was unable to join the REFLECT focus group (see Appendix C for question guides). Overall, the participants agreed with the themed findings, but added clarity to the descriptions for the themes Money Matters, Managing Personal Energy Capacity, and Resources and Supports for Long COVID Management and Recovery, as well as made additional suggestions to the recommendations.
Results
Description of Themes and Subthemes
The six themes that emerged were Challenges Within Medical Systems to Keep Pace With Novel Condition, Impact of Long COVID Condition on Mental Well-Being, Money Matters, Managing Personal Energy Capacity, Resources and Supports for Long COVID Management and Recovery, and Disregard Participants Felt Toward Their Health and Well-Being. While individual participant experiences of the themes differed, as is indicated in the exemplar quotes, the REFLECT phase confirmed participants were in consensus with the themes and recommendations.
There were strong connections and relationships between the themes. Except for Disregard Participants Felt Toward Their Health and Well-Being, a theme represented a support to return to health for participants if they had access to or experience of the services or resources associated with the theme. If a participant was unable to access and/or receive the services or resources associated with a theme, the theme represented a barrier to return to previous health.
Theme 1: Challenges Within Medical Systems to Keep Pace With Novel Condition
This describes the barriers to appropriate care participants experienced because long COVID was novel to many health systems and healthcare providers.
Subtheme 1.1: Lack of National Long COVID Diagnostic Criteria
Positive diagnosis of long COVID was essential for referrals to additional healthcare providers, specialists, and treatments that participants felt would be helpful to managing their care and return to health. Early in the pandemic, limited access to polymerase chain reaction (PCR) testing often made it impossible for participants to obtain a COVID-19 diagnosis. As the pandemic progressed, participants with a positive antigen or PCR test and continued symptoms then experienced challenges to obtain a long COVID diagnosis.
Many participants felt their doctors preferred to conveniently attribute their emerging symptoms to existing, common diseases. Two participants shared that their doctors immediately diagnosed their long COVID symptoms as being related to menopause. Several participants struggled to have the new-to-them heart conditions that they were experiencing associated with long COVID. One participant found it frustrating that more common magnetic resonance imaging couldn’t be used to confirm that their post-COVID rapid heart rate and lung damage might be associated with their fatigue and other debilitating symptoms of long COVID. The COVID clinic here has closed, Mental Health funding has ended in Ontario … I have no pension so no money for treatments not covered by Ontario Health. Other countries are so ahead of us; the hugest hurdle is us. The government has not acknowledged this. This is all in your head. Not neurological. See a psychiatrist … get over this. This is in your head.
Subtheme 1.2: National and Regional Disparities in Long COVID Recognition and Treatment Options
Participants described disparities in long COVID recognition and treatment options within and across the provinces and territories of Canada, and between urban and rural centers. Many participants felt appropriate and coordinated care could best be offered through long COVID clinics. Optimism, including stories of positive outcomes, was shared by participants living in provinces with established long COVID clinics although ultimate experiences varied. The medical system is not working together and collaborating. We would be much further ahead if there was collaboration. Living in the arctic and north we have no supports.
Subtheme 1.3: Access to Non-Pharmacological Methods of Treatment
Almost all participants found care from nutritionists, acupressure practitioners, and osteopaths that included nutritional supplements, meditation, and yoga was beneficial. Most shared that online and community groups motivated them to learn about alternative healthcare and treatment options they wouldn’t have considered exploring before their long COVID experience. One participant however did strongly voice opposition to alternative medicine and methods and described the comfort they found in signing up for a new drug trial that was “science-based.” My doctor doesn’t want to talk about vitamins or supplements that might help or see any research, makes you feel like a second-class citizen. The good news is that when you work on this [meditation], you can gain some of it back, my cognitive has come back quite a bit.
Theme 2: Impact of Long COVID Condition on Mental Well-Being
This describes the psychological, social, and physical impacts on participants’ mental well-being that resulted from their struggle to receive long COVID diagnoses and care. This also includes the negative mental health impacts of trying to secure appropriate mental healthcare. These were often exacerbated when requests for mental healthcare were denigrated or deemed unnecessary and denied.
Subtheme 2.1: Impact of Reception to Long COVID Concerns From Those Participants Trusted
Participants struggled trying to convince medical professionals that the new onset conditions happening in their body were very unlike anything they had experienced before. Many participants voiced devastation when their concerns were met with apathy from family members, friends, and co-workers. The lack of compassion and empathy from those whom participants had hoped to receive support from added to their sense of trauma and grief. A barrier is the general population—why don’t you go for a walk. Just because we look normal. People don’t understand it’s a real thing. Mentally every time I went to see my old doctor I’d be in for a fight. I knew he would diminish me.
Subtheme 2.2: Challenges Accessing Long COVID–Appropriate Mental Health Treatment
Even when participants were offered access to mental health supports, they felt hastily made referrals to cognitive behavior therapy and other approaches were unhelpful, in fact sometimes harmful. They would have preferred treatment aimed at understanding and managing the unique circumstances that long COVID posed to their mental and physical health. This included support to process the grief they were experiencing because of their loss of health and former self which one participant referred to as disenfranchised grief. We have lost our hobbies, supports, lost ourselves. We need grief support. Loss of home and jobs, many things are gone now. Grief support. Validation of losses. Trauma and grief is critically really important. Trauma I am going through. This is going to last forever. The trauma is going to exist. I cry every single day.
Subtheme 2.3: Impact of Isolation and Not Being Able to Engage in Physical and Social Activities
The social isolation participants experienced because of physical limitations and fear of reinfection in social settings with those who were unmasked challenged their mental well-being. One participant, who was extremely physically fit and active prior to experiencing long COVID, described the socially limiting aspects of not being able to walk across a room anymore. Another participant explained how hiking and kayaking were a significant part of who she was before experiencing long COVID and described falling into a negative re-enforcement cycle because of no longer being able to engage in these activities. Isolation has affected me, when I am in a social situation, I have trouble keeping focused and have difficulty following conversations. I (active senior) was in perfect health I don’t drink; I don’t smoke, and it was like “a wall came down”! Just shocking!
Theme 3: Money Matters
This describes the financial instabilities and insecurities that resulted from living with long COVID. This also includes financial challenges to accessing time and treatments participants felt were essential to recovery.
Subtheme 3.1: Impacts of Ability to Earn or Secure a Regular Income
Long COVID symptoms and treatment plans compromised participants’ ability to continue with employment and to earn income. Income insecurity then contributed to worsening of physical symptoms and to deterioration in mental well-being and sense of self-worth. This was expressed as suicidal ideation in one participant story. One participant shared feelings of inadequacy as a husband and father because of not being able to support his family. Although he had intense feelings of guilt, he was thankful his wife was able to earn an income and cover the family expenses. Another participant, who had to live with her adult children after she was unable to continue with self-employment because of her long COVID challenges, also shared intense feelings of guilt and frustration. I have to push myself every day to go to work. I am lucky my wife is able to work. I have three children. This is at the top of my mind every day. Stress of finances.
Subtheme 3.2: Benefits to Participants of Having Income Sources Beyond Just Their Own Employment Income
Participants who did experience personal financial security from existing savings, family members, or other secondary income described this as helpful to obtaining treatment services and supports that included private mental health and alternative treatments. Three participants expressed their strong desire to access treatments offered outside of Canada, but they were unable to do so because they lacked the financial resources this would require. I tap out all the benefits I do have to improve my health and make myself feel better. I think the major support, whether it’s coming from yourself or the government, it’s money, it’s funding. It costs money for people to be sick and get better.
Subtheme 3.3: Accommodations by Employers
Employer accommodations significantly facilitated participants who were able to return to work after their COVID-19 event(s). Employer accommodations improved participants’ financial security, their sense of self-worth, and their mental well-being. Accommodations included support for working from home, reduced or flexible hours, and slight re-definitions of roles and responsibilities so participants could better manage their condition(s). One participant described being supported to continue in their work but with adapted responsibility from what they previously had.
There was angst from those without employer accommodations or even consideration. One participant described over-exerting themself to avoid the very real possibility of losing their job if their employer noticed they struggled to maintain the stamina necessary for an 8-hour shift. Another participant shared that they were trying to maintain their job without any type of leave or accommodation, but the trade-off was that they were unable to contribute meaningfully at home physically or emotionally. This made them feel like they were failing their family members, adding to their emotional stress, and compromised mental well-being. I can’t operate at that level and I am afraid to tell my employer and I am hiding this from my employer. I can’t lose what I have. Financially I can’t work full-time anymore, and I don’t have access to disability insurance. I am lucky my employer lets me set my own hours. Without that I would be destitute.
Subtheme 3.4: Challenges With Insurance Companies and Submitting Claims
Medical diagnosis and confirmation of disease is essential to submitting health and disability-related expense and employment insurance claims. National income security policies were unable to keep pace with the novel disease and dynamic trajectory of the pandemic. This made it challenging for participants to obtain income insurance that would typically be available for other medical conditions. Those who were self-employed at the time of contracting COVID-19, and subsequently long COVID, were also significantly adversely affected by this.
The Workers Compensation Board (WCB) is a national system that employers fund to ensure that workers are taken care of if they are injured at work. One participant who contracted COVID-19 on the job was able to submit a successful WCB claim and felt this was instrumental to being able to focus on her return to health. Refusals by insurance companies to acknowledge long COVID as a disability and to update submission and claim processes accordingly were significant barriers to filing claims that could support essential care and treatment. Participants felt that pandemic precarity allowed private insurance companies to unfairly deny claims and avoid paying out compensation. Government needs to step in and acknowledge this. I have coverage through WCB. Not what I make when I was working. I struggle financially; I have four kids that I like to help that I can’t. Finances is huge. Short term and long-term disabilities won’t touch them. How horrible that I can’t pay my bills. I cannot imagine. Access to coverage is important.
Theme 4: Managing Personal Energy Capacity
This describes the challenges of managing fluctuating, often depleting, physical, mental, and social energy that participants felt during their day. There was a strong relationship between Managing Personal Energy Capacity, Money Matters, Resources and Supports for Long COVID Care and Recovery, and Disregard Participants Felt Toward Their Health and Well-Being.
Subtheme 4.1: Limitations on Personal Energy
Participants expressed frustration about having daily energy levels that were significantly lower than their pre-COVID-19 selves. Participants all shared feelings of guilt for letting loved ones and others down and shared that the inconsistent and sometimes extremely low personal energy participants felt on any given day regularly made daily domestic tasks such as housecleaning, personal care, and cooking, challenging to complete. Lack of personal energy also interfered with the cognitive, relational, and emotional energy needed to sustain inter-personal and familial relationships in healthy ways. If your symptoms get worse with exertion and you need to exert yourself every day because you have to feed yourself, that is a barrier [to recovery].
Subtheme 4.2: Efficiently Managing Personal Energy Reserves
Participants spoke about the trade-offs and hacks they engaged in to effectively manage their personal energy reserves. The limits on their energy capacity meant participants felt forced to prioritize between essential self-care tasks like eating a meal or taking a shower. Participants also mentioned the loss of self-esteem when they felt forced to compromise their personal standards by not completing cooking and/or cleaning tasks as often or as well as they would have liked, and even omitting tasks important to them, like folding their laundry. They also mentioned letting go of hobbies and social engagements they no longer had the energy to participate in. In the words of one participant, this added to the “loss of previous self.” It’s like having a tank of gas and when it’s empty there is no refill. Once the gas is gone, it’s gone. I’m bedridden.
Theme 5: Resources and Supports for Long COVID Management and Recovery
Resources describes print or digital resources that detail care pathways, treatment options, and other informational help to managing care and recovery from long COVID. Participants stressed these needed to be up to date, with accurate information about long COVID from credible sources that is shared in accessible and user-friendly formats and language. Disparities in resources available across the different provinces and territories was also noted; however some provincial health services websites were cited as being helpful. Supports describes the more person-delivered supports long COVID patients might receive from family, community members, and friends. While long COVID relies on a biomedical diagnosis, the ability to access psychosocial elements of healing participants felt was closely connected to their ability to heal.
Subtheme 5.1: Social Media as a Resource and a Support
Social media was discussed as an easily accessible, online platform where participants could go to access a community of support and peer-sourced information about long COVID symptoms and treatment. While participants did suggest it was hard to verify the credibility of some social media information and sources, overall participants said they could always chat with a sympathetic, non-judgmental peer at any hour, and this was critical to feeling ok and supported. One participant did mention that they took a break from the emotional work of responding to managing social media relationships and conversations for a time because they felt they really needed to do so. Facebook long COVID groups are extremely helpful.
Subtheme 5.2: Support From Family Members and Friends
Participants expressed gratitude to spouses, family members, and friends whom they felt were instrumental to obtaining or providing healing supports that made a positive impact to their efforts to pace and heal. These included help with daily tasks such as parenting, finances, and housework. Some spoke of their spouses being their lifelines, mentally and financially.
Several participants who had been self-employed prior to COVID-19 found themselves dependent on spouses, friends, or family members to cover daily living costs. They shared the angst this caused because of feelings of being trapped with no possibility of escape. Two participants shared that their marriages dissolved because long COVID diminished their ability to reciprocate in healthy domestic partnerships and spousal relationships. Marital strife and breakdown added to their personal stress which further impeded their ability to manage symptoms.
Participants also expressed sadness about not being able to be as active as parents and grandparents. One participant relied on a friend staying with her to help with daily tasks and driving to appointments and another felt completely dependent on the support of a friend. This loss of personal independence and associated financial uncertainty manifested in severe despair and depression. Suicidal ideation also came up when a participant, who had to move in with her adult daughter to avoid homelessness, was discussing criticality of family relationships in averting homelessness. The other thing that has helped me most is my partner. He took a break from his career, and it has been amazing to have him. I have a friend staying with me to help with basic, daily tasks. I’m no longer able to be independent.
Subtheme 5.3: Value of Community Caregiving
Housekeeping tasks such as cleaning, laundry, meal prep, and cooking were aspects of daily living most participants struggled with. Several felt the lack of access to more tangible housekeeping and daily living support services was a major barrier to return to health. Only one participant mentioned having access to in-home medical care, nurse foot care. A participant who was able to financially afford a prepared meal service noted that having meal prep and clean up freed up energy to be used elsewhere. The meals that come prepared are on little plates that you nuke so all you need is a fork. Dishes are not accumulating making me depressed. That energy envelope I can now use to be online, to run to the store. If I were to need to do the cooking, the dishes would use my energy up, now I can do other things. I’m far from recovered but what recovery I have been able to do is in one of the biggest factors, it is just having social support in your life whether from your family network or other sources that allow you to do the resting that you need and actually pace.
Subtheme 5.4: Need for Specialist Services
Specialist services including alternative medicines like naturopaths, osteopaths, acupuncture, therapists, social workers, therapies, counseling, legal and administrative support, and lawyers were described as beneficial to supporting a return to health. One participant suggested that services are desperately needed to support patients with filling out the many long and difficult forms to get assistance, services, and treatments they need. I wish there was a guidebook for medical professionals to give to them. These are the first steps of what to do. Transportation is really important. I am not well enough to drive. I have a partner who works from home on his own schedule and can drive me to medical appointments. Otherwise, they would be impossible for me.
Subtheme 5.5: Value of Nature-Based Healing
Supportive and healing-focused ecological environments were often cited as essential to return to previous self and maintaining health. One participant found focusing on breathing and meditation helped because it calmed her. Participants described several times about the peace and hope they felt when being in nature, and one participant described the extreme benefits of taking off their shoes and enjoying feeling earth and grass on their feet in their garden. A participant who was considering medically assistance in dying because of feelings of extreme despair and hopelessness had life return to her face when she spoke about her two cats and the comfort, healing, and inspiration they offered to her.
Theme 6: Disregard Participants Felt Toward Their Health and Well-Being
This was the only theme experienced solely as a barrier to return to health. Disregard for participants’ circumstances and dismissiveness of long COVID as a public health threat were consistently cited as a barrier to return to health. All participants experienced stigma and dismissal from medical and mental health professionals who were inclined to attribute symptoms to other more-established conditions. Participants felt the lack of public safety measures, the politicization of COVID-19, and disinformation campaigns were driving factors behind the general disregard for the reality of COVID-19 as a debilitating illness and serious threat to general population health and healthcare.
Subtheme 6.1: Increased Likelihood of Reinfection and Threat to Personal and Family Safety
Participants expressed concern that reinfection can exacerbate symptoms of those living with long COVID or even introduce new ones. They expressed angst about the lack of mask mandates and people not wearing masks in public. Fear of becoming reinfected led to further social isolation and distancing from family, friends, and work. Participants shared experiences of loved ones accusing them of laziness or selfishness and telling them to “push through” their illness (see also Impact of Long COVID Condition on Mental Well-Being). Safety, we have not talked about the public safety and we are at acute risk. We cannot afford to get sick. A little cold can take us out. Re-infection can take us out.
Subtheme 6.2: Fears of Increases of Long COVID Cases in Healthcare Systems
Participants expressed concern about how future COVID and long COVID waves could affect healthcare and social service system’s ability to manage current and future long COVID cases. They also were saddened about being ridiculed for continuing to take precautions (i.e., wearing masks). We are headed in the wrong direction, too early to drop mandates and extreme groups are telling that masking mandates are going against their liberties and their rights.
Subtheme 6.3: Importance of Recognition by Governments
Participants felt let down by the government because of the disregard for public safety protocols, especially for those with compromised immunity. This contributed to mental angst and to a further sense of isolation. All called for publicly funded long COVID awareness campaigns to educate people about the reality and risks of long COVID. This could help to reduce stigma and to avert future long COVID cases. Participants felt this was the responsibility of provincial and federal health systems. In the Emergency Room I asked the doctor if she knows of long COVID, and she basically ignored me. Canada needs to acknowledge long COVID as a disability.
Subtheme 6.4: Ways Participants Felt Validated
The opposite of disregard is respect, and participants did make cogent the times and spaces where they felt respected and heard. One participant, whose physician attributed her long COVID symptoms to menopause, found validation after traveling a significant distance (6 hours), to participate in a long COVID university-based research study. This participant expressed that the research team actively listened to and validated everything she said and were extremely compassionate; she felt that finally someone not only believed her but also cared about her well-being. Two participants shared that they felt it was their occupational therapist who was most willing to listen and to offer help that included, in both cases, spending time researching possible treatments for long COVID for them. Another participant found their nutritionist, osteopath, and chiropractor very beneficial; however, these treatments were covered through the participant’s personal and private insurance funds. And one participant shared a positive experience of receiving timely and appropriate mental health treatment support.
The World Health Organization (WHO) recognition and definition of long COVID (WHO, 2022) was important to many participants. This offered a global understanding of symptoms and circumstances of long COVID, which they hoped would distill into the Canadian healthcare ecology. For participants who felt a lack of support and acknowledgment by their family physicians, there was hope that the WHO guidance document (WHO, September 2022) could be particularly beneficial as a reference document in doctors’ and specialists’ appointments, providing much-needed acknowledgment, and to a basis for more effective and appropriate treatment. Long COVID is a thing. Its severity and how difficult it is. General conception of not understanding and seeing this. A broken leg people can see. People do not think this is real. It’s an invisible illness. Need access to research trials. Research is slow. Experiential research trials are my hope.
Recommendations
Based on careful review and discussion of the findings, and on direct suggestions made by participants, the team developed the following four recommendations: 1. Establish universal diagnostic criteria and enhanced coordination of long COVID treatment options across national healthcare systems. Increase multidisciplinary training for all healthcare and front-line workers in this area. 2. Co-develop and offer timely, accessible, and long COVID–appropriate mental wellness care pathways and resources that include grief and loss therapy to support loss of health and previous self. 3. Offer long COVID specific income and social support programs to maintain quality and dignity of life. This can also include mandating employer accommodations for work, funding for non-pharmacological medical treatments, administrative and legal supports to access resources, counselors, and peer support groups. 4. Endorse public safety measures (including mandatory masking in healthcare areas) and provide funding to implement public awareness campaigns that share knowledge of long COVID and its impacts. This can contribute to an ethos and environment of care, empathy, respect, and dignity for those living with long COVID.
Discussion
This study aimed to explore essential insights and perspectives of a diverse group of individuals living with long COVID as they pursued a return to health. The team hoped to use the collective experience of those living with long COVID to address gaps in literature and practice. They analyzed the data from peer-to-peer, patient-led focus groups and interviews with the goal of providing patient experience evidence and recommendations that can better inform long COVID diagnosis, care, and treatment going forward.
It is important to recognize the gravity and implications that long COVID presents in the lives of those living with this debilitating condition as well as its impacts on family members, healthcare systems, and societies going forward. Although long COVID is now recognized as a multisystemic illness that presents very real and ongoing physical symptoms and issues, all participants shared challenges in accessing a long COVID diagnosis. Person-centered care is a holistic approach to care that affirms the patient and caregiver’s perspective, recognizes individuals are experts in their own health, and centers on shared decision-making (Santana et al., 2018). Participants expressed frustration in accessing appropriate and person-centered care as well as a lack of continuity and coordination of long COVID care which they all felt was the direct result of lack of recognition of long COVID as a veritable condition and associated lack of clear diagnostic criteria. This was further exacerbated by the challenges health systems experienced keeping pace with identifying, developing, and coordinating supports during the ongoing precarious and dynamic environment of the pandemic.
While compassionate, integrative, and holistic care for long COVID patients cannot cure their very real, physiological symptoms, treating them as human beings worthy of compassion and empathy and who are experiencing a traumatic change in their health status supports them in coping with that change. While all participants were eager for the development of effective treatments and ideally a cure for long COVID, they recognized this was beyond the realm of their personal healthcare professionals. Participants with unsupportive health providers found their attempts to obtain care and treatment a major stressor itself. The term “medical gaslighting” was used by multiple participants to describe the shared experience of having their symptoms invalidated and dismissed, and the research findings they shared disregarded. And while none felt their physicians knew how to effectively treat long COVID, participants who experienced healthcare providers who took their concerns seriously, validated their expertise in their own bodies, and were open to discussing information they brought to appointments experienced more positive mental health outcomes and felt hope that they could return to health. Lack of nationally recognized diagnostic criteria and frequently inconclusive or normal test results were cited by multiple participants as obstacles to an official diagnosis and access to treatment, but neither of these should be prerequisites for compassionate care.
It is important to note that the unique and variable combination of symptoms and conditions that has come to be known as long COVID was first conceptualized by patients living with this condition, and initial recognition and socialization was the result of activation by these very patients (Callard & Perego, 2021). Patients continue to be actively included in defining diagnostic criteria for post-COVID-19 conditions. The participant stories and experiences brought forth in our study confirm the trajectory of this phenomenon from lack of initial recognition to challenges with confirming diagnostic criteria and appropriate treatment options. The lack of clear diagnosis posed challenges to obtaining treatments, submitting insurance and income claims, and the overall ambivalence toward this novel, sometimes invisible, condition. In addition to confirming challenges obtaining long COVID diagnoses, participants also confirmed the lack of accessible, effective, and validated treatments for long COVID (Davis et al., 2023).
All participants shared details associated with a decline in mental health and loss related to their COVID-19 illness. The mental well-being of every participant was also impacted by their experiences seeking treatment for a disease with non-established diagnostic criterion. All had at some point felt despair about being able to recover. Participants expressed challenges in accessing timely and appropriate mental healthcare that recognized the unique challenges of long COVID and long COVID recovery in an environment that often refused to recognize the illness. Participants felt it was important to highlight that mental health services should be specific to specialists trained in loss, trauma, moral injury, and disenfranchised grief. Our findings regarding mental health align closely to the highlights found in Roth & Gadenbusch-Biodo (2022) which showed the use of standard tests to check for physiological damage is proving to be insufficiently sensitive when leading to diagnosis of normal results. This multiplies the suffering experienced by patients. In addition to concern about the national shortage of timely access to mental healthcare, participants said challenges accessing and/or receiving mental health treatment also triggered anxiety, thereby impeding recovery.
While nascent work is being done to assess, understand, and measure the impacts of stigma on long COVID patients and their return to health (Damant et al., 2023; Pantelic et al., 2022), this may be too late for the participants in our study. Lack of understanding and supportive relationships had multiple detrimental impacts on return to health. Our findings align with the gaps identified in social safety nets for those living with the novel long COVID condition (Yuko, 2022). Lack of physical or mental stamina, stigma from those who refused to believe whether COVID-19 or long COVID was a real thing, and fear of becoming reinfected all negatively impacted relationships with spouses, family, and friends, and furthered the social isolation of the participants. Many participants felt that Canada was lagging globally in long COVID recognition and felt patients in other countries had better access to long COVID care resources and care. A few participants shared they would access care globally if they had the financial and other resources to do so.
The best way to avoid long COVID is to avoid exposure to COVID-19 infection (Davis et al., 2023). COVID-19 is not like the common cold, and (re)infection raises risk of exacerbating symptoms in those who already have long COVID or even creating new ones (Nikiforuk, 2022). The fear of reinfection caused significant feelings of additional social isolation and distress. Social media offered participants a sense of community, improved experiences for those living with isolation, and helped bring a collective voice to those seeking greater understanding and health literacy about new-to-them health challenges. Although not always positive, social media platforms can offer a community of practice to advance the patient’s voice and perspective in health research, including generating awareness and socialization of novel illness and collective exploration of management and healing.
While participants found comfort and solidarity in online connection and social media platforms, the overall disregard by medical and healthcare professionals, family members, and society in general caused not only emotional isolation but also angst from more tangible aspects such as the lack of mask wearing and other safe practices. Supports participants found most helpful almost always emanated from and centered on positive affirmation of the very real and debilitating conditions they were experiencing. The WHO support for recognition of long COVID was essential to this.
The WHO describes health as “a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity” (World Health Organization, n.d., paragraph 14) and stresses the importance of social determinants of health (SDH) as important factors in achieving this state of balance. SDH can include income, working conditions and job security, food insecurity, housing and environment, social inclusion and non-discrimination, and access to affordable health services of decent quality (World Health Organization, 2019). There is alignment with these WHO-identified SDH and the themed participant experiences, perspectives, and recommendations. Considering and ultimately implementing mitigating strategies for these non-medical factors into social, economic, and health policy and practice will certainly improve the experiences and outcomes for those living with long COVID going forward.
Limitations
It is important to note that the study does not reflect the voices of those who felt they did not meet our inclusion criteria because of missed diagnosis or misdiagnosis, and those who have withdrawn from the workforce, academic studies, and society overall, and perhaps even died because of their struggles with long COVID. While the team gained many salient insights and perspectives, 13 individuals cannot hope to represent the experiences of 1.4 million Canadians living with long COVID (Government of Canada, Statistics Canada, 2022, October). Data saturation is reached when there is enough information to replicate the study when the ability to obtain additional new information has been obtained and when further coding is no longer feasible (Fusch & Ness, 2015).
While the qualitative study included 13 participants who represented multiple perspectives of background, age, geography, and lived experience of long COVID, the team feels data saturation was not reached. Eleven of the 13 participants identified as women and two identified as men. This aligns with existing evidence that long COVID is known to disproportionately affect more women than men (Bai et al., 2021). However, due to time constraints and the scope of this student project, the team was not able to have individuals from all provinces and territories. These constraints also meant that we were unable to accommodate the ethical and other challenges of including minors in the study. Children and youth represent a demographic that is consistently underrepresented across all long COVID research globally (Trapani et al., 2022). And there were additional socioeconomic and cultural perspectives that the team was unable to capture due to time and budget constraints. It is the hope that because psychosocial supports were identified as urgent and highly important to those living with long COVID, the patient-centered approaches and research priorities identified can inform future research with broader scale and scope of participant base.
Participants were motivated to join the study in the hopes of improving lives and outcomes for others who are living with, or will live with, long COVID going forward. However, some individuals cannot afford to spend their time and energy on research they are not recognized for and that they might not benefit from. While every effort was made to support inclusive approaches to data collection, some participants inquired about financial appreciation for time and essential contribution. A participant appreciation budget would help to address some financial barriers to participation so that communities often missed in the research that impacts them can be more equitably engaged.
Conclusion
In addition to the devastating impacts long COVID has on the health and well-being of individuals and their families, long COVID will continue to have significant adverse effects on healthcare systems, labor forces, and educational systems. Patient experience, knowledge, and collaboration were foundational to the recognition and conceptualization of long COVID (Callard & Perego, 2021). This study demonstrates successful peer-to-peer patient engagement research approaches and considerations for engaging those living with long COVID in the research that impacts them.
This study also highlights patient-identified gaps in care and coordination of resources and highlights evidence that can inform more person-centered (Santana et al., 2018) healthcare policy and practice going forward; care based on individual characteristics and circumstances including background, geography, and the health system(s) patients engage with.
Our participants emphasized the urgent need for timeliness. Long COVID patients continue to suffer, going unheard while existing resources are being mis- or underutilized with little emerging knowledge and evidence being appropriately shared between provincial, federal, and international healthcare systems and society more widely.
Footnotes
Acknowledgments
The long COVID PaCER team would like to acknowledge the support and guidance of Dr. Maria J. Santana, Dr. Paul Fairie, Nicole McKenzie, Ingrid Nielssen, Marcia Bruce, and the PaCER program. We acknowledge the guidance and support provided by Alberta Health Services (AHS) Neurosciences, Rehabilitation, and Vision (NRV) Strategic Clinic Network (SCN) and the Alberta Strategy for Patient-Oriented Research (SPOR) SUPPORT Unit (AbSPORU) Patient Engagement Team. We thank all the patient partners and participants for their time and essential contributions to this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Alberta SPOR SUPPORT Unit (AbSPORU), which is co-funded by the Canadian Institutes of Health Research (CIHR) Strategy for Patient-Oriented Research (SPOR), Alberta Innovates, and the University Hospital Foundation.
Patient and Public Contribution
This research was conducted by a team of student researchers in the University of Calgary’s Continuing Education Patient and Community Engagement Research (PaCER) program. This was accomplished in partnership with the Alberta Strategy for Patient-Oriented Research (SPOR) SUPPORT Unit (AbSPORU) Patient Engagement Team and the Neurosciences, Rehabilitation, and Vision Strategic Clinical Network (NRV SCN) in Alberta Health Services (AHS). All six members of the PaCER team had lived experience with long COVID, either their own or as a caregiver for someone living with long COVID. Using the PaCER process, the team collectively and iteratively developed the research question; designed and developed the study; and collaborated on data collection, analysis, and report writing.