
Abstract
Many methodological approaches have been used to understand cultural dimensions to maternal health issues. Although a well-designed quantitative survey with a representative sample can provide essential information on trends in behavior, it does not necessarily establish a contextualized understanding of the complexity in which different behaviors occur. This article addresses how contextualized data can be collected in a short time and under conditions in which participants in conflict-affected zones might not have established, or time to establish, trust with the researchers. The solution, the Participatory Ethnographic Evaluation and Research (PEER) approach, is illustrated through a study whereby South Sudanese marginalized women were trained to design research instruments, and collect and analyze qualitative data. PEER overcomes the problem that many ethnographic or participatory approaches face—the extensive time and resources required to develop trusting relationships with the community to understand the local context and the social networks they form.
Keywords
Background
There is limited published information regarding the views of hard-to-reach people in resource-limited settings and conflict-affected fragile states on the social determinants of their health. Yet, a comprehensive and common understanding of maternal health needs to be conceptualized and contextualized to meet contemporary challenges. Barriers to maternal health care will continue to pose serious problems and are difficult to define clearly, have no obvious solutions, are socially complex, and involve changing complex behaviors. It is beyond the capacity of any one organization to understand or respond to these issues. Moreover, there is often disagreement about the relevant determinants and a lack of certainty about the best way to tackle them (Elmusharaf, Byrne, & O’Donovan, 2015; Ronsmans, Campbell, McDermott, & Koblinsky, 2002; Ronsmans & Graham, 2006)
Making decisions about maternal health at the household level and about seeking appropriate health care is complex (Brown & Barrett, 2009; Parkhurst et al., 2005). Behaviors are contextualized by the complexity of social institutions and cultures that determine the health outcomes of people in each community (Brown & Barrett, 2009). Each community has its own unique context, which must be understood to address the people’s needs and to plan for accessible maternal health care services that can reduce maternal mortality rates. The approach of identifying and implementing solutions that have been handed down from outside, not rooted in the local history or culture and lacking community ownership, have repeatedly failed and, in some cases, have done more harm than good (Lush, Walt, & Ogden, 2003). This complex and sensitive research area needs a correctly framed approach that includes the perspectives of the hardest-to-reach people to provide better evidence on how decisions are made.
This article discusses an innovative methodological approach that was used to gain an in-depth understanding of maternal health issues in Renk County—an area in the Upper Nile State of South Sudan, near the international border with Sudan. The research team chose Renk county as a study area because it was accessible during the time of the research in terms of security, institutional support, and access to conduct the research.
Context
South Sudan has experienced, and continues to suffer from, repeated eruptions of war, violence, and political instability for the last five decades. The methodology presented here was used in research conducted (Elmusharaf, 2015; Elmusharaf et al., 2016) around the South Sudanese independence referendum in 2011, one of the most critical and tense times in the history of the region. After the referendum, South Sudan became an independent nation as of July 9, 2011. The magnitude of maternal health problems in South Sudan is immense, as indicated by various available indicators, mainly the maternal mortality ratio (2,037 per 100,000 live births), the infant mortality rate (102 per 1,000 live births), and the neonatal mortality rate (51 per 1,000 live births) (Sudan Household Health Survey [SHHS], 2006). Access to existing health facilities is severely limited, as indicated by the percentage of pregnant women receiving antenatal care by any qualified personnel (23%) and the percentage of deliveries attended by trained personnel (10%). Access to emergency obstetric care is low, with a caesarean section rate of 2.2% (SHHS, 2006). Furthermore, reported complication rates during labor and delivery at facilities are very high: The main complications are prolonged labor (45%), infection (49%), convulsions (20%), and excessive bleeding (42%; Faramand & Carballo, 2006; SHHS, 2006). Social determinants of health, and social rules and values in South Sudan have all been devastated by the conflict (Faramand & Carballo, 2006; Macklin, 2003). War and traditional practices have resulted in women in South Sudan having very little control over reproductive decisions, being exposed to sexually transmitted diseases, and having unwanted pregnancies (Macklin, 2003).
Conducting research in conflict-affected settings has many challenges that need to be overcome, and many ethical issues that need to be addressed. One of the main challenges that the research team anticipated was a lack of trust between the researchers, participants, and the local community. The principal researcher was from the northern part of Sudan, so conducting research in South Sudan during the referendum and the period of the independence of South Sudan in one of the border cities was expected to raise suspicion. Careful approaches were needed to build trust, to encourage the engagement of participants and communities, thereby enhancing opportunities to obtain reliable information and provide relevant and timely feedback to communities (Adejumo, 2008).
The researchers also faced competition with organizations providing services and food, while we offered to listen. To address this, there was a need to adopt a research approach that would inspire and motivate the community to be part of the research project and to build their sense of ownership of it.
Challenges were also anticipated in relation to power differences between the researchers and participants, in the sense that typically researchers are knowledgeable on the research methods and the research process, whereas the participants contribute data based on local contextual knowledge. Such a power differential can be augmented by illiteracy and lack of effective communication between researcher and non-literate participants (Meara & Schmidt, 1991). Such a power imbalance, if not addressed, could increase the potential vulnerability or participants and compromise their autonomy (Adejumo, 2008).
Method
The philosophical position in designing and conducting this study is based on an interpretivist approach, which considers the social world as constructed by people through their interactions, understandings, and ownership (Holliday, 2007). Although a well-designed quantitative survey with a representative sample can provide essential information on trends in behavior, it does not necessarily establish a contextualized understanding of the complexity in which different behaviors occur. Unless a contextualized approach is used in generating knowledge and interpreting the data, the resulting understanding of the complexity of social institutions and cultural practices involved in the demand for maternal health care can be limited.
Participatory research is often premised on being ethically and morally right by including the views of people whose lives are to be affected by an intervention or result of the research (Slim, Thomson, Bennett, & Cross, 1994). Involving participants in various stages of the research is also vitally important in identifying and prioritizing research questions, assisting in the design of the research, and identifying the best sources of information (Lehmann et al., 2004). Where the researcher has a significantly different educational and cultural background from the majority of members in the community, involving community members can assist greatly in contextualizing and interpreting the data.
Participatory research often aims for group consensus or for a collective voice to emerge (Lehmann et al., 2004; Slim et al., 1994), and thus tends to encourage generalizations, or the loudest or most senior person’s opinion predominates and neither individual voices nor minority opposition to the status quo are given the space to be aired. Thus, popular participatory approaches and methodologies have been criticized for their technical limitations, and it was realized that there was a need to re-examine these approaches to ensure that the techniques used facilitate more equitable participation rather than perpetuating the status quo (Cooke & Kothari, 2001). There has been considerable debate around the theoretical, political, and conceptual limitations of participation, such as communities being viewed as homogeneous (Guijt & Shah, 1998), or the adoption of a simplistic view of power (Kothari, 2001) and insufficient focus on the structural determinants of well-being (Cleaver, 2001; Francis, 2001). Traditional ethnographic approaches can also be used to gain a contextualized understanding, but resources required for this approach—financial, human, and time—are often not available within the time frame of most health interventions. In addition, using a participatory approach to research often raises the expectations of the participants that they will be rewarded in some way. Participants may accept not to be paid for their time and input upon their understanding that the research will result in a future favorable outcome for them, for example, job opportunities, better education, or a more efficient public sector service delivery (Byrne & Alexander, 2006).
This study used the participatory ethnographic approach known as Participatory Ethnographic Evaluation and Research (PEER) to provide a contextualized understanding of maternal health issues in South Sudan and to provide recommendations on how these can be addressed in a realistic time frame for programmatic health interventions. The PEER approach was chosen to address the scarcity of bottom-up, health system research approaches in such settings (Sheikh et al., 2011). PEER is rooted in anthropological ethnographic studies and, similar to other participatory approaches, recognizes that effective participation occurs when the voices and interests of the poor and marginalized are heard. For this to occur, ownership and trust are essential.
PEER is a participatory and qualitative research approach, based on the ethnographic method of involving ordinary members of the community to generate in-depth and contextual data (Price & Hawkins, 2002) and has been used in reproductive health research in many settings (Hawkins, Price, & Mussa, 2009; Heslop & Banda, 2013). The main aim of PEER is to gain an understanding of social life through collecting views, stories, and narratives, from different members of the social network, regarding social organization, decision-making processes, health-seeking behavior, power dynamics, and how power relations are experienced. Specifically, PEER is an approach that enables community members to design and conduct interviews and analyze data by training these community members as “PEER researchers.”
PEER fieldwork does not require the same amount of time for trust building as other anthropological approaches, because PEER researchers have already an established relationship of trust with the other community members who they are interviewing. Furthermore, data generated by this intensive exploration have the potential to yield a more in-depth understanding than other data collection methods, such as surveys (Hammel, 1990).
PEER fieldwork involved the following composition:
Principal researcher and research project team
PEER researchers: Community members trained in PEER methods by the research project team
Participant community members: Members of the community who were interviewed by PEER researchers.
Ethics, Informed Consent, and Risk Management
Ethical approval for the research was obtained from University of Medical Sciences and Technology in Khartoum, Sudan, and the Ministry of Health in Renk County. Permission and notification from Renk County official authorities was obtained before initiation of the study.
The research followed an informed consent procedure consistent with international standards and appropriate to the research context. All reasonable steps were taken to ensure that PEER researchers were informed that they could collaborate freely and without coercion. The de-briefing sessions were scheduled in advance. Due to high levels of illiteracy, verbal informed consent was obtained from the PEER researchers after the principal researcher described clearly the research and the role of the PEER researchers, the commitment involved, reasonably foreseeable risks, and expected benefits. PEER researchers were asked permission to record the de-briefing sessions. When PEER researchers denied permission, the recorder was not used. The principal researcher explained to the PEER researchers how information that may identify individuals or communities was to be managed, including the extent to which confidentiality and/or anonymity could be guaranteed. Contact details of the principal researcher were given to all PEER researchers with the information that they could contact him should they have any questions or concerns. Throughout the research process, it was emphasized that participation was voluntary, that PEER researchers had a right to withdraw at any time, and that no sanctions would be imposed for either non-participation or withdrawal.
The research project team took reasonable steps to assess and mitigate physical, social, or psychological risks to which those participating or involved in the research might be exposed. Where PEER researchers might be exposed to health-related information that may put them at personal risk, such as misleading health education, the research project team took steps to provide correct information in an accessible format. A 1-day educational session was provided to the PEER researchers at the end of the study, covering the following topics: antenatal care and its importance, pregnancy and its complications, and danger signs in labor and how to deal with them. The session was interactive, with different teaching methods used, including demonstrative models. The research project team members ensured that PEER researchers had a realistic understanding of what they could reasonably expect in terms of outcomes from the research, both for themselves and their community. The research project team ensured that all PEER researchers had the necessary support to participate as equals in the research process.
Steps Involved in PEER
A number of steps are required in the use of the PEER methodology and include the following:
Recruitment of PEER researchers,
Training of the PEER researchers,
Development of data collection instruments,
Data Collection,
De-briefing,
Insider interpretation,
Thematic data analysis.
Recruitment of PEER researchers
The main selection criteria in this study for the PEER researchers, agreed to in a consultative process with the community, were that the researchers were
from the target group, that is, women in their reproductive age (15–49 years);
married with at least two children;
able to communicate orally in Arabic or Juba Arabic;
committed and motivated and with a desire to have a voice and tell the story of their peers;
willing and available to undertake workshop training and participate in the data collection;
able to secure the permission from their family (usually their husbands) to participate, and
representative of typical local women as far as possible (e.g., not holding an official position in the village and not a leader).
Given the social context, it was accepted that some of PEER researchers would be illiterate. South Sudan has one of highest illiteracy rates among females aged 15 years and above in the world at 84% (National Bureau of Statistics [NBS], 2012).
The purpose of the PEER study was explained to representatives of a local Non-Governmental Organization, Women’s Organisation for Development and Capacity Building, the director of preventative medicine, the director of reproductive health, the director of midwifery school at the state Ministry of Health, and the vice-governor of Renk County. The criteria for recruiting PEER researchers and its justification were described to them. They then met with the leaders of 16 villages to formally nominate women to be part of this study. The involvement of the stakeholders at this stage facilitated the recruitment process, minimized the potential challenges, and increased the acceptance of the community.
We aimed to have a minimum of 12 PEER researchers. For attrition reasons (in case candidates did not attend or withdrew from the study), 16 women were initially nominated and enrolled in the research project. Two of the 16 women did not attend after the first workshop.
PEER researchers were compensated for costs associated with attending training and conducting research, such as the bus journey and their telephone calls. In addition, PEER researchers were provided with food and accommodation for the duration of the workshop. No monetary incentives were provided. Table 1 describes the background characteristics of the PEER researchers.
Background Characteristics of PEER Researchers.
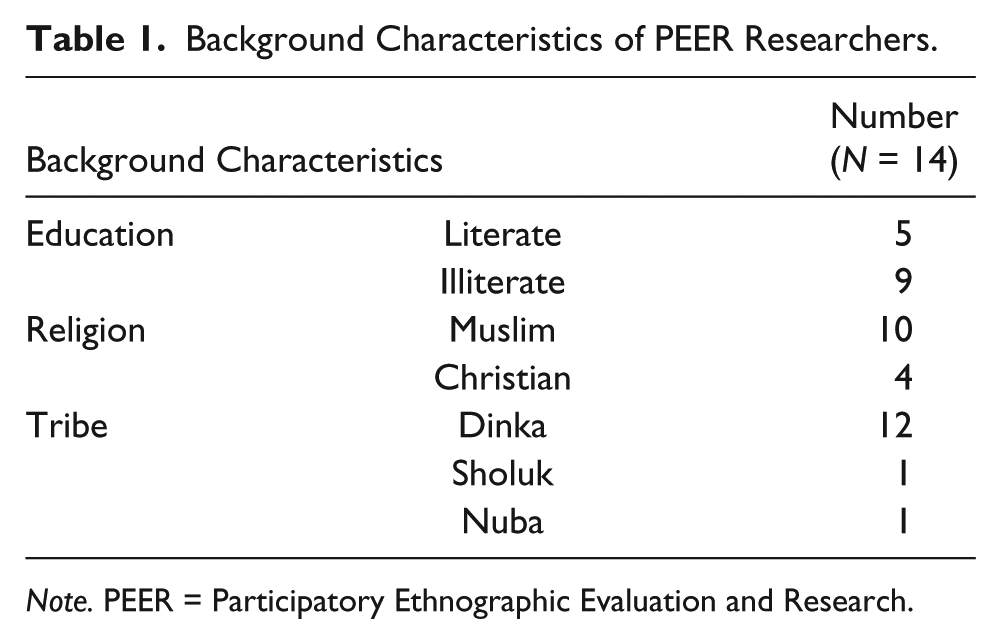
Note. PEER = Participatory Ethnographic Evaluation and Research.
Training of PEER researchers
The PEER researchers attended a 4-day participatory research training workshop during which they were introduced to the concept of the PEER approach and general research principles. The main focus of the research preparation involved discussions and identification of important maternal health issues in their communities.
The women practiced “third-person interviewing” (asking interviewees to talk about “what other people like them” do or say) and were coached in avoiding framing questions that would require interviewees to talk about themselves directly. Interviewing techniques were also practiced and included asking open-ended questions, probing, requesting stories and explaining, and gaining consent. The qualitative research capacity of the PEER researchers was developed in the training process, and at the end of the training, the PEER researchers were able to design research instruments, and collect and analyze qualitative data.
Managing expectations
The first step in the training was to manage expectations. PEER researchers were asked to introduce themselves and to describe why they were there, their understanding of the role of the workshops, and what they hoped to get from being part of this study. Any point of difference was clarified to manage expectations.
Introduction to PEER
The concept of PEER was described to the PEER researchers as a research approach that involves ordinary people from communities and people like themselves, gathering and interpreting stories to inform health policies and programs. The women were assured that no prior skills were needed, and that they would be trained in everything they would need over the 4 days. PEER researchers were informed that they would gather stories and experiences related to maternal health in the area from three of their friends. The “feedback” sessions they would have with the principal researcher after gathering the stories was then explained to them. The training emphasized that there were no right or wrong answers; that the research project team wanted people’s perceptions, opinions, and stories; and that the PEER researchers are seen as representatives of their communities.
The role in data analysis and dissemination was then described to the PEER researchers so that they were aware that the results of the research would be shared with them and that they would participate in the interpretation of those findings. They were also assured that, as part of the research dissemination plan, the findings would be shared with policy makers to influence the development of appropriate maternal health policies or interventions. PEER researchers appreciated that they would gain skills and experience that might help them in their everyday lives, that they would learn things about their community they perhaps never knew, and that they would receive certificates at the end of the study.
Getting good information from friends
The PEER researchers were taught that during the interview, they should maintain privacy and not judge the women they interviewed, and that they were to go, listen, “chit chat,” and come back and share. They were taught not to ask leading questions, not to lead their friend into the answers, and not to give answers or tell the women what to do. As noted above, they were trained on asking questions in the third person format, and how talking about other people in the community can make it easier for people to protect their privacy. Training also covered how to use prompts to explore answers given or why maintaining silence might enable the person interviewed to have time to reflect on answers given. They were trained on how to explore topics or issues more fully using the five Ws (what, where, why, when, how) and how this could be encouraged through the elicitation of stories from the participant community member rather than direct responses to questions asked. Every question in the interview guidelines contained three parts: the main question, follow-up, and the story. To ensure that the participant community members were aware of the purpose and confidentiality of the research, the PEER researchers were also taught about how to introduce the study as “a study about maternal health with no personal details,” how to seek permission, and how to arrange a good time for conducting interviews with their friends.
Demonstrating good versus bad interviews
The PEER researchers were introduced to the concept of good and bad interviews. Examples of “bad” interviews included those with no introduction; that were not prearranged; that were judgmental, leading, and/or rushed; and that involved poor listening and body language skills. On the contrary, “good” interviews were prearranged, had permission sought, involved using the third person format with no names involved, and clarified that the participant community members understood their right not to answer any question they did not want to answer.
PEER researchers brainstormed on the basis of what they were told about good interviewing. They worked in groups to draw pictures of a good interviewer and then presented their work to the other groups. This exercise also gave the women practice in using images and the role of symbols in data collection.
Development of data collection instrument
Understanding the key issues
During the workshop, PEER researchers worked together to develop an understanding of what “maternal health” meant to them and what the important maternal health issues were in their communities. Maternal health included factors that might affect family planning, pregnancy and birthing experiences, and decision making in seeking care. Based on these discussions, key themes and sub-themes for the research were identified and interview questions, which they would use to interview their friends, were developed from these themes.
In four groups, PEER researchers brainstormed about “what comes to mind when we say” daily life, family and family size, pregnancy, and childbirth. Key words that PEER researchers mentioned in each group were written down, and later, the key words were shared with other groups that had not already explored that topic, so that they could add new ideas to their list. The “findings” were presented to the whole group and discussed so that the PEER researchers could agree the most important issues and the least important ones.
In the theme of daily life, the main findings were education for themselves and their children, collecting water from the river, and responsibility for domestic tasks and child care. They stressed the importance of children “as they grow up to be useful,” and that men want a lot of children and “women don’t want many children, because it’s tiring.” In the “family and family size determinants” theme, the main finding was the need for a big family (“You can’t be by yourself, you need a big family,” and “When they grow-up children help you, if you educate them, they get a good job and support you”). In the pregnancy theme, the important topics were pain of delivery, fear of the outcome, happiness, fertility concerns, influence of past experiences (“If first pregnancy good, don’t worry about others”), and, as one participant put it, a “healthy woman means healthy child.” In the birth theme, the main topics were happiness, fear, pain (“labour is like war either life or death”), the outcome being in God’s hands (“If easy birth you don’t remember God, but if difficult they pray to God”), worry about reaching the health center in case of difficulties, young mothers at risk of difficult delivery (as girls might get married as young as 13 years), and fear of complications like swollen body, seizures, and bleeding.
Developing questions
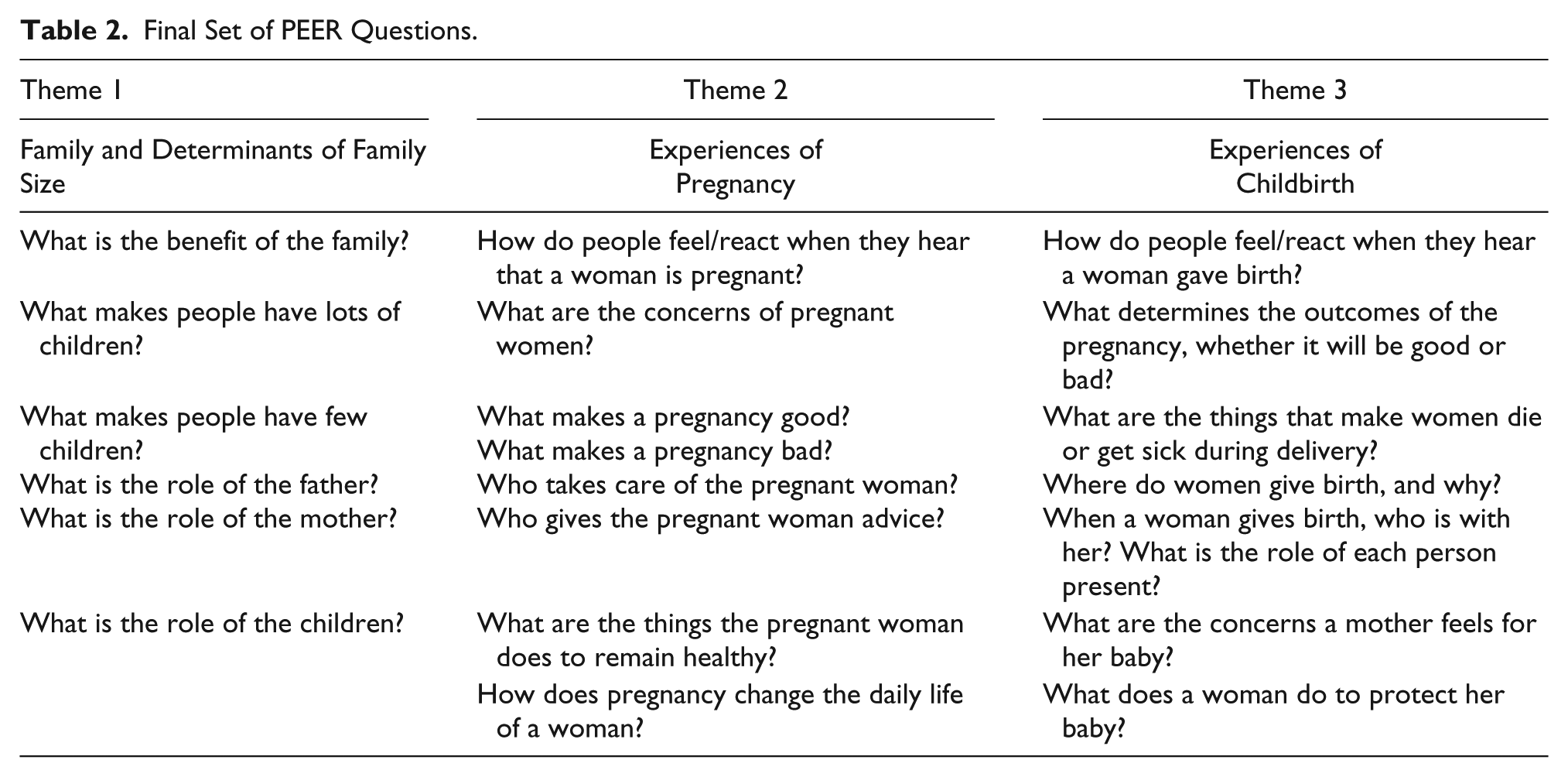
The final maternal health themes that were used as the main themes to explore with participant community members were (a) family and determinants of family size, (b) experiences of pregnancy, and (c) experiences of childbirth. The challenge then was to develop good questions to be used by the PEER researchers to ask their friends who related to the research themes. The key findings from “understanding the key issues” were presented under the three themes. The PEER researchers were asked to develop two questions for each topic while working together as a big group. After this discussion, the PEER researchers were split into three smaller groups to brainstorm each topic for 30 minutes.
The resultant set of questions for each group was shared and discussed collectively. Each question was read out, one at a time, and the PEER researchers were asked to comment on whether they thought the question was good or bad, whether it could be improved in some way, and whether it was something they could ask women in their villages. Modifications were made to the vocabulary and the order of the questions, and some questions were edited or deleted. The final set of questions is shown in Table 2.
Final Set of PEER Questions.
Developing drawings
Because most of the PEER researchers did not read and write, images were developed that would help to remind them of each of the questions. This process involved four stages: (a) drawing the questions, (b) choosing the drawings to use, (c) refining the drawings, and (d) testing the drawings.
Each PEER researcher was asked to draw an image for each of the questions as they were read out, keeping in mind that they would use those images to remember the questions later. The drawings were collected and all drawings representing a particular question were grouped together in a separate envelope. Afterward, the drawings were filtered by the research project team. Drawings that did not reflect their full intended meaning or that were very similar to other drawings were discarded. The rest of the drawings were then ranked by the research project team, and the five drawings that best reflected each question were chosen. The PEER researchers were put into three groups to finalize the drawings within each theme. Each allocated drawing was passed around the group, and the PEER researchers were asked to relate it to a question. The drawings that did not clearly reflect the question were again discarded. The remaining drawings were discussed and refined after combining ideas. The groups switched and continued the same activity using the other group’s drawings. The final drawings were tested by showing each group those drawings developed by the other groups and asking questions such as “What was the question that this picture represented?” and “Was there anything they would change to better represent the question?” In the end, the PEER researchers were brought together to agree on the final drawings. Several clear copies of the drawings were made so that the drawings could be used by each of the PEER researchers during the interviews (see Figures 1 –5).
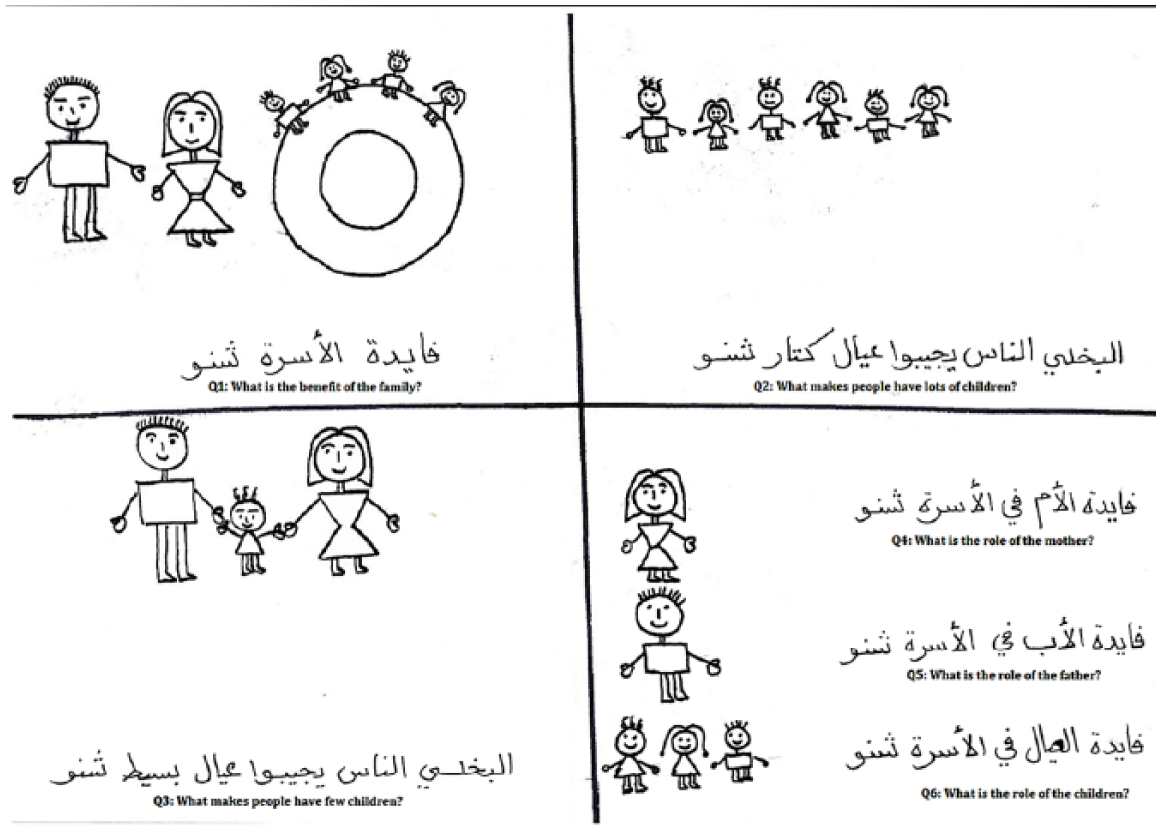
Pictograms for Q1 to Q6.
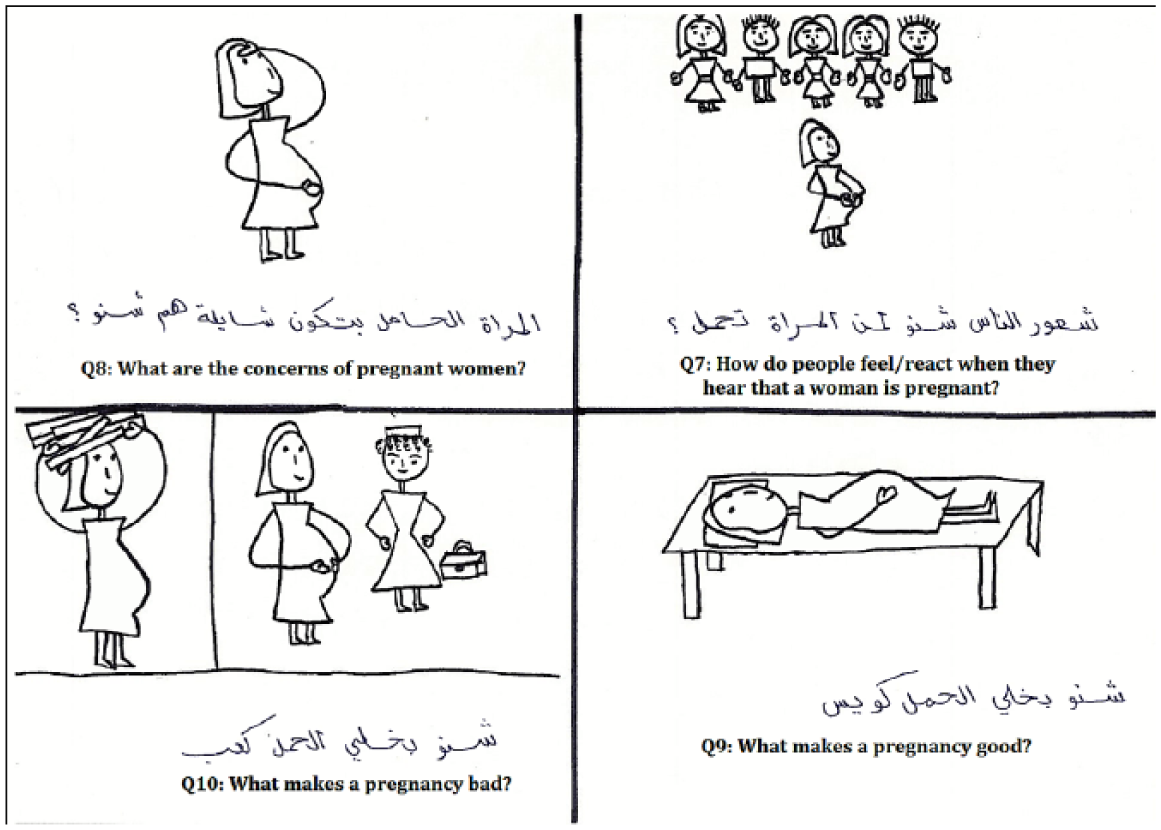
Pictograms for Q7 to Q10.
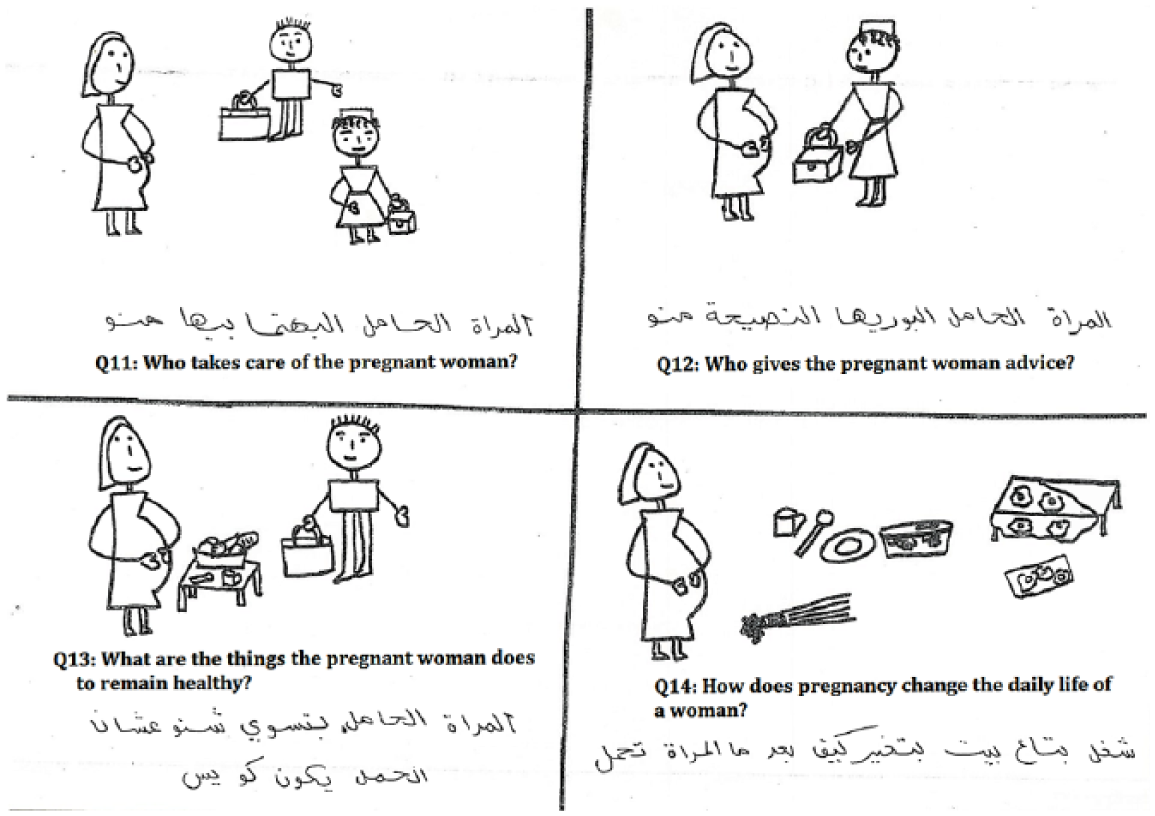
Pictograms for Q11 to Q14.
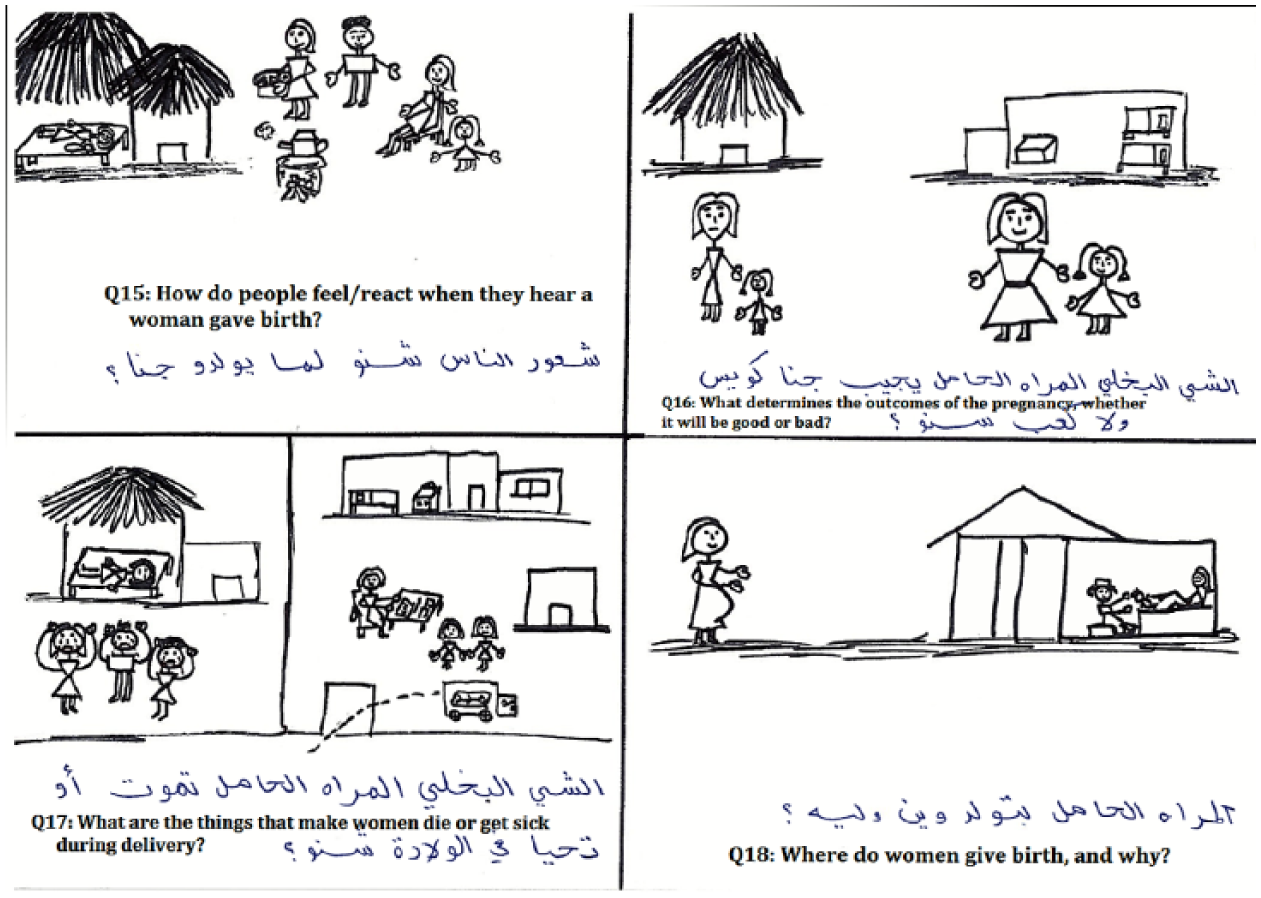
Pictograms for Q15 to Q18.
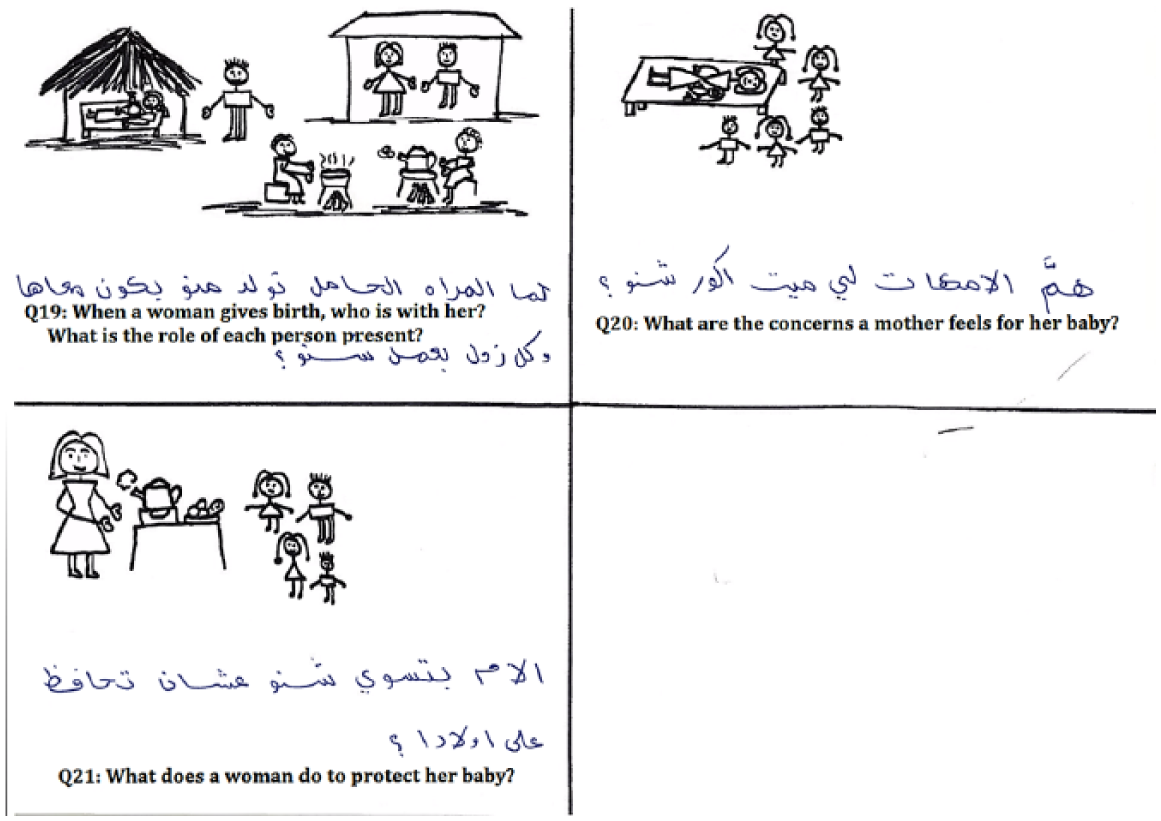
Pictograms for Q19 to Q21.
Data collection
After training, PEER researchers returned to their villages. For 6 weeks, they carried out a series of three in-depth, conversational interviews with each of three of their friends. By doing so, the 14 PEER researchers interviewed 42 participant community members. On each occasion, they interviewed their friend on one theme using the sub-theme questions, and the drawing prompts to guide the conversation. The literate PEER researchers noted down key phrases to remind themselves of the issues covered in the interviews. The illiterate PEER researchers drew pictures or sketches to help them remember stories they heard when interviewing participant community members. The approach of interviewing the same participant community member on three occasions allowed for intensive probing of each participant community member around a number of identified key themes.
The aim of the interviews was to collect narratives and stories, which provided insights into how participant community members conceptualize and give meaning to the experiences and behavior of “others” in their social network. All interviews were confidential and PEER researchers did not note down the names or addresses of participant community members or other people in their social network. Participant community members were not asked to identify who they were talking about, but were asked to simply share their experiences or stories. The third person interviewing approach allowed interviewees to conceptualize the social behavior of “others” in their networks. This approach allowed participant community members to avoid accounting for their own behavior or normative statements and thus not to make themselves vulnerable to their peers, thereby allowing differing and contradictory viewpoints to emerge (Price & Hawkins, 2002).
De-briefing
The research project team visited each PEER researcher to collect her findings in three de-briefing sessions, making detailed written notes of the narrative data that the PEER researcher had collected during that session. The de-briefing sessions were effectively one-to-one interviews. The research project team members collected data from the PEER researchers concerning what the participant community members said to them, and discussed and interpreted what participant community members said. PEER researchers were asked permission to record the interview and none of them denied permission. A total of 42 de-briefing sessions were conducted within 6 weeks.
The research project team arranged meetings with each PEER researcher, for at least 2 hours, in a place that facilitated private discussion. During the de-briefing, the first few minutes were spent having a general discussion about how their interviews went and any problems or questions they may have had. Then they were asked, “What did your first friend say about question 1?” after which they were given the chance to talk. This was followed with prompts as required. Extra questions were often added, such as, “What do you think she meant by that?” or “Why do you think that happens?”
After the de-briefing of the first theme, the PEER researcher received a copy of the next theme’s questions and drawings. After this, a time was arranged for the next de-briefing session within 2 weeks.
Emic or insider interpretation
After the data collection and de-briefing, a 1-day workshop with PEER researchers was conducted. This workshop aimed to get insiders’ interpretation of the data that the PEER researchers had collected. The PEER researchers discussed the key issues arising from their interviews and provided their own analysis of the data. The research project team then facilitated a discussion on the practical implications of the findings in relation to taking further action or developing strategies to address some of the findings. PEER researchers were encouraged to represent some of the main findings by means of telling profile stories and dramas. They were asked to sit together in three groups to develop a story, in a manner that represented the reality in their communities. Representatives of each group narrated their story in front of their fellow PEER researchers. After that, each group was asked to prepare and present a drama that reflected their findings. They role-played these dramas in the presence of all the other PEER researchers.
PEER researchers also provided feedback on their experience of being involved in the study, clarified any outstanding issues, and explored any new questions that arose during the study. The research project team checked their comprehension of the main issues raised by summarizing findings and asking further questions to clarify matters—a “forward vision session.” In recognition of the contribution to the research of the PEER researchers, the workshop included a public acknowledgment and the presentation of a certificate of participation. The main outputs of this workshop were
The identification of the most important findings on maternal health according to the PEER researchers
Profile stories illustrating the main findings
Series of dramas illustrating the main findings.
The latter two were used later by local drama and theater groups to conduct dissemination and health promotion sessions in their community.
Thematic data analysis
Further thematic data analysis was conducted across the entire content of the data in the study—the de-briefing transcriptions, the workshop findings, and outputs. The research project team used an inductive approach to ensure that the identified themes were data-driven and strongly linked to the data, without trying to fit it into a pre-existing coding frame. The entire data set was coded using NVivo from which the major themes emerged by merging, renaming, or making “parent–child” relationships, and trying to identify relationships between pairs. The principal researcher then reduced overlap between codes, sorted the remaining codes into potential themes, and organized all the relevant coded data extracts within the identified themes. How emerging themes related to each other was then further explored. Ultimately, “the defined and refined” themes and sub-themes were organized into a coherent and consistent account with an accompanying narrative. This narrative was fed back to the rest of the research team for validation and disseminated to policy makers and community members using different media, such as presentations, dance, drama, and song. Hence the themes identified, though contained in the narrative, bear little direct relation to the questions that were asked by PEER researchers. Overall, the thematic analysis followed the five phases suggested by Braun and Clarke (2006; see the supplementary file for more details).
Discussion
This article addresses how contextualized data can be collected in a short time and under conditions in which participants in conflict-affected zones might not trust external researchers. PEER overcomes the problem that many ethnographic or participatory approaches have, that is, extensive time and resources needed to develop trusting relationships with the community to understand the local context and the social networks they form. PEER is less intensive in the use of time and other resources required to understand the local context and the social networks they form. Looking for divergent stories and having 14 different PEER researchers conducting the interviews meant that the chances of hearing only voices of the most powerful or most vocal were minimized. In addition, addressing expectations from the outset and providing some benefits for participating (health education sessions and research training participation certificates) for the PEER researchers helped curtail possible misunderstandings of what was promised for participating in the research.
However, PEER can be critiqued with respect to the validation of the data in two respects:
The difficulty in verifying whether the participant community members are reporting an accurate reflection of the lives and behavior of those around them, and
The research project team is removed from the primary source of the data.
With any qualitative data, the objectively verifiable “truth” of what people say is perhaps less important than the interpretation of what they are saying and what it can reflect about people’s social values, judgments, and frames of reference. Why and how people choose to report certain stories and describe things in certain ways are as important as the purported “facts” that they are discussing. It is important to consider the entire qualitative data set. When doing the analysis, patterns building up across several data sources and exceptions to these patterns are examined—and conclusions based on these patterns, rather than any one individual’s “fact” or report, are drawn. What PEER data try to build up is an overall picture of the meanings and frames of reference that people construct and live with—and for this, analysis of discourse and narratives is much more important than the “objective facts” that people may or may not be describing.
The authors cannot completely verify with any degree of accuracy that PEER researchers recorded and retold the interviews accurately—a challenge with any “insider” interview (Mercer, 2007; Merriam et al., 2001). Another layer of removal is that the participants were referring to “others” in their responses and reflected on their own lives and experiences. To address these criticisms, two processes were included in the PEER approach: the use of de-briefing sessions and the 1-day workshop with the PEER researchers.
The de-briefing sessions were used as an opportunity for verification of the data collected by PEER researchers. The verification procedures involved (a) questions verification—verification that PEER researchers asked the questions in the agreed way—and (b) content verification—at the end of each de-briefing session, the principal researcher summarized the information and asked the PEER researcher to determine its accuracy.
The 1-day analysis workshop was used as an opportunity for validation of the data collected by PEER researchers. PEER researchers collectively validated each other’s data. They worked in groups to discuss the data they have collected. Their reflection on the data (profile stories and drama) added another layer of validation.
Additional linguistic and interpretative challenges arose, given that the data were collected in a local language in an area where literacy levels were low. In previous studies that have used PEER (Price & Hawkins, 2002), PEER researchers had to be sufficiently literate to record the interview data. However, in situations where there is high illiteracy, this requirement would have excluded the majority of people in that community as well as the more vulnerable groups. This challenge was addressed partially through the use of symbols and drawings as a way to prompt the conversation and by following up on key issues in the interviews conducted by the PEER researchers. In addition, the de-briefing was a series of sessions over a number of weeks for each PEER researcher. Each de-briefing session covered only one theme so that the PEER researchers could focus their reporting and feasibly manage the recall and retelling of the interviews. In this case, the principal researcher debriefed the PEER researchers in the Juba Arabic language. This “pidgin” language is derived from Sudanese Arabic, which people from both North Sudan (where the principal researcher comes from) and South Sudan can speak and understand (Holm, 1989).
However, compensating for some of these drawbacks is that the PEER researchers are trusted members of the community, so there is the potential for greater participatory dialogue. Furthermore, it was postulated that the existing relationships between PEER researchers and the participant community members helped gain more in-depth and insightful information than if this information were to be collected by an external researcher—an “outsider.”
For community-based research, the contextual background is necessary in the selection of representatives of the community and in the interpretation of data collected (Mosse, 1994). It was neither feasible nor appropriate to use random sampling techniques in the recruitment of the PEER researchers. However, the criteria used for recruiting the PEER researchers and the involvement of different stakeholders in the recruitment process were designed to facilitate representativeness across different community groups and villages. As noted above, one of the recruitment criteria to be a PEER researcher was that PEER researchers were women of childbearing age. The rationale for this was to build on the trust between PEER researchers and the participant community members in their social networks. It would have been culturally inappropriate for the participant community members to discuss issues related to pregnancy and childbirth with men who were unrelated to them.
The ability to participate in research is usually assumed, but there is often the need to develop this capacity (Byrne & Sahay, 2007; Jonsson, 2003). Many scholars criticize participatory action research approaches for ignoring the contextual structures in place that may leave participants vulnerable to power exploitation by the research team (Cleaver, 2001; Francis, 2001). Such approaches have also been critiqued for a lack of clear procedures and mechanisms, and inadequate understanding of power relationships (Kapoor, 2002). Capacity development is required to overcome these constraints and to tackle issues of responsibility, knowledge, and access to resources (Jonsson, 2003). Facilitating community members to share, reflect on, and evaluate their knowledge enables them to plan and act (Byrne & Alexander, 2006; Chambers, 1994).
Although developing this capacity is common in some participatory approaches (Cleaver, 2001), in this PEER research, it was important that this capacity was extended to all aspects of the research process: the design process, the fieldwork, the data analysis, and action. This is where PEER excelled: The initial steps in PEER addressed the capacity of PEER researchers to participate, enhanced their reflective practices, and engaged them in genuine dialogue. People involved in participatory research, particularly in conflict-affected settings, need to be able to reflect on the changing context as their needs and situation also change (United Nations, 2013; United Nations Development Programme [UNDP], 2010). This level of capacity development is critical because it enables individuals to bring about change not only at an individual level but also at a community level. This is further enhanced by including community members as the researchers, whose mode of communication was that of the community under investigation.
The empowerment philosophy is based on the fact that women should have the capacity to make choices (Feste & Anderson, 1995). If those who have been denied the ability to make strategic life choices are to be empowered, they need to be involved in a process that facilitates acquiring such ability (Kabeer, 1999). The involvement of women in the process of PEER provided them with a space for dialogue and reflexivity about maternal health issues in their community and made what is invisible visible to them.
Further research is needed to look at using PEER in different settings and to integrate it with other approaches such as women’s groups practicing participatory learning and action (Victora & Barros, 2013). Further research is also needed to look at how best to promote the voice of citizens in conflict-affected settings. Particular attention should be paid to research investigating how to include and activate the voices of hard-to-reach people, marginalized women, children, youth, men, and community leaders. Attention should also be paid to looking at methodological approaches that simultaneously collect data and build the capacity of local people to engage in research, and to express and exercise their views effectively. PEER is a good approach to adopt in addressing these research gaps.
Footnotes
Acknowledgements
The authors thank Beth Scott for her training contribution in the field. They acknowledge the team at Reproductive and Child Health Research Unit (RCRU) and the MSc Public and Tropical Health Program at University of Medical Sciences and Technology, Khartoum, Sudan. They extend special thanks to Prof. Mamoun Homeida, Dr. Hanan Tahir, Prof. Abdella Alkhawad, Dr. Mohamed Kardaman, Mohammed Abdalla (Molhem), Ayat Abuagla, Amal Khalil, Habab Mekki, Amjad Farah, Hiba Salih, Israa Bakhit, Israa Mustafa, Muaz Ibrahim, Mustafa Morgan, Amani Omer, Sarah Abdalla, Azza Faris, Rania Alahmer, Muhanad Hussein, Ashraf Khalid, Fawzi Victor, and Ahmed Alfadil who have contributed greatly to this project. They also acknowledge Boumkuoth Sir Mach, Mama Marina, Mama Niemat, and Chol Omak from Renk County in South Sudan for all their help and support in the field.
Author Contributions
K.E. (principal researcher) designed the study; conducted the fieldwork training, interviews, and data collection; performed the data analysis; and drafted the article. E.B. and D.O. made substantial contributions to conception and design, and data analysis, and have been involved in drafting the manuscript and revising it critically for important intellectual content. M.M. and J.H. contributed to conception and design, and have been involved in drafting the manuscript and revising it critically for important intellectual content.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded under the Programme of Strategic Cooperation, of Irish Aid and administered through the Higher Education Authority of Ireland. Funding was also received from University of Medical Sciences and Technology (UMST), Khartoum, Sudan.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.