
Abstract
Disordered eating is associated with negative physical and psychological outcomes for those with type 2 diabetes (T2DM), making it an important target for intervention. Theoretical modelling is recommended to inform interventions; however, it is unclear whether established disordered eating models are applicable to those with T2DM. We aimed to evaluate Stice’s dual pathway model of disordered eating within a T2DM population. Participants included 192 adults living with T2DM, who completed a cross-sectional survey incorporating measures of body weight shame, dietary restraint, negative affect, binge eating and other disordered eating behaviours. Structural equation modelling was used to test the model. Results indicated that a dual pathway model demonstrated poor fit, with the restraint pathway not supported. Following removal of the restraint pathway, a revised model produced superior fit, with negative affect mediating the relationship between body weight shame and binge eating. Clinical implications for interventions and future research directions are discussed.
Background
An estimated 529 million people worldwide are living with diabetes mellitus, with global prevalence predicted to almost double to 1.3 billion by 2050 (Ong et al., 2023). Type 2 Diabetes (T2DM) is characterised by insulin resistance, initial hyperinsulinaemia and subsequent progressive impairments in insulin secretion (Ahmad et al., 2022). It is the most common form of diabetes, accounting for approximately 96% of all cases (Ong et al., 2023). Disordered eating appears common amongst those with T2DM, with literature suggesting up to 25% of individuals with T2DM may meet criteria for Binge Eating Disorder (BED; Abbott et al., 2018), with rates of non-clinical disordered eating attitudes and behaviours seemingly even higher (Çelik et al., 2015). Disordered eating may adversely impact individuals with T2DM both physically and psychologically, as it is associated with higher insulin resistance (Ilyas et al., 2019; Kumar et al., 2023; Nip et al., 2019; Stojek et al., 2019; Yang et al., 2017), depression, anxiety and diabetes distress (Huisman et al., 2023), diabetes- and weight-related stigma (Puhl et al., 2022), and body image dissatisfaction (Herbozo et al., 2015). Given these deleterious outcomes, it is imperative we understand the factors contributing to and maintaining disordered eating in those with T2DM in order to inform effective interventions. Theory-grounded modelling is an important phase in the development of complex health interventions (Campbell et al., 2000); however, it is currently unclear whether existing theoretical models for disordered eating apply to those with T2DM.
Several theoretical models exist to explain disordered eating broadly, with Stice’s dual-pathway model (1998) demonstrating some of the most robust evidence (Pennesi and Wade, 2016). The dual pathway model (Stice et al., 1998) posits that external pressures and internalised ideals regarding body weight both contribute to body dissatisfaction (also directly impacted by body mass) and that body dissatisfaction leads to eating disorder symptoms including binge eating via the dual pathways of dietary restraint and negative affect (with dietary restraint also directly contributing to negative affect). While originally developed with a focus on Bulimia Nervosa, the model has since been demonstrated to also explain the onset of BED, subthreshold BED and purging disorder (Stice and Van Ryzin, 2019), and has been shown to better explain binge eating than alternative models (Holmes et al., 2015). Additionally, while originally developed as a longitudinal predictive model, the dual pathway model has also been validated at a state-based level (Holmes et al., 2014).
While the dual pathway model has not been examined in the context of T2DM, a modified version has been evaluated in a Type 1 Diabetes (T1DM) population. Peterson et al. (2015) originally proposed a modified dual pathway model that incorporated unique pathways specific to T1DM, including dietary regime, insulin initiation and weight-regain, and hunger and satiety disruption. Rancourt et al. (2019) tested this model which initially produced poor fit; however, fit improved with the inclusion of additional pathways. The modified model suggests the need to consider disease-specific factors that impact disordered eating, which has important clinical implications for interventions. This finding is particularly significant given that the literature shows standard eating disorder interventions are not as effective in those living with T1DM (Clery et al., 2017). For T2DM, however, the model has not been explored, and findings from T1DM cannot be generalised to those living with T2DM due to differences in the pathogenesis, treatment recommendations and lived experiences between the conditions. Consequently, it remains unclear if theoretical model modifications are similarly required within the context of T2DM. To the best of our knowledge, no existing models have been validated to explain the development or maintenance of disordered eating in T2DM.
To address this gap, the current study aims to evaluate a dual pathway model of binge eating within a T2DM population. The core dual pathway model components, which include body dissatisfaction, dietary restraint, negative affect and eating disorder behaviours, will be used. However, as body image shame has been found to be a better predictor of disordered eating than body dissatisfaction in more recent literature (O’Loghlen et al., 2022), and internalised weight stigma and disordered eating are related in those with T2DM (Puhl et al., 2022), we will use body weight shame in place of body dissatisfaction. Figure 1 presents the dual pathway model of binge eating to be tested in a T2DM population. Additionally, to test if the model applies to disordered eating behaviours more broadly than binge eating within the T2DM population, we will also test the model with emotional and uncontrolled eating included alongside binge eating as a final endogenous latent variable.
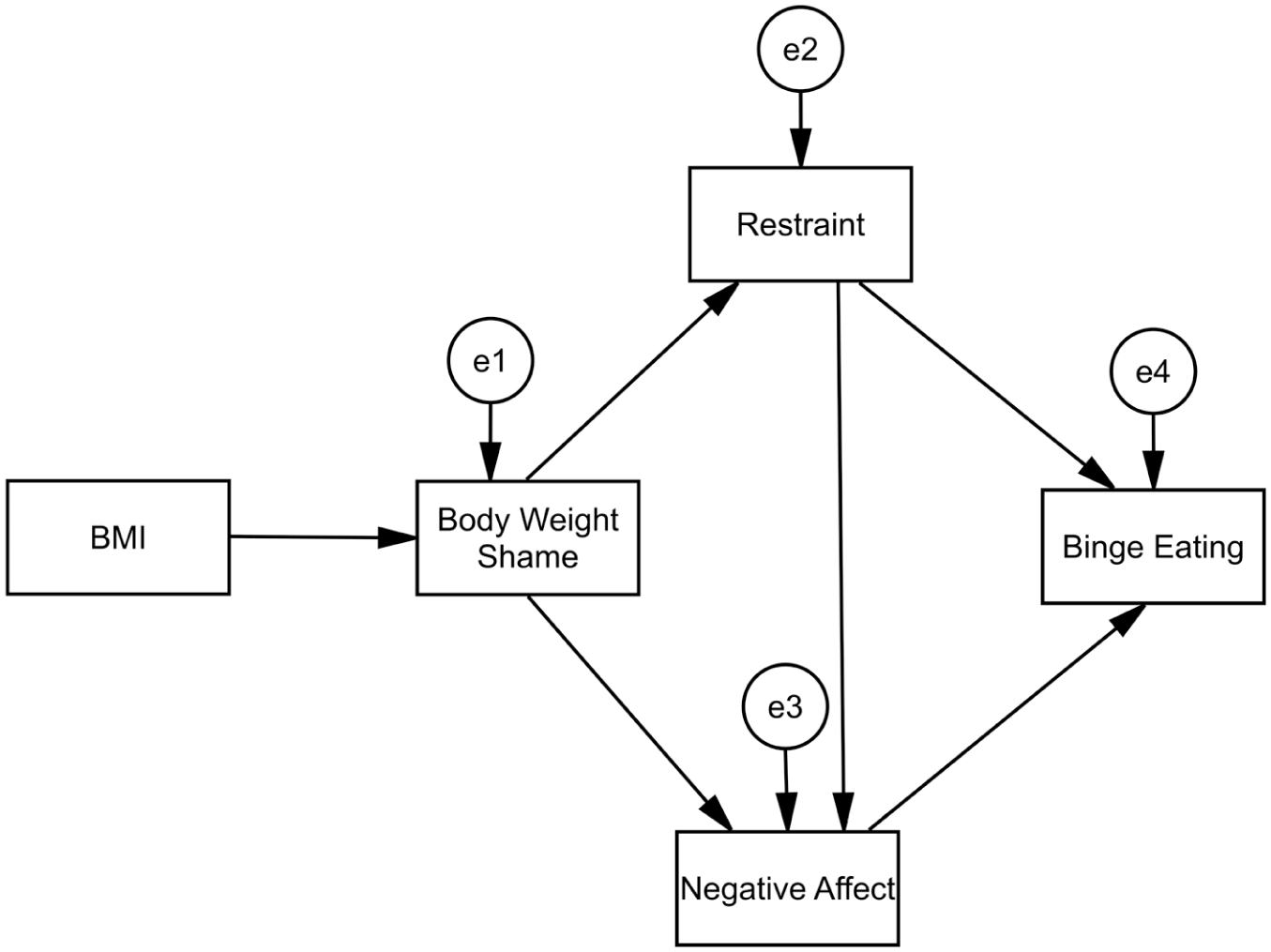
Dual pathway model of binge eating.
Method
Design and procedure
We conducted a cross-sectional, online survey-based study to investigate the relationships between disordered eating and key dual pathway model variables. The Central Queensland University Human Research Ethics Committee approved this research (approval number: 24195). We recruited participants through posters displayed in community health services, Facebook posts in diabetes support groups, word of mouth via professional networks, and the online recruitment platform Prolific. For our study, Prolific participants received reimbursement for their time at an average rate of ~A$11.56/30 minutes. Survey data were collected online using Qualtrics (Qualtrics, Provo, UT) from November 2023 to August 2024. Participation was voluntary, and participants provided informed consent after reviewing the information sheet and agreeing to the study prior to survey commencement.
Participants
People were eligible for the study if they were 18 years of age or older, fluent in English, and living with T2DM or interested in completing a brief T2DM risk assessment tool. Exclusion criteria included having a current diagnosis of T1DM or Gestational Diabetes. All inclusion and exclusion criteria were assessed via self-report. Two hundred and twenty-two people commenced the survey; 11 were excluded. Seven people were excluded due to having T1DM or Gestational Diabetes, one for failing two attention check questions (please select ‘Definitely true’ to show you are paying attention to this question) and three who only completed demographic questions (with no significant differences in age, gender or body mass index from included participants). Therefore, the eligible sample comprised 211 participants, with most recruited from Prolific (n = 196). As this study’s focus was on disordered eating in T2DM, participants with prediabetes (n = 16) or without diabetes (n = 3) were removed from the current analysis, leaving a final sample of 192. Table 1 presents the demographics (self-reported) of the included participants. Based upon the rule-of-thumb that sample size should be 20 times the number of variables (Thakkar, 2020), a minimum sample of 140 would be required for the most complex model in our study, indicating that the sample achieved is sufficient.
Demographics characteristics of participants (n = 192).
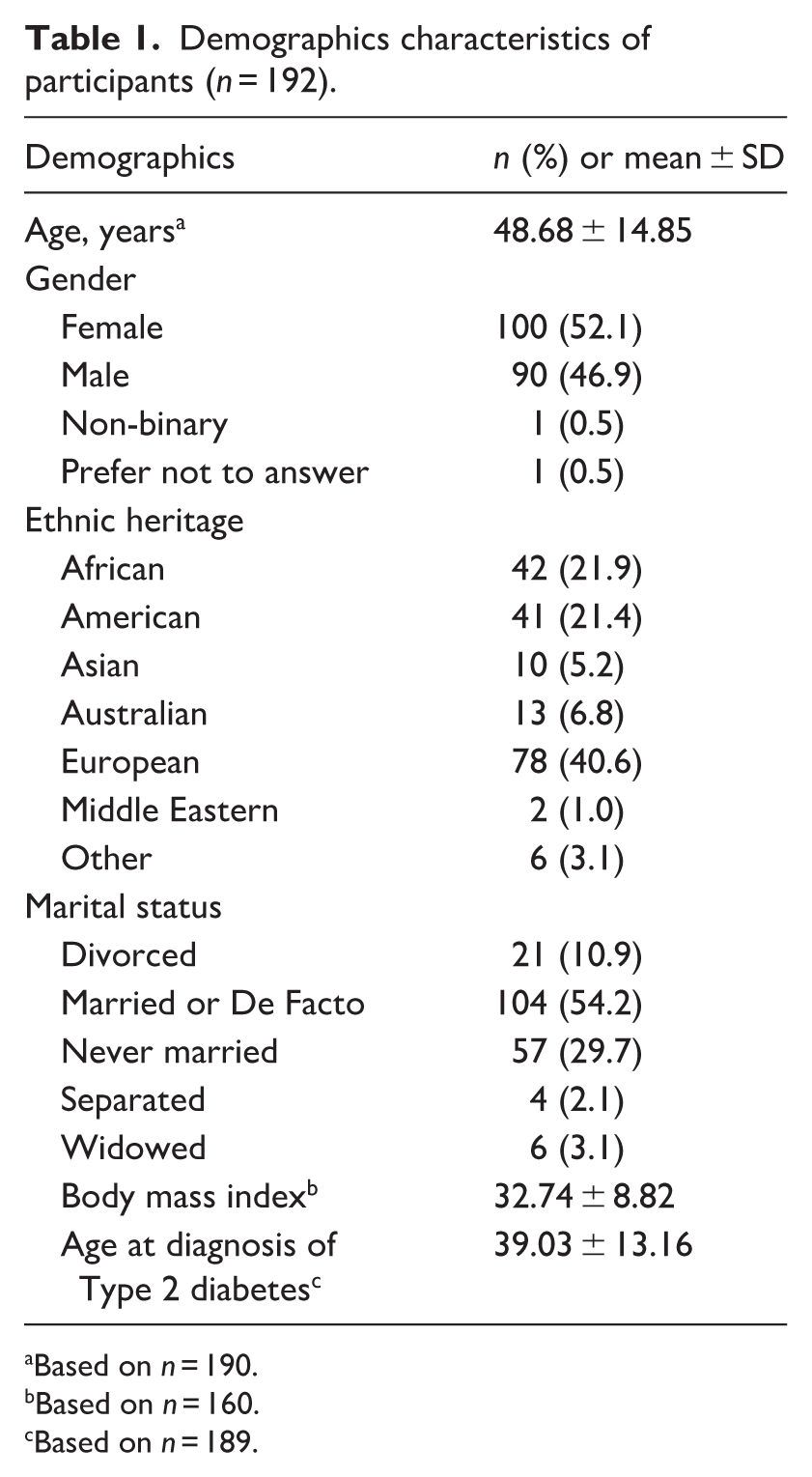
Based on n = 190.
Based on n = 160.
Based on n = 189.
Measures
Demographics and diabetes-specific information
Participants were asked eight demographic items: age, gender, ethnic heritage, relationship status, age at T2DM diagnosis, weight and height (used to calculate body mass index (BMI)). Participants subsequently completed a series of questions on disordered eating and eating behaviours, body weight shame and negative affect, as described below. These questions formed part of a larger survey outside the scope of the current study.
Disordered eating and eating behaviours
Three factor eating questionnaire revised 18-item version (TFEQ-R18)
The TFEQ-R18 (Karlsson et al., 2000) is an 18-item self-report measure that assesses eating behaviours in the domains of cognitive restraint, uncontrolled eating and emotional eating. Responses are given on a 4-point scale (1 = ‘definitely false’ to 4 = ‘definitely true’), with domain scale scores transformed using the following formula: Scale Score = ((Raw Score - Lowest Possible Raw Score)/Possible Raw Score Range) *100. Higher scores indicate greater endorsement of the eating behaviour domain. The TFEQ-R18 has demonstrated good internal consistency for all three scales in both general and higher-weight populations (α > 0.70; Karlsson et al., 2000; Romon et al., 2004). In the current study, internal consistency was similarly good for each of the three subscales (cognitive restraint α = 0.72, uncontrolled eating α = 0.90, emotional eating α = 0.87).
Binge eating disorder screener-7 (BEDS-7)
The BEDS-7 (Herman et al., 2016) is a seven-item self-report screening tool for probable BED as per Diagnostic and Statistical Manual of Mental Disorder – 5 (DSM-5) criteria. If responders answer ‘yes’ to Question 1 and Question 2, select ‘sometimes’ or more on Questions 3 through 6, and select ‘never’, ‘rarely’ or ‘sometimes’ on Question 7, they screen positive for probable BED. Using this scoring criterion, the BEDS-7 has demonstrated 100% sensitivity and 38.7% specificity (Herman et al., 2016). The BEDS-7 has also been used as a continuous measure in past research by summing the scores of all seven items, where higher scores indicate greater symptomology (Abdulla et al., 2023). Given structural equation modelling assumes variables are continuous, we also elected to use this sum scoring method. Internal consistency was good across all items in the current study (α = 0.92).
Body weight shame
Body weight shame scale (BWSS)
The BWSS (Carter et al., 2022a, 2022b) is a 14-item self-report measure that assesses internalised and externalised dimensions of body weight-related shame. It is a is an amendment of the Body Image Shame Scale (Duarte et al., 2015) incorporating weight specific items. Responses are given on a five-point scale (0 = ‘never’ to 4 = ‘almost always’) with higher scores indicating greater body weight shame. The original Body Image Shame Scale demonstrates good construct validity against the shape and weight concern subscales of the Eating Disorder Examination Questionnaire (EDE-Q; Duarte et al., 2015), which have been used to measure body dissatisfaction in previous research assessing the dual pathway model (Holmes et al., 2015). The BWSS demonstrated good internal consistency in the current study (α = 0.97).
Negative affect
Patient health questionnaire-2 (PHQ-4)
The PHQ-4 (Kroenke et al., 2009) is a four-item self-report measure for depression and anxiety. Participants rate how often they have been bothered by problems over the preceding 2 weeks, with responses given on a four-point scale (0 = ‘not at all’ to 3 = ‘nearly every day’), with overall scores ranging from 0 to 12 (Kroenke et al., 2009). A score of three or greater on the depression subscale indicates likely Major Depressive Disorder (sensitivity of 83% and specificity of 92%; Kroenke et al., 2003) and a score of three or greater on the anxiety subscale indicates likely Generalised Anxiety Disorder (sensitivity of 86% and specificity of 83%; Kroenke et al., 2007). The PHQ-4 demonstrates good convergent validity with other measures of depression, anxiety and negative affect (Mendoza et al., 2024). It has also demonstrated acceptable internal consistency in previous research (α = 0.78; Löwe et al., 2010) and good internal consistency in the current study (α = 0.90).
Statistical analysis
Data were cleaned and tested for assumptions before analyses were conducted. There were 32 missing values for BMI (16.7%). Little’s MCAR test indicated missingness for model variables was completely at random (χ2 = 4.841, p = 0.564). Normality assumptions for all model variables were met, falling within acceptable ranges for skew and kurtosis [−2; 2]. Descriptive statistics were calculated using SPSS software (version 29).
Structural equation modelling using maximum likelihood estimation was conducted using AMOS (version 29). A dual pathway model was initially evaluated, with the results of this analysis used to determine a subsequent model involving only the negative affect pathway. Several model fit indices were utilised as follows: χ2 test of significance (p > 0.05); χ2/df with values ⩽ 2 considered good fit and 2–3 acceptable fit; Comparative Fit Index (CFI) with values ⩾ 0.97 considered good fit and 0.95–0.97 considered acceptable fit; and Root Mean Square Error of Approximation (RMSEA) with values ⩽ 0.05 considered good fit, 0.05–0.08 considered acceptable, and 0.08–0.1 considered mediocre fit (Schermelleh-Engel et al., 2003). The indirect effects of Body Weight Shame and Binge Eating through Restraint and Negative Affect (not including BMI) were also analysed in AMOS using bias-corrected bootstrapping with 5000 resamples.
Results
Descriptive statistics
Table 2 presents descriptive and reliability statistics for, and correlations between, key study variables.
Descriptive Statistics and Correlations for Study Variables.
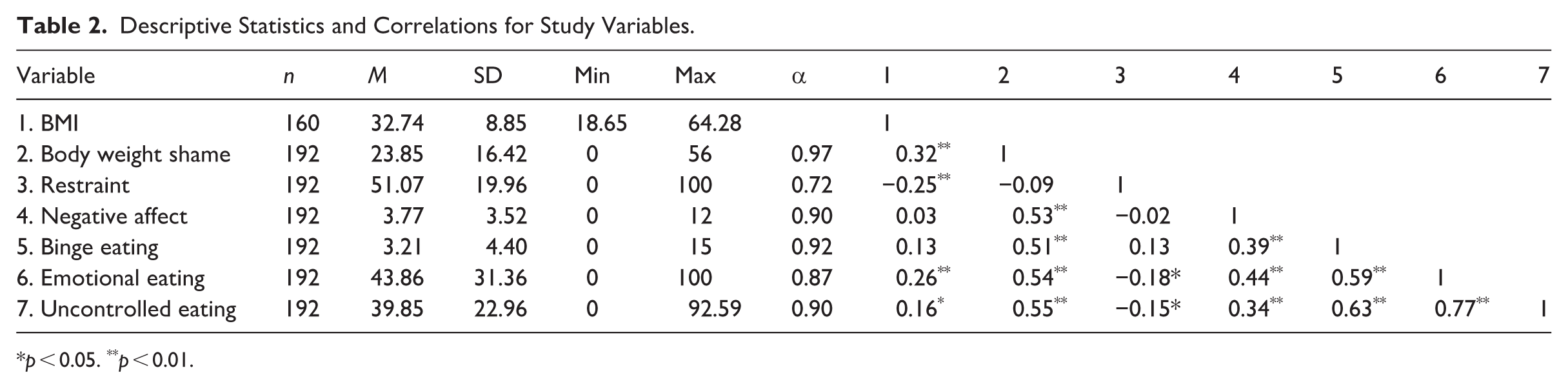
p < 0.05. **p < 0.01.
Structural equation modelling
Figure 2 presents the tested dual pathway model. Path coefficients showed that BMI was correlated with Body Weight Shame (β = 0.32, p < 0.001), Body Weight Shame was correlated with Negative Affect (β = 0.53, p < 0.001), and Negative Affect was correlated with Binge Eating (β = 0.39, p < 0.001). The indirect effect of Body Weight Shame on Binge Eating through Negative Affect was significant (b = 0.06, p < 0.001), suggesting a partial mediating role. However, Body Weight Shame did not predict Restraint (β = −0.09, p = 0.22), and Restraint did not predict Negative Affect (β = 0.03, p = 0.63) or Binge Eating (β = −0.08, p = 0.23). There was no indirect effect of Body Weight Shame on Binge Eating through Restraint (b < 0.01, p = 0.24). Overall, model fit statistics indicated poor fit (χ2 = 43.01, p < 0.001, χ2/df = 10.75, CFI = 0.72, RMSEA = 0.23). An additional path was included from Body Weight Shame to Binge Eating, as was indicated in the Rancourt et al. (2019) study. Model fit improved, however, remained poor (χ2 = 12.68, p = 0.01, χ2/df = 4.23, CFI = 0.93, RMSEA = 0.13).
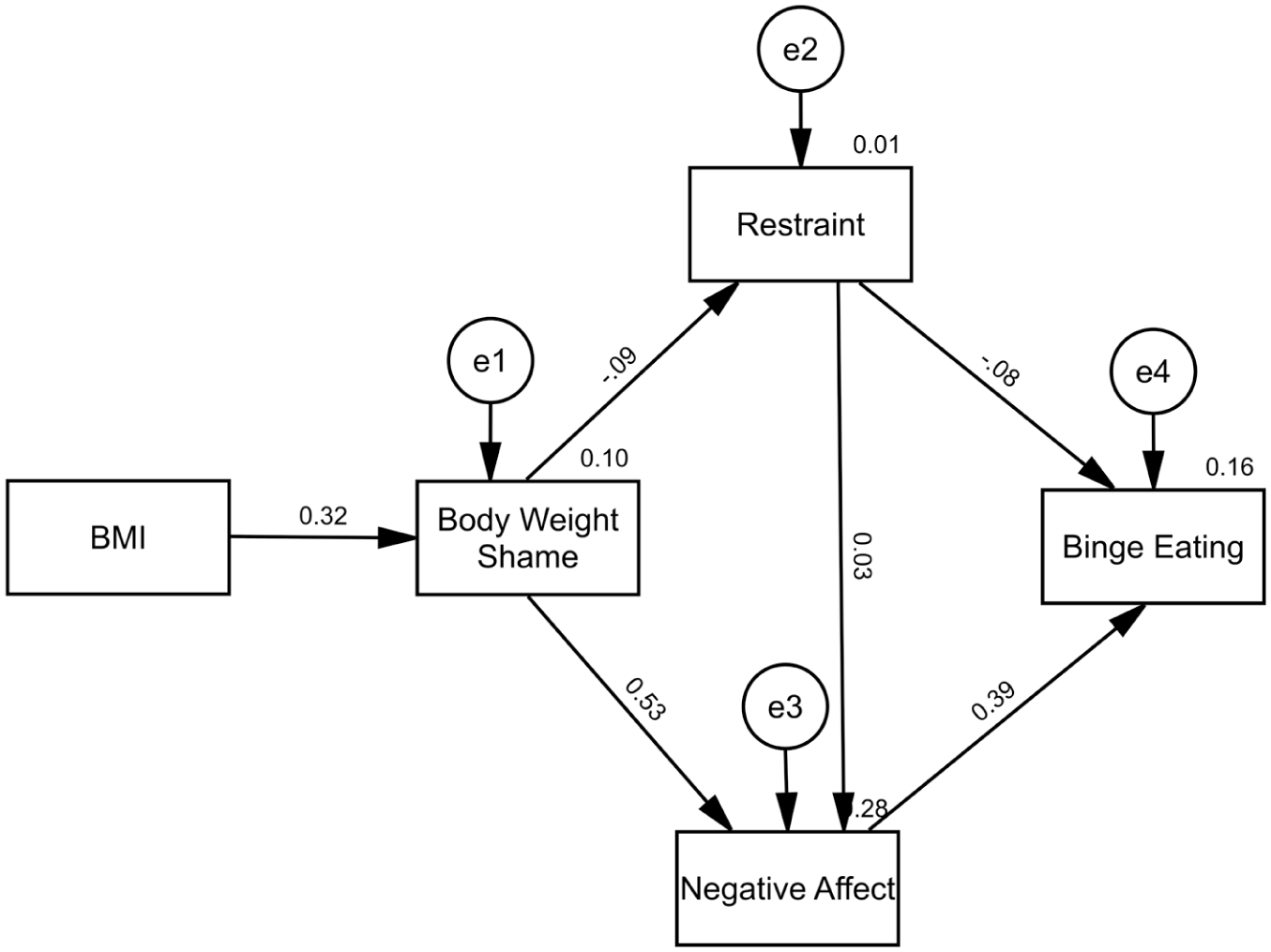
Analysis of the dual pathway model of binge eating.
We subsequently tested the model with the removal of the Restraint pathway to assess if the Negative Affect pathway alone produced a better fit than the full dual pathway model, as presented in Figure 3. Path coefficients showed similar patterns with BMI correlated with Body Weight Shame (β = 0.32, p < 0.001), Body Weight Shame correlated with Negative Affect (β = 0.52, p < 0.001) and Binge Eating (β = 0.42, p < 0.001), and Negative Affect correlated with Binge Eating (β = 0.17, p = 0.02). The indirect effect of Body Weight Shame on Binge Eating through Negative Affect remained significant (b = 0.02, p = 0.04). The model fit indices indicated good (χ2/df = 1.88, CFI = 0.99) to acceptable (RMSEA = 0.07) fit, and the model passed the χ2 test (χ2 = 3.75, p = 0.15).
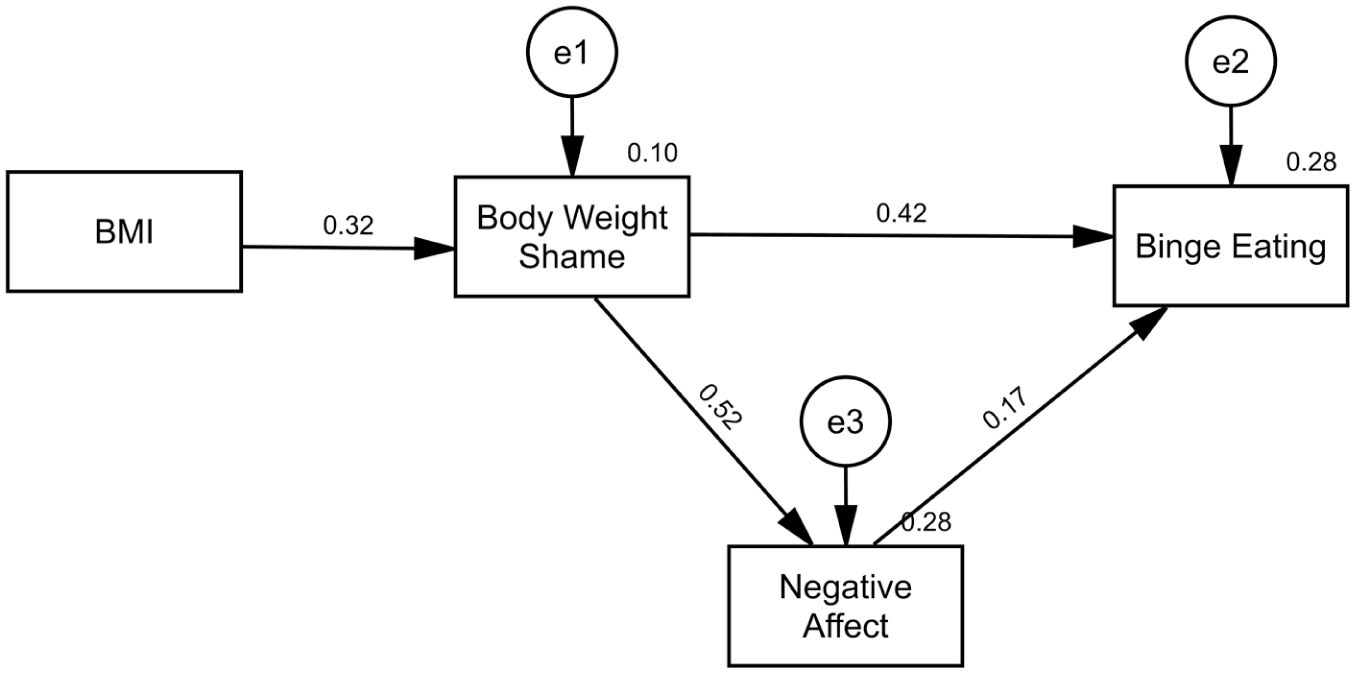
Analysis of the negative affect model of binge eating.
To test if similar patterns were observed for disordered eating more broadly, rather than just clinical binge eating, we subsequently re-ran the models with emotional and uncontrolled eating also included alongside binge eating as a final endogenous latent variable.
Path coefficients showed similar patterns, with BMI correlated with Body Weight Shame (β = 0.32, p < 0.001), Body Weight Shame correlated with Negative Affect (β = 0.53, p < 0.001), Negative Affect correlated with Disordered Eating (β = 0.46, p < 0.001), Body Weight Shame not correlated with Restraint (β = −0.09, p = 0.22) and Restraint not correlated with Negative Affect (β = 0.03, p = 0.63). However, contrary to predictions, Restraint was negatively correlated with Disordered Eating, with an increase in Restraint associated with a small decrease in Disordered Eating (β = −0.17, p = 0.01).
The indirect effect of Body Weight Shame on Disordered Eating through Negative Affect remained significant (b = 0.02, p = 0.02), and there was similarly no indirect effect of Body Weight Shame on Disordered Eating through Restraint (b < 0.01, p = 0.17). Results for the dual pathway model of disordered eating indicated poor model fit (χ2 = 79.83, p < 0.001, χ2/df = 6.65, CFI = 0.85, RMSEA = 0.17). The addition of the path from Body Weight Shame to Disordered Eating improved fit, with some fit indices indicating acceptable (χ2/df = 2.84, CFI = 0.96) to mediocre fit (RMSEA = 0.10). The model did not pass the χ2 test (χ2 = 31.26, p < 0.001), however this may be due to its sensitivity to sample size (Schermelleh-Engel et al., 2003). We again retested the model with the removal of the Restraint pathway to assess if the Negative Affect pathway produced a better fit. Results indicated acceptable (χ2/df = 2.74, CFI = 0.97) to mediocre fit (RMSEA = 0.10); with the model still not passing the χ2 test (χ2 = 21.90, p = 0.01).
Discussion
The current study aimed to evaluate a dual pathway model of disordered eating within a T2DM population. Overall, our findings did not support the dual pathway model in our sample of adults with T2DM. While the negative affect pathway was supported, with negative affect mediating the relationship between body weight shame and disordered eating, the restraint pathway exhibited weak path coefficients and models that included it were inferior than models including the negative affect pathway alone.
To date, there has been limited research on the associations between dietary restraint and disordered eating in T2DM. Kenardy et al. (1994) found no relationship between binge eating and restraint in a sample of women with T2DM. However, Huisman et al. (2023) found that individuals with T2DM who engaged in binge eating had higher restraint scores than those who did not. Additionally, contrary to our findings, Park et al. (2018), van de Laar et al. (2006), and van Strien et al. (2020) found that restrained eating was positively associated with emotional eating. It is noteworthy that all studies finding significant associations between restraint and binge or emotional eating (Huisman et al., 2023; Park et al., 2018; van de Laar et al., 2006; van Strien et al., 2020) used the Dutch Eating Behaviour Questionnaire (DEBQ; van Strien et al., 1986), while our study and that of Kenardy et al. (1994) used variants of the Three Factor Eating Questionnaire (TFEQ; Stunkard and Messick, 1985). When examining differences between the restraint subscales of the TFEQ (Karlsson et al., 2000; Stunkard and Messick, 1985) and DEBQ (van Strien et al., 1986) it could be argued that the TFEQ takes a more cognitive lens, highlighting deliberate, conscious choices, compared to the DEBQ taking a somewhat more behavioural lens, highlighting whether respondents do or do not take certain actions. The discrepancy in previous findings may consequently be explained by restrained eating behaviours, rather than restrained eating cognitions or beliefs, uniquely contributing to binge or emotional eating in T2DM populations. Additionally, 70% of items on the DEBQ restrained eating subscale (van Strien et al., 1986) explicitly refer to weight, compared to 50% of items on the TFEQ-R18 cognitive restraint subscale (Karlsson et al., 2000). Thus, the DEBQ may be capturing primarily weight-related dietary restraint, whereas the TFEQ-R18 may also be capturing dietary restraint driven by other factors, such as those specific to diabetes. This may explain in part why body weight shame did not predict cognitive restraint in our sample.
A further explanation for why the restraint pathway was not supported in our T2DM population may be that a normative level of restraint may act to obscure possible relationships. One study assessing the TFEQ-R18 (Karlsson et al., 2000) in a general population sample (n = 857) found restraint norms as follows: middle-aged males = 22 ± 18; middle-aged females 39 ± 21; teenaged and young adult males = 18 ± 16; teenaged and young adult females = 34 ± 20 (Romon et al., 2004). These norms are notably lower than our mean of 51.07 ± 19.96, suggesting higher-than-average levels of restraint in our sample. This finding is unsurprising given that health professionals commonly recommend dietary restraint as part of T2DM self-management. For certain individuals living with T2DM, cognitive restraint may consequently serve a different cognitive function than that posited by the dual pathway model, stemming from a desire to manage their diabetes rather than purely from body dissatisfaction or shame, further strengthening our hypothesis discussed above.
Our lack of support for the dual pathway model may also be due in part to differences in demographic variables such as gender and age, as the model was originally based on adolescent female populations (Stice, 2001; Stice et al., 1998). Rancourt et al. (2019) found in their T1DM population that restraint was only associated with disordered eating behaviours in adolescents (13–17 years) and young adults (18–25 years), not adults. Given that our sample only included four participants under 25 years, which is not unexpected considering T2DM has a peak incidence at 55 years (Khan et al., 2020), this may have important implications for our results.
Our findings must also be considered in the context of study limitations. Given the cross-sectional nature of the research, we cannot draw conclusions regarding the temporal order or development of the variables analysed. Previous research has suggested that disordered eating may develop prior to T2DM onset (Gagnon et al., 2017; Kenardy et al., 2001; Salvia et al., 2022), often by a decade or more. While restraint did not predict binge eating in our study, we cannot rule out that restraint may still contribute to the development of binge eating, even though it is not a useful predictor once T2DM has been diagnosed. We recommend future longitudinal and ecological momentary assessment-based research to clarify the temporality and development of disordered eating alongside T2DM, building upon our preliminary findings. Future longitudinal research is also recommended to identify risk factors for disordered eating in T2DM, which will guide prevention efforts.
Our conclusions are also limited by the measures utilised in our study. While the supported negative affect pathway resembles Escape Theory (Heatherton and Baumeister, 1991) and Affect Regulation models of binge eating (Hawkins and Clement, 1984), our study did not capture all relevant variables required to test these models, such as cognitive narrowing and reduction of negative affect. We recommend that future research explicitly tests alternate theory-driven disordered eating models in T2DM populations, particularly analysing the function of negative affect. Such future examination of negative affect-based models of disordered eating in T2DM may also benefit from the inclusion of diabetes-specific outcomes, given that SEM research has shown negative affect to also predict poorer glycaemic control and quality of life amongst those with T2DM (Conti et al., 2017).
Additionally, to improve recruitment and reduce participant burden, we utilised short-form measures and screeners where appropriate, given known associations between stated questionnaire lengths and response rates (Galesic and Bosnjak, 2009). One such example is the PHQ-4 (Kroenke et al., 2009). While we found the PHQ-4 to have good internal consistency (α = 0.90), and it has demonstrated convergent validity with other negative affect measures (β = 0.48, p < 0.001; Mendoza et al., 2024), its brevity does limit its ability to enquire about all aspects of depression and anxiety. It may thus be limited in scope to capture the full spectrum of these experiences.
Despite these limitations, our findings have important implications. A key study finding was that cognitive restraint was not a significant predictor of disordered eating behaviours in those with T2DM. This finding is important when considering the screening and assessment of disordered eating and eating disorders in this population. Common eating disorder screening tools such as the EDE-Q (Fairburn et al., 1993), including its dietary restraint subscale, have been found to be highly influenced by living with T1DM (Powers et al., 2013). While diabetes-specific measures exist for T1DM populations, such as the Diabetes Eating Problem Survey Revised (DEPS-R; Markowitz et al., 2010), they are not appropriate or validated for T2DM populations. Since we conducted our study, Klinker et al. (2025) recently published a 10-item version of the DEPS-R, validated in a T2DM population. This work shows promise in addressing the gap in validated measures for those with T2DM. However, further research is required for external validation. In the interim, health professionals should exercise caution when interpreting the results of existing measures on an item-by-item basis.
Our findings also have implications for psychological interventions and the rationale and formulation guiding treatment. Currently, Cognitive Behavioural Therapy (CBT) is the most widely evaluated psychotherapy for eating disorders (Russell et al., 2023). Addressing dietary restraint is a core element of common enhanced CBT protocols (CBT-E; Fairburn, 2008). However, our findings suggest that dietary restraint may play a different function in the formulation of disordered eating in those with T2DM than it does in broader disordered eating populations. While there is some preliminary evidence for the use of CBT-E guided self-help in those with T2DM (Vela et al., 2023), this one existing efficacy and acceptability trial notably incorporated additional content on links between stress and disordered eating in its protocol.
Alternative to the CBT-E model, our finding that only negative affect, not dietary restraint, mediated the relationship between body weight shame and disordered eating indicates that interventions targeting negative affect and affect regulation explicitly may be beneficial. Currently, we are aware of only one trial evaluating the impact of such an intervention on disordered eating behaviours in those with T2DM (Sheikh et al., 2021). A trial of Dialectical Behaviour Therapy (DBT), which is underpinned by an affect regulation model, found that those who received DBT had significantly lower levels of emotional eating at post-intervention than controls (Sheikh et al., 2021). This finding adds further support to a proposed negative affect model of disordered eating in those with T2DM; however, further research is required to assess intervention impacts on other disordered eating behaviours, such as binge eating, and to evaluate alternative psychological interventions.
An alternative psychological intervention of Compassion Focussed Therapy (CFT) may additionally be best suited to target the variable of body weight shame, which we also found to be a significant statistical predictor of disordered eating. While not yet trialled in T2DM populations, CFT has been shown to significantly reduce body weight shame for individuals with higher weight (Carter et al., 2023). While further research is required to assess these interventions in those living with T2DM, in the interim, health professionals should carefully consider individual client presentations and formulations, particularly regarding the role of dietary restraint, on a case-by-case basis.
In conclusion, our findings suggest that a negative affect model may better explain disordered eating than a dual pathway model in individuals with T2DM. Screening for and addressing the psychological domains of body weight shame and negative affect may help us to reduce the impact of disordered eating on the lives of those living with T2DM. Further research is required to assess longitudinal associations, and to test model-informed interventions within this population.
Footnotes
Ethical considerations
This research was approved by the Central Queensland University Human Research Ethics Committee (approval number: 24195).
Consent to participate
Participation was voluntary, and participants provided informed consent to participate and for anonymised data to be published for research purposes after reviewing the information sheet and agreeing to the study prior to survey commencement.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data.
Author contributions
Emma Reid: Conceptualisation, Methodology, Data Curation, Formal analysis, Investigation, Visualisation, Writing - Original Draft.
Melissa Oxlad: Conceptualisation, Methodology, Writing - Review & Editing, Supervision.
Alicia Carter: Conceptualisation, Methodology, Writing - Review & Editing, Supervision.
Talitha Best: Conceptualisation, Methodology, Writing - Review & Editing, Supervision.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by an Australian Government Research Training Program (RTP) Scholarship doi.org/10.82133/C42F-K220.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.*