
Abstract
Cognitive functional therapy (CFT) is a person-centered biopsychosocial physiotherapy intervention that has recently demonstrated large, durable effects in reducing pain and disability in people with chronic low back pain (CLBP). However, exploration of the treatment process from the patients’ perspectives, including the process of gaining control and agency over CLBP, is relatively understudied in this patient population. This qualitative study explored the experiences of eight participants from the RESTORE trial through longitudinally following their experiences, including interviews during baseline, mid-treatment, end-treatment, and 12-month follow-up. Data were analyzed according to a narrative approach. Findings described the overarching narrative themes of “The Journey to Self-Management.” Within this overarching narrative, four distinct narratives were identified, beginning with “Left High and Dry,” capturing the experience of isolation and abandonment with CLBP before commencing CFT, and concluding with three narratives of the experience of CFT from the start of treatment through to the 12-month follow-up. These included “Plain, Smooth Sailing,” describing a journey of relative ease and lack of obstacles; “Learning the Ropes and Gaining Sea Legs,” capturing an iterative process of learning and negotiating setbacks; and “Sailing Through Headwinds,” describing the experience of struggle to gain agency and control over CLBP through CFT. Clinicians treating individuals with CLBP can use these insights to more effectively facilitate self-management, and people living with CLBP may find resonance from the narrative themes to support their journeys.
Introduction
Chronic low back pain (CLBP) is a common condition, which continues to be the leading cause of disability globally (GBD, 2021 Low Back Pain Collaborators, 2023). The societal costs of CLBP are profound across high-, middle-, and low-income countries, largely reflecting loss of work participation and care-seeking (Fatoye, Gebrye, Mbada, et al. 2023; Fatoye, Gebrye, Ryan, et al., 2023; Gaskin & Richard, 2012; Hartvigsen et al., 2018). For the individual, CLBP reduces quality of life and is associated with significant distress and disability, described as putting lives “on hold” (Bunzli et al., 2013).
The individual multi-dimensional factors that contribute to a person developing CLBP are well documented and include psychological factors such as negative pain beliefs, pain catastrophizing, low self-efficacy, pain-related fear, depression, and anxiety; passive behavioral coping including avoidance of movement and activity; and social factors such as lower socioeconomic status (Chen et al., 2018; Hartvigsen et al., 2018; O’Sullivan et al., 2018; Puschmann et al., 2020; Ramond et al., 2011; Stevans et al., 2021). However, the pathway to recovery for a person living with CLBP is less researched or understood (Buchbinder et al., 2018, 2020; Ebadi et al., 2020; Maas et al., 2017; Rubinstein et al., 2019). Guidelines advocate for person-centered care, evidence-informed education, and coaching self-management skills, while targeting both physical and psychosocial barriers to recovery unique to the individual (Hartvigsen et al., 2018). To date, the experience of people with CLBP receiving this model of care is relatively unexplored.
Cognitive functional therapy (CFT) is a person-centered physiotherapist-led cognitive and behavioral intervention that identifies and targets individual physical, psychological, social, and lifestyle barriers to recovery in people with CLBP, in order to guide them toward self-management (O’Sullivan et al., 2018). CFT is underpinned by a flexible clinical reasoning framework and comprises the following key components: (i) making sense of pain, (ii) exposure with control, and (iii) lifestyle change (O’Sullivan et al., 2018). CFT is based on the biopsychosocial model of pain (Gatchel et al., 2007; Turk & Monarch, 2002). It integrates pain neuroscience, behavior change theory (Cane et al., 2012), and contemporary process-based approaches to pain psychotherapy (McCracken, 2023) that ideographically target factors which uniquely interact to maintain a person’s pain. The recent RESTORE clinical trial has demonstrated long-term clinical effectiveness and economic efficacy of CFT for the management of people with disabling chronic CLBP, compared with usual care (Kent et al., 2023). However, the underlying mechanisms driving these clinical improvements are not well understood (Kent et al., 2023). Improvements in self-efficacy, fear, catastrophizing, and pain control are likely mechanisms (Caneiro et al., 2017; O’Neill et al., 2020; O’Sullivan et al., 2018), although these may operate differently across presentations (Caneiro et al., 2019). While mediation analysis is one approach to understanding the mechanisms of change (Cashin et al., 2023), longitudinal qualitative research is well positioned to explore change at the individual level from the perspective of people undergoing the intervention (Audulv et al., 2022).
One previous qualitative study on CLBP participants who underwent CFT reported that people who experienced large improvements in disability after treatment described changing their pain beliefs toward a biopsychosocial perspective. Participants in this study also described achieving a sense of independence that was underpinned by improved problem solving, self-efficacy, and stress coping (Bunzli et al., 2016). However, this study involved cross-sectional retrospective interviews and called for future qualitative studies to use prospective designs to gain richer insights to how CFT unfolds and promotes change at an individual level (Bunzli et al., 2016).
In response to this knowledge gap, the present qualitative study was embedded in the RESTORE trial and prospectively followed a purposive sample of participants through their CFT treatment process at four time points over 12 months. This study adopted a narrative approach, where the primary aim was to explore the treatment process of CFT from the patients’ perspective, including the process of gaining control and agency over CLBP. The results of this study may provide clinicians and patients with practical insights into the lived experiences of undergoing CFT, including important facilitators of change across individuals.
Methods
Design
This qualitative narrative inquiry was embedded within the RESTORE trial testing treatment effectiveness and efficiency of CFT for disabling chronic CLBP (Kent et al., 2023). A full description of CFT and the RESTORE trial can be found in Kent et al. (2019, 2023). This research was approved by the research institution’s ethics office.
Narrative inquiry methodology is considered in this research as “a conceptual framework of qualitative research used to study stories, work with narrative materials, and tell stories about stories” (Riessman, 1993; Squire et al., 2014; Weiss & Johnson-Koenke, 2023, p. 390). Narrative inquiry has been described as being fundamentally underpinned by a philosophical view of experience as narratively composed (Clandinin, 2016) and offers researchers a “flexible form to explore layers of meaning within and across whole stories” (Riessman, 2008; Weiss & Johnson-Koenke, 2023, p. 390). A narrative inquiry approach was taken for this research as it was considered to provide rich descriptions of a longitudinal experience of those living with CLBP and receiving CFT, granting the participant coherence over time and nuance to the factors influencing their experiences.
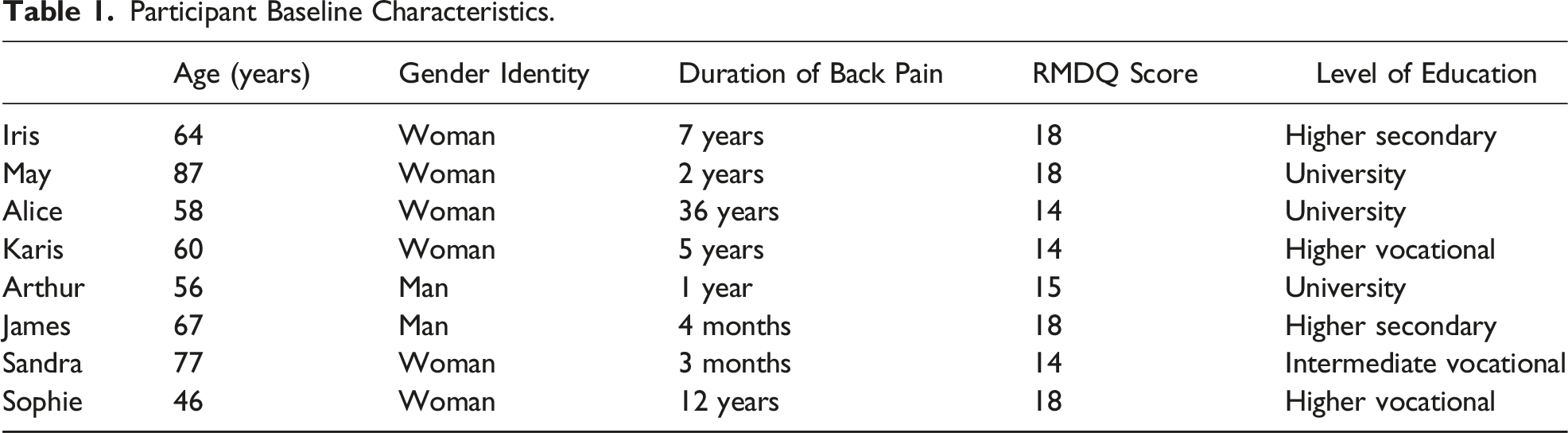
Participants
Participant Baseline Characteristics.
Interviews
Distinct from data collection approaches such as diaries or observations, interviews were chosen as the data collection approach so that rich understandings of the participants’ experiences may be gained through questioning (Zimmerman & Kim, 2017). Interviews were conducted separately to CFT treatment and took place at baseline (prior to commencement of CFT; interview 1), at week 6 (mid-way through CFT treatment; interview 2), at week 13 (end of the CFT treatment; interview 3), and at week 52 (12-month follow-up from the baseline interview; interview 4). Interviews aimed to explore the participant journey through CFT. This included exploring how participants’ understandings of, and approaches to, CLBP evolved over the course of a year that involved 3 months of CFT treatment and 9 months integrating this into ongoing self-management. This narrative design largely focused on the content of the interviews aligned with a naturalistic approach: on what was said rather than how it was said (Elliott, 2005).
Initially, interviews were conducted in person; however, phone interviews were predominantly used in follow-up interviews due to participants’ preference and COVID-19 lockdowns toward the latter half of the trial. Initial interviews were conducted between February and July 2019, with final interviews conducted between June and September 2020. During the interviews, the participants had the freedom to stop the interview at any time or refrain from answering questions at their discretion. The format for the interview was consistent across the participants and included the interviewer RS inviting the participants to share their experiences with CFT and CLBP using a semi-structured schedule (Appendix 1; Brinkmann & Kvale, 2018). A naturalist approach to the interview was adopted, whereby questions focused on the complications, actions, and evaluations elements of a narrative: “What experiences have people had?,” “What is happening?,” and “What does it mean to them?” (Elliott, 2005). RS was an active listener to these accounts but at appropriate times would seek clarification or greater elaboration, particularly related to any changes occurring in participants’ understanding or approach to their back pain. Interviews were audio recorded and transcribed verbatim. Initial interviews lasted 60 min on average, while follow-up interviews lasted 30 min on average.
Theoretical Underpinnings
The authors position the analysis within the biopsychosocial (BPS) model of human health experience (Engel, 1977), which considers the complex and highly individual interplay of biological, psychological, and social factors in a person’s experience of CLBP (Mescouto et al., 2022). Cognitive functional therapy is informed by the BPS model, facilitating clinicians to consider the weighting of each domain, which informs how treatment should be delivered to the individual. Approaching CLBP under this framework has been a radical shift from a traditionally biomedical approach to pain, which now considers the individual as a whole as distinct from their pain or injury. This “whole person” approach positions the authors consider the multi-dimensional experiences of CLBP and how this is influenced by CFT. This system of ideas is aligned with a constructionist paradigm, composed of ontological critical realism and epistemological subjectivism (Levers, 2013). Meaning is created through interaction of the interpreter and the interpreted (Crotty, 2020), necessarily shaped through interpretation, the phenomena (CFT for CLBP), and social influences (Levers, 2013).
Researcher’s Positionality
Although this design reflected the primary interest in the stories the participants told about their experiences of CFT and CLBP, the researchers were sensitive to the way meaning was constructed as part of the interview interaction and subsequent analysis (Elliott, 2005). The interviewer RS is a man, a clinical psychologist who specializes in the area of persisting pain conditions, and an experienced qualitative researcher. RS has extensive experience working with the population sampled (people with disabling chronic CLBP) and conducting interdisciplinary care with physiotherapists under a CFT treatment approach. Data analysis was led by NRK, a woman, an experienced qualitative researcher, and a clinical physiotherapist. NRK is not trained in CFT. Two other research team members, POS (man) and AS (woman) who were involved in the study design and data analysis, are research professors and physiotherapists who have developed and researched CFT over several decades. Both researchers have experience in qualitative approaches, and POS works clinically as a specialist physiotherapist using the CFT approach. All authors with the exception of NRK were on the RESTORE trial.
Analysis
The analytic process adopted in this study was aligned with a narrative thematic analysis, which provides a method for exploring themes within the content of what was told (Riessman, 2008). This approach is concerned with patterns and themes within the narrative rather than form and use of language (Riessman, 2008). Under this approach, analysis focuses on “what” was said, aiming to thematically categorize participants’ experiences of CLBP and CFT (Riessman, 2008). Analysis began with familiarization where each block of four interviews for each participant was listened to several times by NRK while simultaneously editing transcripts for verbatim accuracy transcribed from an external source. During this time, NRK made initial notes and memos regarding the key ideas from the data, focusing on “big picture” concepts, such as “what is happening here?,” “what are the mechanisms influencing this person’s experience?,” and “how is this person making sense of their experience?.”
Following this, the 3-D narrative framework was used to assist NRK to holistically consider elements of a participant’s experience. The 3-D narrative framework also positioned the authors to organize and capture the impact of temporality and change over time. This analytic framework is also aligned with the theoretical underpinnings of the BPS model, facilitating the analysis to consider the multifactorial contributors to the experience of CLBP while keeping the participant narratives intact. The framework consists of three key elements: interaction, continuity, and situation/place. Interaction consists of the “personal” that ask the researcher to consider the feelings, hopes, reactions, and desires of the participants and the “social,” which is linked to external conditions, the environment, surrounding factors, and people from the participant’s context. Continuity considers the “past,” “present,” and “future,” which prompts the researcher to analyze the transcript for past experiences of the storyteller, in addition to present experiences and actions that may occur in the future. Lastly, situation/place seeks specific situations in the storyteller’s landscape, which may be physical or the overarching context. The 3-D framework was completed across each transcript for each participant (Appendix 2: example of the 3-D template for Arthur) which created a scaffolding to reconstruct narrative stories considering the important elements of interaction, continuity, and situation/place. The process of reconstruction was used as means to narratively organize the participants’ longitudinal data and focus on the key elements of their experience prior to development of themes.
Development of themes began by focusing on the key elements of each person’s narrative at each time point. This analytic stage consisted of a horizontal analysis (e.g., all baseline narratives were horizontally analyzed), whereby common thematic categories were sought. These analyses were then amalgamated seeking common narrative threads across the participants for each time point, considering convergences and divergences in each participant’s stories. Thematic analysis was iterative in nature, whereby NRK would move back and forth between the individual narratives, raw data, 3-D analysis, and construction of the narrative findings. During this process, metaphors were generated to aid in the crystallization and understanding of narrative themes. The analysis adopted a conceptual perspective on metaphor use, whereby the metaphorical sentence carries meaning beyond its linguistic composition (Aita et al., 2003). Lakoff (1993) describes the use of metaphor in this way as a process of mapping, where we impose one concept or idea (the metaphor) on another (the experiences of participants in CFT). The intention behind Lakoff’s concept of mapping is to understand ideas spatially and describe the relationship between ideas where a metaphor provides an efficient means of capturing complex information and crystalizing it into a meaningful set of concepts.
For the present study, a maritime metaphor became appropriate to capture the varying narrative themes of the participants. The notion of how sailors must negotiate the different conditions of the ocean toward their destination resonated with how the participants held hope to work toward recovery and self-management; through the process of CFT, participants learned to ride the waves of setbacks, challenges, and victories that came with living with CLBP, where some participants experienced more success with this process than others.
Regular team meetings and feedback were conducted during the analytic process to ensure the metaphorical narrative themes reflected the experiences of the participants and highlighted the key stories from the participant data. Despite theoretical knowledge of the key mechanisms of CFT, the research team remained reflexive in their approach to the analysis to ensure the narratives were told from the perspectives of the participants rather than deductively according to a CFT framework.
Results
Narrative Theme Summary.
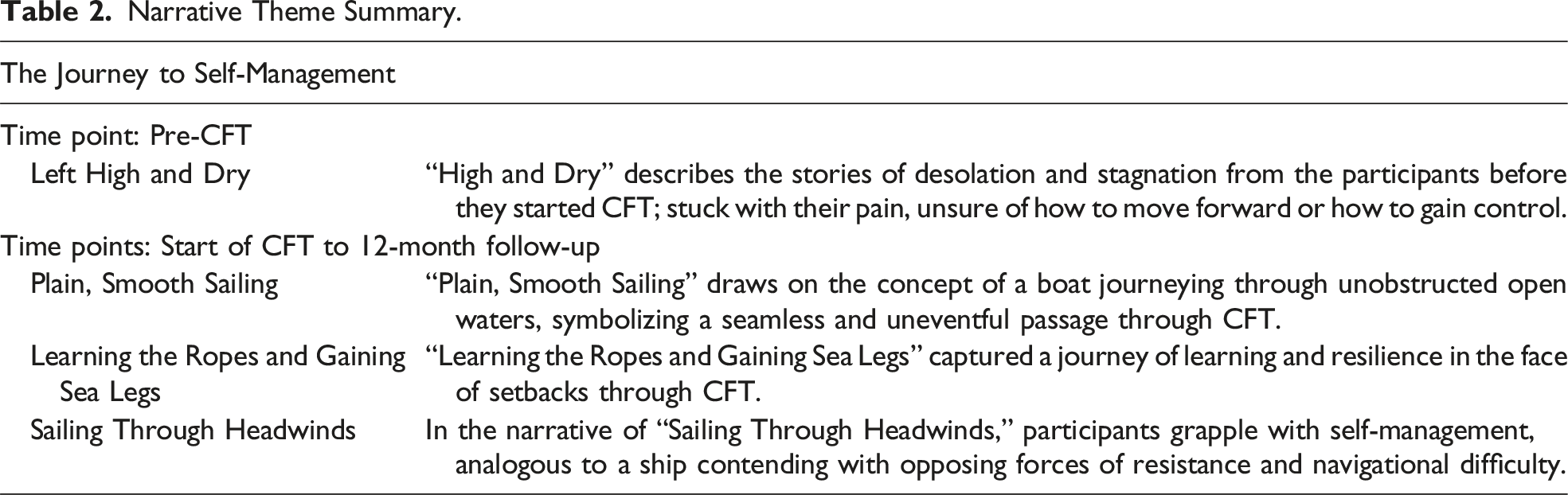
Left High and Dry
“Left High and Dry” describes a boat being beached and stuck on dry sand, stranded by the sea and without resources or help. This metaphor resonated with the stories of desolation and stagnation across all the participants before they started CFT: stuck with their pain, unsure of how to move forward or how to gain control. Participants reported experiencing multiple failed medical interventions, stuck with what to do next, and scared about their future and what their structure-based diagnoses meant. As James described, fear from pain flares and diagnoses could be overwhelming: “Scary…I was concerned that if I didn’t watch what I was doing, it could damage the spinal cord or some of these sorts of things.” The fear meant participants’ only way to cope was to reduce the size of their worlds—do less and avoid more. Participants described avoiding movements or activities and relying on medicine for even the smallest amount of relief. This resulted in being unable to live their lives and losing their sense of self. For example, Alice described feeling “slightly less of a person” and as though life was passing her by, “living but not living your life—it’s like being in a shell. Protecting.” Like a vessel being stranded by the sea, many participants reported being left with no options by health professionals, either through failed interventions or through being dismissed. Karis described how she was left with no options other than to do the best she could to live with her pain: There is nothing that—apart from a fusion. But because there are so many discs involved, it’s just gonna put pressure on the next ones and then I’d have to have them fused. So, I’m not in a point where I really have a choice of having surgery or anything like that. I have to manage this and do the best that I can.
Despite the challenges the participants faced, they held on to hope that a solution would arrive, or as Sandra put it, “a pot of gold at the end of the rainbow.”
Plain, Smooth Sailing
The narrative theme of “Plain, Smooth Sailing” draws on the concept of a boat journeying through unobstructed open waters, symbolizing a seamless and uneventful passage. This metaphor encapsulates the trajectory of Arthur, who adeptly applied the learnings from CFT, navigating toward self-management with apparent ease, unburdened by challenging events or uncertainties. Arthur described a harmonious integration of CFT principles, facilitating an unhindered progression. His narrative reflects an absence of the obstacles that often punctuate the navigation of self-management, portraying a journey unmarred by the destabilizing waves of adversity. This journey resulted in reduced threat of low back pain, amplified confidence, and a renewed engagement with activities.
In the early stages of CFT, Arthur quickly learned the presence of bulging discs on his scan was normal and the way he was moving was a larger contributor to his pain. With the acquisition of this knowledge challenging previously held beliefs about needing to protect his spine and avoid bending movements, he was able to learn to relax his body and return to loading and movement of his back in all directions. This ultimately resulted in a reduction in pain and improved movement for Arthur: There might be a bulge there, but you know, I realised that, that anybody can have bulging disc like that without pain, but it’s more the, the tensed back … It’s keeping the back straight like that is, is part of that pain. And then look, part of that was also the tight back. So, um, I’m really bending now.
As his CFT journey progressed, there was a loss of CLBP identity and a realignment with an “old” sense of self—returning to kite surfing and traveling with his son’s rugby team overseas. By the 12-month follow-up, Arthur said, “There is nothing wrong with my back,” and his larger focus was on maintaining a healthy lifestyle by keeping fit and strong and losing weight.
Learning the Ropes and Gaining Sea Legs
In the narrative theme of “Learning the Ropes and Gaining Sea Legs,” participants embarked on a journey toward self-management, characterized by a continual process of learning and resilience in the face of setbacks. Drawing a parallel to novice sailors, individuals in this phase grappled with the intricacies of mastering the fundamentals of sailing: skillfully tying knots and deftly manipulating ropes to harness the optimal force of the wind. As they navigated unpredictable waters, they found themselves adjusting to a new way of living, cultivating a sense of mastery and adaptability. Five distinct voices resonated within this narrative, those of Iris, Alice, Karis, Sandra, and Sophie. Through their unique experiences, this narrative finding captures their paths to gaining agency and control over the challenges posed by CLBP through CFT.
For Karis and Alice, this included a pulling and pushing between a biopsychosocial and structural understanding of their pain. On one hand, they found safety and control in learning to relax their bodies, moving away from protective breath holding and bracing behaviors, but on the other hand, these structure-based beliefs of pain persisted. Karis described how the new movements have been helpful, but she remains cautious of her fragile spine: “One day I might just move the wrong way and then it is gonna mean I have a fusion, but until then I just gotta get on with it.” While others who were “Learning the Ropes and Gaining Sea Legs” were more able to integrate biopsychosocial understandings of their pain, they still required repeated practice of the link between their bodies and pain, including recognizing when they were falling into old patterns and behaviors, as Iris explained: “No more holding my stomach and trying to sit upright. I’ve gotta slouch more to be able to relieve the pain … it’s been a challenge and I’ve got to keep reminding myself.”
With continued integration and practice, participants’ beliefs about pain and understanding of the link between their bodies and pain became easier. At the 12-month follow-up, Iris explained how she had a deep understanding of the link between her body and pain, with skills to control and reduce her experience of pain should it come on: “Instant feedback. I know exactly. If I’m sitting in the car and I’m sort of tensed up, the minute I relax it [the pain], it eases.” Similarly, Karis described her new knowledge about her spine as not being easily damaged: “I don’t need to treatment myself like this fragile piece of glass anymore.”
Being exposed to and supported through feared movements with their physiotherapist was also an important part of the participants’ journeys to self-management. Success with these movements reduced the threat of their pain and supported agency and confidence for those “Learning the Ropes and Gaining Sea Legs.” Iris described how mastering a feared movement impacted her: I think it’s very important to be able to be shown that if you do something that you maybe are a little bit scared of doing, and you do it, and it’s fine. You are obviously going to feel much more confident in doing it in the future.
Much like a novice sailor needing someone to teach them new skills and support them in a new environment, so was the participants’ relationship with their physiotherapist during their journeys. This relationship was built on taking time with the participants, listening to their stories, and building trust to embark on the journey together. This was especially important for Sophie when she attempted a movement she was fearful of: If he turned around and said, oh look, try this, I’d be like, well, I can try it, but I don’t know what that’s gonna do. So, I would’ve probably reacted differently to him, but because he was so accommodating of my thoughts, and acknowledged all those thoughts, and then gave me the skills I was like, well, alright. I can try that because you’ve tried to help me.
Part of this learning process included the navigation of pain flares: like novice sailors needing a map and plan for embarking on a journey, including how to make it through challenging conditions, so did the participants. With the support of their physiotherapist, mastery of flares meant they gained confidence in their ability to control these events and their overall control of their pain. Sophie explained her use of basic strategies to successfully ride the wave of a pain flare at the end of the treatment period: I was like, can you work through this? Do you need support for this? And I was like, well, do you know what, no … You can get through it, is how I was thinking about things, and I just went back to basics, and I’ve done a couple of the exercises that [physio] gave me … picking a pen off the floor to try and stretch your back out, sitting in the chair the proper way … I took it right back to basics.
By the final 12-month follow-up, participants who had a narrative of “Learning the Ropes and Gaining Sea Legs” had progressed to competence over the skills learnt through CFT. Though they still experienced low back pain, they weren’t limited by their pain through having the skills and knowledge to control their pain. Participants were returning to activities they enjoyed and prioritizing healthy habits. Iris described her future as “looking pretty bright.”
Sailing Through Headwinds
In the narrative of “Sailing Through Headwinds,” participants grappled with an arduous journey to self-management, analogous to a ship contending with opposing forces of resistance and navigational difficulty. Much like headwinds impede a ship’s forward movement, factors such as a lack of resonance with their understanding of pain, unsuccessful attempts to control flares, and struggles with self-efficacy act as formidable “headwinds,” creating resistance and impediment in the journey toward pain control and self-management.
This narrative unfolds through the lived experiences of two contributors, James and May, who illustrated the struggles inherent in navigating these metaphorical headwinds. Their uncertainty with the drivers of their pain, coupled with a deficiency in confidence and skills to manage flares, compounded the resistance, creating a headwind to the attainment of self-management for their CLBP. Both participants found themselves ensnared in persistent headwinds, struggling to “tack” or maneuver toward and through the wind, to assert control over their CLBP.
During CFT, May grappled with integrating her exercises into her daily routine. While she reported understanding the reasons behind her exercises, she didn’t put her learnings into practice, what she described as “not being completely in the driver’s seat.” May described various headwinds to feeling in control, including pain in multiple areas of her body and her medications making her sleepy. Although May said her medication use had reduced during CFT, she still took them to feel able to attempt her exercises, what she called a “bit of a vicious circle.”
The most significant headwind for James was having a pain flare out of the blue during the treatment period, which he described as leaving him feeling as though he hadn’t improved and stuck with how to move forward: Up until then I’d been sort of fairly, fairly positive. Cause although I was having sort of problems off and on, they weren’t severe problems. And, so I’m thinking, that we’re actually making progress. But what happened then, this last flare up was as bad as it’s ever been, it’s like all previous work was just hadn’t achieved anything.
This pain flare caused a significant blow to James’ confidence in managing his pain, leaving him uncertain about how this physiotherapy approach could help him move forward.
Despite low confidence and agency over their pain management, both May and James had cognitively shifted toward an understanding of their pain that was not related to significant structural problems: James was satisfied with the understanding that his pain was more muscular than something wrong with his spine, and Joy now understood that exercise was the best way to manage arthritis rather than medication alone. Due to this, the threat of their pain was reduced, but the presence and unpredictability of it presented resistance to re-engaging with movement and activity.
By 12-month follow-up, May described feeling better equipped to know what to do about her back pain but still grappled with putting her learnings into practice. To address this, she decided to continue her engagement with a home-visit physiotherapist to do exercises with her twice a week. Though her pain persisted, the knowledge that someone was there to support her gave her comfort and her ability to cope with pain had improved. Similarly, James continued to struggle with his back pain and acknowledged he had not been doing his exercises. James did not understand how the exercises were addressing his back problem, nor could he make sense of the reasons why his pain persisted, which he described as being “beyond my understanding these days.” With the knowledge he gained through his learnings in CFT of spines being strong and resilient, he described being more comfortable attempting valued activities, though still slightly apprehensive, able to “muddle through” pain flares knowing he would not cause permanent damage.
Discussion
The aim of this study was to explore the experiences of people undergoing CFT within the RESTORE trial (Kent et al., 2023), including the process of gaining control and agency over CLBP. To achieve this, we conducted the first prospective longitudinal qualitative study of CFT for CLBP using a narrative inquiry approach. Analysis resulted in an overarching narrative theme of “The Journey to Self-Management.” Within this overarching narrative theme, four distinct narrative themes were identified, beginning with “Left High and Dry,” capturing the experience of isolation and abandonment with CLBP before commencing CFT, and concluding with three narrative themes portraying the different trajectories of CFT from the start of treatment through to the 12-month follow-up. These included “Plain, Smooth Sailing,” describing a journey of ease and lack of obstacles; “Learning the Ropes and Gaining Sea Legs,” capturing an iterative process of learning and negotiating setbacks; and “Sailing Through Headwinds,” describing the experience of struggle to gain agency and control over CLBP through CFT.
Illustrating the prevailing biomedical view of CLBP, “Left High and Dry” described how prior to the CFT intervention, participants’ pain was approached through the lens of attempts to “fix” painful structures, which did not support participants to re-engage meaningfully in their lives. Instead, pain impacted all parts of their functioning, resulting in their world becoming smaller and smaller. Reflecting this biomedical approach to CLBP, participants described a structural understanding of their pain informed by negative imaging findings and advice from clinicians, while undergoing various passive and failed management approaches. Participants discussed fear and uncertainty about their pain resulting in avoidance and protection, leaving them feeling stuck and scared without a clear direction for treatment. These findings are consistent with the broader, and extensive, qualitative literature exploring the lived experiences of people with CLBP (Bunzli et al., 2013; Froud et al., 2014), including a previous qualitative synthesis where CLBP was conceptualized as suspended “wellness,” “self,” and “future” (Bunzli et al., 2013).
The primary aim of CFT is to coach people with CLBP to self-manage their condition by addressing their individual biopsychosocial barriers to recovery (O’Sullivan et al., 2018). Understanding the mechanisms through which people can achieve self-management of CLBP through CFT may have important implications for care in this patient population. The present study offers the first prospective qualitative inquiry during the CFT treatment process, described through three distinct narrative themes that capture different journeys toward self-management. The findings of this study have some alignment with previous qualitative research on CFT for low back pain where participants respond in different trajectories. Bunzli et al. (2016) described a group that was unchanged, a group of small improvers, and a group of large improvers from CFT. The present study also found different response journeys; however, the longitudinal nature of this study granted insight to the potential mechanisms supporting a process to self-management of CLBP.
One theoretical model to interpret these different journeys is self-determination theory, which articulates the processes through which a person acquires motivation for the initiation and maintenance of health behaviors (Ryan & Deci, 2000). Self-determination theory presents a continuum from externally regulated motivation (least autonomous) to intrinsically determined motivation (autonomous; Ryan & Deci, 2000). The theory assumes that the more autonomously motivated an individual is, the more likely they are to adopt behaviors resulting in more positive well-being (Ryan & Deci, 2000). Autonomous motivation is considered to be dependent on three key psychological needs: competence (feeling capable and developing mastery), autonomy (feeling in control of one’s actions), and relatedness (feeling connected to and valued by others; Ryan & Deci, 2000).
Potential mechanisms supporting autonomous motivation illustrated by the narrative themes included participants making sense of their pain through understanding the relationship between their body and pain. Participants expressed this as an increased awareness of the tension they held in their bodies and/or unhelpful movement behaviors they had adopted, which may have facilitated the psychological need for autonomy over their pain. They described the importance of being guided toward breathing, relaxing, moving, and exercising for pain relief and learning that pain is rarely an accurate measure of tissue damage (Kasch et al., 2022). Supporting this and facilitating the psychological need for competence were successful experiences during guided exposure to provocative, feared, and previously avoided movements. The mechanisms underpinning guided exposure are likely related to facilitating the learning of new safety memories that compete with old fear memories through inhibitory learning strategies (Craske et al., 2012; Sotres-Bayon et al., 2006; Wallwork et al., 2016), which functions as “exposure with control” within CFT (O’Sullivan et al., 2018). These findings are consistent with previous mixed-methods research exploring changes in movement patterns after CFT treatment, whereby participants were guided to adopt a “conscious non-protection” approach to movements and activities, resulting in shedding of damage beliefs and more positive emotional responses to their pain (Wernli et al., 2022).
Interestingly, participants in this study were able to develop autonomous motivation despite an ongoing tension between new biopsychosocial and old biomedical pain beliefs and behaviors during treatment, primarily demonstrated by participants in the narrative theme “Learning the Ropes and Gaining Sea Legs.” Despite mixed beliefs, most participants still described improvements in pain and disability, suggesting behavior change can occur independent of a complete pain reconceptualization, aligning with previous research on CFT for people with knee osteoarthritis, where participants simultaneously held beliefs about tissue pathology while managing pain through movement and exercise (Caneiro et al., 2024). These findings may underscore the importance of the experiential element of CFT in supporting developing competence, mastery, and behavior change. This interpretation is further supported by the narrative theme of participants in “Sailing Through Headwinds” who indicated they no longer considered their pain dangerous but did not describe consistent successful experiences of pain control or returning to valued activities. These narrative themes may collectively explain why previous research exploring pain neuroscience education alone has demonstrated limited efficacy for reducing pain and disability (Shin & Kim, 2023; Watson et al., 2019, 2021).
Further potential mechanisms related to gaining autonomous motivation within the narrative themes were the role of pain flare-ups during the treatment period. While James’ experience resulted in a loss of confidence and doubt about managing his back pain, Karis and Sophie described gaining confidence and feeling more in control as a result of having the skills to get through the flare. These findings highlight how pain flares are an important learning opportunity that may either facilitate or hinder the psychological needs for competence and autonomy in the development of autonomous motivation. Previous qualitative research on the impact of pain flares for people with low back pain described the highly distressing and disabling nature of a flare for this patient population, including a strong link between low mood and psychological changes (Tan et al., 2019). This may suggest the need for additional clinical support for patients during flares that may be beyond what is described in the RESTORE trial to support people with CLBP in learning to negotiate these fluctuations in symptoms.
A final component of self-determination theory is the role of relatedness in supporting autonomous motivation and subsequent positive behavior change. The narrative themes suggest that potentially underpinning the effectiveness of gaining body awareness, mastering feared movements, and developing competence over flares was the therapeutic relationship with their physiotherapist. Participants reported how the interactions with their physiotherapists gave them confidence to engage in movements and activities they feared and avoided. These findings are consistent with other qualitative inquiries embedded in trials of both exercise-based and psychologically informed interventions for CLBP (Joyce et al., 2023; Saunders et al., 2022; Tankha et al., 2023), and previous cross-sectional research on CFT for CLBP (Bunzli et al., 2016). Beyond the therapeutic relationship, participants described how re-engaging with valued activities facilitated feeling valued and connected in their communities, which in turn further motivated their self-management efforts and highlights the role of relatedness in developing autonomy. These findings are consistent with qualitative inquiries exploring treatment mechanisms for pain reprocessing therapy and a large meta-ethnography exploring the process of recovery from CLBP both identifying that understanding the multifactorial contributors to pain, reducing pain threat, and social connectedness were important perceived facilitators of improvement (Tankha et al., 2023; Toye et al., 2021).
Strengths and Limitations
This study employed a narrative approach, focusing on how participants construct meaning chronologically (Riessman, 2008). Unlike previous CFT research which used interpretive description (Bunzli et al., 2016; Wernli et al., 2022), this narrative approach delves into participants’ evolving perspectives and offers a comprehensive view, granting the participants coherence over time (Riessman, 2008). These novel findings demonstrate how the nature of change can occur quickly for some people, such as “Plain, Smooth Sailing,” or can take repeated practice with continued support like participants in “Learning the Ropes and Gaining Sea Legs.” Alternatively, this process can hit roadblocks that require more time and support than what is captured in this study, like the experiences of “Sailing Through Headwinds.” Through exploring the experience of CFT longitudinally, the findings also describe potential mechanisms of change during and after CFT treatment. This includes the importance of successful experiences of pain control, connecting with the body, and therapeutic alliance. These insights should be explored in future treatment mechanism studies using various methodologies, which are important for understanding and improving effective treatments like CFT.
However, several limitations must be acknowledged. The transferability of this study is limited. Participants were solely from Greater Perth Region (Western Australia), lacking representation from younger age groups and diverse populations, such as Aboriginal and Torres Strait Islanders and people with English as a second language. While the range of CLBP duration (3 months to 36 years) demonstrates diversity in experiences in this study, this may have affected the participant narratives. Increasing the sample size to capture more representation across CLBP duration may have been beneficial to uncovering experiences and potential mechanisms to supporting self-management in this patient population.
To support the continuing development and refinement of CFT and understanding self-management of CLBP, future research may also consider exploring the barriers and enablers of change from the perspectives of people with CLBP and their physiotherapists.
Conclusion
This qualitative narrative inquiry described the overarching narrative theme of “The Journey to Self-Management” for people with CLBP. Within this overarching narrative theme, four distinct narrative themes were identified, beginning with “Left High and Dry” and concluding with three narratives capturing the different trajectories of CFT from the start of treatment through to the 12-month follow-up: “Plain, Smooth Sailing,” “Learning the Ropes” and “Gaining Sea Legs,” and “Sailing Through Headwinds.” In exploring CLBP self-management using CFT, the findings of this study emphasized the importance of linking body and pain awareness, reconceptualizing and reducing the threat of pain, gaining control, and resuming essential and valued activities. This was enabled through sense-making processes and successful exposure to movement and activity, underpinned by a strong therapeutic relationship. Those who experienced “headwinds” in their journey reported lacking confidence or a comprehensive understanding of their body and pain. Clinicians treating individuals with CLBP can use these insights to facilitate the CFT treatment journey more effectively, including the journey toward ongoing self-management. Lastly, the different paths taken by the participants, depicted in metaphorical narrative themes, may offer resonance, validation, helpful insights, and different perspectives, for people living with CLBP as they learn the ropes or bravely face headwinds in their own journeys to self-management.
Supplemental Material
Supplemental Material - A Prospective Qualitative Inquiry of Patient Experiences of Cognitive Functional Therapy for Chronic Low Back Pain During the RESTORE Trial
Supplemental Material for A Prospective Qualitative Inquiry of Patient Experiences of Cognitive Functional Therapy for Chronic Low Back Pain During the RESTORE Trial by Nardia-Rose Klem, Peter O’Sullivan, Anne Smith, and Robert Schütze in Qualitative Health Research
Supplemental Material
Supplemental Material - A Prospective Qualitative Inquiry of Patient Experiences of Cognitive Functional Therapy for Chronic Low Back Pain During the RESTORE Trial
Supplemental Material for A Prospective Qualitative Inquiry of Patient Experiences of Cognitive Functional Therapy for Chronic Low Back Pain During the RESTORE Trial by Nardia-Rose Klem, Peter O’Sullivan, Anne Smith, and Robert Schütze in Qualitative Health Research
Supplemental Material
Supplemental Material - A Prospective Qualitative Inquiry of Patient Experiences of Cognitive Functional Therapy for Chronic Low Back Pain During the RESTORE Trial
Supplemental Material for A Prospective Qualitative Inquiry of Patient Experiences of Cognitive Functional Therapy for Chronic Low Back Pain During the RESTORE Trial by Nardia-Rose Klem, Peter O’Sullivan, Anne Smith, and Robert Schütze in Qualitative Health Research
Supplemental Material
Supplemental Material - A Prospective Qualitative Inquiry of Patient Experiences of Cognitive Functional Therapy for Chronic Low Back Pain During the RESTORE Trial
Supplemental Material for A Prospective Qualitative Inquiry of Patient Experiences of Cognitive Functional Therapy for Chronic Low Back Pain During the RESTORE Trial by Nardia-Rose Klem, Peter O’Sullivan, Anne Smith, and Robert Schütze in Qualitative Health Research
Footnotes
Acknowledgement
We thank Dr Robert Wells for his role as a critical friend during the revision process.
Author Contributions
(i) All authors made a substantial contribution to the design of the work or acquisition, analysis, interpretation, or presentation of data; (ii) all authors drafted the article or revised it critically for important intellectual content; (iii) all authors approved the version to be published; and (iv) each author participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PO and RS have received speaker fees for lectures or workshops on the biopsychosocial management of pain, including on CFT, from special interest physiotherapy groups and multi-disciplinary audiences of clinicians and researchers. PO is a clinical director of a physiotherapy clinic that provides person-centered care including CFT. RS has received a part-time salary from the Insurance Commission of Western Australia to work on another clinical trial of CFT.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We thank the participants in the study and both the Australian National Health and Medical Research Council (grant number: 1145271) and Curtin University, Perth, WA, Australia, for funding of the RESTORE trial.
Correction (February 2025):
The Conflict of interest section in the article has been updated since its original publication. See correction notice (10.1177/10497323251320187) for more details.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.