
Abstract
Objective
We explored differences in postural stability between subgroups of patients with low back pain (LBP) and varying risk levels for developing chronicity measured using the Subgroups for Targeted Treatment (STarT) Back Tool.
Methods
This was a cross-sectional, single-session, double-blind experimental study among 65 participants who had LBP for more than 14 days. Postural stability was assessed by measuring the center of pressure (COP) range, displacement area, and velocity in anterior–posterior and mediolateral directions under four sensory and cognitive conditions: (i) eyes open and counting forward, (ii) eyes closed and counting forward, (iii) eyes closed and counting forward in multiples of seven, and (iv) eyes closed and counting backward in multiples of seven. The participants were stratified into low-/medium- (n = 53) and high-risk (n = 9) subgroups.
Results
There were no significant between-group differences among patients with LBP stratified as having a low/medium or high risk of chronicity in postural stability and sensory and cognitive conditions.
Conclusions
Impaired postural stability is important to consider when treating patients with LBP. However, we found that these impairments were not strongly aggravated in groups with a higher risk of chronicity, as measured using the STarT Back Tool.
Keywords
Introduction
Low back pain (LBP) is the leading cause of disability globally 1 and in most cases, its origin is idiopathic. A growing body of evidence in the literature supports that pain is multidimensional and includes all aspects of the biopsychosocial model. 2 Owing to the multidimensional nature of pain, patients with LBP constitute a heterogeneous group, and there is an increased focus on identifying subgroups of patients to improve treatment, which may help clinicians to tailor treatments accordingly. 3 An applied method for subgrouping patients is the Subgroups for Targeted Treatment (STarT) Back Tool (SBT), which has been translated into more than 20 languages and is now a widely used tool for subgrouping patients with LBP. 4 The SBT stratifies patients into three groups, with either low-, medium- or high-risk of developing ongoing debilitating LBP on the basis of different baseline characteristics. 5
Patients with LBP display postural control strategies that differ from people not experiencing LBP, especially during tasks involving increased complexity.6–8 Moreover, postural stability during standing is altered in patients with chronic LBP.9–12 However, there is conflicting evidence in this regard, with some studies reporting no impaired postural stability in patients with LBP.13,14 This discrepancy in findings may be explained by unrecognized subgroups of patients with LBP, in which postural stability is affected in some and not in others. Postural stability is reliant on somatosensory input of vestibular, proprioceptive, and visual sensory information, triangulating the body’s position in space and calculating the adequate somatosensory response to maintain postural control. 15 Manipulating the quality of the available sensory information, for example by asking individuals to stand on different surfaces with eyes open and closed, allows for a more detailed evaluation of how this sensory information is integrated to generate proper postural strategies, including in populations with chronic pain conditions.16,17 Therefore, maintaining postural stability is believed to demand a certain level of cognitive capacity, which is evident in decreased postural stability with the addition of cognitive tasks to a postural task, which is termed cognitive loading.18–20 The conscious interpretation of (or attention to) painful stimulation is a cognitively demanding process that requires a considerable amount of available cognitive resources,21,22 which can impair physical performance.8,23,24 Furthermore, in addition to pain, patients with LBP stratified to the SBT high-risk group might have further cognitive challenges owing to anxiety, depression, and stress coping, 25 as measured using the distress subscale of the SBT. 5 This may result in decreased postural stability compared with patients in the low- and median-risk groups. If postural stability is more affected among patients scoring as high risk according to the SBT than among patients in the other two SBT groups, this can guide practice in identifying patients who may respond to balance exercises. The purpose of this study was to compare postural stability between patients with LBP in SBT high-risk groups with those in SBT low- and medium-risk groups using a platform to measure postural sway. We hypothesized that challenging postural stability under conditions where sensory information is reduced and cognitive load is increased has a greater impact on postural stability among patients in the SBT high-risk group than among those in SBT low- and medium-risk groups.
Methods
Design
This was a cross-sectional, single-session, double-blind experimental study. The study was registered in ClinicalTrials.gov before recruitment was initiated (NCT03065439). This study was conducted in accordance with the Declaration of Helsinki. 30 All data were handled and stored in accordance with local Danish law. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies. 31
Study participants and centers
Patients were seen in primary care clinics and recruited from a physiotherapy and chiropractic clinic and from a general practitioner practice. Inclusion criteria were patients aged 18 to –65 years, presenting with LBP (pain above the gluteal fold and below the 12th rib) 32 for more than 14 days. We excluded patients with signs of serious pathology (e.g., fracture, cauda equina syndrome, malignancy, osteoporosis, or spinal inflammatory arthritis) and those with blindness, dyslexia, pregnancy, and patients unable to walk unassisted or unable to complete the questionnaire unassisted.
Outcome measures
After patients provided their written informed consent, we collected their demographic data: age, sex, educational level (college degree, yes/no), employment status, sick leave, comorbidities other than LBP (yes/no), pain duration (2–6 weeks/subacute or chronic), pain intensity (numerical pain rating scale, NPRS), 33 23-question Roland Morris Disability Questionnaire (RMDQ), 34 and self-reported health status (EuroQol Five Dimensions [EQ-5D] visual analogue scale). 35 After completing the questionnaire, patients removed their jacket and shoes and emptied their pockets before height and weight were measured.
Postural sway was measured using a force plate (Metitur Good Balance System® version 2.67, Metitur, Jyväsklä, Finland). The force plate was placed in front of the patient, at a distance of 100 cm from a wall and with more than 100 cm of free space to the sides and behind the force plate. The force plate is an equilateral triangle (800 mm) with four strain gauge transducer signals converted via a three-channel DC amplifier and transformed into digital data (50 Hz) that are subsequently filtered digitally, using a three-point median filter and infinite impulse response (IRR) filter with 20 Hz cutoff frequency. Finally, the center of pressure (COP) position was calculated using dedicated software (Metitur Good Balance System®). COP position data were then exported and loaded in Matlab R2016a software (MathWorks, Natick, MA, USA) where the COP area (95% prediction ellipse 36 range [the difference between maximum and minimum COP position] and velocity [the first derivative of the COP position] sway in both the mediolateral (ML) and anterior–posterior (AP) directions was extracted.
During the static balance test, patients were asked to stand as still as possible for 35 s under four different conditions, in the following order: (i) eyes open and counting forward (EO easy) (ii) eyes closed and counting forward (EC easy), (iii) eyes closed and counting forward in multiples of seven (EC medium), and (iv) eyes closed and counting backward from 500 in multiples of 7 (EC hard). Patients were instructed to maintain the standing position and to avoid lifting their feet off the floor. During the condition with eyes open, patients were instructed to focus on a 12-cm circular green plate placed at eye level on the wall, 1 m in front of the patient. The order of testing represented increased difficulty, and it was likely that learning took place during testing under the four conditions. Therefore, to ensure equal test procedures between groups and to thereby minimize the risk of bias, the ordering was not counterbalanced.
Following balance testing, the nine-item SBT was administered. This screening tool includes an overall score and a distress subscale, the latter indicating psychological and social dimensions of the patient’s experience of LBP. 37 Patients who scored four or more points overall with a subscore of three or fewer points were stratified to the low-/medium-risk group; patients who scored four or more points overall and four or more points on the subscale were stratified to the high-risk group. 4
Data analysis
A pilot test was conducted among 13 individuals without LBP under the condition EC hard (eyes closed, counting backwards in multiples of seven). The mean additional lateral sway was found to be 0.51 (0.68) cm and was used to estimate the sample size for the study. We set an 80% power to detect twice the lateral sway in the high-risk group compared with the low- and medium-risk groups combined, with a difference of 0.51 in lateral sway (pilot study). On the basis of the pilot study, a mean 0.51 cm extra lateral sway in the low- and medium-risk groups and an additional sway of 1.02 cm in the high-risk group was expected. Results were omitted from the final analysis in the case of missing or compromised data.
The study was powered with 63 patients needed. Patients’ characteristics are reported as number (%) for categorical variables and mean (standard deviation) or median (interquartile range) for continuous variables, depending on the distribution of the data.
Normal data distribution was determined by reviewing boxplots and using the Shapiro–Wilk test. Parametric or non-parametric analysis was performed as appropriate, on the basis of the distribution. Mean and standard error of the mean are reported for patient characteristics with between-group comparisons made using independent sample t-tests for continuous variables and the χ2 test for dichotomous data. Data for postural stability were non-normally distributed so the median and interquartile range are reported with between-group comparisons made using the Mann–Whitney U test.
Spearman rank-order correlation was performed to explore the relationships of COP area, range, and velocity under the four conditions (EO easy, EC easy, EC medium, and EC hard) in both the low-/medium- and high-risk groups. The strength of the interpretation was considered negligible (0.00 to −0.03), low (−0.3 to −0.5), moderate (−0.5 to −0.7), high (−0.7 to −0.9), or very high (−0.90 to −1.00) correlation. 38 The assumptions for all tests were met and the level of significance for the tests was set at 0.05.
Ethics
This study was approved by the regional ethics committee in the North Denmark Region on 5 January 2018 (N-20170014). All patients provided their signed informed consent no earlier than the day after having been provided verbal information regarding the study.
Results
Flow of participants and study centers
Sixty-five participants aged 20 to 64 (mean 46.5) years were included in the study, with 38 (58.5%) women; 49 participants (75.5%) had experienced LBP for more than 3 months. Three participants were excluded from the final analysis owing to missing postural stability data. The remaining 62 patients were stratified to the low-/medium-risk group (n = 53) or high-risk group (n = 9). There was no significant difference between the groups at baseline for the variables age, body mass index, education level, employment, presence of comorbidities, or pain duration. A significant difference was found for sick leave (p = 0.001) as well as for pain intensity (NPRS), self-reported health status (EQ-5D visual analogue scale), and disability (RMQD) (all p<0.001), as presented in Table 1.
Baseline characteristics of participants according to STarT Back Tool grouping of low/medium and high risk.

Data are expressed as n (%) or mean ± standard error of the mean. χ2 test used to determine between-group differences for sex, college degree, employment status, presence of comorbidities, and pain duration. Student t-test performed to assess between-group differences for age, body mass index, sick leave, pain intensity, self-reported health status (EQ-5D), and RMQD scores.
LBP, lower back pain; EQ-5D, EuroQol Five Dimensions; RMQD, Roland Morris Disability Questionnaire; NPRS, numerical pain rating scale.
Postural stability
Figure 1 shows the median and interquartile range for COP range and velocity in the ML and AP directions, as well as the COP area for all four conditions (EO easy, EC easy, EC medium, and EC hard). For the ML CoP range, the Mann–Whitney U test showed no significant difference between low-/medium- and high-risk groups and the dependent variables EO easy (Z = 0.03), EC easy (Z = 0.43), EC medium (Z = 0.79), and EC hard (Z = 0.03). For the AP COP range, there was no significant difference between low-/medium- and high-risk groups and the dependent variables EO easy (Z = 0.69), EC easy (Z = 1.21), EC medium (Z = 0.81), and EC hard (Z = 0.13). We found no significant difference for ML velocity between low-/medium- and high-risk groups and the dependent variables EO easy (Z = 0.43), EC easy (Z = 0.17), EC medium (Z = 0.11), and EC hard (Z = 0.03). AP velocity showed no significant difference between low-/medium- and high-risk groups and the dependent variables EO easy (Z = 0.73), EC easy (Z = 0.91), EC medium (Z = 0.51), and EC hard (Z = 0.21). Lastly, for COP position, there were no significant differences between low-/medium- and high-risk groups and the dependent variables EO easy (Z = 0.19), EC easy (Z = 1.07), EC medium (Z = 1.27), and EC hard (Z = 0.55).
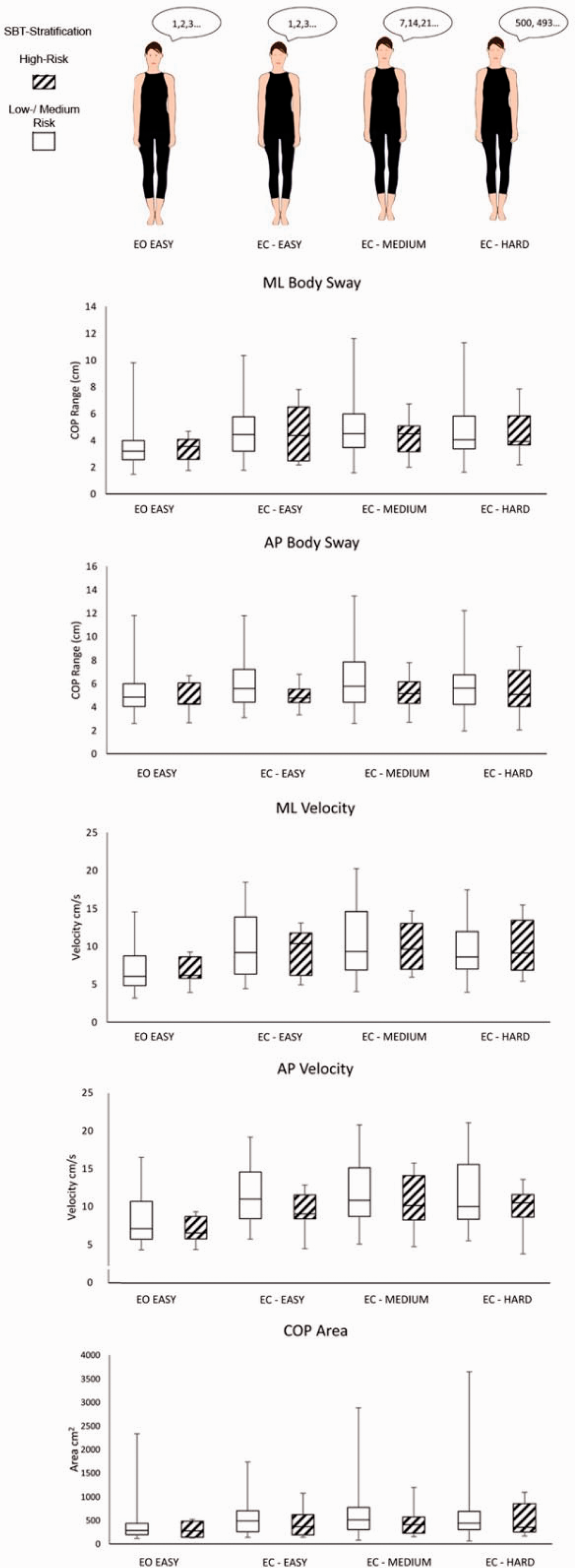
Body sway and velocity. Median body sway and velocity shown in the anterior–posterior (AP) and mediolateral (ML) directions as well as the center of pressure (COP) area for the combined low-/medium- and high-risk groups, according to STarT Back tool (SBT) stratification, and under four conditions: eyes open counting forward (EO easy), eyes closed counting forward (EC easy), eyes closed counting forward in multiples of seven (EC medium), and eyes closed counting backwards in multiples of seven (EC hard). Error bars show the interquartile range.
Spearman correlation analysis showed no significant association between low-/medium- and high-risk groups for COP range or velocity in the ML or AP directions or for COP area (Table 2).
Association between SBT risk groups and postural stability.

Spearman rank-order correlation showed no significant association between velocity in the anterior–posterior (AP) and mediolateral (ML) directions, as well as center of pressure (COP) area, in the combined low-/medium- and high-risk groups, according to STarT Back Tool (SBT) stratification and under four conditions: eyes open counting forward (EO easy), eyes closed counting forward (EC easy), eyes closed counting forward in multiples of seven (EC medium), and eyes closed counting backwards in multiples of seven (EC hard).
Discussion
In this study, we did not find decreased postural stability among patients with LBP identified as having a high risk of developing chronic LBP, according to the SBT, as compared with their counterparts in the low- and medium-risk groups.
The reason we found no between-group differences could be owing to the stratification of participants. The distress subscale of the SBT 37 includes items associated with decreased postural stability, including pain catastrophizing, 26 depression, 27 and fear.28,29 The SBT may not being sufficiently sensitive to identify the domains within these psychological states that pertain to decreased postural stability. However, one study reported that when decisions to refer patients with LBP for cognitive intervention were based on SBT stratification rather than the physiotherapists’ judgment, patients reported higher quality of life after 4 months, 39 indicating a cognitive component of patients’ condition that could possibly influence their postural stability.
Rabey et al. 40 found that participants stratified to the SBT high-risk group had higher pain summation and two-point discrimination than patients in the low- or medium-risk groups, indicating that the high-risk group had a higher level of sensitization associated with their chronic LBP. Increased stiffness has been associated with higher levels of sensitization in participants with knee osteoarthritis. 16 Although not measured in this study, it is possible that patients in the high-risk group also had a higher level of sensitization, which could result in decreased postural stability owing to increased stiffness.
Previous studies comparing postural stability in subgroups of patients with LBP have found that those with more severe LBP (higher pain and disability levels) have decreased postural stability compared with patients who have moderate LBP and pain-free controls.41,42 Cognitive load did not affect postural stability in both patient groups in those studies. This is in contrast to a previous study where participants who were exposed to experimental pain were given a cognitive task (i.e., counting forward) similar to the EO easy task in the present study. Patients had reduced COP sway, and COP sway was increased when patients were asked to count backwards in intervals of three. 43 Suda et al. 43 considered that the reduction in postural sway in patients while experiencing pain was a protective strategy to avoid falling by limiting excessive translation of the body. It is possible that this protective strategy is not present in patients with longstanding pain, which would explain the results of the present study. Furthermore, Suda et al. used tandem standing, 43 thus challenging postural stability to a greater degree than in our study, which could account for the difference in findings. Another possible explanation is that patients with LBP who are stratified to the SBT high-risk group have been found to be less physically active, 44 which has been associated with higher rates of falls in older people 45 and increased postural sway in middle-aged men and women. 46
Future research should focus on movement variability among patients categorized as having a high risk of chronicity according to the SBT. The results of the current study indicate that during all tasks, patients in the high-risk group had less movement variability, indicated by the interquartile range converging on the median for body sway, velocity, and COP area, in comparison with the combined low-/medium-risk group. This is in line with previous findings where patients with spinal pain displayed a decrease in postural sway; 47 this change in postural stability appears to be sensitive to the amount of pain reported by the patient. 48 This could possibly be owing to decreased movement variability in the SBT high-risk group, in line with previous findings among patients with LBP; 49 however, further investigation is needed.
Limitations
The small sample size for the high-risk group (n = 9) is the primary limitation of this study. Furthermore, we did not control for the number of cognitive errors made by participants when counting, and we could have further elucidated the impact of the cognitive task on available cognitive resources among participants. Previous research has shown that when performing a cognitive task concurrently with a motor task in which postural stability is challenged, individuals will prioritize cognitive resources to maintain postural stability, thereby sacrificing accuracy in the cognitive task.29,50–52
Participants were only tested once under each of the four conditions. Having multiple test results for each condition could strengthen the reliability of the data. The inclusion criteria for age was broad in this study (18–65 years). Age-related changes in postural control have previously been reported, which could affect the findings of our study, with possible bias most likely influencing the results in the direction of no difference between groups. However, given the relatively small difference in age between groups, we do not believe that bias was introduced according to age. Simple testing for static postural stability was used in this study as a proxy measure for cognitive load, and we found no significant differences between subgroups of patients with LBP. We do not know if the findings also apply for functional stability. Future research is needed to study this further.
Conclusion
Patients with LBP, identified as having a high risk of poor prognosis according to stratification using the SBT, did not display significantly decreased postural stability, compared with patients considered to have low and medium risk of a poor prognosis.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221112046 - Supplemental material for Difference in postural stability between STarT Back Tool subgroups of patients with low back pain under conditions of sensory deprivation and cognitive load
Supplemental material, sj-pdf-1-imr-10.1177_03000605221112046 for Difference in postural stability between STarT Back Tool subgroups of patients with low back pain under conditions of sensory deprivation and cognitive load by Stian Ingemann-Molden, Rogerio Pessoto Hirata, Martin Bach Jensen, Thomas Graven-Nielsen and Allan Riis in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605221112046 - Supplemental material for Difference in postural stability between STarT Back Tool subgroups of patients with low back pain under conditions of sensory deprivation and cognitive load
Supplemental material, sj-pdf-2-imr-10.1177_03000605221112046 for Difference in postural stability between STarT Back Tool subgroups of patients with low back pain under conditions of sensory deprivation and cognitive load by Stian Ingemann-Molden, Rogerio Pessoto Hirata, Martin Bach Jensen, Thomas Graven-Nielsen and Allan Riis in Journal of International Medical Research
Footnotes
Data availability statement
To ensure patient confidentiality, data included in the current study are not publicly available but are available from the corresponding author upon reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: TGN is a part of the Center for Neuroplasticity and Pain (CNAP), supported by the Danish National Research Foundation (DNRF121). AR was supported by the Magda and Svend Aage Friederichs Memorial Fund (2016).
Author contributions
All authors have contributed to conceptualization of the study. SIM, RPH, and AR conducted the analysis. All authors have read and commented on the manuscript in rounds of revision and all have approved the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.