
Abstract
During the COVID-19 pandemic, the need to triage COVID-19 patients in ICUs emerged globally. Triage guidelines were established in many countries; however, the actual triage decision-making processes and decisions themselves made by frontline medical providers may not have exactly reflected those guidelines. Despite the need to understand decisions and processes in practice regarding patient ICU admission and mechanical ventilator usage to identify areas of improvement for medical care provision, such research is limited. This qualitative study was conducted to identify the decision-making processes regarding COVID-19 patient ICU admissions and mechanical ventilator allocation by frontline medical providers and issues associated with those processes in an ICU during the COVID-19 pandemic. Semi-structured, in-depth interviews were conducted with ICU physicians and nurses working at an urban tertiary referral hospital in Japan between February and April 2022. Patient characteristics that influenced triage decisions made by physicians and the interaction between physicians, nurses, and senior management staff upon making such decisions are discussed in this article. An implicated issue was the lack of legal support for Japanese physicians to practice withdrawal of life-sustaining treatments even during emergencies. Another issue was the impact of non-clinical forces—likely specific to health emergencies—on physicians’ decisions regarding mechanical ventilator allocation, where such forces imposed a significant mental burden on the medical providers. We consider public policy and legal implications for future pandemics.
Keywords
Introduction
Since the start of the COVID-19 pandemic, the overwhelming number of COVID-19 cases requiring intensive care made triage inevitable for frontline medical providers (Azoulay et al., 2020; Herreros et al., 2020; Truog et al., 2020). In the context of COVID-19, the term triage has been used for both patient selection into the ICU and mechanical ventilator allocation during times of medical resource constraint (Truog et al., 2020). Triage was inevitable even in regions like New York that prepared for pandemics via mechanical ventilator securement (Chou et al., 2021; New York State Department of Health, 2015). Consequentially, triage has imposed significant burdens on medical providers (Butler et al., 2020; Mediavilla et al., 2021; Xu et al., 2021).
The Italian and Swiss COVID-19 pandemic guidelines became known for their age-cutoff for intensive care provision to elderly patients (Tyrrell et al., 2021). Such guidelines ignited global discussion on age-cutoff adoption in triage guidelines (Emanuel et al., 2020; The Office of the High Commissioner for Human Rights [OHCHR], 2021). In other nations whose guidelines lack age-cutoffs, the extent to which medical providers consider age when making triage decisions is difficult to assess (Emanuel et al., 2020).
While substantial research on medical providers’ patient admission and ventilator allocation preference (Butler et al., 2022; Merlo et al., 2021), mental health (Laurent et al., 2021; Song et al., 2021), and general ICU experiences (Moore et al., 2022; Parsons Leigh et al., 2021) during the pandemic has been conducted globally, studies on the actual triage process/decisions are limited (Orfali, 2021). This trend also applies to Japan, where triage preferences of medical providers and ethical/social issues during the COVID-19 pandemic were studied, but research on the actual triage process/decisions and issues surrounding those processes is lacking (Norisue et al., 2021; Seino et al., 2022).
By June 30, 2020, Japan reported a total of 974 deaths—most of which were patients above 70 years old—compared to 128,250 deaths in the United States (Cabinet Secretariat, 2020; Mathieu et al., 2020). Just examining the numbers, one may think the burden imposed on Japanese medical providers was comparatively less. However, the number of hospitals that accepted COVID-19 patients was also comparatively low—only 18% of all medical institutions accepted COVID-19 patients by June 1, 2020 (Ministry of Health, Labour and Welfare, 2020). Accordingly, COVID-19-admitting hospitals were overflooded with COVID-19 patients (Seino et al., 2022).
In Japan, there is inadequate discussion and information regarding triage practices in the context of pandemics. Reasons for the lack of discussion include the general uncomfortableness surrounding discussion concerning death and the lack of daily clinical issue discussions by hospital ethics committees (Ikka, 2013; Norisue et al., 2021; Seino et al., 2022). The absence of national guidelines and consensus regarding triage during the pandemic—only the availability of ventilator allocation guidelines released by professional medical organizations—has limited public understanding of the actual triage process and decisions made by frontline workers (Sawamura et al., 2020). Given this background, we conducted a study to identify the actual decision-making processes and decisions regarding COVID-19 patient ICU admission and mechanical ventilator allocation by frontline medical providers, as well as issues associated with the processes.
Methods
Interview Site
The interview site was an ICU within a tertiary-care hospital (hereafter “Hospital-A”), capable of hospitalizing about 500 patients overall, that mainly accepted moderate to critical COVID-19 cases from the earliest period of the pandemic. Located in a metropolitan city in Japan, in early 2020, Hospital-A experienced one of the largest in-hospital clusters in Japan. Hospital-A did not perform extracorporeal membrane oxygenation (ECMO) for COVID-19 patients but accepted those who required mechanical ventilation. They could accept 16 COVID-19 patients simultaneously: 9 moderate, 4 severe, and 3 critical cases requiring mechanical ventilation, according to the World Health Organization’s (WHO) COVID-19 case classification (WHO, 2021).
Participants
We asked the ICU’s leading physician (hereafter “L.P.”) to recruit both physicians and nurses working in Hospital-A’s ICU. The purposive sampling method was adopted to ensure all participants had experience in caring for COVID-19 patients.
L.P. asked all ICU physicians (n = 6) who completed their subspecialty training for intensive care and looked after COVID-19 patients since the pandemic unfolded in spring 2020 to be interviewed for our research. Documents explaining the research objectives, ethical considerations, and interview themes were sent along with the recruitment email.
ICU nurses who met the following criteria were recruited: 1. Took care of COVID-19 patients during the fifth surge, caused by the Delta variant, in Japan (the fifth surge, defined by Anan et al. (2022), happened between July and September in 2021). 2. Joined the emergency center before FY 2020 and have worked in the ICU from pre-pandemic times. 3. Had various work experience ranging from novice to management-level staff who fulfilled conditions (1) and (2).
50% (n = 3) of physicians and 24.4% (n = 10) of nurses agreed to be interviewed. Work experiences of the nurses ranged from 3 to 23 years, and their positions (in increasing hierarchy) were either “staff,” “chief,” or “vice leader.” Physicians’ work experience ranged from 8 to 21 years, and all were associate professors. Nurses and physicians were randomly assigned unique codes N1 to N10 and D1 to D3, respectively.
Ethical Considerations and Data Collection
This study was approved by the Institutional Review Board of Grinnell College (ID # 21-22-4) and the Ethics Committee of Tohoku University (ID # 2021-1-678). The interview schedule was made when a declining trend was observed in the number of COVID-19 cases. However, preceding the interviews, another surge started, and medical providers were faced with intensive work during the interview schedule (Ministry of Health, Labour and Welfare, 2021). Informed consent was obtained from all participants after they read the document with general information of the interview—including the project aim and data confidentiality—and listened to the first author read aloud the research principles before the interview. Consent was obtained verbally and via signature on a consent sheet, which was sent back to the first author electronically via email. No relationship existed between the researchers and participants before the interview.
Semi-structured interviews were conducted online in Japanese and recorded. Each participant was interviewed once for 40–70 min. Recording started after obtaining verbal consent. One-on-one interviews were conducted by the first author with nurses. Two-on-one interviews were conducted with physicians, where the second author joined the first author to assist with technical terms. Interviewees discussed major findings after each interview to gain a shared understanding of each interview. Additional information and clarification were obtained via email when necessary. A sample interview guide is available in the supplementary material.
Data Analysis
Interview recordings were transcribed verbatim in Japanese and then translated into English. Translations were reviewed by native Japanese researchers and discussed with English-speaking researchers to maintain the original meaning and nuances. Content analysis was conducted, where two researchers first conducted open coding of the verbatim transcript, whose codes were compared, and a consensus was reached (Bernard, 2017; Elo & Kyngäs, 2008). The code definitions were clarified and reviewed iteratively throughout the entire process. Codes were then compared and grouped into higher order categories. Before submitting the article, a stakeholder check was conducted.
Definitions
In this study, Japan’s Ministry of Health, Labor and Welfare’s (MHLW) definition of “elderly people” was adopted, defined as those over the age of 65 (MHLW, n.d.). Additionally, WHO’s (2021) COVID-19 case classification (moderate, severe, and critical) was adopted. In this article, triage will refer to the situation where certain patients were prioritized over others upon ICU admission and mechanical ventilator allocation (Truog et al., 2020).
Results
Four themes were identified each for ICU patient admission and mechanical ventilator allocation decision-making (Figures 1). The decisions and decision-making processes for COVID-19 patient admission into the ICU and mechanical ventilator allocation are presented below in detail according to themes and subthemes. (a) Identified categories for decisions and decision-making processes by frontline medical providers regarding ICU patient admission. (b) Identified categories and subcategories for decisions and decision-making processes by frontline medical providers regarding mechanical ventilator allocation in the ICU.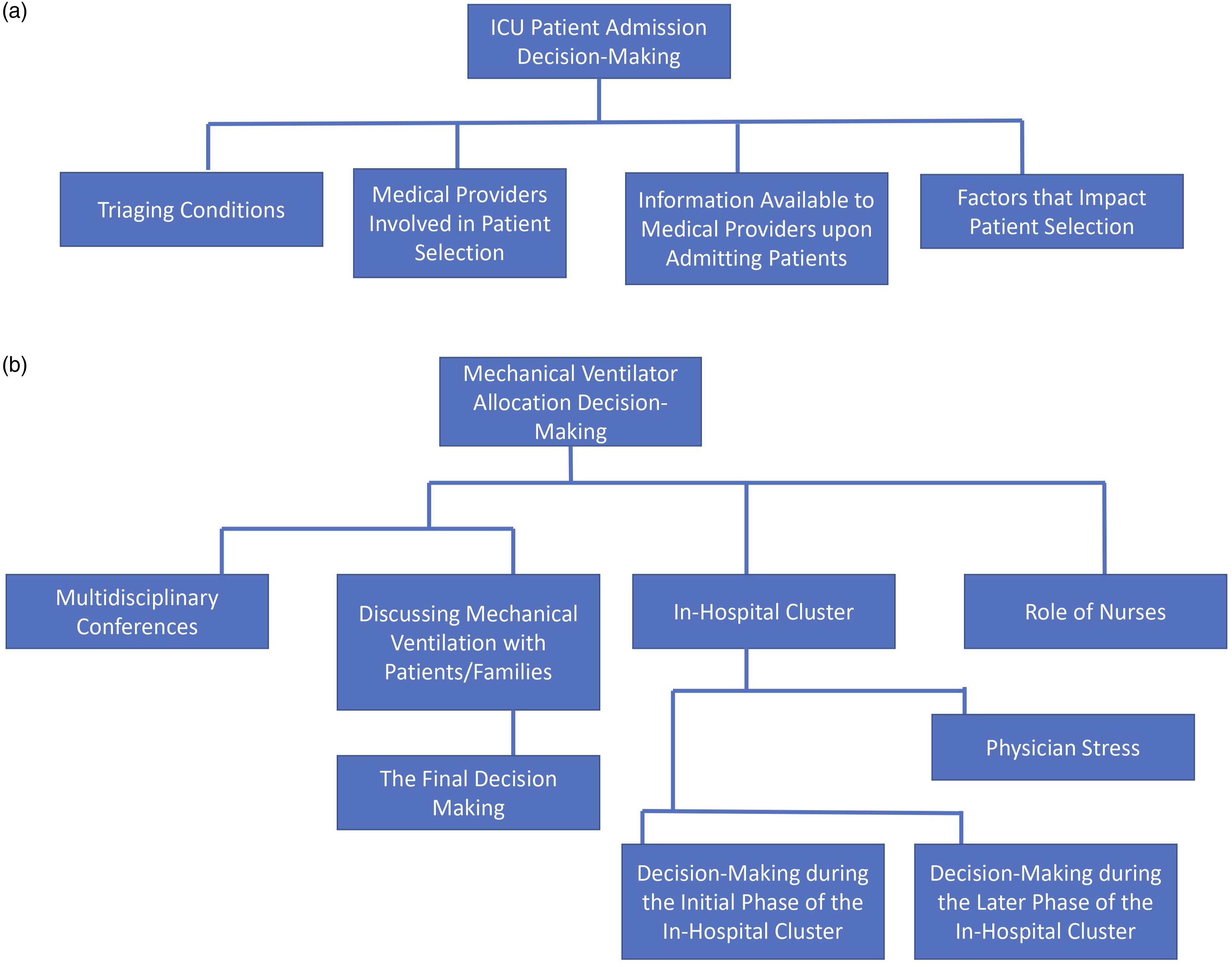
Patient Admission Into the ICU
Triaging Conditions
Triage occurred throughout different periods of the pandemic, especially during the fifth surge and the in-hospital cluster. The fifth surge was characterized by the unprecedented increase in severely/critically ill, non-elderly patients due to two main reasons: low vaccination rate of non-elderly population resulting from elderly vaccination prioritization and the surge of the Delta variant, which caused severe diseases compared to predecessor variants (MHLW, 2022). Physicians had to choose whether to admit elderly or non-elderly patients. The fifth surge was expressed as “an extremely tough period” (D2). However, physicians sometimes “had no time” (D2) to triage; they instead accepted patients on a first-come, first-served basis. I accepted patients on a first-come, first-served basis; the fact that those things [medical resource allocation] weren’t effectively carried out was stressful for the medical staff. (D2)
Medical Providers Involved in Patient Selection
When Hospital-A received calls regarding potential COVID-19 patient admission from emergency medical services/a municipal team dedicated to COVID-19 patient-transfer, the on-duty floor-managing physician selected patients mostly without consulting others. Only chief and managerial level nurses (Figure 2) were consulted regarding the admission of severely/critically ill COVID-19 patients that might require special nursing care. For example, N3 described how accepting a patient with severe cognitive impairment was difficult: I’m not in a position to decide; the floor-managing physician decides, but sometimes I’m asked for my opinion. For example, I’ve said it’s very difficult to treat COVID-19 patients with cognitive impairment or mental illness. Those patients who wander around need constant nursing care, and it’s difficult and risky for us to go into their rooms to care for them, wearing PPE [personal protective equipment] for many hours. We don’t want COVID-19 patients to wander around the room and fall, so I found those cases difficult to deal with. It was difficult, but when such patients were one of the patients who wanted to be hospitalized, I didn’t say “I don’t want to treat them,” but rather, I said, “taking care of them at our facility is difficult.” (N3) Organizational chart for the ICU division at Hospital-A.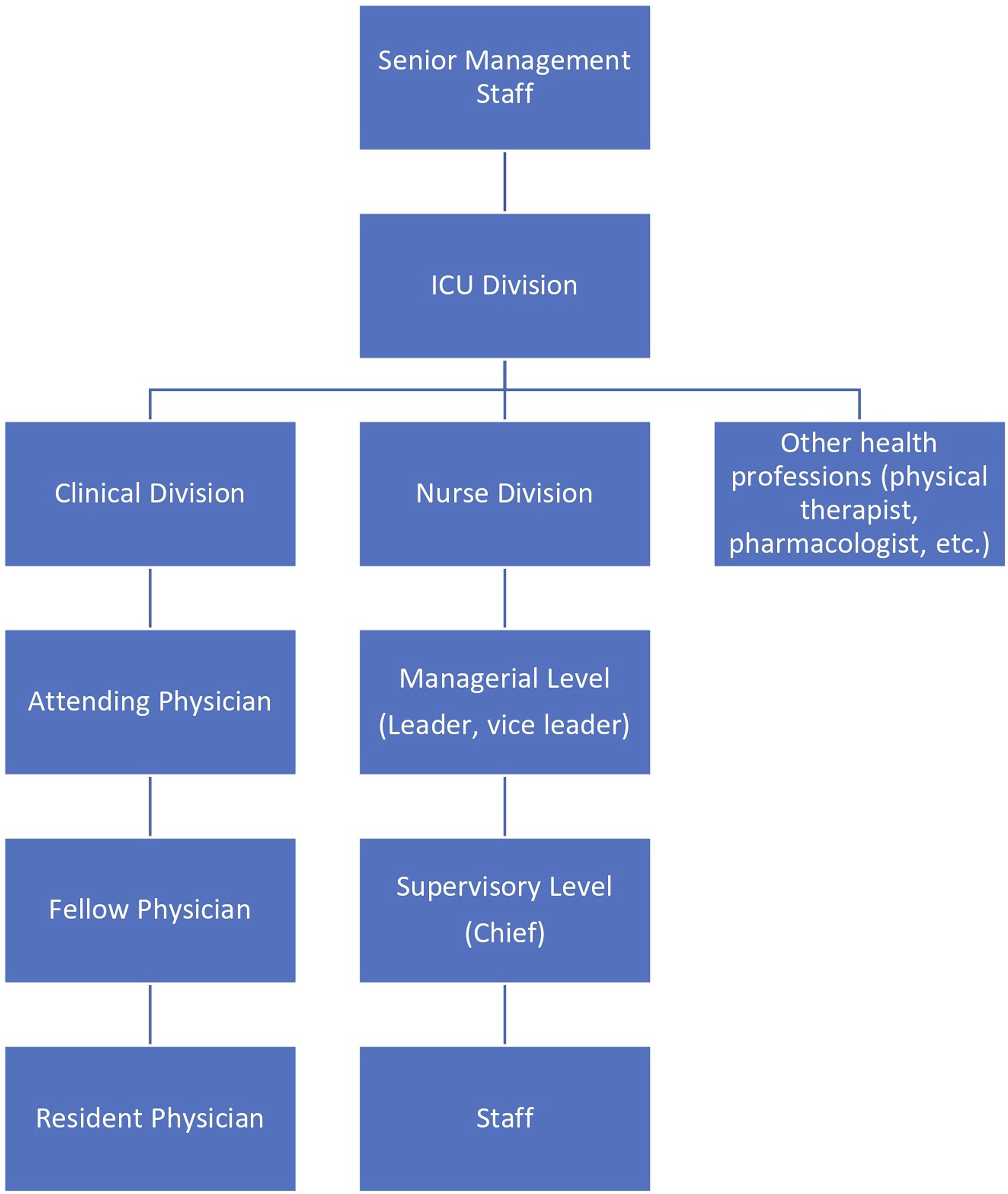
Only participants with triage experience mentioned that triage was happening. A young nurse, with no prior patient selection experience said, “I’m not sure of the [patient admission] decision-making process …” (N1).
A physician was uncertain about how other peer physicians selected patients; this indicated that physicians made decisions on their own. Interviewer: You mentioned earlier that you sometimes accepted younger patients at your own discretion, but did other physicians tend to do the same? D3: I don’t think there was a huge difference. I think there was a strong tendency to accept younger patients. There may have been physicians who believed the patients’ age or ADL [activities of daily living] shouldn’t affect [their decisions], and those physicians may decide whether to accept a patient solely based on the patient’s symptom severity.
Information Available to Medical Providers Upon Admitting Patients
The main information available to the floor-managing physician when selecting COVID-19 patient(s) for admission included the patient’s COVID-19 symptom severity, age, ADL, and public assistance reception status. The information we received included the infection status of family members living with the patient, whether the patient was receiving public assistance, and their COVID-19 symptom severity. (N2) When I had to decline all requests, about 20 cases per night, if a unit became available, I tried to take the next person who was previously relatively healthy but was severely ill [because of COVID-19]. For example, if a person who was 50 years old, who used to work before infection had severe COVID-19 pneumonia; oxygen saturation of 70%; and absolutely required ventilation, we would say, “Yes, we’ll admit him.” (D1)
Factors That Impact Patient Selection
Among the patient information available to the medical providers, factors that affected the patient’s likelihood of being admitted into the ICU were reported to be the patient’s pre-infection ADL, age, and symptom severity. Public assistance reception status did not impact patient selection. COVID-19 severity information helped physicians decide whether a patient required/may require ICU care. As a tertiary hospital with advanced medical devices, Hospital-A was expected to admit the city’s severe/critical cases, which led to the prioritization of those cases. Physicians predicted the patients’ survival chances and quality of life (QOL) after recovery based on the patients’ pre-infection ADL and age. The higher the ADL independence level and younger a patient, the higher the chances of recovery and the more likely the physicians were to admit the patient. I feel that patients are healthy until about 20, 30, 40, 50, or the first half of 60. If they don’t have any preexisting disease, I consider patients in their late 60s to mid-70s to be early seniors. Those between 75 to 84 are quite frail, and those above 85 are extremely frail in my impression. Their age and pre-infection ADL I mentioned earlier are also important. If a person is 68 years old but had a cerebral infarction five years ago and is paralyzed and does his best to go to the bathroom by himself, but uses a care cab to visit the hospital, he might be 68, but his body would be older . . . I always try to judge holistically. (D1)
Decision-Making Regarding Mechanical Ventilator Allocation
Once patients were admitted to the ICU, the next medical decision to be made was patient treatment. After admitting a patient into the ICU, medical providers asked the patient/family about their treatment preference. We always check [with the patient] at an early stage of hospitalization whether they prefer mechanical ventilation or similar treatments, or whether we shall endeavor to provide conservative/internal medical treatment other than ventilation. (D1)
When the blood oxygen level of patients decreases to a critical level, mechanical ventilation becomes necessary. While guidelines exist for mechanical ventilator usage, the decision-making is largely dependent on each physician because the decision entails prognosis analysis, followed by a risk-and-benefit assessment. I think the most important point of discussion or consultation would be decisions regarding mechanical ventilator allocation. We also must decide whether a ventilator would be beneficial to the patient. (D3)
Hospital-A’s ventilator availability didn’t impact their decisions regarding mechanical ventilator allocation during the pandemic, even during surges, except during the in-hospital cluster (see the section Special Case: In-Hospital Cluster). Ventilator shortage was not an issue at Hospital-A as they did not take patients beyond their bed capacity, which was less than the number of ventilators they had. At our hospital, it seemed like the hospital bed availability was reaching the limit faster than the mechanical ventilators. Therefore, we never had to reject ventilation requests from our patients because of ventilator shortage. (D3)
Below, the decision-making processes for mechanical ventilator allocation are laid out.
Multidisciplinary Conferences
Multidisciplinary conferences were held by physicians, nurses, social worker(s), pharmacist, and physical therapist(s). Multiple physicians and nurses were involved, including those who oversaw patients and those in leadership positions. Resident physicians and young nurses were not usually asked to participate. During the pandemic, the conference was held specifically for COVID-19 patients who met the following criteria: no relatives, unconscious, ADL-dependent, and low recovery chances even with mechanical ventilation. For patients who don’t have family members with whom they can consult, but we have to say, “I don’t think it’s in the patient’s best interest to escalate the treatment any further,” we often hold multidisciplinary conferences. (D1)
Multidisciplinary conferences were usually held when medical providers in charge of a COVID-19 patient weren’t inclined to escalate care, often regarding mechanical ventilation. Discussion between multiple medical professionals regarding mechanical ventilator usage prevented physicians from being the only one responsible for the decisions. Decisions were made using Jonsen’s Four-Topic Approach during the conference (Jonsen et al., 1982). The physician cannot just decide by themself that a patient wouldn’t use a ventilator. For example, it would be unethical for me to say, “Oh, we don’t need [a ventilator for] this person”; so I hold a multidisciplinary conference to confirm that everyone agrees with my opinion . . . The physician would present the overall information, then, using the four-topic approach, they’d write on the whiteboard the amount of pain the patient would suffer and the amount of benefit that the patient would receive from the treatment. Just because the patient lives alone and has no relatives doesn’t mean that we should abandon them. We may decide to do our best to give them conservative medical treatment, like intravenous infusion and regular oxygen administration. However, we might agree that ventilation, dialysis, ECMO, etc., won’t benefit them and that it’ll only be painful; we confirm that everyone’s consensus is that the best treatment plan for the patient is to not use a ventilator, and officially document it. The physicians and nurses document [the patient’s situation] and then multiple professionals examine the facts from their own point of view [to judge the appropriateness of not allocating a ventilator]. (D1)
Participants unanimously agreed there were no significant disagreements among the medical professionals during the multidisciplinary conference: Everyone who examined the situation would think that ventilation would be painful for the patient and other people too, so we never really disagreed upon making a decision [regarding mechanical ventilation] during the multidisciplinary conference. (D1)
Discussing Mechanical Ventilation With Patients/Families
For patients who did not require multidisciplinary conferences, physicians explained COVID-19 treatment options and recommendations to the patients/family. Even if the patient isn’t that old, if they have an underlying disease, or if they’re weak, but they are conscious, we make treatment decisions together, taking their previous ADL into consideration. When the patient is unconscious, we decide with the family. (N9)
How physicians discussed mechanical ventilation to the patients/families depended on the patient’s age and medical history/underlying disease, which were used to predict mechanical ventilation effectiveness for COVID-19 patients. Here, we present how physicians introduced and explained mechanical ventilation to patients based on the patient type: elderly and frail; elderly and immunocompromised; non-elderly patients who are not severely immunocompromised; and non-elderly patients who are severely immunocompromised.
Explanation of Mechanical Ventilator Usage to Elderly, Frail Patients
One physician insisted that Japanese physicians are unlikely to recommend usage of mechanical ventilators to elderly patients because in Japan, withdrawing care might be considered murder; physicians thus wanted to avoid risks and were careful about placing elderly, frail patients on a mechanical ventilator. In Japan, the so-called withdrawal-care is an ethically controversial issue, and the academic societies are now sorting it out. Withdrawal-care is the decision to remove a ventilator when there is no hope of recovery after treatment. Our department has decided that it’s not yet ok for me to do it here in Japan, so I never say, “let’s just try using a ventilator.” (D3)
Before elderly, frail patients and/or their families made a decision regarding mechanical ventilation, physicians explained that their survival chance would be low due to their frailty, and even if they survived, their QOL would be severely compromised. A physician mentioned they would explain the potential scenarios of ventilator usage to the patient/family: So the family doesn’t suffer later, I categorized the ventilator treatment outcomes into three possibilities: the possibility that the patient won’t survive even if allocated a ventilator, the possibility that the patient could ultimately extubate and survive, and the possibility that the patient will be bedridden with a tracheostomy and be connected to a ventilator forever. If the physician says none of the above has zero possibility, the patients wouldn’t know what the percentage distribution is, so they wouldn’t be able to decide . . . So, for example, if a patient needs nursery support to eat every day, I would explain that there is a 60% chance that they won’t survive even if allocated a ventilator, a 10% chance or less that they will survive after extubating, and about a 30% chance of surviving but being weaker more than now, require a tracheostomy, and be connected to a ventilator forever, and that the last scenario would be considered a huge success. If the family says, “Oh, really? Then please don’t use a ventilator,” I won’t. But if they still prefer to use the ventilator even if the patient becomes bedridden and connected to a ventilator forever, I’ll do what they prefer. (D1)
When an old, bedridden patient and their family preferred ventilation in opposition to the physician’s suggestion, the physician re-explained and emphasized how much the treatment could make the patient suffer and lower their post-ventilation QOL. They mentioned the patient and/or family would usually agree with them to withhold care after re-explaining. The phrase I use is, “If the ventilator cannot be removed, the patient will need a tracheostomy, which will make it difficult for the patient to speak and eat. In the long term, the patient will be bedridden and unable to communicate; will have to live in a hospital or at home, lying in bed; will eventually develop pneumonia or some other infectious disease again and again; and will be hospitalized repeatedly. Eventually, the body will wear out and die” . . . Mostly, when I reiterated my explanation, they would say something like, “I wouldn’t prefer it if that’s the case.” I would change my suggestions and level of recommendation [when re-explaining]. (D3)
When elderly patients, especially those in their 80s and 90s, did not prefer ventilation but their family did, the physician would explain to the family that “the patient doesn’t prefer care escalation” (N2) and that they would respect the patient’s decision. For example, there are cases where the patient does not want to use a ventilator, but the family asks for it, and in such cases, we basically tell the family that we’ll respect the patient’s wishes. (D3)
Explanation of Mechanical Ventilator Usage to Elderly, Immunocompromised Patients
If the patient was immunocompromised, physicians explained to the family that mechanical ventilation may cause complications and worsen the patient’s situation compared to immunocompetent patients. Basically, we explain the benefits and risks of using a ventilator. If the patient uses a ventilator, there are concerns of other complications, since various sedatives and, sometimes, muscle relaxants [i.e., neuromuscular blocking agents] are used to put the patient completely to sleep. In such cases, there’s a possibility that patients with underlying diseases—not just lung disease—may develop complications, so even if the symptoms of COVID-19 are alleviated, there were many patients whose general condition deteriorated due to complications. (N6)
Explanation of Mechanical Ventilator Usage to Non-Elderly Patients Who Are Not Severely Immunocompromised
For patients up to about 60 years old, physicians strongly suggested ventilator usage; some mentioned that there was no other option but to use a ventilator. They also explained that there was a potential for requiring a tracheostomy, but that they can recover: “Ventilation is the best option. We may need to perform a tracheostomy, but we can get over it together” (N3). Another phrase used by physicians was: “Because you’re young, you should be placed on the ventilator” (N4).
Explanation of Mechanical Ventilator Usage to Non-Elderly Patients Who Are Severely Immunocompromised
Depending on the patient’s pre-infection ADL, age, and symptom severity, physicians explained the risks and benefits of ventilation to the patient/family. The extent they recommended mechanical ventilation depended largely on the type and degree of their underlying disease. Even if the patient is young, if they have a serious underlying disease, we say “We may need to do a tracheostomy, which may be difficult [in terms of long-term outcome].” We would discuss the risks and benefits of the procedure depending on the patient’s background [i.e., medical history] before the family decides. (N3)
The Final Mechanical Ventilation Decision-Making: Asking the Patient/Family Their Ventilation Preference Upon Deterioration of Their Medical Condition
Medical providers are encouraged to seek consent to use ventilators from their patients/families whenever possible (Japan Federation of Bar Associations, 2011). Families are consulted too when possible, since the Japanese tend to cherish family involvement in important decisions (Nagai, 2016).
When patients were at the point of requiring ventilation, physicians asked them their preference regarding mechanical ventilation, regardless of their prior preference. No matter what the physician’s view regarding mechanical ventilator usage for a patient was, if the patient/family rejected their suggestion, the physician followed the patient/family’s treatment preference. If their [the patient/family’s] decision [to use a ventilator] didn’t change even after I explained the consequences, I decided to put the patient on a ventilator because there was no other choice. (D3)
Role of Nurses in the Context of Treatment Decision-Making
While treatment suggestions/recommendations were made primarily by physicians, nurses occasionally impacted the suggestions/recommendations.
Nurses interacted with patients longer than physicians. Hence, patients were more likely to discuss their honest feelings toward treatment options with nurses than physicians. When nurses felt their patient had shared something related to treatments that physicians should know, they communicated the patient’s feelings with the physicians. Physicians sometimes asked nurse leaders what treatment they thought might be best for the patient.
Some physicians used the information from nurses to decide how to improve patient satisfaction regarding the treatment they recommended. For example, D3 was unlikely to change their treatment recommendation based on information from nurses, but rather used them to assess whether they should re-explain the treatment recommendation. Since they [nurses] are the closest to the patient, they often tell me what the patient thinks about a treatment, what they said after a physician explained the treatment, or what they said when they came to their senses. If a nurse said it’d be better to talk to the patient once more, I’d talk to them again. (D3)
Special Case: In-Hospital Cluster
Because the medical staff deemed their hospital’s response to the in-hospital cluster as controversial and “highly sensitive” (D3), information on this topic was provided by only few physicians.
The in-hospital cluster occurred during the earliest stage of the pandemic in 2020. Ventilator shortage occurred and ICU demand increased during this period since patients hospitalized for non-COVID-19 reasons became infected and many of them were critically ill. The ventilator allocation decision-making during this period was different from other periods and could be divided into two phases: the initial and later phases. The mechanical ventilator allocation decisions and decision-making processes for each phase are presented below.
Initial Phase
Initially, due to the limited ventilator availability and capacity of providable care, in addition to studies that reported the high mortality of elderly patients despite being placed on a ventilator, a physician (D2) explained to patients above the age of about 80 that even if they are placed on ventilators, they have a low survival chance (Grasselli et al., 2020; Richardson et al., 2020). D2 mentioned they did not necessarily explain the merits of mechanical ventilation to their patients. Reflecting on this experience, D2 mentioned their thought process was affected by the state of emergency. I think we were explaining to the elderly patients in their 80s and 90s, those with a high degree of frailty, that it would be very difficult [to survive] even after mechanical ventilation ... We probably should have mentioned that we’ll do our best regardless of their decision … The way physicians explained mechanical ventilation varied, so I think we needed to be careful. I feel that this result was due to us being caught up in a “disaster mode.” (D2)
Later Phase
D3 mentioned they were urged by the senior management staff to change how they explained mechanical ventilation as a treatment option: to strongly recommend mechanical ventilation by minimizing the explanation of its potential risks/harms. . . the senior management staff noticed that many hospitalized [in-hospital cluster] patients were dying, and [they] suddenly started discussing placing all patients on ventilators . . . It would be more correct to say that I was told to change my explanation [regarding mechanical ventilator usage towards patient/families] . . . To be honest, depending on the way the medical staff explained to the family, for example, if I say, “there’s the option to not use a ventilator, but we believe you should use it,” the families usually don’t disagree with us. However, if we emphasize the risks [of ventilation] too much, there is a possibility that the families will refuse ventilation, so during [the later phase of] the in-hospital cluster, we had to actively direct them to use ventilators by saying “We strongly recommend it” . . . From the hospital’s standpoint, placing all patients on ventilators seemed to be in their favor. I think they were desperate to know how many patients died after all treatment measures have been taken due to rising concerns about medical malpractice lawsuits. However, whether mechanical ventilation really improved the patients’ medical conditions depended on each patient, so I can’t make a blanket statement; I think it’s a case-by-case basis. Some patients improved, while others had to fight the disease for a long time and eventually died. (D3)
Physicians’ Stress Associated With the In-Hospital Cluster
A physician regretted persuading patients to avoid ventilator usage during the initial phase. The physician repetitively mentioned “反省 (hansei),” which means to reflect and regret one’s actions. I’m unsure if we were making the right decisions at the time of the cluster; it was a dilemma for me … I cannot change what has already happened even if I regret and deeply reflect on it, but I feel that it must have been a very bizarre and disastrous situation . . . I think I may have given a slightly biased opinion regarding what their prospects were and am regretting it ... to be honest ... (D2)
The later phase of the in-hospital cluster also placed immense stress on the physicians and impacted their mental health. When I reflected on the in-hospital cluster that occurred, I noticed I probably had clinical depression. I believe I was clearly in a depressive state, and now that I look back, I must have been under a lot of stress. When I was told to take a stress checkup from the hospital during the pandemic, my stress level was really high . . . I had to place patients on ventilators and things were abnormal; I thought I was doing okay, but in reality, I was extremely stressed out. (D3)
A physician shared their struggles regarding the placement of all critically ill COVID-19 patients on mechanical ventilators. When we were told to allocate ventilators to everyone, it was a real dilemma, and I was conflicted as to whether we should really do that … I’ve told them [the senior management staff] this isn’t right, but they seemed really irritated. (D3)
Discussion
The COVID-19 patient mortality in Japan is considerably lower than many Western countries (Mathieu et al., 2020). However, this study revealed the significant struggles of Japanese frontline ICU staff regarding COVID-19 patient triage. Overall, triage decisions were primarily made independently by each attending physician. Occasionally, leader nurses and nurses in charge of patients were consulted. Physicians were likely to prioritize admission of, and ventilator allocation to, patients who were more likely to recover, predicted by their underlying disease, age, pre-infection ADL, and COVID-19 symptom severity, which were globally adopted criteria in guidelines for ICU admissions and medical resource allocations (Tyrrell et al., 2021). For admitted patients who required/likely required mechanical ventilation, if patients met the four criteria (no relatives, unconscious, ADL-dependent, and low recovery chances even with mechanical ventilation), multidisciplinary conferences were held, and a consensus was reached by the attending medical providers regarding mechanical ventilator usage. Otherwise, physicians explained the risks/benefits of mechanical ventilation to the patients/families and asked for their preference.
Upon deciding whether to provide mechanical ventilation to elderly patients, physicians made decisions more carefully and were more hesitant to recommend its usage compared to non-elderly patients. Behind this tendency is the social background where in Japan, withdrawing care still carries the risk of murder charges, despite a growing international consensus that such an act is not murder (Aita & Kai, 2009; Emanuel et al., 2020). Historically, in Japan, there have been ventilator withdrawal cases by physicians that were referred to prosecutors, most of which were dismissed but some charged with murder (Ogata, 2014; Tanaka & Kodama, 2016). Ventilator withdrawal hesitancy remains strong also because of the mental burden associated with withdrawing life-sustaining treatments (Aita & Kai, 2009). To reduce physicians’ stress associated with mechanical ventilation decision-making, there’s a need for hospitals to adopt a systematic, multidisciplinary decision-making approach (Daugherty Biddison et al., 2019). Public discussion regarding the establishment of national medical guidance/laws that explicitly support withdrawing care, especially during emergencies, is also necessary.
Despite this tendency to avoid placing patients who may not be able to extubate on mechanical ventilators, during the later phase of the in-hospital cluster, physicians were influenced by senior management staff and mentioned they were urged to intubate every in-hospital cluster COVID-19 patient. Physicians presumed the management staff were concerned the hospital would be held accountable for the cluster, leading to lawsuits; by allocating ventilators to every patient, families will likely believe the hospital endeavored to save the patients. Yet, we must be mindful that this was the physician’s personal take, and it’s possible the senior management staff had different viewpoints. Overall, these findings suggest the need to develop a system that ensures all medical staff are in communication even during medical emergencies, so important decisions can be shared and discussions can take place to avoid confusion.
To understand the in-hospital cluster outcomes communicated by the physicians, it’s important to understand the social context of both the interviews and the in-hospital cluster. The period the interviews took place—spring 2022—likely affected how medical providers reflected on their dilemmas/actions; had COVID-19 medical counter measures still not been available during the interview, the interviewees may have responded differently. As for the senior management staff attitudes during the in-hospital cluster, it’s plausible they were impacted by the social tendency to denounce in-hospital clusters as a failure of infection prevention/control practice, attributing to hospital mismanagement and inadequate medical precaution (Eiju General Hospital, 2020; Honda, 2021).
For senior management staff to influence clinical decisions, transparency and accountability is essential to gain public/patient trust and to reduce the stress of frontline workers. Research supports the importance of evidence-based medical decisions as opposed to decisions based on non-clinical forces, like pressure from management-level staff, which entails the risks of negative clinical consequences (Hajjaj et al., 2010; Janati et al., 2018). More research on effective measures that could protect physicians/patients from non-clinical forces is essential to make fair medical decisions and maintain care quality, even during medical emergencies. A first step may be to determine the effectiveness of holding regular meetings between frontline medical providers and senior management staff in sharing and clarifying each other’s thoughts and concerns. In situations where tension is high, a neutral third party may assist in facilitating the discussion.
While age-cutoffs were adopted in the ICU COVID-19 patient admission guidelines in countries like Italy and Switzerland, age-cutoff was largely avoided at Hospital-A (Tyrrell et al., 2021). Instead, age was considered as one of the important clinical data necessary for triage decision-making, where often a higher age was positively associated with a lower recovery chance. Internationally, age-cutoff adoption in triage guidelines has been criticized (OHCHR, 2021). However, in a super-aging society like Japan, developing medical guidelines and policies that entirely disregard age would be challenging, and further debate is warranted (Norisue et al., 2021).
Upon establishing medical guidelines, patient/public involvement and engagement is strongly recommended by policy experts and ethicists, since citizens themselves would be impacted by the policies (White et al., 2019). In 2007, New York exemplified effective public engagement regarding ventilator allocation during their influenza pandemic preparedness planning, by posting a draft policy online for public review (Powell et al., 2008). Successful public engagement was also seen during organ transplantation policy development, where such engagement uncovered discrepancies between the public and policymakers’ attitudes, ultimately resulting in policies based on mutual consensus (Egan & Kotloff, 2005). However, in Japan, there’s much room for public discussion regarding triage criteria and withdrawal care-practice during pandemics (Norisue et al., 2021). As a first step to developing a sustainable medical system in preparation for future pandemics, there’s a pressing need for public awareness and discussion regarding triage and withdrawal care-practice during pandemics.
Limitations
Our study was limited to one ICU within a tertiary-care, urban hospital in Japan. Thus, the results may not be generalizable to other ICUs of different size/location/culture. Also, our study may not capture the entire triage process, since triage may have occurred even before patients were transferred to the ICU, which was beyond the scope of our research. Additionally, due to the limited number of hospital staff that we could recruit, especially physicians, data saturation was likely not achieved, despite efforts to maximize the respondent number. Furthermore, while we could not interview the senior management staff, we were able to receive valuable feedback from them during the drafting process. Notwithstanding those limitations, our study provided valuable insight into the actual ICU patient admission and treatment decisions and decision-making processes during the pandemic from both ICU physicians and nurses.
Supplemental Material
Supplemental Material - Patient Admission and Mechanical Ventilator Allocation Decision-Making Processes by Frontline Medical Professionals in a Japanese Intensive Care Unit During the COVID-19 Pandemic: A Qualitative Study
Supplemental Material for Patient Admission and Mechanical Ventilator Allocation Decision-Making Processes by Frontline Medical Professionals in a Japanese Intensive Care Unit During the COVID-19 Pandemic: A Qualitative Study by Sakura Ishizaki, Kazuaki Jindai, Hiroki Saito, Hitoshi Oshitani, and Tess Kulstad Gonzalez in Qualitative Health Research
Supplemental Material
Supplemental Material - Patient Admission and Mechanical Ventilator Allocation Decision-Making Processes by Frontline Medical Professionals in a Japanese Intensive Care Unit During the COVID-19 Pandemic: A Qualitative Study
Supplemental Material for Patient Admission and Mechanical Ventilator Allocation Decision-Making Processes by Frontline Medical Professionals in a Japanese Intensive Care Unit During the COVID-19 Pandemic: A Qualitative Study by Sakura Ishizaki, Kazuaki Jindai, Hiroki Saito, Hitoshi Oshitani, and Tess Kulstad Gonzalez in Qualitative Health Research
Footnotes
Acknowledgments
We appreciate all interview participants for their time and kindness for sharing their experiences and personal insights as frontline medical providers. We also thank stakeholders who provided feedback on our article. We appreciate Dr. Yumiko Oyama (Associate Professor, Yokohama City University, Japan) for providing advice to improve our interview questions/research methodology and Erin Todey (Multilingual Writing Specialist, Iowa State University, US) for her advice upon refining the article. A part of the study was presented at the 50th Annual Meeting of the Japanese Society of Intensive Care Medicine on March 4, 2023, and at the 83rd Annual Conference by the Society for Applied Anthropology on March 28, 2023.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Anthropology Department at Grinnell College and Japan Society for the Promotion of Science KAKENHI: Grant-in-Aid for Challenging Exploratory Research (grant # JP21K19624).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.