
Abstract
Shadowing is a research method that combines observing events and short on-the-go interviews to investigate people’s roles and behaviours in various settings. Even though it is not a widely used method in architectural research, it can be adapted to focus on the interaction of individuals with the built environment. This is especially important in healthcare environments, where people are vulnerable and more dependent on their surroundings. In this article, I reflect on the experience of adapting and using the shadowing method to explore stroke inpatients’ interactions with the built environment during their recovery in rehabilitation centres. This research study was the first to employ shadowing in the stroke patient population on such a large scale. One day (12 consecutive hours) was spent with each of the 70 participating stroke inpatients, recording their interactions with the built environment in different forms – on the floor plans, as narrative descriptions, creating sketches of situations and noting down patients’ remarks. This method was useful in capturing the built environment’s role in patients’ daily experiences in rehabilitation centres. Research in healthcare facilities includes various challenges, and close contact with the patient population of older adults with stroke introduces numerous unexpected events and ethical dilemmas in the field. At the same time, this method provides research insights that would otherwise be unobtainable. Researchers are given practical information and recommendations on how to prepare for using shadowing for architectural research and what to expect in the field.
Keywords
Introduction
Shadowing entails closely observing events as they occur during everyday activities (Meunier & Vasquez, 2008). One of the main values of this method lies in “closely following a subject over a period of time to investigate what people actually do in the course of their everyday lives, not what their roles dictate of them” (Quinlan, 2008, p. 1480). Shadowing allows the researcher to both observe the event and assess what it means to the shadowed person by combining debriefing sessions and short, on-the-go interviews in which the participant is asked to explain or reflect on particular events or behaviours (van der Weele & Bredewold, 2021). Thus, shadowing entails a structured observation that gathers behaviours and personal views, resulting in ‘rich, thick descriptive data’ (Quinlan, 2008).
Overview of Shadowing as a Research Method
McDonald (2005) distinguishes three unique goals of shadowing: (1) experiential learning, (2) behaviour recording, and (3) in-depth qualitative understanding of roles or perspectives. Each of these goals requires a distinct approach. The first goal (experiential learning) relates to ‘job shadowing’; for example, nurses and trainee teachers frequently shadow a more experienced professional to understand how things should be done in the workplace (Gilliat-Ray, 2011). Because of the widespread use of ‘job shadowing’ in many industries and a lack of critical examination of the shadowing technique, there are numerous misconceptions regarding shadowing as a scientific research method (Bartkowiak-Theron & Robyn Sappey, 2012). In scientific research, shadowing is used for recording behaviour and exploring roles in an in-depth qualitative way. When conceptualising shadowing studies, researchers from different disciplines have often drawn inspiration from sociology and anthropology, which pioneered various observation-based methods (McDonald & Simpson, 2014). Within the larger group of observational methods, shadowing could be characterised as continuous participant observation without using a structured data collection form (Lipson-Smith & McLaughlan, 2022), with the addition of occasional interactions with the observed persons in the form of quick on-the-go interviews.
One of the main strengths of the shadowing method is that the collected data “are grounded in actual events rather than reconstructions of previously occurring events” (Quinlan, 2008, p. 1482). McDonald also acknowledges that “shadowing activity will be as various and complex as the job of the individual the shadower is investigating” (2005, p. 456). It can, therefore, be a highly flexible method adapted to different contexts, participants, and research questions (van der Weele & Bredewold, 2021). The amount of time spent together requires a significant investment of time and energy for both the shadower and the shadowed person (van der Weele & Bredewold, 2021) since shadowing a single person might span from a single shift to an entire month or even longer (McDonald, 2005).
Shadowing in Health Services
The healthcare system is complex, with a growing gap between clinical outcomes, patient experiences, and actual cost (O’Brien et al., 2018). Spatial observation methods are frequently used in healthcare environment research to examine the behaviours and experiences of different user groups (Lipson-Smith & McLaughlan, 2022). Shadowing, as one of the observational methods, also has a different tradition – it has long been used in medical, nursing, and other health professions to educate prospective employees or train them for a position in the form of ‘job shadowing’ (Kitsis, 2011; McDonald, 2005; McDonald & Simpson, 2014; Stoeckle et al., 1993), while its use as a research method has grown in popularity in recent years. Despite this increasing interest in patient shadowing and the existence of some guidelines for good practice, there is still a lack of detailed evaluation of its practical, methodological, and ethical challenges (Liberati, 2017).
During patient shadowing in health services, an empathetic observer follows patients across various care experiences while recording information gathered through observations (Shaw et al., 2014). Thus, shadowing enables ethnographic observation of various stages and touchpoints in the care process (Gallan et al., 2021). It is a valuable method in healthcare environments as it allows for real-time feedback from patients (and family members) about their experiences while receiving care (DiGioia et al., 2011). These insights can be invaluable for identifying inefficiencies and understanding where improvements are needed from the patient’s point of view (O’Brien et al., 2018).
Some applications of the shadowing method in health services are presented to illustrate its versatility. Van der Meide et al. (2015) adopted a phenomenological embodied enquiry design using the shadowing method to explore the experiences of a single older patient during hospitalisation. Multiple days were spent with this patient in a hospital, and the researcher attempted to document as much of the unfolding events as possible. In another example, eight patients undergoing hip or knee surgery were shadowed from hospital admission until discharge to explore patient experiences through the hospital journey and how it can be captured (Gualandi et al., 2019). In the van der Weele and Bredewold (2021) study, on the other hand, assisted living facility residents with intellectual disabilities were shadowed for 1 or 2 days at a sheltered living institution to explore the experiences of dependency in their everyday lives. Calvert et al. (2015) focused on medical students observing patients at care experience touchpoints to offer input for organisational quality improvement, while DiGioia et al. (2010) incorporated shadowing into a larger group of methods (including care flow mapping, patient storytelling, and patient surveys) conducted by caregivers to improve patient- and family-centred care. These examples demonstrate a variety of scales, settings, participants, and research aims to which the shadowing method was applied, all with a focus on health services.
Shadowing With a Focus on the Built Environment and Patients
While numerous studies using observation-based methods show the tendency to record behaviours and sort them into categories, capturing and documenting the essential aspects of the built environment is much more challenging (Lipson-Smith & McLaughlan, 2022).
In a shadowing study aiming to assess the experiences of patients and their families during the joint replacement care procedure, the environment was identified as one of five main aspects affecting patient experiences (Marcus-Aiyeku et al., 2015), with a very brief and general description of the environment. Goodrich et al. (2020) found that the physical environment and relational care were the two key characteristics of the care environment that healthcare staff participants observed while shadowing patients in various end-of-life settings. Only several brief examples of the elements in the built environment are provided. Gallan et al. (2021) discovered that the physical environment was one of the factors influencing patients’ comfort and experience, most notably in frequent navigation issues in the facility while documenting patient experiences in an outpatient family medicine clinic. The wayfinding challenge was briefly described as being unable to navigate from the back area to the door to the check-out desk (Gallan et al., 2021).
Even though these studies were conducted in healthcare environments, they focused primarily on general health services. The built environment is (an accidental) part of the results rather than part of the research question; the mentions of the built environment in the findings are also fragmented and limited to short and non-specific descriptions. Furthermore, visual maps (such as floor plans) are also not a part of the reported findings, making it challenging to situate the discussed experiences spatially. Nonetheless, the findings of the mentioned studies emphasise the importance of the built environment in the patient experience. Investigating how patients interact with the physical environment of healthcare facilities is essential as patients, especially older adults, are often in a vulnerable health state, making them more dependent on the built environment, which in turn has a greater impact on them (Lawton & Simon, 1968). Motor, cognitive, and other impairments experienced during their stay in healthcare facilities affect how they interact with the built environments and what challenges they encounter when moving through space. Research focus on the built environment helps actors involved in planning healthcare facilities to identify what can be improved in the design of these environments, and not just medical care provision, as the main aim of other shadowing research in healthcare. Consequently, methodologies for studying this relationship are continuously being broadened.
A recent review of the studies using the shadowing method to study the relationship between behaviour and the built environments in healthcare settings found that this method was not well-defined (Kevdzija, 2022a), contributing to general misunderstandings surrounding the method. This article aims to advance the understanding of shadowing as a research method that can be adapted and employed to study how various patient groups in healthcare facilities interact with the built environment and how this environment could be improved to enhance their experiences. To illustrate this, I draw on my experiences shadowing stroke patients during rehabilitation. Based on these experiences, the lessons learned and the implications of using patient shadowing in architectural research are presented, addressing the gap in the current body of literature. This article focuses on methodological reflections, while the results have been published elsewhere (some of the related publications: Kevdzija, 2022b; Kevdzija et al., 2022).
Research Outline: Shadowing Stroke Patients in Rehabilitation Centres
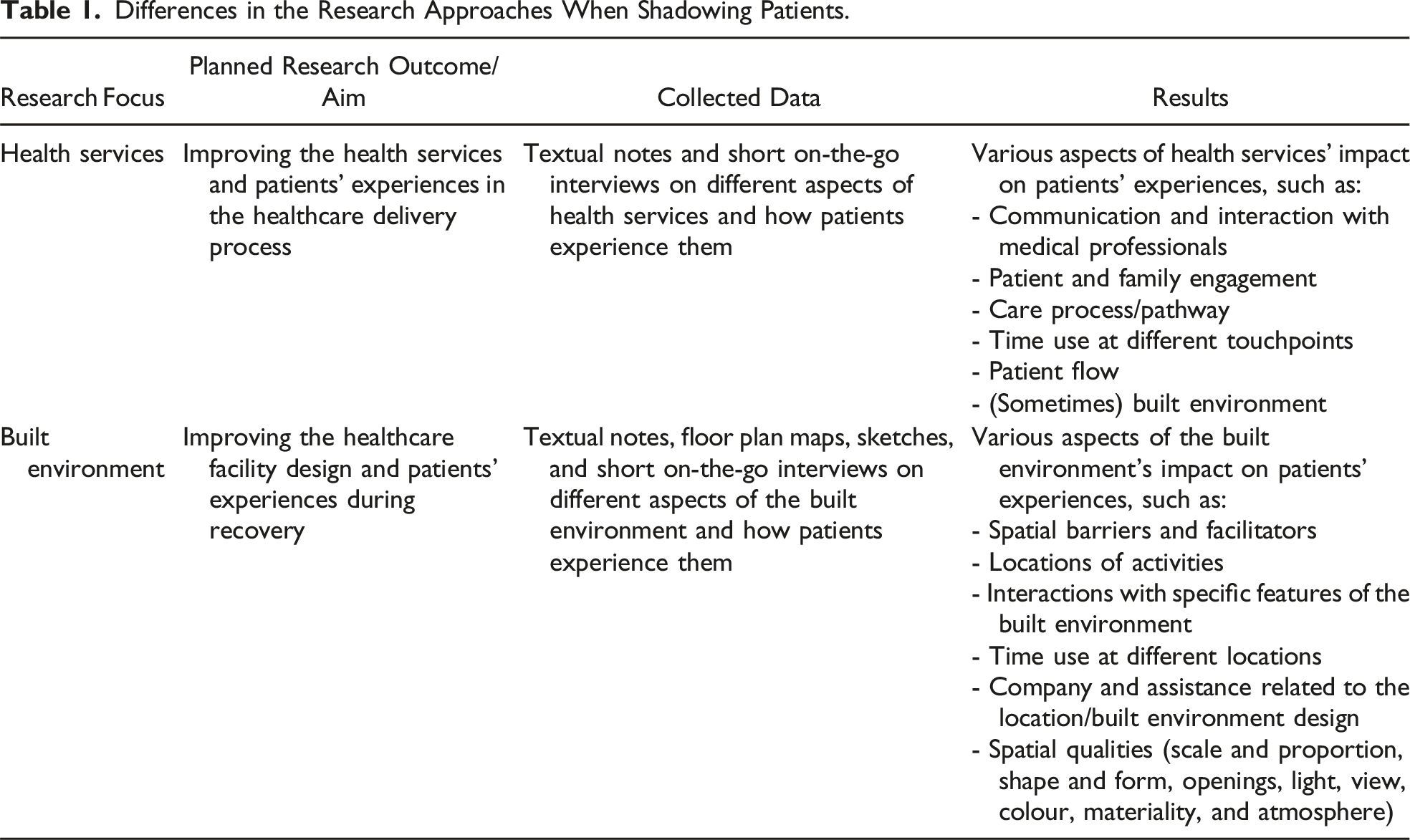
Differences in the Research Approaches When Shadowing Patients.
The Motivation Behind the Methodological Choice
The research question guiding this study was: ‘How does the built environment of rehabilitation centres hinder or support the independent mobility of stroke patients?’ Shadowing, combined with patient and staff surveys, was selected as the primary research method to examine the role of built environment features in patients’ daily activities for several reasons: (1) Focus on the individual: Shadowing allows researchers to explore what individual patients do between official sessions (therapies and other appointments), where they choose to go, and how they explain their activities (McDonald & Simpson, 2014). It is advantageous for research with stroke patients since it enables the researcher to adapt to each patient’s pace and capacities (van der Meide et al., 2013). (2) Richness of data: The shadowing method is not used to validate a hypothesis but to collect a thick descriptive layer of data to be explored (Quinlan, 2008). This method is recommended by ethnographers when the time–space dynamics of the activities at hand are too complex to capture using more conventional forms of static observation (Czarniawska, 2007). (3) More representative sample: Instead of focusing on participants’ limitations, shadowing allows them to also express themselves through actions and reactions, which helps to gain insights into experiences of the built environment they might be unable to describe or recall verbally (van der Weele & Bredewold, 2021). This enables the inclusion of stroke patients with speech impairments who are often excluded from research.
Access to Healthcare Facilities and Recruiting Participants
Eleven out of 56 contacted rehabilitation centres in Germany agreed to be visited, and all were visited during this initial research stage. A staff member at each visited centre gave a tour of the facility. After this initial visit, seven centres agreed to participate in the study. In the following steps, ethical approval was obtained from the Ethical Committee at the Technische Universität Dresden (approval number: EK 452102016), floor plans were gathered from each centre, and the documents were prepared for the field study (patient information sheets, floor plan sheets, consent forms, etc.).
Considering each patient’s physical and mental health and the pre-established inclusion and exclusion criteria, the medical staff chose 10 patients per centre. Patients who had a stroke, who could move independently (with or without using a wheelchair or walker), and who were capable of consenting and gave their consent were included in the study. A staff member known to the potential study participants approached them with the researcher (author); typically, when alone in their rooms, patients were then given a brief explanation of the study and asked to participate. If the patient was interested, they were given a large print consent form and an information sheet. On that occasion, the observation day was also scheduled. In total, 70 patients were included in the study.
How Shadowing Was Used
It is essential to recognise the large volume of data that can be captured using shadowing, even in a short period (McDonald, 2005). This is due to every shadowing session recording at least the following data: activity, start and end time, location, and activity notes (Nanda & Wingler, 2020). This study adopted the shadowing method to record patients’ daily routes and interactions with space during an ordinary rehabilitation day. Due to the nature of shadowing (an individual carefully following a subject for an extended period) and due to ethical considerations (asking for consent), the researcher could not remain a completely secret observer. As a result, the Hawthorne effect may have impacted the participants’ behaviour. The study’s objectives were not disclosed to patients; they were only informed that their regular daily routes in the centre were being observed to reduce this impact.
Duration
Each patient was observed for around 12 hours on a typical rehabilitation day in the centre, and the observation times differed somewhat between centres due to different meal times (Figure 1). The typical meal times are presented in 2-hour time frames since patients were usually given a time window when the meal was available and went when it was convenient for them. Shadowing usually began shortly before patients’ breakfast and ended soon after dinner. The patient was asked about their plans after dinner, and the shadowing session ended if they withdrew to their room. The observation was prolonged if the patient planned to engage in another activity. This shadowing timeframe was selected to capture most of their movement and interactions with the built environment on a usual day in rehabilitation. The total observation time in all centres exceeded 840 hours. Usual daily schedule in the participating rehabilitation centres.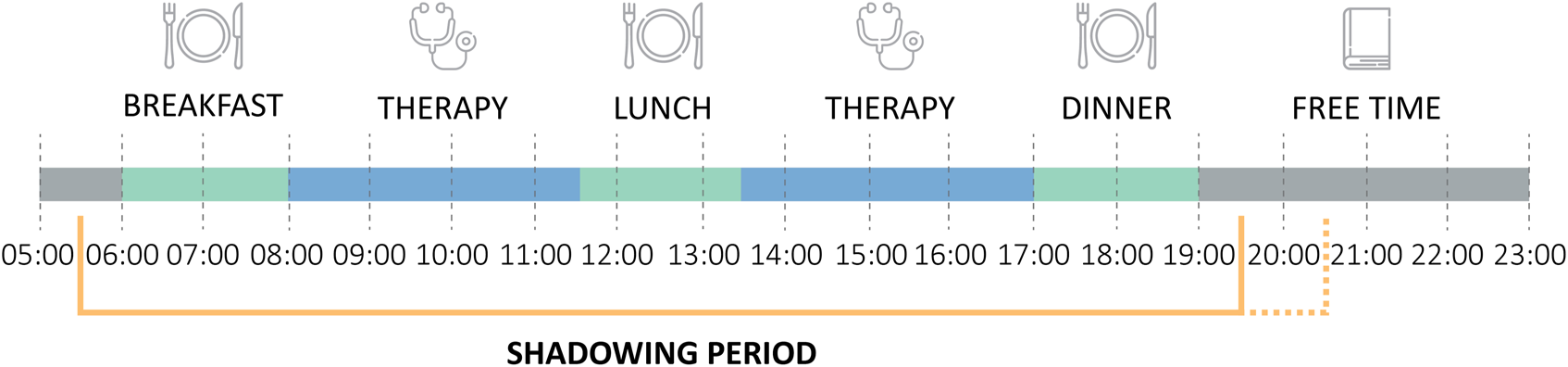
Defining What Will Be Recorded
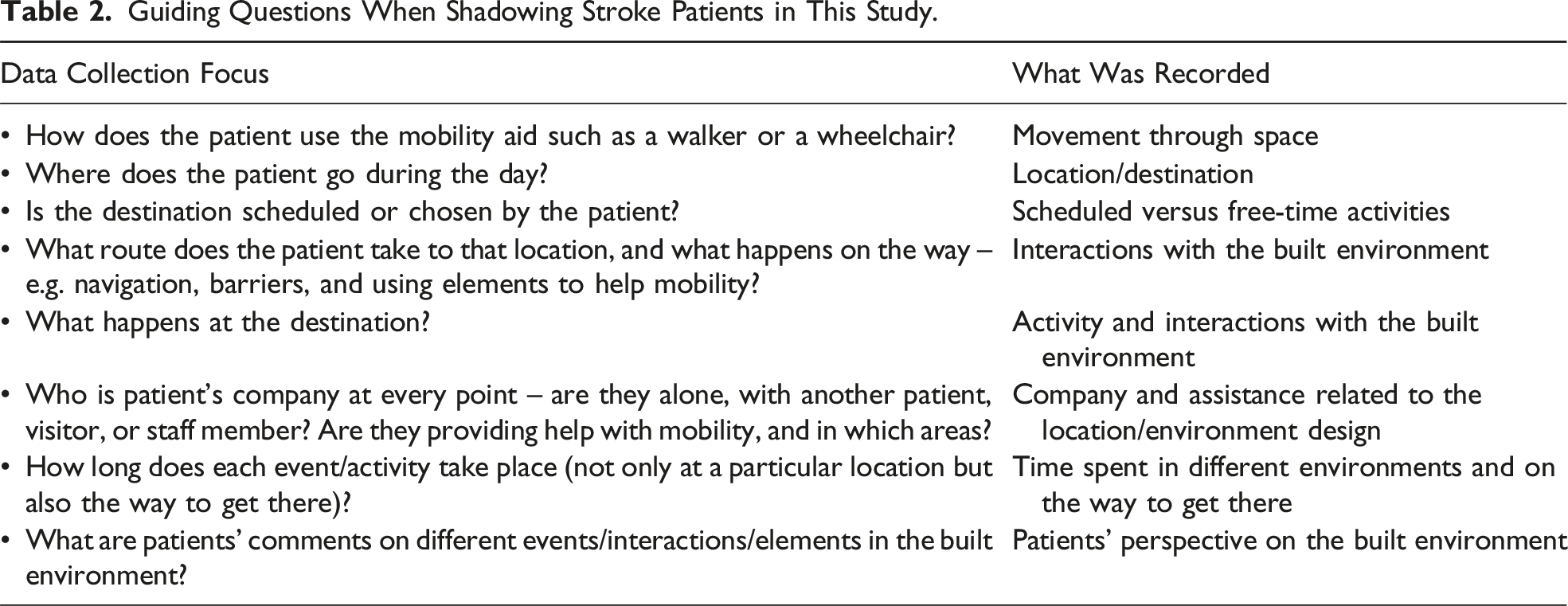
Guiding Questions When Shadowing Stroke Patients in This Study.
Interactions With the Built Environment
The routes of patients in the centres were recorded on previously prepared and printed sheets with building floor plans, with an additional sheet for the activity time log. This strategy enabled precise mapping of patient locations, the nature of their routes, and all the built environment elements they interacted with (as a mobility barrier or facilitator). An example of a recording of a single patient’s routes on the floor plans during one observation day is shown in Figure 2. An example of a single patient’s recorded routes during the observation day.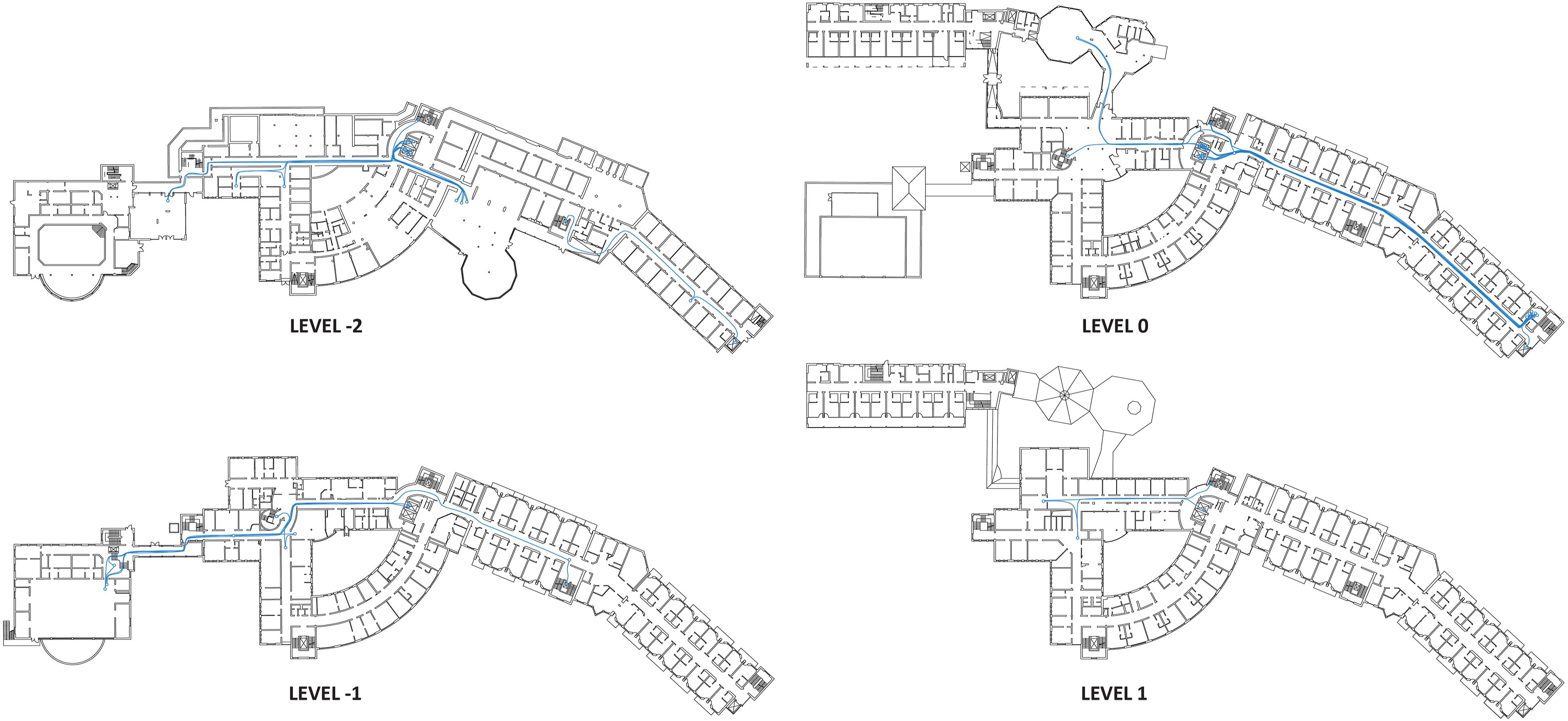
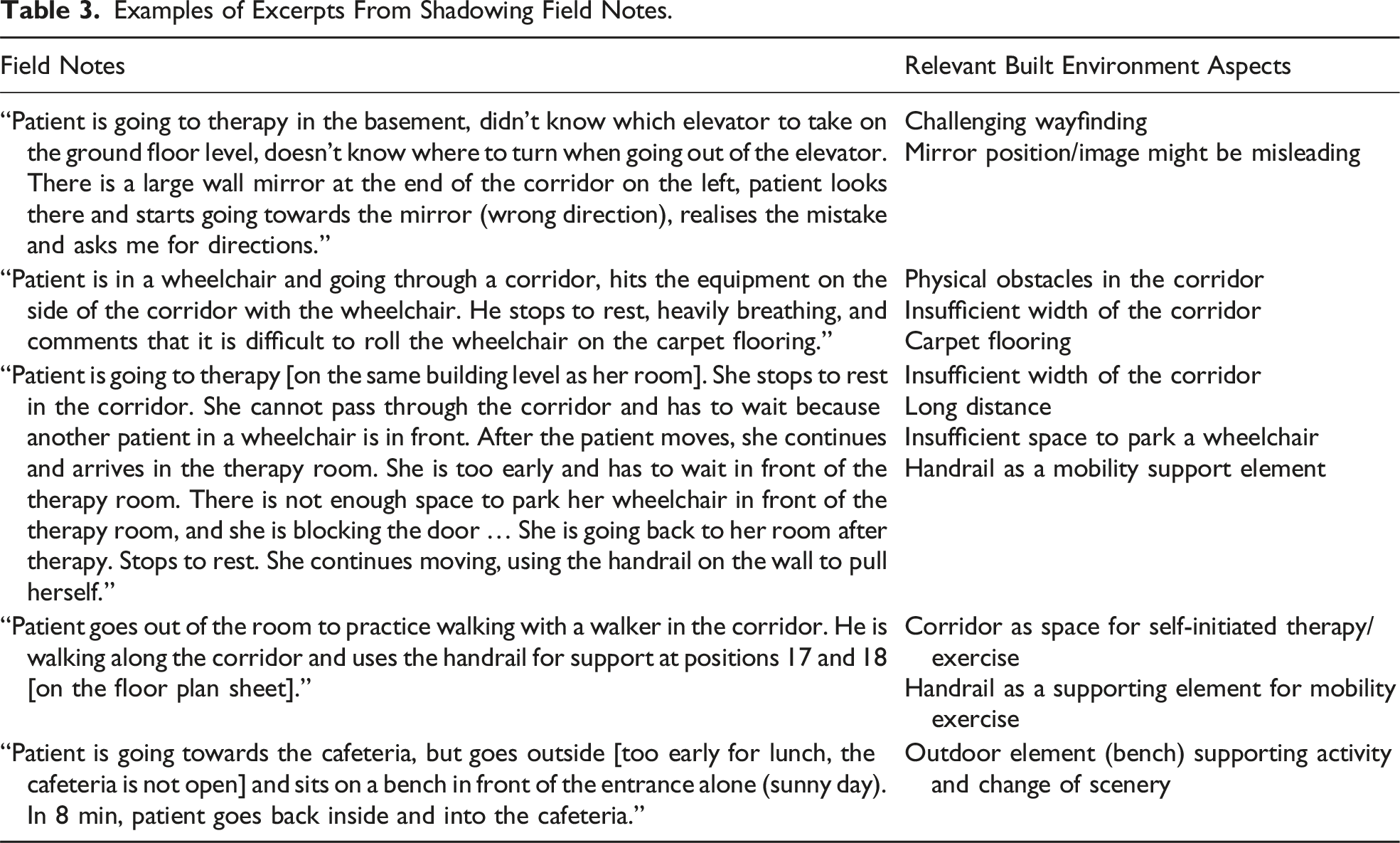
Examples of Excerpts From Shadowing Field Notes.
How Building Floor Plans Were Used During Data Collection and Analysis
The distinctiveness of this research study compared to previous shadowing studies in health services is the research question, which focuses on the built environment and its role in hindering and supporting the independent mobility of stroke patients in rehabilitation centres. That is why, besides the usual textual notations and two- and three-dimensional sketches, floor plans were used to map participants’ routes through the building and specific points of interest where important interactions with the built environment occurred. This section outlines how floor plans were used in this study, with illustrated examples in Figures 3 and 4. It is important to note that the data collected on the floor plans were used together with typically collected textual shadowing notes. Routes of a patient whose room was on the same floor as the therapy area were selected for this illustration, as this involves only a single floor plan (one building level). This patient was using a wheelchair for mobility. Most other patients were mobile throughout the whole building (regardless of the mobility aid they used), and their daily routes spanned multiple building floors. How building floor plans were used during the data analysis process—individual patients (the floor plan was cropped to the area used by the shadowed patient). How building floor plans were used during the data analysis process—all patients.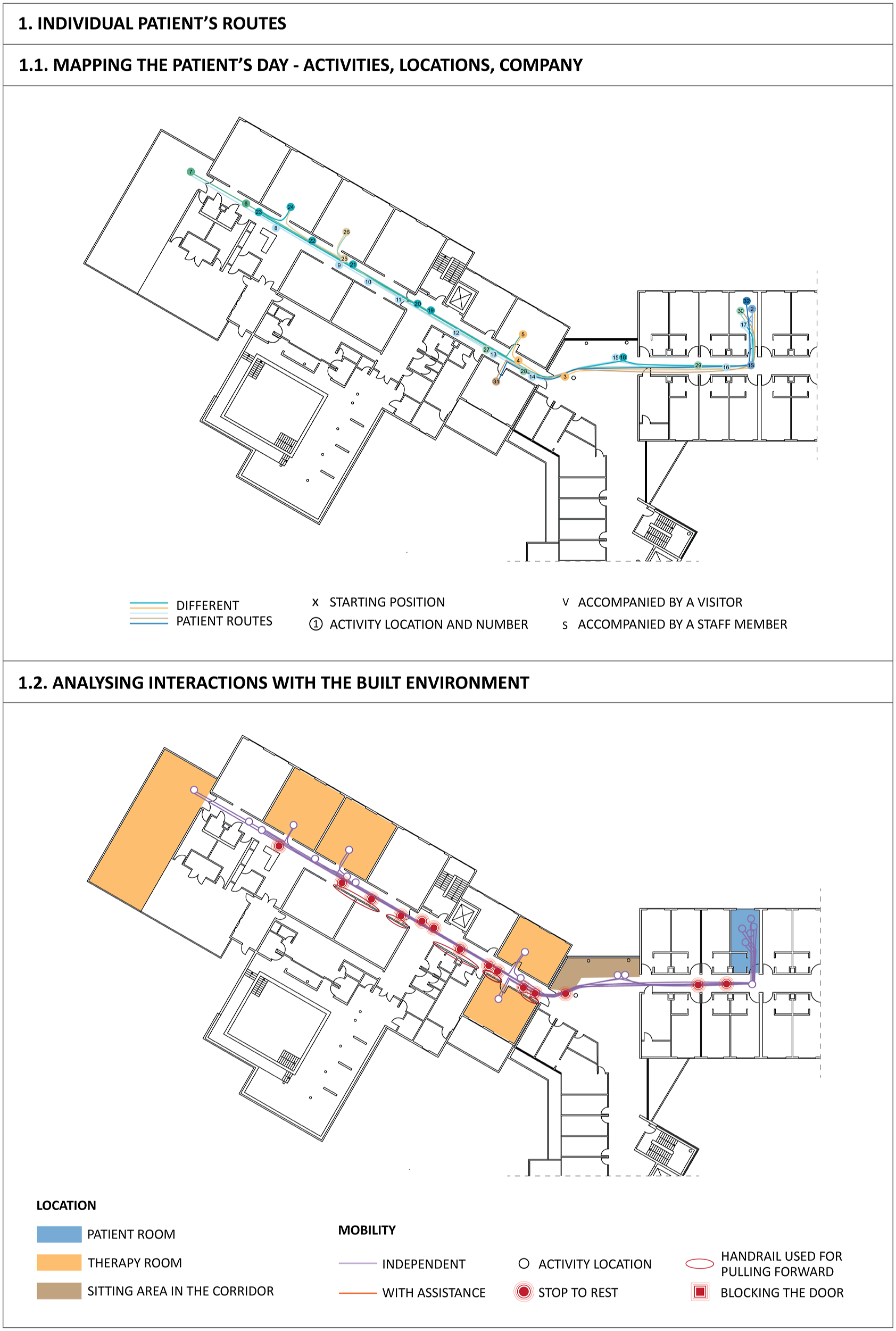
The paper data were digitalised using the Autodesk AutoCAD software in the first step. The first map was the direct copy of the paper data, showing patients’ routes in the building, the locations of patients’ activities, a number for each activity (for connecting it to the time log sheet and the textual notes), and the symbol for patients’ company (i.e. visitor and staff member) (Figure 3). With the help of textual notes and sketches taken during shadowing, another map was created (Figure 3, 1.2), showing the spaces the patient visited during the day and all notable interactions with the built environment. This approach enabled an understanding of the individual patients’ travel through space on the shadowing day and how the built environment might have supported or hindered their independent mobility.
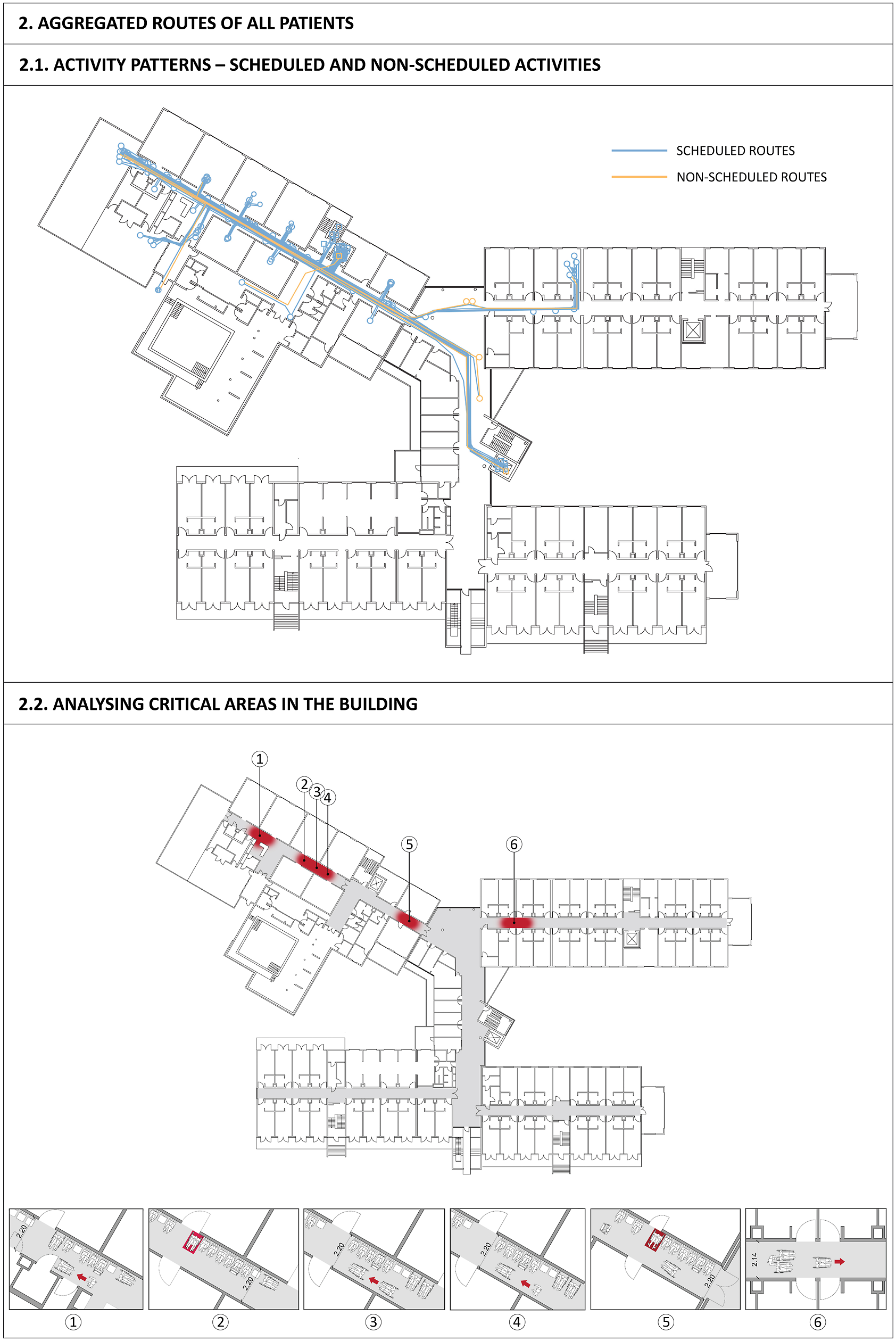
In the next step, routes of all patients from the same rehabilitation centre were placed on the floor plans of that centre. When routes of all patients were aggregated on the floor plans of one clinic, this allowed for examining the patterns of activities and their locations (scheduled vs. non-scheduled), as well as the time used in these locations (in combination with the time log sheet) and distances that patients covered (by measuring the routes) (Figure 4). Furthermore, this permitted the detection of critical areas in the building by examining different situations encountered by patients in, for example, a specific corridor. This analysis was only possible in combination with textual notes and sketches taken during shadowing. The illustrated example (Figure 4) shows the issues with the corridor dimensions (width and parking space for a wheelchair) that different patients encountered in the therapy area.
Experiences in the Field
The following section introduces some situations and challenges encountered during data collection in seven rehabilitation centres. Even though extensive preparation was done before the fieldwork, these situations were somewhat unexpected and could help other researchers prepare their shadowing research study in healthcare environments. A degree of flexibility needs to be ensured throughout the data collection process to overcome unforeseen situations and maintain methodological commitments (Quinlan, 2008).
Unexpected Observations of Patients’ Interactions With the Built Environment
Many surprising interactions of patients with the built environment were observed during shadowing, and some of them are illustrated here. When recruited, patients were sorted into mobility categories based on the mobility aid they used (wheelchair, walker, and independently walking). During shadowing, it was observed that they sometimes changed the mobility aid during the day – for example, a patient switched from a walker to a wheelchair at the end of the day because he was exhausted. It was then observed that the patient’s interactions with the built environment completely changed – elements that were not a barrier before now became a barrier and vice versa. Additionally, some spatial elements were interacted with in unusual ways, for example, one patient in a wheelchair used a handrail to pull themselves forward along the whole 50-metre long corridor multiple times in one day. Several patients were observed changing direction and rolling (or ‘walking’) their wheelchairs backwards on the carpet flooring, ramps, and slopes. Patients with walkers often experienced heavy doors as barriers because the walker would make it challenging to manoeuvre opening the doors. Walkers would also be used as seats that could be placed anywhere, creating opportunities for patients to rest on the way or gather and stay in any area inside or outside of the building. Furthermore, patients created informal gathering spaces in corridors, which became hubs for different activities – from self-initiated exercise to socialising.
Misinterpreting the Researcher’s Role and Data Collection Disruptions
On several occasions, patients I shadowed had mistaken me for a care staff member. They would ask me to push their wheelchair, enter their room to help them find their glasses, or pour coffee. These situations made it difficult to keep a strict division between the role of the shadower and the role of someone who can help. As these were minor tasks, I often did them if they didn’t interfere with patients’ privacy and safety. It is unclear whether this confusion was due to the type of care setting, my wearing usual clothes without a name tag, patients’ advanced age, or another underlying condition. Even though role confusion was expected to some extent and measures were taken to mitigate this, for example, I was introduced to each participant before shadowing, and my role was clearly explained, multiple such situations occurred. During these occasions, the patient was reminded that the researcher was not a care team member at the rehabilitation centre where they received treatment. A similar observation was made in the study by van der Weele and Bredewold (2021) conducted in assisted living facilities for people with intellectual disabilities. The authors argued that the immediate need for support without a care worker in sight might have been one of the situations when this role confusion was likely to occur.
As my data collection in the centres spanned 2 weeks in most cases, I became known as ‘the architect’ and ‘the one with the floor plans’ in several centres a few days into my visit. This meant that other patients approached me for directions to their therapies and appointments while shadowing a patient, which caused disruptions in the data collection process. For this reason, only patients who appeared lost or in distress were given directions quickly and clearly. Otherwise, I would politely explain that I was following another patient and unable to help. This study’s use of floor plans for data collection introduced this unique problem.
Inviting Me Into Spaces Where Shadowing Was Not Planned
While some patients misinterpreted my role, others wanted to invite me to participate in their experiences. For example, one patient asked me to join and be present in the room while he was receiving therapy for his paralysed hand. While performing an exercise of trying to pick up a small wooden cube from the table, the patient told me about his life and hobbies. The exercise of picking up the cube and the frustration resulting from his unsuccessful attempts inspired the patient to reflect on his feelings about the current situation caused by the sudden occurrence of his stroke. On multiple occasions, patients also invited me to join them as a participant in therapy, such as gym exercise or relaxation therapy. This gave me a better understanding of patients’ therapies and the spatial aspects of the locations where these treatments take place. Even though it was decided not to shadow patients inside their rooms and treatment rooms to protect their privacy, these brief glimpses inside the therapies have proven helpful in uncovering patients’ daily experiences in rehabilitation centres.
When invited and when it does not adversely impact the patient, joining patients in therapy as participants should be considered another level of exploration of their experiences of rehabilitation. However, researchers should be aware of the risks to them and the patients when the boundary between ‘(semi-)public’ (corridors and living rooms) and ‘private’ (patients’ rooms and therapy space) is crossed and they insert themselves further into patients’ lives; patients may share sensitive information that the researcher may not be prepared to deal with. Recommendations for clinical practice (e.g. Gutheil & Brodsky, 2011) could be taken as a guideline on how to maintain a professional relationship with the participant during shadowing fieldwork.
Other Possibilities for Patient Recruitment
Many patients were highly eager and happy to engage in this research study. After the day was over, patients often expressed their enjoyment of the day. They talked about it to fellow patients in the following days, recommending them to participate in my study. Other patients would then get interested and ask questions about my research study. Unfortunately, this referral type was not helpful for the study setup since the centres’ staff recruited patients according to the inclusion and exclusion criteria. Still, when suitable, this might be used as a snowball sampling strategy for participant recruitment in future research studies.
Staff Members’ Distrust
Shadowing a single patient over the course of one day meant an abundance of waiting in front of patient rooms and therapy rooms. These breaks were used to write thoughts/reflections and make sketches about previously observed situations. Therefore, I was present in the ward or therapy area with paper and a pen and continuously writing things down. Several times, a centre’s staff member approached me and asked who I was and if I was evaluating them. Not everyone was informed that a researcher was conducting a study with patients, and I was perceived as someone who was there to assess their performance. In these situations, I delicately explained my temporary role in the facility. Similar scenario was observed in the study of Goodrich et al. (2020); when patients were shadowed by healthcare staff, their colleagues felt like they were being observed and judged. Informing the staff members before the study is conducted and wearing a distinguishing symbol (different colour coat or a name tag) could help with this challenge caused by the nature of shadowing data collection.
The Emotional Toll of Data Collection
As an architect, I am not used to the environment of healthcare facilities where many people are ill and undergoing recovery. While preparing for the field study, I familiarised myself with the impairments that might result from a stroke. Even though reading about these conditions and recognising various symptoms was very helpful for the field study, it was not enough to emotionally prepare me for some difficult situations that were emotionally impactful. Furthermore, observing patients during a single day in their recovery process meant that I could not learn how their rehabilitation progressed, which was a difficult realisation. After a day with a patient, I felt emotionally involved in their recovery journey. Additionally, spending such an extended period of 12 hours per day in healthcare facilities was very emotionally impactful, and I felt emotionally drained when going home.
There could be multiple reasons for this unpreparedness for the emotional impact of research in healthcare environments. A researcher might be familiar with how to use the method and aware of who to observe and why but not be aware of how emotionally challenging this could be (Gill et al., 2014). One observation by Wincup (2001) states that researchers might be uncomfortable talking about the emotional toll of conducting research and that avoiding the topic likely results in new researchers being surprised by its impact while in the field. This situation is very likely in many research environments. Rager (2005a) suggests better training and education of new researchers, better mentoring regarding the personal impact of qualitative research, and planning one’s own emotional self-care during fieldwork (2005b). Those who may find shadowing personally challenging should be provided emotional and practical assistance before and after shadowing fieldwork (Goodrich et al., 2020). This is especially important when conducting research with vulnerable populations.
Ethical Dilemmas
As data collection can be “highly unpredictable and uncertain” when shadowing (Gill et al., 2014, p. 71), it is challenging to prepare for all situations that can occur in the field. In the case of this research, numerous ethical dilemmas were encountered during data collection. Examples include a patient who became too tired while returning to his room after therapy and asked the author to push his wheelchair, a patient who accidentally entered another patient’s room and stayed there thinking it was their room, and multiple distressed patients who would stop the author to ask for directions while another patient was shadowed. In these instances, letting the patients find their way independently and observe how they interact with the built environment would be more beneficial for data collection and learning about how patients navigate these difficulties independently. However, if the patient directly asked for help, what was ethically and morally appropriate for the observed patient was prioritised over the quality of the collected data. These situations were impossible to predict before the field study and unfolded as the study occurred. Therefore, flexibility (Quinlan, 2008) and the ‘do no harm’ attitude (Sanjari et al., 2014) must be adopted when conducting shadowing research in healthcare facilities. Furthermore, concerning ethical dilemmas, relational ethics, and the researcher’s role, recommendations from medical ethnography (Hackett & Hayre, 2021; Higginbottom et al., 2013) can serve as guidance.
Discussion
The illustrated application of the shadowing method demonstrates its major strengths when used in vulnerable populations, consistent with the conclusions of previous studies (van der Meide et al., 2013, 2015; van der Weele & Bredewold, 2021). In contrast to previous research mainly focusing on health services, the main contribution of this article is the illustrated potential of this method to explore the fit between the mobility (dis)abilities of patients and the various aspects of the built environment.
However, shadowing as a method also introduces multiple limitations and challenges that need to be acknowledged when considering this method, including its improvisational nature (Gill et al., 2014; Meunier & Vasquez, 2008), power imbalance between the researcher and the participant and constant renegotiating of consent and boundaries (van der Weele & Bredewold, 2021), close contact with the participant and emotional impact on the researcher (Gill et al., 2014), the necessity for constant balancing between “sympathetic proximity” and “critical distance” (Gilliat-Ray, 2011, p. 482), and the general misunderstanding of the method within academic community (Bartkowiak-Theron & Robyn Sappey, 2012). This section highlights additional considerations specific to conducting research focusing on the built environment and patient populations, as the method’s limitations and challenges have been widely covered in prior research. Practical ‘how to’ recommendations for shadowing patients in healthcare facilities are offered.
Important Considerations When Shadowing Patients
One of the main challenges of shadowing encountered before the fieldwork can even occur is negotiating access to the research setting and recruiting participants. This process can be complex and time-consuming in healthcare facilities, where patients’ security, data protection, and confidentiality are crucial. Since this method is not commonly used in research, the unfamiliarity causes the ethical committees to be more reluctant to provide ethical approval (Bartkowiak-Theron & Robyn Sappey, 2012) and the healthcare facilities and patients more reluctant to participate. Also, people recovering from an illness or injury may not be willing to engage in research lasting many hours, which is typical for shadowing research. Therefore, shadowing can be an intense method for both the researcher and the participant due to its length and intimacy (Ferguson, 2016; Gill et al., 2014; van der Meide et al., 2013); the emotional, physical, and mental toll on the researcher can be substantial (Dickson-Swift et al., 2009; Eriksen, 1995; Lofland & Lofland, 1995) due to the extended time spent in the presence of people with various health conditions.
Multiple biases affect shadowing data, starting with participant recruitment. The medical staff likely chose the patients assessed as able to handle the shadowing method. This approach affected the diversity of participants included in the study, which did not offer a complete picture of their rehabilitation experiences. Similar conclusions were made by van der Weele and Bredewold (2021) in their research with residents of assisted living facilities with intellectual disabilities. The participants might have also felt obliged to participate in the research study when asked by their therapists or physicians, who are in a position of power concerning their health (Johnson, 2014). Furthermore, the researcher’s impact on the behaviours and actions of the shadowed persons cannot be avoided in observational research (Quinlan, 2008). In cases where the interactions with the built environment are the main focus of the shadowing investigation in contrast to the usual roles and work practices (McDonald, 2005; Meunier & Vasquez, 2008), the Hawthorne effect might not play such a significant role but could still be minimised by not precisely sharing what is being observed with the participant, depending on the research question. Another bias is the selectiveness of data determined by the participant moving through space and time; the researchers will only see where the shadowed person takes them (McDonald & Simpson, 2014).
Finally, the researchers’ experiences in the field and how they interpret the observed events are influenced by their personality, identity, and previous (research) experiences (Gill, 2011). At the same time, shadowing practice is shaped by the research setting, the involved participants, and the researcher’s theoretical commitments (Gill et al., 2014). This openness is a great advantage of the method, which offers flexibility and adaptability to various research settings, participants, and research questions (Meunier & Vasquez, 2008). However, the fieldwork can be unpredictable and challenging since it is impossible to predict how shadowing will unfold in the field (Gill et al., 2014).
Advantages of the Method to Study Behaviours in the Built Environment
Shadowing has shown great promise for practice-based research that connects the behaviours to the built environment and records their interactions that other observational approaches might overlook. A comprehensive examination of architectural design and its impact on the users’ experiences can be undertaken by asking ‘how’ the participants are affected by the built environment and mapping and observing their interactions in real time. Combining building floor plans, textual notes, sketches, and mini on-the-go interviews helps anchor the observed behaviours and actions in space and, in the case of this study, identify what supports or hinders patients’ mobility in the built environment. When continuous observations are combined with open notes and interaction with participants, as compared to unobtrusive structured observation techniques, an interpretive layer is added to what is observed, leading to a more complete understanding of practices and their relationship to healthcare facility design. As most human communication is nonverbal (Argyle, 1972), shadowing enables researchers to include and analyse the activities of patients who cannot express themselves verbally (van der Meide et al., 2013). Because spatial context is taken into account during shadowing, this method allows for interpreting the events—for example, the patient’s frustration when they realised they were going in the wrong direction.
Recommendations for Shadowing Patients to Investigate the Built Environment
Gill et al. (2014) gave 10 recommendations for conducting shadowing research in their publication ‘Shadowing in/as work: ten recommendations for shadowing fieldwork practice.’ Building on these recommendations, further, more specific recommendations are given to any researcher interested in doing research with patients (in healthcare facilities) and focusing on their interaction with the built environment. These practical recommendations for shadowing fieldwork draw on my personal experience of doing research with stroke patients as an architect, and they could be regarded as an optional supplement to the recommendations by Gill and colleagues, which offer general and helpful methodological guidance also used to prepare for my research.
Recommendations Related to Shadowing Focused on the Built Environment
Preparation
As the research focuses on the participants’ interactions and experiences of the built environment, extensive floor plan preparation is needed before starting the fieldwork. This, sometimes, involves redrawing the complete building plans in case the plans received are drawn in different scales (building growth in different phases) or if only the fire escape plans are obtained. Furthermore, the floor plans should be simplified to show only relevant elements for the investigation. Certain elements, such as a grid or columns corresponding to the actual situation in the building, can be used to map the location more precisely (Zeisel, 1984). Another important consideration before starting the fieldwork would be to define what will be observed, as it can be easy to lose track of the unfolding activities while taking notes. Notetaking could be simplified, depending on the research question and aim. An example would be to record activities as a whole and not as fragmented elements (e.g. ‘the patient is eating’ instead of ‘the patient is taking a spoon’, ‘using it to take food from the plate’, ‘bringing the spoon close to the mouth’, and so on).
Notetaking
Because of the focus on the built environment, the notes taken during the shadowing session can be used to describe not only the observed person’s activities but also the role of the physical environment in these activities (Nanda & Wingler, 2020). The sheets for taking notes should be as open as possible, but how the researcher looks at unfolding events should be structured and targeted based on the research question and focused on the interactions with the built environment. Otherwise, making continuous notes of everything going on could risk missing some important events in real time. There are examples of taking continuous notes of everything going on and extracting data related to the built environment later (Eriksson et al., 2010). However, these observations were done in timespans of a maximum of 2 hours per day; longer observation periods would require a sharper focus on events related to the built environment. It is strongly encouraged to map specific events and activities on the floor plans of the building where the person was shadowed. Furthermore, two-dimensional and three-dimensional sketches can be immensely useful for mapping specific interactions with particular elements in the built environment. These also help to better recall particular events in addition to the textual notes after the fieldwork.
It is important to plan well the material that will be used to record shadowing data. During my fieldwork, data collection was done on paper. In this case, floor plans were printed on A3 paper and stapled (multiple-story buildings). Coloured pens are helpful to differentiate between mapped paths, especially if the shadowed person passes through the same corridors multiple times during the session, which is highly probable in healthcare environments. Symbols on the floor plan could also be used to map specific points on the route and connect them better with the textural notes.
Analysis
Even though it is predominantly used in qualitative research, shadowing as a method is “neither truly qualitative nor truly quantitative” (McDonald, 2005, p. 468). Therefore, the researchers need to be open and flexible when interpreting the collected data, as there can be multiple ways to approach the data analysis depending on the data types collected (textual notes, visual notes, voice recordings, etc.) and the research question(s) guiding the study. The multiple data types could be analysed following the principles of mixed methods research (Creswell & Plano Clark, 2017) since shadowing can blur the boundaries between multiple complementary methods, such as, on-the-go debriefing interviews, observations, and tracking of walked distance or time use.
Presentation of the Results
As shadowing can result in quantitative and qualitative data (McDonald, 2005), the results can be presented in various ways. When investigating the role of the built environment in patients’ behaviours and experiences, the use of visual material such as building floor plans, situational sketches, or photographs is crucial for situating the observed events in space and gaining a better understanding of their impact.
Recommendations Related to Observational Research With Stroke Patients
Notetaking
Stroke patients might use a wheelchair, walker, crutches, or a walking stick to move around. These mobility aids can significantly alter how they interact with the built environment and which elements might be experienced as a mobility barrier. It is important to note details in how patients use the space and the particular elements in space they interact with. Here, notes are focused on where they move (routes and locations) but also what they do with the whole body and different body parts when interacting with various elements in the built environment (e.g. a patient in a wheelchair moving backwards along the entire corridor using their leg because they are not able to roll their wheelchair on carpet flooring).
While taking notes, the researcher should be prepared for the person being observed to ask to look at notes/sketches created during shadowing. Sharing them should be done simply and openly, discussing and interpreting them together. Because the researcher already had insight into the lived experience of the shadowed person, the data production in the debriefing sessions is more collaborative and does not rely only on information recounted by the participants (Quinlan, 2008).
Openness
Sharing experiences during shadowing helps develop ‘contextualised understanding’ and experience the world of the shadowed person (Gilliat-Ray, 2011). While shadowing stroke patients in rehabilitation centres, joining patients during therapies was not planned as it was considered to invade their privacy. However, patients expressed the wish for me to join them on several occasions, which was immensely helpful in understanding their experiences while in rehabilitation and immersing myself in their world. When conducting fieldwork, general openness and flexibility should be regarded as key characteristics of shadowing (Meunier & Vasquez, 2008). Accessing (with permission) unexpected spaces and situations where important events and routines that make up a day in a healthcare facility take place can provide opportunities for better understanding and studying their spatial context. Another challenge researchers embarking on research with patients should be aware of is that, depending on their condition, some participants might be unable to express themselves verbally. The shadowing method has the advantage of enabling research with vulnerable groups because the emphasis is placed on communicating the whole body (van der Meide et al., 2013). This is especially the case when studying the role of the built environment in patients’ experiences; here, interactions of the whole body with the built environment should be observed.
Communication
Stroke patients can experience various forms of speech impairments, most commonly aphasia (Pedersen et al., 1995). This limits the communication and on-the-go debriefing sessions during shadowing. For example, in my study, one patient could only say ‘na’ and nothing else but understood what was spoken to him. In such situations, the researchers need to focus on nonverbal communication and interactions with space and rely on their interpretation of the observed events for data analysis.
Approach
A healthcare environment setting introduces specific challenges in recruiting participants. The persons that will be shadowed can usually not be recruited before the researcher arrives at the centre, and the recruitment is done on the spot from the participants pre-selected by the centres’ medical staff. Approaching potential participants in the healthcare facility together with a person who is well-known to the patient (e.g. a nurse or therapist) has proven successful. The study can be explained to the potential participants, and they can be left with an information sheet about the study and the consent form. In the following days, the person can be asked about their decision. Additionally, the researcher should know that ethical issues and dilemmas will arise during the project (von Unger, 2021). In rare situations, the researcher might be ethically obligated to interfere in the care processes or practices (Liberati, 2017). One simple example from my experience would be interrupting and alerting the nurses working at the nurses’ station that a patient entered another patient’s room unnoticed and stayed there, thinking it was their room. The researchers should be aware that different events can occur and be ethically accountable, even if they occasionally interfere with data collection. Additionally, the interactions of participants who did not consent to participate in the study (other patients, nurses, therapists, physicians, and visitors) with the shadowed person might be recorded during informal, unplanned encounters. These occurrences should not immediately be considered unethical but should be evaluated within the research setting and context (Johnson, 2014).
Being Inconspicuous
Disruptions to the regular flow of activities in healthcare facilities are another issue that can arise occasionally (McDonald, 2005). Patients could become confused and late for therapies, therapists’ work could be delayed as a result, and so on. Shadowing should entail making an effort to be as unobtrusive as possible, although this might mean very different things in different settings (Quinlan, 2008). Constant navigation between distance and proximity is also required; the role of an observer is, therefore, challenging since it necessitates balancing in-depth insight into patients’ experiences with respect for their privacy (Liberati, 2017).
General Recommendations
Planning
Getting access to healthcare facilities is one of the most challenging parts of fieldwork planning. The flexibility needs to be maintained and plans adapted according to the availability of research sites. A round of familiarising with the built environment should be done before shadowing the participants – using notations on the plans, sketches, or photos. Here, some observations and assumptions about the environment can already be recorded (Zeisel, 1984), which could be helpful when observing participants’ behaviour.
Study Design
Planning the study in multiple increments is recommended if multiple participants are shadowed in the same setting over an extended period. In my research, shadowing 10 patients in a row, each for 12 hours (with a weekend in between to rest), was too physically and emotionally challenging. I advise shadowing 2–3 participants close to each other and leaving yourself time to reflect and decompress after the fieldwork.
Identity
Negotiating for identification (a distinctive uniform or a tag) would help with role misunderstandings with staff members of the participating facilities. The role confusion involving patients cannot always be prevented, and the researchers need to be aware of their potential impact on the participants (van der Weele & Bredewold, 2021).
Time Use
Shadowing patients in healthcare buildings means following the patients’ schedule because the entire session revolves around their usual schedules and routines in this setting. This can introduce physical demands on the researcher, especially regarding eating and bathroom breaks (Gill et al., 2014). I adopted the approach of eating when the patient eats and having bathroom breaks while in therapy. This was possible because I was given the patient’s therapy plan for the day with the duration of each therapy. Nevertheless, the first 5–10 minutes of patients’ therapy should be used for breaks, as therapy may be shorter than scheduled (as seen several times). Waiting for the patient to finish with therapies is another challenge when shadowing patients in healthcare settings. These waiting times can be best used to reflect on the previously observed events, revise the notes and sketches, and think about potential questions for the shadowed person about specific actions or events.
Revisioning
Because shadowing is such a complex method involving multiple layers of notetaking, the amount of collected data is often substantial (Quinlan, 2008). Returning to the collected data with some time distance (a year or longer) is essential, as new ways of looking at the data could be applied and new valuable insights obtained.
Conclusion
Shadowing shows potential for research looking into the role of the built environment in the experiences, behaviours, and activities of patients in healthcare facilities. The illustrated example and the offered practical recommendations are based on the individual experience with conducting shadowing research. They are intended to demonstrate the possibilities of shadowing in architectural research and to advance the methodological discussion surrounding shadowing as a scientific research method. Floor plans can be an invaluable instrument in shadowing research for understanding patients’ spatial experiences and evaluating the adequacy of healthcare facilities for their intended purpose. The improvisational nature of shadowing can be viewed as both a challenge for an inexperienced researcher and a significant advantage for obtaining insight into the worlds of recovering patients in healthcare settings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research study was supported by the European Social Fund (ESF) and the Sächsische Aufbaubank (RL ESF Hochschule und Forschung 2014 bis 2020, scholarship agreement number: 100235479). The author(s) acknowledge TU Wien Bibliothek for financial support through its Open Access Funding Programme.