
Abstract
Aboriginal Australians experience a high prevalence of chronic obstructive pulmonary disease (COPD), with high rates of potentially preventable hospitalisations. However, little is known about Aboriginal peoples’ experiences of living with COPD and how they navigate health care systems. This study used thematic analysis and Aboriginal methodology to explore Aboriginal peoples’ lived experiences of COPD, their health care journey from receiving a diagnosis of COPD to the clinical management, and the impact of COPD on their daily lives. We conducted in-depth semi-structured interviews over a 6-month period with 18 Aboriginal adults diagnosed with COPD from four Aboriginal Community Controlled Health Services (ACCHS) in New South Wales, Australia. Reflexive thematic analysis was employed to ensure rigour. The findings revealed deeply personal and reflective stories shaped by historical, social, and cultural realities of Aboriginal peoples living with COPD. Four themes were identified characterising their experiences. Based on the findings, the following guidance is provided on future COPD care for Aboriginal peoples: Better alignment of existing COPD management with Aboriginal peoples’ cultural contexts and perspectives to improve access to culturally safe care; Increased funding for ACCHS to enhance COPD management, such as early detection through case finding and access to ACCHS-led pulmonary rehabilitation; Engaging family members in COPD management and providing culturally centred COPD education that facilitates discussions and builds health literacy and self-management skills; Implementing health promotion initiatives to increase awareness and counteract fear and shame to improve early COPD detection.
Keywords
Background
Aboriginal and Torres Strait Islander peoples (hereafter respectfully referred to as Aboriginal peoples, as the preferred terminology in New South Wales (NSW) where the study was conducted) are the Indigenous peoples of Australia. Aboriginal peoples have inhabited Australia for tens of thousands of years (McDonald et al., 2018) and are heterogeneous, comprising hundreds of diverse Aboriginal language groups, each with their distinct cultural traditions, customs, and practices (Australian Institute of Health and Welfare [AIHW], 2015, 2023b; Karidakis, 2021; Simpson & Wigglesworth, 2019). Presently, Aboriginal peoples represent 3.8% of the Australian population (AIHW, 2023b). Significant disparities in morbidity and mortality between Aboriginal peoples and non-Aboriginal populations have been extensively documented and continue to persist, despite well-intentioned government policies (Australian Bureau of Statistics [ABS], 2017; AIHW, 2015; Gruber, 2017; Productivity Commission, 2023). These disparities are due to complex intergenerational issues, such as the ongoing impacts of colonisation, dispossession of traditional lands, racism and socio-cultural determinants of health including economic and education factors, and lack of access to health care services, which together contribute to the unequal burden of disease (AIHW, 2022; Gatwiri et al., 2021).
Chronic obstructive pulmonary disease (COPD) is a preventable chronic lung disease characterised by airflow obstruction, leading to symptoms such as cough, mucus production, and shortness of breath, significantly affecting an individual’s exercise capacity and quality of life (World Health Organisation [WHO], 2023). The burden of COPD on the Australian health care system is high, estimated at $929 million/year (Access Economics, 2008; Brooke et al., 2017). The prevalence of COPD in Aboriginal adults is 2.5 times higher than other Australians (AIHW, 2014). Aboriginal peoples are disproportionately impacted by COPD compared to non-Aboriginal peoples, with higher rates of potentially preventable hospitalisations and limited access to best practice COPD management within primary health care (ABS, 2017; AIHW, 2014, 2019; Yang et al., 2022).
Australian COPD guidelines emphasise the importance of increasing knowledge and awareness of COPD, implementing self-management strategies to slow disease progression and reduce exacerbations (Yang et al., 2022). To achieve meaningful health outcomes for Aboriginal peoples living with COPD, there is a growing recognition of the need to reorient health care in culturally centred ways that actively engage Aboriginal peoples and incorporate Aboriginal voices in service co-design and implementation (Durey et al., 2016).
In Australia, like other colonised countries, it is evident that mainstream health systems are failing to meet the needs of Indigenous peoples (Harfield et al., 2018). Aboriginal peoples have reported various barriers to accessing health care, including racial discrimination, impacting timely and essential treatment (Nolan-Isles et al., 2021). To address service shortcomings in Australia, Aboriginal Community Controlled Health Services (ACCHS) were established to deliver culturally safe primary health care aligned with local Aboriginal communities’ priorities and needs (National Aboriginal Controlled Controlled Health Organisation [NACCHO], 2022; Panaretto et al., 2014). Broadly, cultural safety refers to how care is delivered and how care is experienced by the person receiving care. Addressing cultural safety requires health care organisations and professionals to respect Aboriginal cultural identities, and reflect and respond to conscious or unconscious bias and power imbalances, ensuring care delivered is free from racism, accessible, and appropriate for Aboriginal peoples (AIHW, 2023a). ACCHS have successfully delivered care within the cultural interface of a western biomedical model and Aboriginal ways of knowing, being, and doing, to improve Aboriginal health outcomes (Pearson et al., 2020). Fundamental to ACCHS success has been delivering care aligned with Aboriginal culture, holistic concepts of health (Campbell et al., 2018; DOH, 2021), and Aboriginal peoples’ perspectives about their local health needs and services (Jongen et al., 2020).
Previous studies have examined Aboriginal peoples’ experience with chronic conditions, such as diabetes (Straw et al., 2019; Weaver et al., 2022). However, no previous studies have focussed on Aboriginal peoples living with COPD, despite the disparate impact in Aboriginal communities (AIHW, 2014). Recent research with Aboriginal communities has increasingly embraced a narrative or storied approach to data collection, incorporating the cultural practice of “yarning” (Kennedy et al., 2022; Walker et al., 2014). Yarning is grounded in Aboriginal ways of knowing, being, and doing and is a conversational process involving sharing stories, knowledge, and experiences (Bessarab & Ng’andu, 2010; Martin & Mirraboopa, 2003; Walker et al., 2014). Studies have highlighted the importance of this narrative approach, which prioritises Aboriginal voices and improves understanding from Aboriginal perspectives (Rieger et al., 2023), empowering Aboriginal peoples to share their experiences in their own terms in their own way (Cunsolo Willox et al., 2013). Developing an evidence-informed understanding of Aboriginal peoples’ experiences living with COPD may support implementation of COPD-specific services for Aboriginal peoples (Haynes et al., 2021; Straw et al., 2019) by privileging Aboriginal worldviews and reorienting services with the needs of Aboriginal communities (Haynes et al., 2021; Shahid et al., 2009; Straw et al., 2019).
This study aims to explore and describe the lived experiences of Aboriginal peoples with COPD in Australia.
Methods
Study Background and Setting
This qualitative study on the experience of care of Aboriginal peoples with COPD was conducted as part of the Breathe Easy, Walk Easy, Lungs for Life (BE WELL) Project (Meharg et al., 2022), which aimed to evaluate the design and implementation of culturally safe pulmonary rehabilitation (PR) within four NSW ACCHS located in towns defined by the Modified Monash geographical classification as Category 3 (large rural towns) and Category 4 (medium rural towns) (DOH, 2019). The NSW Aboriginal Health & Medical Research Council Human Ethics Committee (HREC 1261/17) provided approval for this study.
Participants
Convenience sampling was used to recruit participants. Inclusion criteria were being a client of one of the four NSW ACCHS implementing the BE WELL project; identifying as Aboriginal and/or Torres Strait Islander; and having a confirmed diagnosis of COPD. ACCHS staff generated a COPD client list from Communicare, the local clinical data management system (AIHW, 2020), and invited potential participants to join the study. Written informed consent was obtained prior to data collection. Participants could bring a family member or Aboriginal health worker to the interview for support. Participants were offered a gift voucher of $50 as reimbursement for their time.
Data Collection
The semi-structured interviews were audio and video recorded. They comprised questions about participants’ lived experiences of COPD and interactions with health service providers (see Supplemental File Interview Guide, Additional File 1).
To offer participants choice, and to minimise potential COVID-19 exposure, interviews were conducted either face-to-face at the ACCHS or remotely using the video or phone function within Zoom (Zoom Video Communications Inc., 2016), an online video-conferencing platform.
Aboriginal peoples maintain a deep connection to oral traditions of storytelling (Yunkaporta, 2019). Increasingly, yarning methodology is being used by researchers as an appropriate method for data collection when conducting research with Aboriginal peoples, as this storied approach recognises the importance of storytelling in Aboriginal cultures (Yunkaporta, 2019). Yarning guided the interview conversation and interactions (Burke et al., 2022). Yarning is an Aboriginal conversational process to share experiences, perspectives, and ideas based on Aboriginal ways of knowing, being, and doing (Bessarab & Ng’andu, 2010; Martin & Mirraboopa, 2003; Walker et al., 2014) and enable Aboriginal knowledges to inform western approaches and health service delivery (Haynes et al., 2021; Shahid et al., 2009). Interviews commenced with formal introductions to place the researcher and participant within Aboriginal social structures and kinship systems, and then transitioned to the interview questions. Participants set the speed and flow of discussions. Interview questions were intertwined into participants’ narrative, strengthening the conversational “yarning” nature of the interviews.
Recruitment ceased after participants from each of the four ACCHS had been interviewed. Debriefing occurred amongst the three researchers (DM, JA, and SD), confirming data saturation had been reached. Audio recordings were transcribed verbatim and de-identified to maintain participants’ confidentiality. Two researchers (DM and JA) reviewed transcriptions against audio recordings for accuracy.
Data Analysis
NVivo (QSR International Pty Ltd, 2020) was used to code the interview data. Reflexive thematic data analysis was applied within a schema of six areas of COPD experience from receiving an initial COPD diagnosis, sharing a diagnosis, COPD management, health literacy, impact of living with COPD, and opportunities for COPD service improvement. Initial coding was conducted by three researchers (DM, JA, and SD) with subsequent team meetings to verify coding and discuss themes with an additional researcher (JMc).
Guiding Approach
Reflexive thematic analysis was used to explore Aboriginal peoples’ lived experiences of COPD (Braun & Clarke, 2019) because it offered a rigorous analytic process aligned with our research question. It also captured and analysed the rich insights gained from interviews about the participants’ worldviews and supported the identification of key themes, allowing the research team to continually engage in reflexive practices and consider our positionality and assumptions throughout the study (Braun & Clarke, 2012, 2019). Indigenous standpoint theory was used as a guiding framework because it acknowledges Aboriginal peoples’ knowledge and perspectives and demonstrated the research team’s commitment to cultural respect (Smith, 2021). This framework privileges Aboriginal voices, experiences, and worldviews, while simultaneously recognising Aboriginal peoples as experts in their own experiences. By using this framework, the research team could apply Aboriginal yarning methodology to data collection and strengthen participants’ cultural safety, while being informed by Aboriginal ways of knowing, being, and doing (Martin & Mirraboopa, 2003; Smith, 2021).
The research team (DM, JA, and SD) utilised a thematic analysis framework (Braun & Clarke, 2006). We immersed ourselves in the data by listening to audio recordings and reading and re-reading the transcriptions, taking additional notes, enabling a thorough exploration of the data to uncover the underlying meanings. The transcripts were coded inductively by the team. Aspects of the participants’ experiences, which may be downplayed in their everyday familiarity, were considered in relation to what was being described and shared so not to be overlooked. To ensure rigour of our coding process, the team included four researchers, two experienced qualitative researchers (SD and JMc), an Aboriginal researcher (DM), and two experts in COPD (SD and JA). Finally, key themes were identified and labelled, drawing on central concepts and achieving consensus amongst these four researchers. Member checking was conducted in person with participants to discuss, amend, and confirm the interpretation of the findings. An infographic was developed to visually present the findings and guide discussions (see Supplemental File Experience of Care Infographic, Additional File 2).
To enhance the robustness, credibility, and overall quality of the study, the researchers (DM and JA) employed reflexive rigour to ameliorate the potential influence of their professional, personal, and cultural perspectives throughout all stages of the study. To increase the quality of coding and data analysis, two authors (SD and JMc) engaged critical inquiry, verifying the inductive coding framework and coded text with the other two researchers (DM and JA). This collaborative process further strengthened rigour (Braun & Clarke, 2019; Mays & Pope, 2000).
Results
Participant Characteristics.
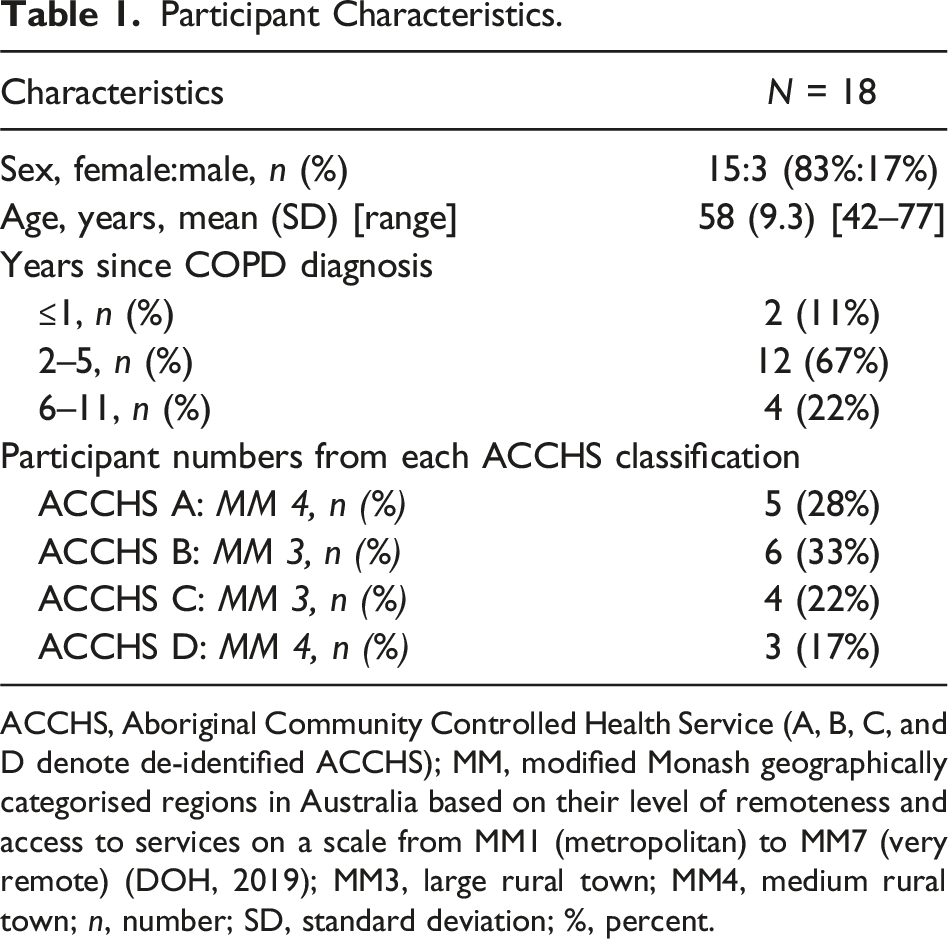
ACCHS, Aboriginal Community Controlled Health Service (A, B, C, and D denote de-identified ACCHS); MM, modified Monash geographically categorised regions in Australia based on their level of remoteness and access to services on a scale from MM1 (metropolitan) to MM7 (very remote) (DOH, 2019); MM3, large rural town; MM4, medium rural town; n, number; SD, standard deviation; %, percent.
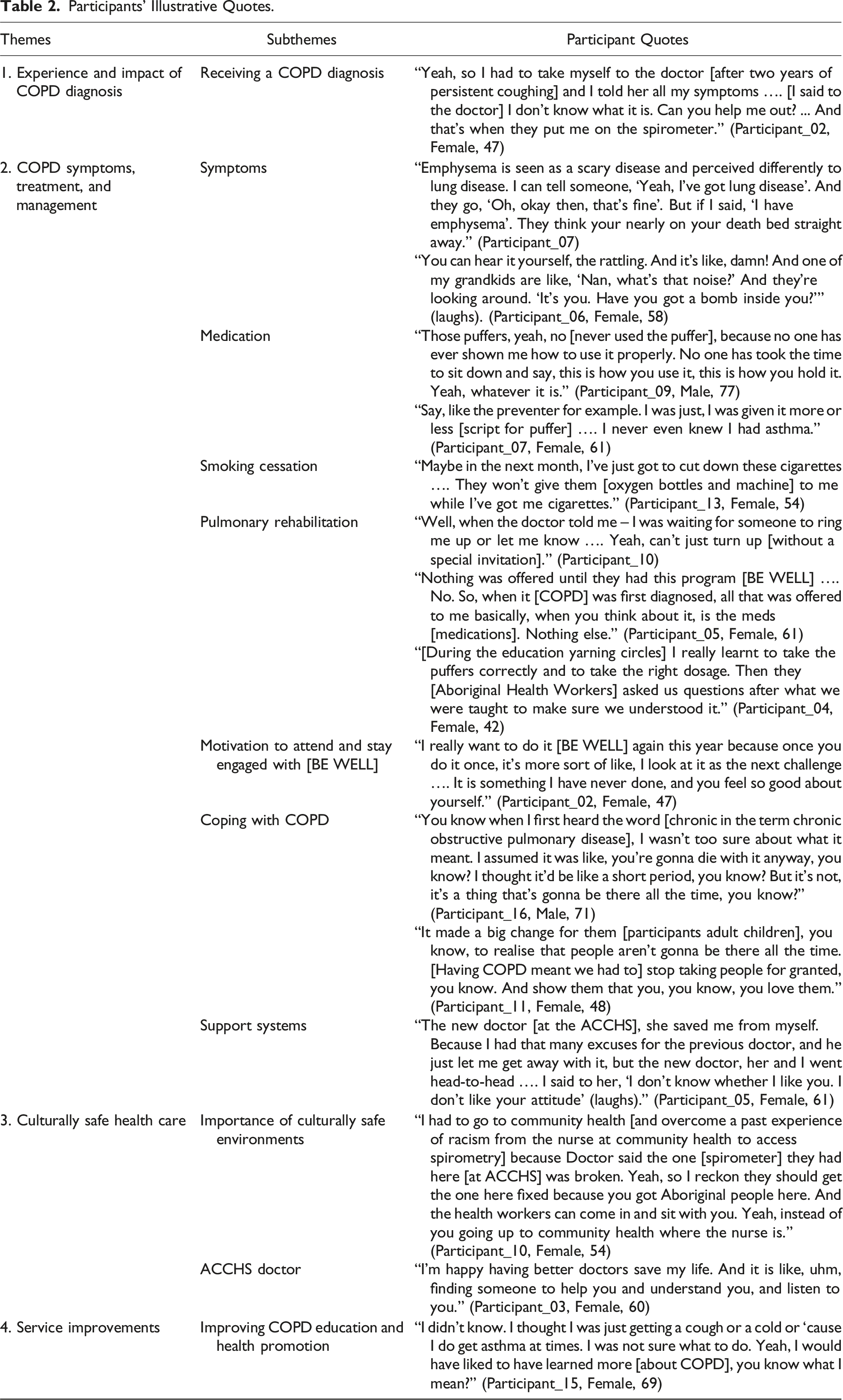
Participants’ Illustrative Quotes.
Theme 1: Experience and Impact of COPD Diagnosis
Receiving a COPD Diagnosis
Participants received a COPD diagnosis between 2 weeks and 10 years prior to this study. Nearly all were diagnosed by a doctor at their ACCHS, with three diagnosed during a hospital emergency department admission. Participants routinely reported delays seeking medical advice for their symptoms related to the fear and stigma of COPD, or emphysema (the more commonly used term), which is strongly associated with imminent death in Aboriginal communities. At the time of diagnosis, participants were symptomatic, including breathlessness, lethargy, fatigue, recurrent chest infections, limitations in daily physical activities such as walking to the letterbox, and a persistent chesty cough lasting several months or years before seeking medical attention. A subset of participants described experiencing severe COPD symptoms at the time of diagnosis including collapsing in public and a pneumothorax requiring resuscitation. Many wished that they had had an earlier COPD diagnosis. Many participants had previously been diagnosed with asthma, but later in life, when their inhaler medications seemed less effective, they received a COPD diagnosis.
Lack of Information About COPD
When receiving a COPD diagnosis, most participants recalled the doctor providing limited information. At diagnosis, pharmacological management was often implemented along with advice to stop smoking supported by smoking cessation products but almost no referrals to PR. Participants also described limited understanding of COPD and medications despite some of their family members having COPD. Additionally, some participants believed that COPD was hereditary because it had affected multiple generations within their family. Retention of information provided around the time of diagnosis was limited due to the association between COPD and death. As soon as he [Doctor] mentioned COPD and my lungs were worse. I was like well hell, I’m gonna die…. And I didn’t wanna die either. It was scary. And then nothing else registered. I was just thinking, I was gonna die. (Participant_06, Female, 58)
Emotional Impact of a COPD Diagnosis
Participants spoke of the intense emotional impact of receiving a COPD diagnosis. Feelings included “shame,” “shock,” “confusion,” “devastation,” “worry,” “sadness,” and being “scared” about what lay ahead, fearing social exclusion and isolation. Self-blame, guilt, and regret were common, particularly in relation to tobacco smoking. The fear for many stemmed from firsthand experience of witnessing older family members smoking, requiring oxygen, suffering, and dying with emphysema. One participant described memories of family members having COPD, making them adamant from an early age they would not follow the same path so were in shock when they received a diagnosis. Some still reported feeling helplessness because they believed nothing could be done.
Smoking and COPD
Participants spoke extensively about smoking and developing COPD. Smoking is the main cause of it, but you don’t realise until you really go to the doctor and get tested. (Participant_01, Female, 61)
Most were current smokers, commencing in their mid-teens or early adulthood commenting that smoking was common in their family. Many participants reported attempts to stop smoking and smoking at reduced levels, but some were not ready to stop. A couple of participants believed stopping smoking would result in an immediate reduction in COPD symptoms, severity, and progression. Others questioned the value of stopping because from their experiences stopping smoking made no difference to the outcome. Mum, she used to smoke, but then she gave it up. And she still ended up on the oxygen and everything, so that’s why you think, “Well... why bother?” (Participant_08)
Telling Others About Having COPD
Most participants revealed they had not shared their diagnosis with close or extended family or friends. Reasons included they did not want to “worry them,” be “a bother” or “a burden,” or get them “caught up” with COPD.
Sharing their COPD diagnosis with non-Aboriginal friends was associated with the fear of reinforcing racist stereotypes about Aboriginal peoples having “germs” and diseases. A participant expected her neighbourhood walking group would “scatter,” abandoning her because she had “something.” Some participants required several months to feel comfortable to share the diagnosis with family, often because of their difficulty accepting and/or explaining the diagnosis. No matter what you read, no matter what people say to you, you have to accept it before you can accept anybody else saying what they say. And it took me a long time to accept that I actually had COPD. (Participant_06, Female, 58)
Theme 2: COPD Symptoms, Treatment, and Management
Symptoms
Most participants reported symptoms of shortness of breath, coughing, and tiredness, stating “breathlessness is a struggle” and COPD had “slowed them down”. They believed symptoms were due to ageing, smoking, or a chest infection, but on reflection realised they had these symptoms for years.
COPD Education
Very few participants had received COPD education. There did not seem to be a relationship between the length of time since diagnosis and participants’ COPD knowledge. Current knowledge was limited to describing COPD as a lung disease, common symptoms experienced, and tobacco smoking had to be reduced or ceased. Several mentioned their preference for not wanting to know too much about COPD. I don’t want to know more because like I said, it’s sort of like, that’s when you get scared and things like that and I don’t want to be like that. I manage it through fitness, and I’ve cut my smoking right down. (Participant_07, Female, 61)
Medication
Participants reported benefits of puffer medications combined with pacing and breathing techniques for managing symptoms. Several spoke of good relationships with their doctor, who actively reviewed medications in line with changes in symptoms or severity and developed an Aboriginal chronic care management plan, enabling access to affordable medications. In these instances, doctors had explained how to take medications correctly. However, many spoke of instances where reasons for needing inhaler medication and how to use inhalers were not explained. Some reported having inhaler medication dispensed but not using it or giving the inhaler to others. Oh yes, I have a few [inhalers]. But like I said, I have seen people with lungs worse than me, and I gave it to them. (Participant_09, Male, 77)
Participants found it challenging to remember to take medication regularly as prescribed. Two described taking it only when they had noticeable symptoms, and another two would not use medication in public. I kept it [puffer] from everybody. Like, just my family knew. I didn’t want people to know that I had germs (COPD). (Participant_06, Female, 58)
Several highlighted the role of community pharmacists who spent considerable time providing education about the type, function, and correct use of medication using printed instructions with pictures. He [community pharmacist] knew I hadn’t been taking it either .… He knew it was all new. So, then he made sure that he had it all printed out for me and took me aside and explained it to me. And it was all awesome. So, I had no problems since then. (Participant_05, Female, 61)
Smoking Cessation
Doctors proactively engaged participants in conversations about stopping smoking and facilitated access to nicotine replacement therapy (NRT) and smoking cessation programs through the ACCHS. Many participants acknowledged support from ACCHS for reducing their tobacco consumption and COPD symptoms.
Participants mentioned frequent smoking cessation attempts using NRT, with some lasting several weeks or months and two had successfully stopped smoking. Reasons for continued smoking included stress management, living alone, and smoking for company. Some enjoyed smoking and were not ready to stop, or it was the only thing they did “wrong” or joked they needed one vice. Some wanted to stop smoking but felt the damage was already done.
Some mentioned that their decision to continue to smoke caused distress to family members and led to disputes, resulting in participants being defiant, despite acknowledging the need for family support to stop smoking. I thought, you [participant’s children] won’t tell me what to do. Yeah, so it was a bit of a battle there…. They said, “You would be wanting to give up smoking.” Like, Oh shame. (Participant_02, Female, 47)
Participants also reported confrontational discussions with doctors about the difficulty stopping smoking. Repeated conversations made participants feel frustrated, pestered, and resistant to medical advice. I haven’t stopped smoking. And he (Doctor) would pester me, pester me, and in the end, I said, “Look, I can only do one thing at once” …. Um, I ignored him. Well, I just kept adding the (puffers) sprays and made excuses. (Participant_05, Female, 61)
Pulmonary Rehabilitation
Most participants had only been offered medication to manage COPD, despite being diagnosed for several years. They were not aware of the availability or role of PR to manage COPD. Only two participants reported a previous referral to a local health district PR program, with only one completing two 8-week programs, which had increased their COPD knowledge and the use of exercise to manage symptoms. The other never attended PR due to timing of the program and limited public transport.
The BE WELL PR Program had recently commenced at three of the four ACCHS. Subsequently, roughly half the participants mentioned being referred by an ACCHS doctor and completed the program. Some had not heard about the BE WELL PR Program.
Several reflected on what helped overcome their initial resistance to starting BE WELL PR. It [exercise] was something I hadn’t done for a long time. I was thinking back, if you get me to move, you will start to feel good about yourself, like you know. I felt good. (Participant_02, Female, 47)
Participants frequently spoke positively about attending the BE WELL PR Program. They appreciated access to COPD information, exercising at their local ACCHS, an environment where participants felt safe and received support from other Aboriginal participants and staff. They reported improvements to COPD knowledge and self-management of symptoms, and in some instances reduced smoking. So, they don’t pressure me into giving up because they go, “No, you, you’re doing so many good things. Start there (with exercise), we’ll worry about that [smoking] later.” So, no pressure on it. I found I don’t smoke as much, and I breathe much better. (Participant_05, Female, 61)
Some highlighted attending the BE WELL PR Program gave them more energy and reduced breathlessness, allowing them to be more engaged in family activities. After completing BE WELL, one participant used a home exercise program and had a COPD Action Plan, so the family knew what to do in an emergency. As part of PR, participants enjoyed the COPD yarning circles led by Aboriginal health workers for providing group education and discussions using Aboriginal cultural approaches for learning and knowledge-sharing, aligned with Aboriginal cultural values of creating a space free from shame and judgement, and where connections with other Aboriginal participants were formed. Many had not discussed COPD with doctors or within their families or broader Aboriginal community; therefore, BE WELL allowed them to share their fears and challenges living with COPD in a way not previously experienced. That’s the same with me, I notice in some things people are like, they’re too shame or whatever but if you don’t talk about it [COPD here at BE WELL], you don’t get [to talk about COPD] anywhere. (Participant_12, Female, 47)
Exercising with other Aboriginal peoples living with COPD made participants feel physically better, increased social connectivity, and strengthened existing community bonds. Yeah, yes, we were really tight …. I knew that she [another BE WELL participant] had been where I was. She lived with it [COPD] for most of her life. So, she knew exactly where I was coming from, you know? (Participant_04, Female, 42)
Motivation to Attend and Stay Engaged With BE WELL
Participants shared positive experiences engaging with BE WELL staff who took a personal interest in them, ensured they exercised safely, and motivated them to stay engaged during the program through phone calls and arranging health appointments. Participants credited the collaborative, proactive, and committed approach of the referring doctor and BE WELL for their improvements in COPD management and wellbeing. Two participants joked the referring doctor had tricked them to attend BE WELL. When attending BE WELL, these participants experienced supportive and “lovely” staff and built personal connections with all participants. And she [referring doctor] made me come here [to BE WELL]. And that’s the best thing anyone ever did …. It’s just wonderful. And look, I lost all the weight, and I don’t smoke as much now. (Participant_05, Female, 61)
Several participants proudly revealed they attended all 16 sessions of the 8-week BE WELL program. Several wanted to re-attend the program as their next health goal or support new BE WELL participants on their COPD journey and encouraged other Aboriginal peoples in the community who may be feeling shame about COPD or attending BE WELL. It’s nothing to be shamed about COPD. We now have this good program and that helps …. Some of them would be feeling scared, but they will be with people dealing with the same feelings. It will help knowing what it [COPD] was to start with, learning you can live with it and knowing that it is manageable. (Participant_04, Female, 42)
Since the recent establishment of BE WELL, many reflected on their new appreciation of the role of exercise in relieving COPD symptoms and the benefit of exercising at the ACCHS with other Aboriginal peoples living with COPD. For some, making the decision to start exercising at BE WELL was a catalyst for change, reporting improved COPD management, healthy eating, weight loss, and reduced symptoms of breathlessness, coughing, and fatigue.
Recent Hospitalisation
Half the participants reported recent hospitalisations, one of which was COPD-related. Two participants experienced racism during their hospitalisations. These experiences left participants feeling hesitant about receiving health care as in-patients at hospitals and concerned about racially fuelled comments and interactions they might encounter during a hospital admission. I hate it [hospital]. It’s the last place I want to be …. I hear little comments, like when I first went to hospital there was this old lady across from me and she said, “Oh, we’ve got some dark blood in here.” Just little comments and that. (Participant_12, Female, 47)
Cultural Impact of COPD
Participants reflected on the impact of COPD on their lives, acknowledging complex experiences influenced by social and historical contexts. Interestingly, many had not previously contemplated the cultural impact of COPD and now recognised how COPD symptoms that limited their physical and emotional function affected their cultural roles and responsibilities, such as community connection, supporting family members, participating in Sorry Business (the grieving process when an Aboriginal person dies), and cultural responsibility to travel to their Country (the traditional lands of their ancestors). Being on their traditional Country was described as a “spiritually uplifting” experience, “being at peace,” and a sensation of their “lungs being full.”
Discussions about Aboriginal culture led participants to share their deep connection with family, cultural knowledges, and practices, emphasising the reciprocal relationship between Aboriginal culture and healing. They highlighted the connection to the metaphysical world and importance of breathing as a link to one’s Spirit, Country and Family. It’s like with your breathing, it is your spirit, and its why you got to keep on breathing, to be connecting with your family. (Participant_13, Female, 51)
Visiting local bushlands enhanced cultural connectivity and made their lungs feel better, enabling them to breathe easier. I give to the land. The land gives back to me. You can’t breathe? Go to the bush, it’ll give back to you because you have given to it. (Participant_13, Female, 51)
Traditional medicine was also discussed, including using eucalyptus leaves for relieving respiratory symptoms. An Aboriginal elder described the process of gathering, preparing, and utilising eucalyptus leaves and how other Aboriginal families from their Country use traditional practices for treating respiratory symptoms. You boil them up. Put them in a bowl and with the leaves soaking in there, it lets off the fumes of the eucalyptus tree. So, you put the towel over your head, and you just breathe in, and that relieves you. (Participant_14, Female, 61)
Coping With COPD
Due to the commonly held belief that COPD was a death sentence, challenges coping with the long-term condition were discussed. One participant described the distress and confusion misunderstanding the term “chronic” used by the doctor, believing it meant they would die shortly, leading to them having a “bad time” coping with COPD.
Psychological distress of the impact of COPD symptoms compounded participants’ ability to make positive COPD-related choices. Self-blame and shame were common amongst participants who attributed COPD to their smoking. Fatigue and tiredness challenged some participants to remain motivated to exercise and adhere to medications and self-manage COPD. They experienced stress and sadness over their reduced ability to fulfil caregiving responsibilities. Some shared concerns about COPD symptoms worsening and the future impact on their families. Those with severe COPD and heart failure reported panic attacks using oxygen in public and struggled to adjust to losing their driving license on health grounds, resulting in a significant loss of independence. For some, receiving the COPD diagnosis served as an opportunity for repairing family bonds, contributing to positive COPD outcomes.
Those who disclosed their COPD diagnosis to family members eventually found comfort in open discussions about its impact, enabling reflection and identification of negative behaviours. I started getting depressed and, you know, constantly thinking about, are they [participant’s children] all right, are they going to be all right. My youngest makes bad choices, so that’s the hardest thing. Yeah, so then I smoke more, don’t exercise, then I get sicker. I wouldn’t take my meds, so it’s a vicious circle. (Participant_05, Female, 61)
Support Systems
Participants highlighted the importance of social supports and close friendships to motivate them and achieve better personal progress in COPD management. A good network of friends, because they don’t know what is going on with you, but they are willing to learn …. I think having the support around you is what keeps you sane. (Participant_06, Female, 58)
Professional support from ACCHS doctors and staff was also valued, as it improved COPD management and facilitated access to respiratory physicians and the BE WELL program.
Theme 3: Culturally Safe Health Care
Proud of Their ACCHS
Participants consistently spoke of their family’s enduring association with and being proud of the local ACCHS in maintaining their own and the community’s health. Many valued the way ACCHS protect and care for them and enable Aboriginal peoples to self-determine the local health agenda based on community priorities. All were overtly positive and protective when discussing the range and quality of existing services and opportunities for improving COPD management. Participants also valued the availability of multi-disciplinary teams and integrated services enabling self-management, such as routinely accessing gym facilities at the ACCHS for health events or healthy lifestyle programs, often focussed on weight loss. All just fabulous, you know? It [local ACCHS] really makes you proud to be Aboriginal, you know, really. (Participant_16, Male, 71)
Importance of Culturally Safe Environments
Several participants spoke passionately about ACCHS providing culturally safe environments for Aboriginal peoples to access health care without fear of intimidation, where they are treated with kindness and respect and services incorporate their perspectives. They shared experiences of how they, their family, and the broader local Aboriginal community were historically mistreated, verbally and physically abused, and impacted by direct and institutional racism, which continues to impact access to mainstream health care. Some participants spoke broadly about Aboriginal peoples avoiding doctors, worried about being judged or treated differently than non-Aboriginal peoples. Participants also discussed the positive changes in Australia and their communities during their lifetime. You know, that, that you sort of come into these places here [ACCHS] and everyone treats you like a person. I think it’d be so cool if my mum would have been alive to come in there, sit in this waiting room and to be addressed as Mrs. [Surname] or [First Name]! (Participant_16, Male 71)
Staff Support Access to Health Care
ACCHS staff were described as friendly and helpful, who facilitated access to services and medical appointments and invited participants to join relevant health programs, which made them feel important and valued as a human being.
ACCHS Doctor
Participants were grateful for the care received from the ACCHS doctors and felt they were accessible and cared deeply for clients. However, regular changes in doctors impacted continuity of care, requiring additional time for participants to re-tell their story, build trust, and develop a meaningful relationship to enable them to openly share their health journey incorporating Aboriginal worldviews.
Participants reported attending the ACCHS for routine health check-ups which tended to focus on other chronic conditions and stopping smoking, rather than COPD. You don’t hear about much with lungs. I’m just saying that you don’t hear about it even when you go to the doctors, even for your monthly check-ups ... But there’s nothing about our lungs. It’s just diabetes, heart failure, kidneys and the liver. (Participant_01, Female, 61)
Theme 4: Service Improvements
Improving COPD Education and Health Promotion
Participants identified the importance of the ACCHS providing greater education around the time of diagnosis to combat the associated fear and confusion of COPD. They reported individual education could be conducted during health assessments when doctors are creating health plans. They suggested developing a COPD information package, explaining lung function, COPD symptoms, and how medications work, including visual resources and written information, with pictures of the lungs they could re-read later at home.
Participants reported health promotion initiatives need to be informative, practical, and realistic of Aboriginal peoples living with COPD in the community. They stressed not utilising extreme-based advertising techniques focused on severe symptoms or fear which may cause alarm or vilify Aboriginal peoples with COPD.
Group education was also reported as being effective to increase COPD knowledge but must be culturally centred, such as using Aboriginal yarning circles to guide discussion, and engage local Aboriginal community members to share their COPD journey. You might have something with a picture, you know, so they understand, and what you say, like, you got to connect it to culture. (Participant_02, Female, 47)
Participants thought existing ACCHS staff could be trained to deliver or support COPD services, such as increasing physical activity via walking groups and improving access to ACCHS gyms by locating these facilities on ground level.
More Discussions About the Lungs
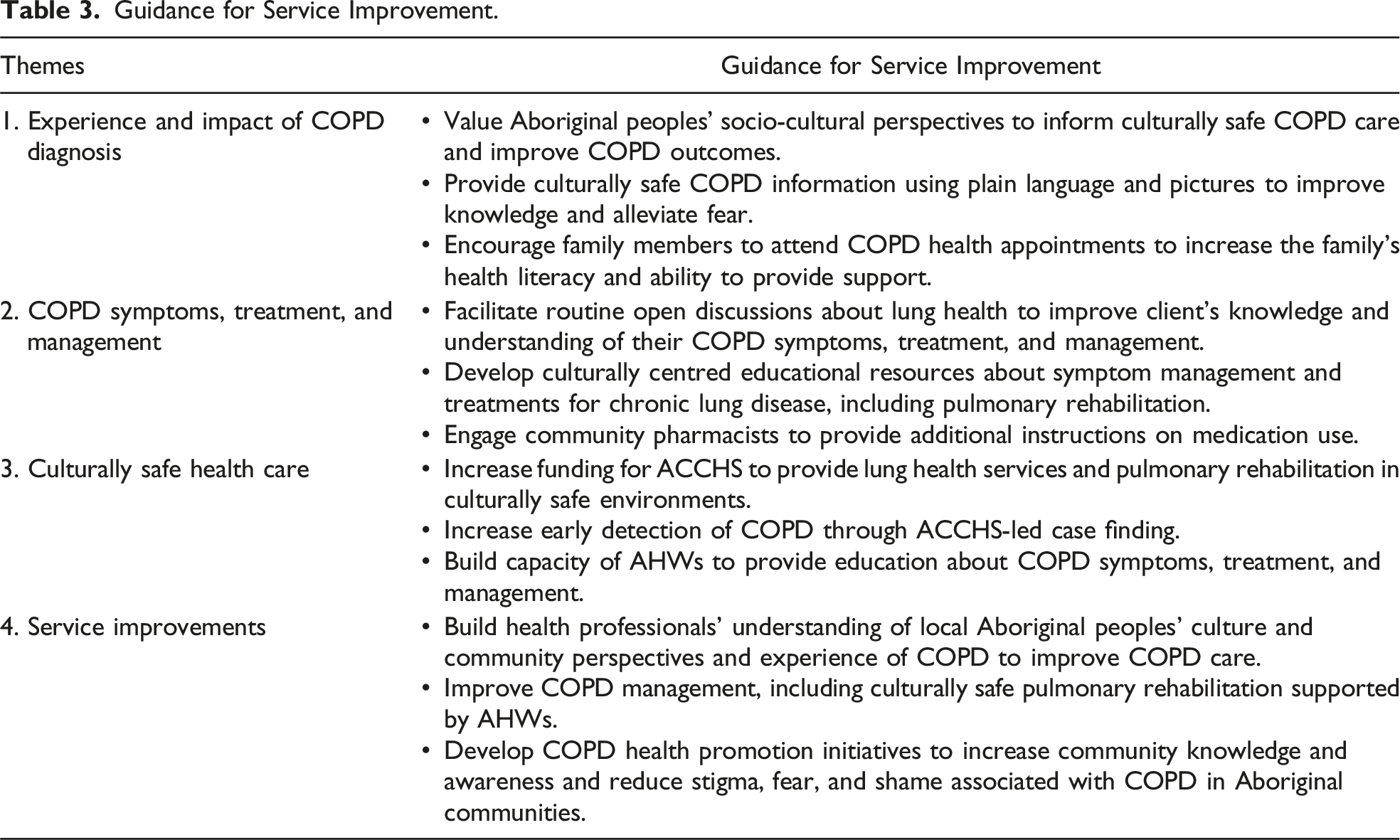
Guidance for Service Improvement.
Discussion
This qualitative study sought to understand Aboriginal peoples’ experiences living with COPD. The study examined participants’ journey from receiving a COPD diagnosis, COPD treatment and management, and engaging health care systems. Four themes emerged: (1) Experience and impact of COPD diagnosis; (2) COPD symptoms, treatment, and management; (3) Culturally safe health care; and (4) Service improvements. To the authors’ knowledge, this is the first study to conduct in-depth interviews with Aboriginal peoples living with COPD in Australia.
Diagnosis
Receiving a COPD diagnosis profoundly impacted the lives of participants who frequently held a fatalistic perspective of COPD, despite advancements in treatment and management (Dabscheck et al., 2022). However, this fatalistic perspective reflects their realities navigating COPD with limited knowledge and feelings of shame and stigma, and few opportunities to learn about COPD care, while processing the intergenerational trauma of COPD, amidst community misconceptions. Delays seeking a diagnosis and use of avoidance tactics were also reported in this and other studies about chronic conditions, resulting in missed opportunities for early intervention (Johnson et al., 2018; Rix et al., 2015). The absence of lung-focused discussions while accessing care revealed practical challenges managing multiple chronic conditions (Liddy et al., 2014). Exploring COPD from Aboriginal worldviews appropriately contextualises the condition within the broader Aboriginal lung health landscape, characterised by high morbidity and mortality rates, and a substantial burden of respiratory disease (AIHW, 2019; Heraganahally et al., 2019). Many aspects described about living with COPD are not unique to Aboriginal peoples, having been reported by other First Nation communities (Candy et al., 2020; Davey et al., 2014; Levack et al., 2016; Pal et al., 2022) and other peoples (de Sousa Pinto et al., 2013; Glenister et al., 2019; Madawala, Barton, et al., 2023; Madawala, Warren, et al., 2023); however, valuing the socio-cultural differences and realities presented provides insights to improve COPD care and outcomes (Henry et al., 2004).
Sharing Diagnosis
Participants often reported reluctance sharing the diagnosis with their family, resulting from the emotional impact of receiving a diagnosis (Miravitlles & Ribera, 2017), and having an insufficient COPD knowledge to explain the diagnosis. Reluctance to share the diagnosis was also grounded in the stigma of COPD within Aboriginal communities and the communal notion of shame reported by many Indigenous communities globally, which differs from individualist focus of colonial societies (Shaouli et al., 2016; Walker et al., 2017). Some also reported reluctance disclosing to non-Aboriginal peoples, concerned it may reinforce racist stereotypes that Aboriginal peoples have diseases (Aspin et al., 2012; LFA, 2022).
Framing of COPD
Engaging participants in deep discussions revealed how they perceived their relationship with COPD, crystalising the compounding burden of respiratory conditions and risk factors experienced by Aboriginal peoples across the life span. Interestingly, many participants used language that distanced connection between themselves and the condition, characterised by the absence of possessive nouns and adjectives, which differed when talking about heart disease, asthma, and asthma medication. COPD discussions were also intrinsically linked with asthma and smoking, with the high smoking rate amongst participants mirroring the high tobacco smoking prevalence in Aboriginal communities (Gould et al., 2014). Most valued the ACCHS smoking cessation programs and health promotion initiatives (Gould et al., 2014; Kennedy et al., 2023).
Culturally Safe Services – ACCHS
The cultural safety of ACCHS, grounded in Aboriginal ways of knowing, being, and doing, is seen as a major strength in the provision of health care (Panaretto et al., 2014; Sinka et al., 2021) and was identified by participants as a key factor in promoting trust and facilitating access to care aligned to Aboriginal peoples social and cultural needs and values (Aspin et al., 2012; NACCHO, 2022). Participants expressed immense pride and support for their local ACCHS and valued the establishment of an ACCHS-led PR program. Attending BE WELL was synonymous with participants increasing their COPD knowledge, overcoming shame associated with the condition, building COPD self-management skills, and accepting the COPD diagnosis, while also developing relationships with other Aboriginal peoples with COPD. BE WELL highlights the value of PR designed for Indigenous peoples to achieve measurable outcomes (Davey et al., 2014) and create culturally meaningful connections by learning and exercising together (Levack et al., 2016).
Improving COPD Services and Care
Participants suggested a range of COPD service improvements, which if implemented could transform existing COPD treatment and management to better reflect Aboriginal peoples’ community and cultural contexts and health care systems where Aboriginal peoples live and receive care (LFA, 2022; Meharg et al., 2020; Pal et al., 2022). Participants suggested initiatives to enhance early detection of COPD through ACCHS-led case finding. They also highlighted the need for COPD health education to reduce fear, confusion, and stigma especially around the time of diagnosis, while increasing community awareness of COPD and the low COPD health literacy within Aboriginal communities (Meharg et al., 2020; Pal et al., 2022), using Aboriginal methodologies such as yarning (Parter et al., 2019). The participants noted that other chronic conditions such as diabetes, cardiovascular disease, chronic kidney disease, and liver disease received greater attention during medical appointments and general discussion in Aboriginal communities. Addressing this imbalance through education and lung health service provision across the life span may improve COPD services and care.
Many mentioned gradually accepting COPD and better self-management of symptoms through the support provided by the ACCHS, attending BE WELL PR, and having access to COPD information. Based on their experiences, there is value increasing access to ACCHS-led PR that collaborates with the referring doctors and considers integrating smoking cessation programs and engaging community pharmacists (Fathima et al., 2021; Idowu et al., 2021).
Reflexivity
Participants shared their knowledge and experiences of COPD, often for the first time, while offering a wealth of contextual information about COPD and rich cultural differences describing this chronic condition within Aboriginal communities. To fully appreciate their perspectives requires acknowledging the historical, social, and cultural realities of Aboriginal peoples’ survival in Australia (Usher et al., 2021), further emphasising the importance of ACCHS delivering culturally centred and racism-free COPD health care. The participants’ trust enabled researchers to temporarily occupy the participants’ mindsets and lives. Non-Aboriginal researchers used reflexivity to transcend their own beliefs and embrace the worldviews of participants to guide data analysis and interpretation (Hyett et al., 2018). Participants’ perspectives remained central during data coding, analysis, and interpretation, which is fundamental when conducting thematic analysis (Braun & Clarke, 2012, 2019). Simultaneously, all researchers recognised the heavy cultural responsibility, obligation, and advocacy, stemming from exposure to participants’ unfiltered experiences (Eades et al., 2021; Hyett et al., 2018), which guided careful reflection and honouring individual and collective journeys living with COPD.
Strengths and Limitations
The strength of this study is that it is grounded in lived experiences of Aboriginal peoples with COPD, reflecting their voices and perspectives as participants. The inclusion of Aboriginal researchers during the design and analysis phase enhanced the research team’s understanding of Aboriginal cultural subtleties, enriching the depth, complexity, and meaning of the data. Interviews were conducted by two researchers (DM and JA) either face-to-face or via Zoom; however, further research is necessary to validate the impact of Zoom on the quality of data collection (Archibald et al., 2019). The use of Zoom during the COVID-19 pandemic when Aboriginal communities were particularly concerned about infection enabled researchers to conduct the interviews safely. In addition, three researchers (DM, JA, and SD) independently conducted the initial coding and a fourth (JMc) during data analysis and team discussions, increasing rigour.
Although the study included the lived experiences of Aboriginal peoples accessing COPD care from four diverse regional and rural NSW-based ACCHS, findings may not be generalisable to other ACCHS or Aboriginal communities in Australia.
Conclusion
Aboriginal peoples in Australia experience a high prevalence of COPD, compounded by limited COPD health literacy and poor access to comprehensive culturally safe management, such as PR programs. Aboriginal peoples’ lived experiences have provided a clearer understanding and appreciation of the complexities of the Aboriginal lung health landscape and the needs of Aboriginal peoples with COPD. These perspectives offer vital insights and importance of clear culturally centred COPD information following a diagnosis and ongoing management approaches that build health literacy, develop self-acceptance of COPD, and incorporate family for ongoing support. The respectful use of Aboriginal research methodologies and partnering with ACCHS to authentically engage Aboriginal peoples has informed the exploration of COPD from Aboriginal perspectives. Investment in ACCHS is vital to ensure the sector is appropriately resourced, and staff are trained to deliver comprehensive evidence-based COPD management, incorporating PR. The new insights from this study may lead to improvements in delivering culturally safe COPD management, incorporating PR programs, and educational resources designed with Aboriginal peoples for the Aboriginal health sector.
Supplemental Material
Supplemental Material - A Qualitative Study of Aboriginal Peoples’ Health Care Experiences With Chronic Obstructive Pulmonary Disease
Supplemental Material for A Qualitative Study of Aboriginal Peoples’ Health Care Experiences With Chronic Obstructive Pulmonary Disease by David P. Meharg, Sarah M. Dennis, Justin McNab, Kylie G. Gwynne, Christine R. Jenkins, Graeme P. Maguire, Stephen Jan, Tim Shaw, Zoe McKeough, Boe Rambaldini, Vanessa Lee, Debbie McCowen, Jamie Newman, Hayley Longbottom, Sandra Eades, and Jennifer A. Alison in Qualitative Health Research
Supplemental Material
Supplemental Material - A Qualitative Study of Aboriginal Peoples’ Health Care Experiences With Chronic Obstructive Pulmonary Disease
Supplemental Material for A Qualitative Study of Aboriginal Peoples’ Health Care Experiences With Chronic Obstructive Pulmonary Disease by David P. Meharg, Sarah M. Dennis, Justin McNab, Kylie G. Gwynne, Christine R. Jenkins, Graeme P. Maguire, Stephen Jan, Tim Shaw, Zoe McKeough, Boe Rambaldini, Vanessa Lee, Debbie McCowen, Jamie Newman, Hayley Longbottom, Sandra Eades, and Jennifer A. Alison in Qualitative Health Research
Footnotes
Acknowledgments
We would like to acknowledge the participants who invested their time and knowledge and shared their personal experiences for this study. We also acknowledge the Aboriginal Community Controlled Health Services and staff, in particular Jye Stokes, Leeny Kemp, Kalinda Wills, Willow Firth, and Zara Crawford for their advice and support for this study.
Author Contributions
JA and DM conceived the study, and JA, DM, SD, JMc, KG, CJ, GM, SJ, TS, ZM, BR, VL, DMc, JN, HL, and SE contributed to aspects of the study design. JA and DM conducted participant interviews. JA, DM, SD, and JMc analysed and interpreted participant qualitative data. BR, VL, JN, HL, SE, and DM provided an Aboriginal and/or Torres Strait Islander perspective to the study design. All authors read and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a National Health & Medical Research Council Australia, Global Alliance for Chronic Disease grant (1116081).
Ethical Statement
Data Availability Statement
The data are not publicly available due to them containing information that could compromise research participant privacy and consent. Materials supporting this study are available as supplementary information files.
Supplemental Material
Supplemental material for this article isavailable online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.