
Abstract
Up to 25% of people with type 2 diabetes (T2D) may binge eat which is almost 10 times as many as in the general population. Binge eating is associated with depression, anxiety, and social isolation. Moreover, binge eating may increase the risk of obesity and high blood glucose levels, both of which can accelerate the onset of complications to diabetes and death in people with T2D. Still, little is known about the experiences, needs, and preferences of people with T2D and binge eating that can inform and develop current and future treatment efforts. The aim of the study was therefore to gain in-depth insights into the experiences and biopsychosocial support needs of women and men with T2D and binge eating. Twenty semi-structured individual interviews (65% with females) were conducted and analyzed according to the methodology of Interpretive Description. Four themes were identified: (a) T2D and binge eating: Feeling trapped in a vicious circle; (b) Unwanted outcasts: Responding to continuous criticism; (c) Biomedical relief: Blaming and adjusting the body; and, (d) Silent struggles: Wanting to cease the secrecy. Pertinent to all themes were the guilt, shame, and worries about developing complications that the participants experienced when binge eating despite having T2D. Although binge eating triggered emotional distress, binge eating was at the same time a way of coping with such distress. Implications for treatment and future research are discussed, including the need to systematically assess and address binge eating in routine T2D care.
Keywords
Introduction
The global prevalence of type 2 diabetes (T2D) is estimated to be at 536 million people and increasing (Sun et al., 2022). Living with T2D may be burdensome due to the constant vigilance and continuous multiple self-management tasks required regarding diet, physical activity, and medication administration to attain the recommended glycemic levels (Davies et al., 2022). However, many people with T2D (PWT2D) have increased glycemic levels, which may give rise to anxiety due to the awareness of the associated risk of developing serious complications, such as heart disease, blindness, and amputations (Polonsky et al., 1995). The reasons for elevated glycemic levels are complex and multifactorial (including genetic dispositions, medication, and psychosocial components), and various degrees of support are therefore needed by most PWT2D (Davies et al., 2022; Winkley et al., 2020).
Psychological problems like depression and diabetes distress and their associations with diabetes management, including glycemic levels, are well described (Fisher et al., 2010; Hessler et al., 2014). Disordered eating, however, has been studied less. The most common eating disorder in the general population, and in PWT2D, is binge eating disorder (BED) (Guerdjikova et al., 2019). BED is defined by recurrent episodes of eating an objectively large amount of food in a discrete time while experiencing a loss of control (American Psychiatric Association, 2013). Typically, this binge eating (BE) is followed by marked emotional distress, but in contrast to bulimia nervosa, the BE is not followed by compensatory behaviors (e.g., vomiting) (American Psychiatric Association, 2013). The emotional distress usually includes guilt and shame (American Psychiatric Association, 2013), which can be described as undesirable emotions linked to a person’s negative self-evaluation (Miceli & Castelfranchi, 2018). More specifically, guilt entails a sense of doing something wrong when not meeting one’s own standards (e.g., beliefs and goals) for which one is responsible, whereas shame may imply hopelessness linked to a perceived lack of power to live up to one’s ideal self (Miceli & Castelfranchi, 2018).
BE exists in various degrees, and severity indicators include frequency and duration with BE for ≥1 day/week for 3 months being the diagnostic cut-off for BED (American Psychiatric Association, 2013). Although high-quality epidemiological studies are lacking, systematic reviews have estimated a substantial increase in the prevalence of BED in PWT2D compared to the general population (1.4%–25.6% vs. 2.0%–3.5%, respectively) (Chevinsky et al., 2020; Harris et al., 2021). The differences in prevalence may stem from varying recruitment strategies, exclusion criteria, and cultural variations (Chevinsky et al., 2020). Moreover, BED was included as its own psychiatric condition in the American Diagnostic and Statistical Manual of Mental Disorders (DSM-5) and the International Classification of Diseases (ICD-11) as recent as 2013 and 2018, respectively (American Psychiatric Association, 2013; World Health Organization, 2023). BED is therefore estimated to be under-diagnosed because clinicians are not yet familiar with its diagnostic criteria (Chevinsky et al., 2020).
Reasons for BE are multifactorial, including biological (e.g., genetic), behavioral (e.g., prior dieting), and psychosocial components (e.g., trauma or adverse childhood events) (Harris et al., 2021; Rienecke et al., 2022), and, if left untreated, subthreshold eating disorders tend to evolve into clinical eating disorders (Koreshe et al., 2023). In this article, the term “BE” refers to BED and subthreshold BED with the distinction being whether an individual fulfills the diagnostic criteria to obtain the BED diagnosis or not (American Psychiatric Association, 2013). Both are explored because any level of BE should be addressed, especially in diabetes due to the risks involved. In systematic reviews, BE in PWT2D is associated with obesity and could result in higher glycemic levels than recommended (Abbott et al., 2018; García-Mayor & García-Soidán, 2017; Harris et al., 2021), both of which may accelerate the onset of diabetes complications (Davies et al., 2022). Furthermore, a systematic review showed that BED in the general population was associated with increased levels of depression compared to individuals without BED (Araujo et al., 2010). Finally, a recent cross-sectional study demonstrated that BE in PWT2D correlated with perceived weight stigmatization (i.e., being poorly treated by others due to their negative beliefs, attitudes, and judgments linked to body weight) (Puhl et al., 2022).
To our knowledge, only three articles have explored the experiences of people with co-existing T2D and BE in-depth (Ritholz et al., 2022; Salvia et al., 2022, 2023). The articles are based on qualitative analyses of interviews with 21 women from the United States living with BED and T2D or prediabetes. Findings were that although BE preceded the T2D diagnosis in the women interviewed, they sometimes experienced T2D treatment as triggering their BE due to an increased focus on diet and weight management (Salvia et al., 2022). Experienced weight stigma from clinicians along with negative thoughts and feelings of failing when not adhering to the recommended treatment could also lead to BE as a way of coping which, in turn, further exacerbated the experience of being a failure (Ritholz et al., 2022; Salvia et al., 2023). The experiences of people with T2D and BE living outside the United States still need to be investigated due to contextual dissimilarities that may affect them. American clinicians refer to the DSM-5, for example, whereas clinicians in Denmark, where this study was conducted, adhere to the ICD-11 whose implementation process was initiated in January 2022 and is still ongoing (Danish Health Data Authority, 2022). Furthermore, the three existing articles did not include men. BED is, however, the most common of eating disorders in men (Guerdjikova et al., 2019), and their perspectives and treatment preferences may differ from those of women (Richardson & Paslakis, 2021). Finally, the inclusion of both T2D and prediabetes in the existing studies may have obfuscated some experiences and support needs that are specifically pertinent to PWT2D. For instance, based on a large sample (N = 55,882), Neumann and colleagues documented higher health-related quality of life in people with prediabetes than people with T2D (Neumann et al., 2014), indicating that the experiences of living with diabetes may differ between the two groups. The aim of this study was therefore to gain further in-depth knowledge from another setting about the experiences and the biopsychosocial support needs of both women and men living with co-existing T2D and BE.
Methods
This study applied qualitative and quantitative methods. To illuminate the aim of the study, individual interviews were conducted according to the qualitative methodology of Interpretive Description (Thorne, 2016). Survey data were collected to ensure that varying demographic participant characteristics had been obtained while being able to summarize these in addition to characteristics specific to diabetes, eating disorder symptoms, and mental well-being. Below, the two approaches are described in more detail.
Interpretive Description
Interpretive Description was applied, as it aspires to explore, inform, and improve clinical practice (Thorne, 2016). In Interpretive Description, patterns and themes are explicated not only to explore human experience but also to create knowledge and understanding about what is taking place in clinical settings and to generate awareness about it (Thorne, 2016). Interpretive Description draws on selected parts of ethnography, phenomenology, and grounded theory to pursue an in-depth understanding of individual experiences while seeking to account for the impact of contextual events in which the social setting and the research topic mutually form each other (Thorne, 2016). However, Interpretive Description also differs from these research disciplines by highlighting the importance of applying a “research logic” that allows for the use and combination of the methods required to fully answer the research question. This flexibility is practical when setting out to explore “new grounds,” where unforeseen discoveries may demand an altered research strategy (Thorne, 2016).
The relevance and rigor of an Interpretive Description study are sought by carrying out the data generation and data analysis concurrently (Thorne, 2016). In addition, a detailed audit trail is kept. The former permits the preliminary analysis to enlighten and alter the succeeding data generation and vice versa, while the latter keeps track of the preliminary findings and any methodological adjustments made during the study (Thorne, 2016). Furthermore, the concurrent data generation and data analysis guides the decision regarding whether additional study participants are required, or whether recurring, valid findings have been identified by continuously testing preliminary findings against newer data material (Thorne, 2016).
According to Thorne (2016), theoretical frameworks can be adopted to initiate a study. Thus, such frameworks may inspire, design, and guide but not define a study whose findings should be able to stand on their own as the “theoretical scaffolding” is removed (Thorne, 2016). To set the study in motion, the biopsychosocial model was applied to integrate the overall perspective that a person’s health is a reflection of complex interactions between biological, psychological, and socio-environmental factors (Engel, 1977). The theoretical frameworks guiding the data generation and analyses were enhanced cognitive behavioral therapy (CBT-E) for eating disorders as described by Fairburn (2008) and social support theory as understood by Cullen (1994).
Interview Data Generation and Analysis
Semi-Structured Interview Guide.
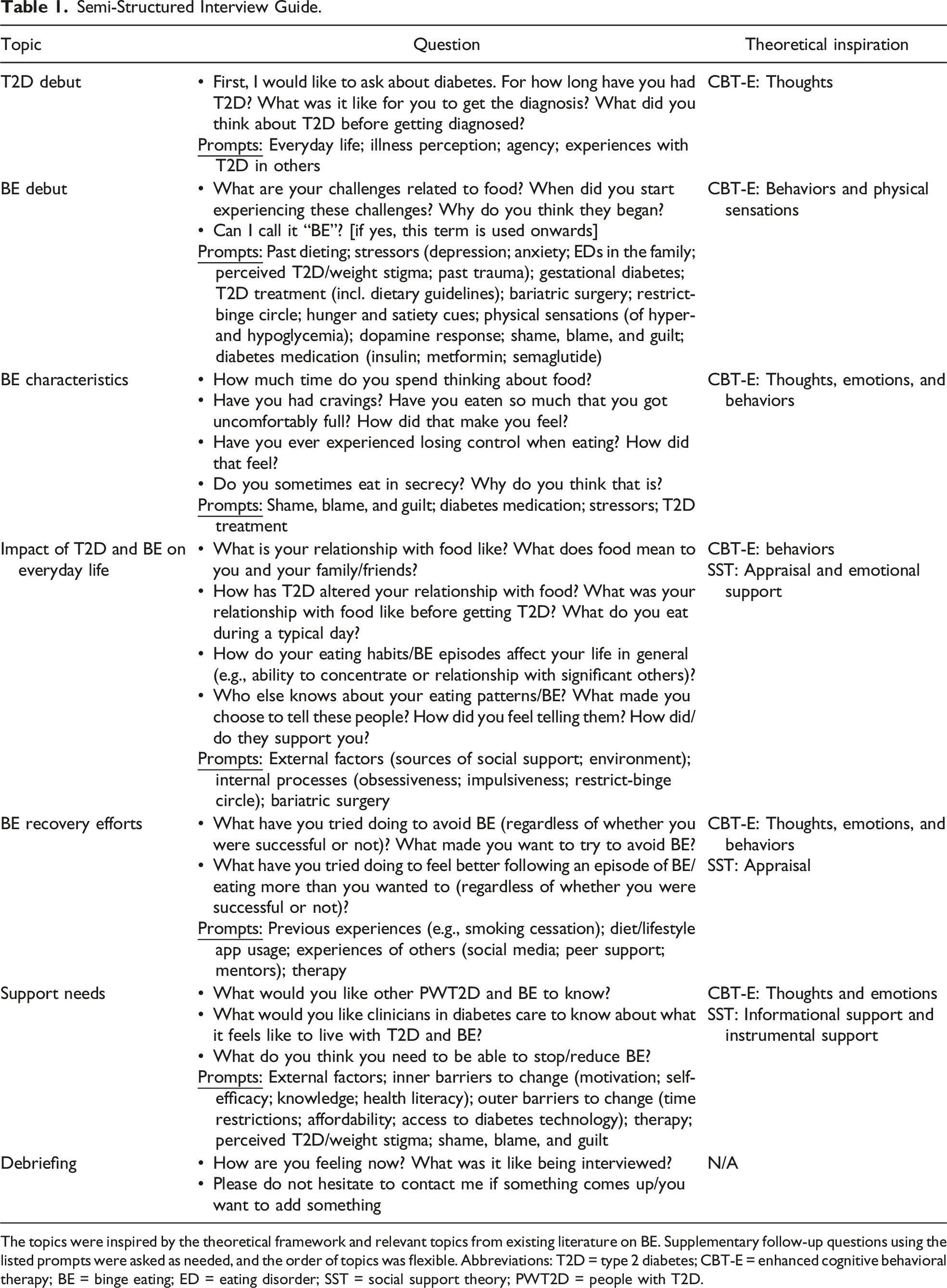
The topics were inspired by the theoretical framework and relevant topics from existing literature on BE. Supplementary follow-up questions using the listed prompts were asked as needed, and the order of topics was flexible. Abbreviations: T2D = type 2 diabetes; CBT-E = enhanced cognitive behavioral therapy; BE = binge eating; ED = eating disorder; SST = social support theory; PWT2D = people with T2D.
The interview audio was recorded using a digital voice recorder and transcribed verbatim by a student worker with a BSc in sociology who had received detailed instructions (e.g., regarding how to mark the tone of voice). To validate the transcripts, PL compared randomly selected parts of every fifth transcript to the corresponding audio-recording, and the transcripts were deemed satisfactory. The interview transcripts were sorted and analyzed using NVivo software (QSR International Pty Ltd., 2018).
The data analysis included four overall steps which, because the data were generated and analyzed simultaneously, were repeated as the data material was acquired (Thorne, 2016).
First, PL performed a broad, systematic coding to sort and make sense of the extensive data material. The initial codes were inspired by the theoretical frameworks and relevant topics from existing literature on BE (Supplementary Material 1). During the coding, PL made sure to alternate between the process of coding parts of the data and taking “a step back” to assess the data material as a whole, thus revisiting previously examined data (Thorne, 2016). To best fit the data material as it was generated, new codes were added inductively when needed, while others were merged. When the findings began repeating themselves more frequently, as additional data material was included in the analysis, the recruitment of additional participants was ceased (Thorne, 2016). The initial coding structure and its adjustments were continuously discussed with co-authors (IW, LC, KI, and BC).
Second, irrelevant data (e.g., on technical difficulties using insulin pens) were discarded, while the data contributing to illuminating the study aim (e.g., on factors inducing or preventing BE) were retained to make the amount of data material manageable (Thorne, 2016).
Third, PL described the preliminary themes and discussed them with all co-authors. If in doubt about the rigorousness of the themes, the broad coding was repeated by PL to confirm that the themes were grounded in the original data material (Thorne, 2016).
Finally, the critically assessed themes were described in detail, augmented by quotations from the raw data underpinning the findings along with pseudonyms and age of the cited participants to enhance the transparency of the study (Thorne, 2016).
To challenge the preconceptions of the authors further and to ensure the relevance of the study, three user representatives (i.e., PWT2D and personal experience with BE) were consulted throughout the study regarding its aim, design, and preliminary findings.
Survey Data Collection and Analysis
Participant Characteristics (N = 20).
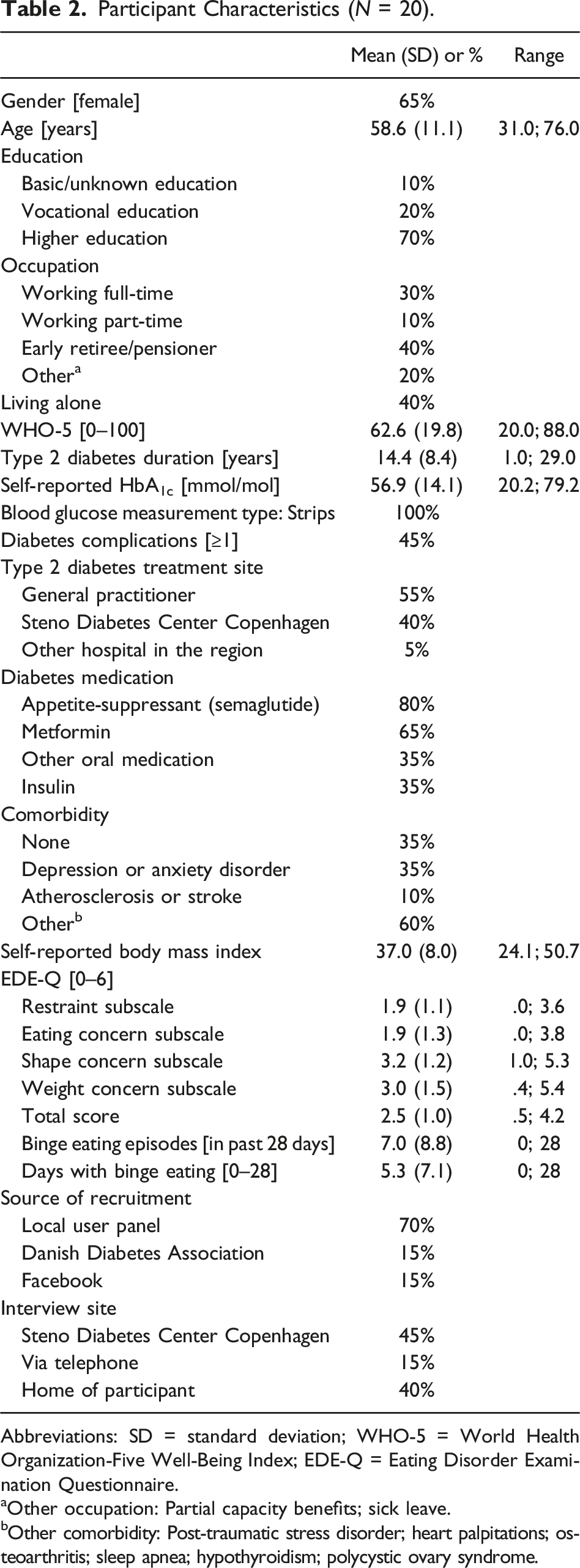
Abbreviations: SD = standard deviation; WHO-5 = World Health Organization-Five Well-Being Index; EDE-Q = Eating Disorder Examination Questionnaire.
aOther occupation: Partial capacity benefits; sick leave.
bOther comorbidity: Post-traumatic stress disorder; heart palpitations; osteoarthritis; sleep apnea; hypothyroidism; polycystic ovary syndrome.
The World Health Organization-Five Well-Being Index (WHO-5) is a 5-item scale measuring mental well-being within the previous 14 days using a 6-point Likert scale. The WHO-5 produces a score on a scale ranging from 0 to 100 (from the worst to the best imaginable mental well-being) with a cut-off of 50 or less typically being applied to screen for depression (Topp et al., 2015). The Eating Disorder Examination Questionnaire (EDE-Q) is a 28-item measure assessing the range and severity of eating disorder symptoms within the previous 28 days by four subscales (Restraint, Eating Concern, Shape Concern, and Weight Concern), each measured on a 7-point Likert scale, a total score (i.e., the mean across the subscales), and binging and purging frequencies (Carey et al., 2019). The WHO-5 and the EDE-Q are translated and validated in Danish (Lichtenstein et al., 2021; Topp et al., 2015).
Descriptive statistics of the survey data were calculated using RStudio version 4.3.0.
Recruitment
Eligible interview participants (a) were adults (≥18 years); (b) had a diagnosis of T2D (for ≥1 year); (c) were able to communicate verbally in Danish; and (d) had a self-reported eating disorder or were currently (or had previously been) experiencing self-reported disordered eating to a degree that they experienced as detrimental to their quality of life. Purposive recruitment of participants was carried out to include women and men with various demographic characteristics in the sample (Thorne, 2016). Recruitment took place from May to July 2022, through the email newsletter of the Danish Diabetes Association, Facebook (due to a post about another yet related study, made in a T2D-specific group), and a user panel hosted by SDCC with members volunteering to be contacted, for instance, for research purposes. At the time of recruitment, the user panel had 265 adult members with T2D, who were all invited to participate in an interview. Everyone responding to the interview invitation was contacted by phone by PL to further discuss the aim and methods of the study and to assess whether the inclusion criteria were fulfilled.
Ontology, Epistemology, and Reflexivity
This study holds a realist interpretive perspective on knowledge (Thorne, 2016). According to Interpretive Description, epistemological integrity in research is obtained when there is consistency between the ontological foundation, the research question, and the methodology and methods applied to answer this research question (Thorne, 2016). In this study, such epistemological integrity was pursued by applying Interpretive Description as its aim of exploring individual, yet socially dependable, experiences embedded in a “real world” complies with the ontological assumptions of a realist interpretive perspective.
Researchers inevitably impact their studies when formulating and conducting them (Malterud, 2001; Thorne, 2016). Thus, to avoid simply “seeing what they wanted to see,” the authors pursued reflexivity by continuously attempting to identify and challenge their own preconceptions about the topic as well as those of co-authors (Malterud, 2001; Thorne, 2016). The multidisciplinary clinical and academic backgrounds (i.e., in nursing, endocrinology, psychiatry, (health) psychology, nutrition, public health, and medical anthropology) of the authors helped this process.
Ethical Statement
Before the interviews, PL provided oral and written information on the study aim and methods, voluntary participation, and the right to withdraw from the study at any time. If they agreed to be included, the participants signed an informed consent form. All data material was pseudonymized and stored on encrypted drives with limited access, back-up, and 24-hour logging. The study was approved by the Danish Data Protection Agency (ID: P-2022-27) and conducted according to current legislation (Danish Ministry of Health, 2020, 2022). As only self-reported data material was included, no ethical approval was needed, and an exemption letter was obtained from the Regional Committee on Health Research Ethics (ID: H-20082723).
Findings
Fifty-one people from the user panel responded to the invitation to participate of which 31 were excluded, as they were not currently or had not previously experienced BE themselves. The remaining 20 participants were interviewed and completed the survey within 1 week following the interview. Overall, varying demographic participant characteristics were obtained with an age range of 31–76 years, 65% female, 70% having a higher education, 40% working full- or part-time, and 40% living alone. However, no ethnic minorities were represented. The mean diabetes duration was 14.4 years, and 45% had ≥1 diabetes complication(s) (all participants characteristics are listed in Table 2). The data analysis generated a total of four themes and four subthemes (Figure 1), which are described in the following. Depiction of themes and subthemes. Abbreviations: T2D = type 2 diabetes; BE = binge eating.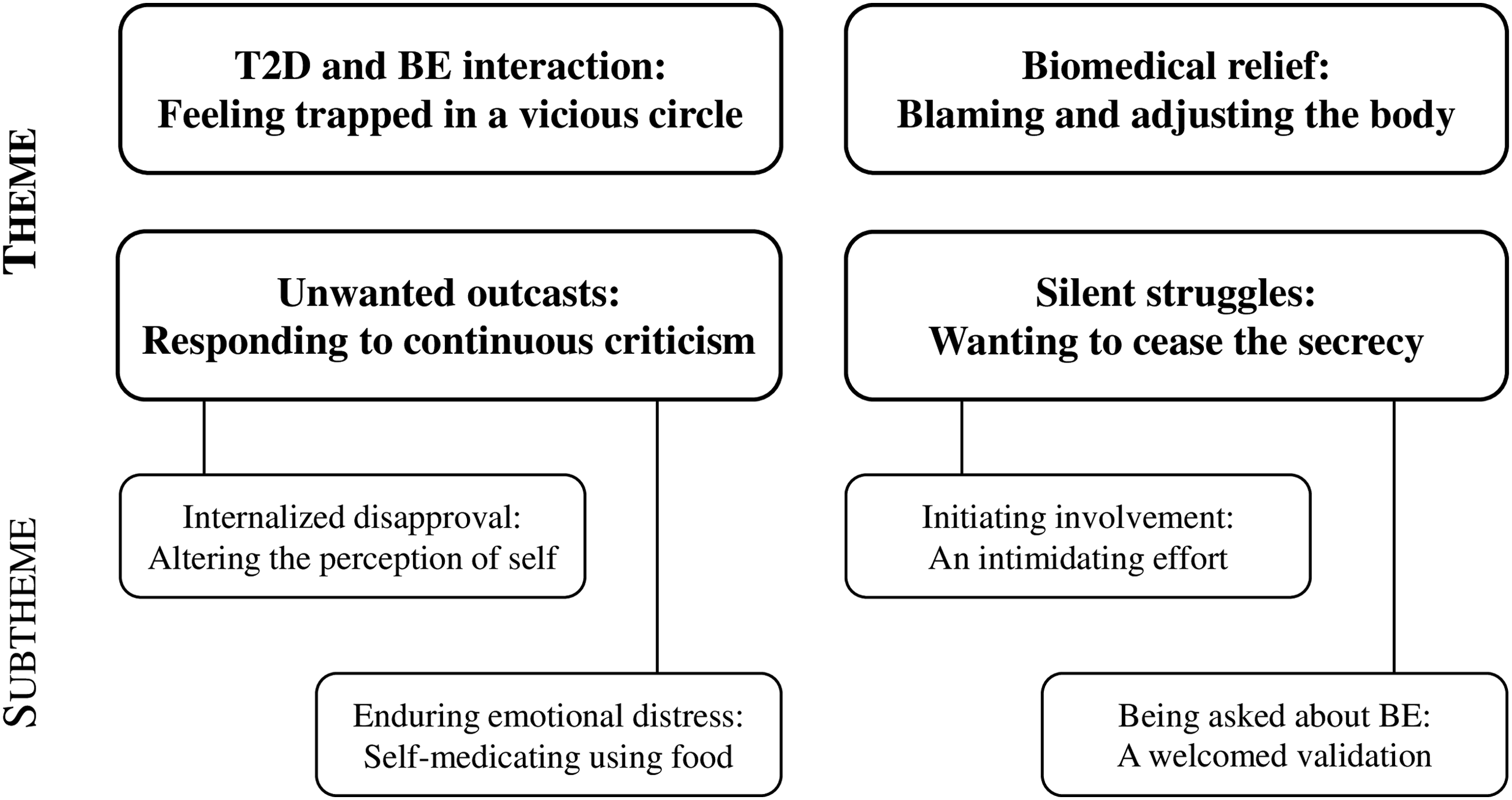
T2D and BE Interaction: Feeling Trapped in a Vicious Circle
The participants described T2D and BE not simply as co-existing but interacting which meant that diabetes-related concerns often triggered an episode of BE and vice versa. Although the participants had engaged in some degree of BE for years before developing T2D, they described how BE could escalate because of their T2D diagnosis, due to the dietary treatment guidelines: “It is like an extra layer of frustrations related to food has been added” (Mindy, 31). Participants were familiar with the increased risk of complications associated with higher glycemic levels than recommended. Therefore, they blamed themselves when BE for negatively affecting not only their mental well-being but also their glycemic levels thereby increasing the risk of complications. To cope with feelings of guilt, however, the participants often engaged in additional BE as it felt comforting to them at the time. Furthermore, participants felt that they had failed by BE in the first place, and therefore, they might as well keep eating: “Blaming yourself is the road to hell. I’ll be like ‘oh, you can’t do anything right anyway’, and then it [BE] will get completely out of hand. But I don’t know what else to do other than eat” (Ann, 63). The additional BE, however, led to increased feelings of guilt, thus solidifying a vicious circle of T2D-related concerns and BE in which the participants felt trapped.
Besides being informed by clinicians, several participants had become aware of the risk of complications by witnessing relatives with diabetes getting them. Such experiences increased the participants’ worries about developing complications themselves due to BE, while, for some, also intensifying the urge to binge as a way of managing the emotional distress. One participant, whose father had died from cardiovascular complications of diabetes, described how concerns about complications would overwhelm her after BE: “His [father] vision got severely impaired. And he started having strokes. He was like a stranger in the end. It was a nightmare […] I’m terrified to end up like him when I can’t control it [BE]” (Mary, 60).
The cyclic relationship between T2D and BE also appeared in relation to insulin. Participants taking insulin described how it induced an intense desire for sugary foods. When giving in to the craving, the participants were remorseful due to worries about the impact on their long-term blood glucose (HbA1c) as well as their increased need for insulin to adjust for the BE episode: “It [insulin] makes me insanely hungry. I crave sugar. And I’ll do anything to have some. And then, my blood glucose will get too high, and I will need more insulin. Then, I feel guilty” (Daniel, 73). Likewise, participants not taking insulin were reluctant to start doing so, even when recommended by clinicians, primarily due to concerns about its effect on appetite and weight.
Participants had also experienced intense hunger when restricting their diet to lose weight, which typically led to BE and, with that, concerns about the impact on glycemic levels. A participant described how he sometimes kept busy working to avoid eating until he got so hungry that he could not ignore it anymore: “When I start eating, I binge. And that’s not healthy at all, especially not with diabetes. I feel so guilty” (John, 42). Yet, the next day, participants often restricted again to compensate for BE, which triggered another BE episode, thus completing the vicious circle.
Unwanted Outcasts: Responding to Continuous Criticism
Participants described how they had repeatedly been criticized by others, including family members and friends as well as clinicians, which resulted in feelings of shame, worthlessness, and being “the odd one out” (Joseph, 47). Thus, the continuous disapproval seemed to be internalized by the participants, affecting their perception of self: “I guess something’s the matter with me. I should be able to just pull myself together […] I’m the one who can’t figure it out [how to stop BE]” (Daniel, 73). To manage the emotional distress of feeling like an outcast, and in the absence of other coping strategies, participants resorted to BE or “self-medicating using food” (Betty, 58). Hence, this theme is composed of two subthemes expanding (a) the process of internalizing continuous criticism and its effect on the perception of self and (b) the participants’ rationale for resorting to BE to manage emotional distress. Both subthemes are described below.
Internalized Disapproval: Altering the Perception of Self
Over time, the participants apparently internalized the recurrent disapproval from others regarding T2D, body weight, or both, which negatively affected their view of themselves. For instance, a participant described how her step mother’s repeated negative comments about weight had made her feel wrong when reaching puberty where she, naturally, got heavier: “She would pinch me saying I was chubby. I was 14 […] It’s clear to me where that feeling of being fat and wrong and uncomfortable in my body comes from” (Amanda, 48).
The participants’ negatively altered self-perception seemed to be aggravated by their BE behaviors, resulting in them describing themselves in an undesirable manner, for example, as “being gluttonous” (Richard, 50), “stuffing one’s face” (John, 42), or “going berserk [when eating]” (Steven, 76). In a similar manner, being diagnosed with T2D exacerbated the participants’ experiences of being an outcast: “Then, you get T2D, and you’re not just fat anymore. You’re even more wrong” (Amanda, 48). The recurrent criticism from others made the participants worry about further judgment and shaming from others. The desire to evade such distress was strong enough to influence the participants’ decision-making and overruled other competing concerns: It [BE] was really bad for my health and diabetes, but also my bank account because I spent so much money on food. And I’m embarrassed about that. Being embarrassed has played a really big part in the decisions I’ve made. (Mary, 60)
Enduring Emotional Distress: Self-Medicating Using Food
Several participants had experienced adverse childhood events, which instigated or accentuated their experiences of being outcasts or “the black sheep of the family,” as Carol (62) said when explaining how her family, who had consistently bullied her throughout her childhood, had made her feel. Similarly, other participants gave accounts of previous trauma, including sexual abuse, physical violence, and severe parental neglect.
With time, the participants, who provided accounts about experienced traumatic events, linked these to their current relationship with food and concluded that they had resorted to BE as a way of coping with emotional distress: “As a child, I never learned how to regulate my emotions. The only thing I had was food. If I was scared, food was there to help, and if I was angry. Or sad” (Betty, 58). Thus, BE had become a way of regulating or numbing unpleasant feelings to find rest: “I’d eat until I was full enough to pass out. If I don’t, I’ll lie there rotating, almost like a grilled chicken, until I go eat even more” (Mindy, 31).
Some participants described having realized that to be able to stop BE, they would need to establish other strategies to cope with emotional distress. For example, a participant explained how she lacked other ways of managing her anxiety than BE: “I’ve tried restricting my diet to lose weight, but eventually, I will have an anxiety attack that will go away when I start eating” (Amanda, 48). Despite being mindful of the need to identify new ways of regulating one’s emotions, doing so without support was considered difficult by most participants as they were still overwhelmed by the urge to binge eat regularly: Although I’m aware of this [coping by BE], I still find it extremely difficult to eat like I should. I still have a terrible craving. Constantly. It’s physical, but also in my head. My thoughts. You can’t simply choose not to feel it. (Timothy, 58)
Identifying BE as a coping strategy was helpful to the participants as it partially relieved them of some of the guilt and shame that they endured when BE although having T2D. Referring to prior sexual abuse, a participant explained, “There’s been a lot of reasons for me to binge-eat. I sought refuge in food. And down the road, I’ve figured out that it [BE] isn’t really my fault” (Angela, 58).
Biomedical Relief: Blaming and Adjusting the Body
For years, the participants had considered a lack of self-discipline or will power to be the main reason for BE: “I have the backbone of an earthworm,” Gregory (71) said about his determination to restrict his diet. He continued, “I might make fun of it, but in fact, I am extremely embarrassed. It’s just easier to joke about it.” Participants wanted to learn about biomedical mechanisms for BE, as it provided them with alternative explanations for BE than “weak character traits” (Susan, 70). Thus, being able to blame the body for BE rather than the mind or personality relieved the participants of some of the guilt linked to BE. For instance, a participant taking antipsychotic medication said: “I blame my metabolism and diabetes for being fat. And the [antipsychotic] pill I’m taking. It gives me cravings and makes me binge. So, it’s not just a matter of me being greedy” (Helen, 54). Participants also found it helpful to explain the recurrence of the urge to binge as caused by the addictive “dopamine high” (Timothy, 58) that they believed that BE would instigate. Referring to a TV show depicting the weight loss efforts of a group of people with obesity, a participant said: I remembered this scene. She bought six large cookies and I thought to myself “get a grip”. But then I realized that I’m exactly the same. Like me, she didn’t want to do it, but we need that [dopamine] high […] I can’t escape it, but it’s not really my fault. (Carol, 62)
Another physiological explanation for BE that some participants had become aware of was overwhelming hunger as a response to restrictive dieting or fasting with the aim of losing weight or compensating for a specific binge. A participant explained how restriction resulted in BE: “I’d only have water and coffee before lunch […] But then, I could easily drink a liter of sugary drinks or more. And I’d convince myself I needed three pieces of cake. I wasn’t conscious about it then. How the one caused the other” (Grace, 59).
The body having “a will of its own” (Gregory, 71) or betraying them was a common perception among the participants: “I haven’t done anything in my life to get them [health conditions] I don’t know why they happened. It feels like things, and my body especially, have been ganging up on me” (Ruth, 73). Relatedly, participants described the view that their bodies needed to be medically adjusted or “fixed.” To stabilize glycemic levels and reduce body weight, several participants had been prescribed with appetite-suppressants (semaglutide) and had been informed that vomiting, nausea, and diarrhea were common but temporary side-effects. In some participants, however, these side-effects remained. Regardless, the participants adhered to the medication as its ability to reduce the urge to binge, thus potentially resulting in weight loss, exceeded its disadvantages: “I’ll gain three kilos simply from looking at a glass of water. It’s been an ongoing battle until I started injecting it [appetite-suppressant]. Something must be wrong with my body in that sense, so I endure them [side-effects]” (Marie, 69).
Silent Struggles: Wanting to Cease the Secrecy
Secrecy regarding BE played a significant role in the participants’ lives. The majority of participants had not told anyone about the BE due to worries that disclosing it would result in humiliation and judgment from others, particularly if they knew about the T2D diagnosis, too. Richard (50), who had been BE for 25 years said: “I haven’t told anyone but you [about BE]. I think it’s extremely embarrassing that I can’t help myself but eat.” Nevertheless, participants wanted others whom they trusted to know about their struggles with BE, as involving others was expected by the participants to reduce unpleasant feelings of loneliness and isolation. Thus, the participants wanted to cease the secrecy regarding BE but made a clear distinction between the process of (a) taking the initiative themselves to speak up about BE, as opposed to (b) others taking the initiative to ask about it. The two approaches constitute each their subtheme, which are expanded below.
Initiating Involvement: An Intimidating Effort
Participants were reluctant to take the initiative to disclose their BE to family and friends because they were embarrassed and afraid of being judged and humiliated. Furthermore, the participants wanted to spare others from worrying about the potentially harmful impact of BE on glycemic levels. Besides keeping BE episodes to themselves, participants would therefore “cover the tracks” (Lauren, 52), for instance, by disposing of empty candy bags in dumpsters outside the house to avoid family members discovering them, or by hiding food for future binges around the house “just like if you were an alcoholic hiding bottles of booze” (Helen, 54). Participants were concerned that the secrecy would ultimately—if it had not already—harm their relationships with their partner, children, or friends by introducing dishonesty, thus causing tension. Moreover, concealing the BE kept the participants from explaining related mood swings to others: “You want them to know so they can understand why you’re acting in a certain way. That it’s not because of something they did, but I simply can’t make myself say it out loud” (Joseph, 47).
Due to concerns that clinicians would not comprehend the compulsive aspect of BE but merely misinterpret overweight and increased HbA1c as results of “poor self-discipline” (Grace, 59), participants were also reluctant to involve clinicians: “It [BE] is like a magnet pulling you. I can’t escape it. But I worry that they [clinicians] wouldn’t understand” (Marie, 69). A few participants had, however, confided in clinicians, but typically, it had taken a long time, for some even years, to “build up the courage, because it [BE] was such a big secret” (Ann, 63). These participants had involved clinicians following the T2D diagnosis to inform them that developing diabetes was essentially a consequence of prolonged BE as opposed to being “greedy and lazy” (Mindy, 31). Angela (58) who had been BE most nights for 17 years said: It seems ridiculous that you need to be relieved of some of the guilt […] But I wanted to tell my doctor why it [T2D] happened. Because it’s not just a matter of lifestyle. There are lots of reasons why you behave as you do, the urge to BE being one of them.
Being Asked About BE: A Welcomed Validation
Being asked directly about BE behaviors by clinicians was perceived by the participants as a sign of sincere interest and consideration, and in such circumstances, they felt that they would be much more inclined to disclose these behaviors. Over the years, a few participants had been asked by clinicians about BE, which had been welcomed, because it validated BE as a relevant concern. Being asked about BE also served to normalize it as the participants inferred that their clinicians would not inquire about it if it was uncommon. Thus, being asked about BE by clinicians was helpful in counteracting the burdensome secrecy linked to BE as well as past experiences of being different from others and feeling wrong. A participant who had been asked about BE by her general practitioner stated: “Saying it out loud was helpful. I stopped eating so much that it would physically hurt. I still binged, but not as much as I used to. And I felt less weird” (Carol, 62).
Most participants, however, had not encountered any clinicians inquiring about BE, which they ascribed to the healthcare system in general not recognizing patients as complex human beings whose health-related challenges have multifactorial causes. Thus, PWT2D or any other condition cannot be delimited to one single medical specialty, such as endocrinology: “Within each specialty at the hospitals, they [clinicians] are really good, but they should sometimes try to acknowledge the entire human being” (Ruth, 73).
Discussion
The findings of this study demonstrate how living with the two interacting and often mutually aggravating conditions, T2D and BE, can be experienced as lonely, shameful, and highly challenging. In alignment with previous research (Ritholz et al., 2022; Salvia et al., 2022), immense feelings of guilt and worry linked to BE when having T2D may not only be exhausting but also self-reinforcing, triggering further BE to regulate these difficult emotions. Thus, it appears crucial to relieve emotional distress in PWT2D and BE to improve their mental and physical health. Rooted in this study, several biopsychosocial support needs of PWT2D and BE can be identified that may help reduce such emotional distress if addressed in clinical practice. First, the burden of guilt may be linked to the self-stigmatizing yet common belief among PWT2D and BE—as well as some clinicians—that BE is merely caused by absent self-discipline or will power (Liu et al., 2017; Salvia et al., 2023). This perception may be counteracted, if clinicians were more knowledgeable about, and thus more open to, the complex and multifaceted nature of BE, building on several predisposing, precipitating, and perpetuating biopsychosocial factors that are mutually dependent. For this purpose, it may be helpful for clinicians to gain insights into CBT-E as defined by Fairburn (2008), as the model elaborates on the interactions typically occurring between negative thoughts (e.g., thoughts about failing when BE), negative emotions (e.g., fear of complications), physical sensations (e.g., hunger triggered by insulin), and behaviors (e.g., BE to regulate difficult emotions) (Fairburn, 2008). Thus, CBT-E may be applied as an explanatory model to guide clinicians and PWT2D and BE to gain an understanding, for example, of specific mechanisms involved in the vicious circle of T2D and BE (Ritholz et al., 2022; Salvia et al., 2022). Yet, competent delivery of CBT requires proper training (Fairburn, 2008), which should be considered, for instance, when developing novel treatment programs. Regarding the influence of social support as described by Cullen (1994), clinicians and PWT2D and BE may mutually explore what sources of social support exist (e.g., family or friends) and in which situations the social support may be especially helpful. Yet, clinicians need to be familiar with and recognize the potential impact of social support on BE to do so. The first step for PWT2D and BE toward identifying individual BE triggers and potential strategies to interfere with these may be to gain awareness of existing sources of social support as well as mechanisms relating to BE in the context of T2D specifically.
Based on the findings, it may also benefit PWT2D and BE if clinicians provide information about the high prevalence of co-existing T2D and BE, as this may normalize the issue, thus limiting feelings of being an outcast. In other, yet related contexts, group-based interventions aiming to normalize the experiences of participants have proven helpful in reducing feelings of loneliness, for example, in relation to diabetes distress (Due-Christensen et al., 2021; Joensen et al., 2017) and generic eating disorders (Fairburn, 2008). Along the lines of Cullen (1994), group-based interventions may also allow for the desire for social support to be fulfilled, for instance, by facilitating emotional support among peers (Joensen et al., 2017). Considering the need for social support, it is, however, unfortunate that, while wanting to involve their clinicians, most PWT2D and BE in this study were not asked about BE by any clinicians. Reasons for this may be clinicians’ concerns about invading the personal space of patients or that clinicians are unaware of the prevalence and complexity of BE in T2D. The latter claim may, in part, be supported by the study participants’ experiences of clinicians being a significant source of criticism regarding weight and diabetes management. Such criticism may stem from clinician weight bias, which has been documented in prior research (Bennett & Puhl, 2023; Sabin et al., 2012). Weight stigmatization in healthcare settings is a concern due to its negative impact on patient–clinician interactions, which may lead to avoidance of care and poorer clinical outcomes in patients (Puhl et al., 2022; Sabin et al., 2012). In any event, future research should investigate potential barriers and facilitators to assessing and addressing BE in PWT2D during routine diabetes care from the clinicians’ perspective.
Based on this study, systematically assessing BE in routine T2D care seems crucial to improve detection rates. On this note, future research is encouraged to investigate appropriate methods to screen for BE in PWT2D. Although several screening tools for BED exist (House et al., 2022), these may not be fit for purpose, as they are generic and do not, therefore, assess BE in PWT2D specifically. Moreover, existing tools are designed to screen for BED which, if detected (or suspected), should warrant referral to proper psychiatric assessment and treatment (Fairburn, 2008). To prevent exacerbation into clinical eating disorders, however, subthreshold BE should also be addressed, especially in a T2D-specific setting due to the aforementioned associated risks (García-Mayor & García-Soidán, 2017; Munsch et al., 2012; Raevuori et al., 2015). Thus, more research is needed investigating feasible and valid methods of systematically assessing different severity levels of BE in routine T2D care, for example, in the form of dialogue tools facilitating the conversation between patients and clinicians (Cleal et al., 2022). If BE is identified, proper support should be offered, and therefore, research-based interventions addressing various degrees of BE in T2D treatment should be developed. Such an intervention was described in a recent article by Coales et al. (2023) from the United Kingdom. Using co-design, an existing and evidence-based guided self-help intervention for BED was adapted into an online and T2D-specific version (Coales et al., 2023). According to the authors, the next steps are to conduct a pilot trial that will—in the case of promising results—be followed by a full-scale trial to test the effectiveness of the intervention (Coales et al., 2023). If effective, this intervention may offer the support needed by PWT2D and BE, although translations and cultural adjustments are needed if the intervention is offered to non-English speakers and in other countries (Heim & Weise, 2021).
This study explores the novel topic of co-existing BE and T2D. The sample reflects the gender distribution of BED in the general population (Erskine & Whiteford, 2018), and the inclusion of male participants makes the study the first to explore in depth the experiences, perspectives, and support needs of both women and men with T2D and BE which is warranted (Striegel et al., 2012). Yet, the findings of this study were comparable to those of prior research (Ritholz et al., 2022; Salvia et al., 2022), suggesting that gender does not necessarily define the experiences and support needs of PWT2D and BE. However, whether PWT2D and BE have experienced adverse childhood events or not may be of significance, and the impact of previous trauma should, therefore, be investigated further when designing future interventions specifically for PWT2D and BE. In this study, a rather wide representation of demographic characteristics was obtained, except for the representation of ethnic minorities. As ethnicity may affect treatment-seeking behavior and treatment response in individuals with BE (Lydecker & Grilo, 2016), efforts should be made in future studies to explore the experiences and support needs of PWT2D and BE with other ethnic backgrounds than Scandinavian. Other limitations apply that should also be taken into consideration when interpreting the findings. Due to the recruitment strategy, participants were included via self-referral, which may have affected the results. For instance, findings related to the participants’ wish to cease the secrecy of BE may reflect characteristics of the specific sample rather than a support need pertinent to the target population. In addition, the participants were not included based on BE assessment criteria but on self-reported experiences with BE (current or prior). These varying levels of current BE in the study participants may complicate the process of translating the findings to other yet similar contexts, such as clinical settings treating patients with current full-syndrome BED only. Still, the applied recruitment strategy enabled an in-depth exploration of the experiences of PWT2D and various degrees of BE, including those in recovery. The participants’ EDE-Q scores, shape concern and weight concern especially, were elevated compared to the general population as was the frequency of BE, indicating that the sample did, in fact, struggle with BE (Welch et al., 2011). Similarly, the range of the participants’ WHO-5 scores (from 20 to 88) may illustrate the various degrees to which they, at the time of the study, were struggling with BE or in recovery. Finally, the findings demonstrated that medications—for diabetes as well as other conditions—may affect how BE is experienced and made sense of by PWT2D which corresponds with research documenting the impacts on appetite regulation, for instance, of several types of antipsychotic medication (Lett et al., 2011). Future studies on co-existing T2D and BE should therefore properly assess and report the prescribed medication of participants.
Conclusion
This study highlights how women and men with T2D and BE may find it emotionally distressing living with two conditions that mutually exacerbate each other. Although apparently wanting support from clinicians, PWT2D and BE may be reluctant to request it due to the shame and the feelings of guilt that are typically linked to BE behaviors. Thus, PWT2D and BE may need clinicians to bring up the sensitive topic of BE during T2D consultations. Effective and clinically feasible methods of assessing BE in a T2D-specific setting should therefore be developed along with interventions increasing clinician knowledge and addressing the biopsychosocial support needs of PWT2D and BE.
Supplemental Material
Supplemental Material - “I Haven’t Told Anyone but You”: Experiences and Biopsychosocial Support Needs of People With Type 2 Diabetes and Binge Eating
Supplemental Material for “I Haven’t Told Anyone but You”: Experiences and Biopsychosocial Support Needs of People With Type 2 Diabetes and Binge Eating by Pil Lindgreen, Ingrid Willaing, Loa Clausen, Khalida Ismail, Helle Nergaard Grønbæk, Charlotte Humble Andersen, Frederik Persson, and Bryan Cleal in Qualitative Health Research
Footnotes
Acknowledgments
The authors are grateful to the study participants for sharing their experiences, the user representatives for their input during the study, and student worker, Freja Bang Mikkelsen, for transcribing the interviews. In addition, the authors would like to thank the Danish Diabetes Association and the Novo Nordisk Foundation for granting financial support.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PL and IW own stocks in Novo Nordisk. HNG has conducted clinician teaching sessions paid by Novo Nordisk. FP has served as a consultant on advisory boards or as an educator for Astra Zeneca, Novo Nordisk, Sanofi, Mundipharma, MSD, Boehringer Ingelheim, Novartis, and Amgen and has received research grants to the institution from Novo Nordisk, Amgen, and Astra Zeneca.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the Danish Diabetes Association (Jubilee scholarship 2020) and the Novo Nordisk Foundation (NNF22OC0079561).
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.