
Abstract
The COVID-19 pandemic has had a significant impact on medical practitioners’ professional identities due to its novelty and intensity. Using constructivist grounded theory, we investigated how the COVID-19 pandemic shifted individuals’ identities as medical practitioners in Indonesia, where the pandemic caused high death rates among healthcare workers, particularly medical practitioners. By interviewing 24 medical practitioners and analyzing relevant documents and reports, we developed a grounded theory of professional identity shifts. We found two patterns: (1) identity growth, in which the medical practitioners thrive and claimed stronger professional identities, and (2) psychological and moral distress leading to attrition, facilitated adaptation, or professional identity collapse. We also found several primary protective factors including religious beliefs, good leadership, team cohesion, healthy work boundaries, connection to significant others, and public acknowledgment. Without adequate protective factors, medical practitioners experienced difficulties redefining their professional identities. To cope with the situation, they focused on different identities, took some time off, or sought mental health support, resulting in facilitated adaptation. Others resorted to attrition or experienced professional identity collapse. Our findings suggest that medical practitioners’ experience of professional identity shifts can be improved by providing medical practitioners with opportunities for knowledge updates, better organizational leadership and work boundaries, strategies to enhance team cohesion, and other improvements to medical systems.
Keywords
Introduction
Medical practitioners in low-income countries like Indonesia faced significant challenges practicing during the pandemic, and yet we still know very little about how medical practitioners navigate changing practice environments in contexts where there are fewer social or economic resources. Furthermore, we know little about the impact of these practice challenges on the professional identities of medical personnel. In this paper, we report findings from a grounded theory study that seeks to broaden our understanding of how the COVID-19 pandemic shifted medical practitioners’ professional identities in Indonesia and identify factors that might help decision-makers improve medical practitioners’ identity and well-being.
Background
Professional identity is an individual’s self-conception of their profession and role in society, which is continuously shaped by workplace factors, beliefs, and values and regulated by professional bodies (Webb, 2017). Professional identities have distinctive role boundaries, specialties, privileges, and claims in society, which create distance from people outside the professional group (Webb, 2017).
Healthcare practitioners’ professional identities have been studied in medicine and nursing (e.g., Apker & Eggly, 2004; Johnson et al., 2012; Hoeve et al., 2014). The medical professional identity is constructed through medical education, socialization, and continuous role performances (Apker & Eggly, 2004; Cruess et al., 2015; Wald et al., 2015) and maintained through knowledge and skill enrichment (Apker & Eggly, 2004), re-definition of work responsibilities (Dadich et al., 2015), and adherence to professional values and ethics (Wald et al., 2015; Woo et al., 2014). Despite these strategies for identity continuity, challenges and discrepancies between defined roles and everyday experience can upset a person’s professional identity, causing identity reconstruction or loss (Charon, 2010; Dadich et al., 2015; Hendrikx, 2018).
Hopkins (2021) found the nature of the pandemic and the risks taken by medical practitioners enticed the public to perceive them as heroes. Similarly, early in the pandemic, the public regarded healthcare practitioners in countries like Spain as martyrs and heroes until they switched to remote consultation to limit risk exposures, triggering public displeasure (González et al., 2021). Meanwhile, reports from various countries, including Mexico, Malawi, Zimbabwe, and India, identified stigmatization by the public, who perceived medical practitioners as infection spreaders and exclude them from their communities despite their crucial roles during the pandemic (Bagcchi, 2020).
A medical practitioner’s professional identity is generally important and meaningful; therefore, professional identity shifts will significantly impact their mental health and psychological well-being (Shuval, 2000). Failing to perform obligations and societal expectations as medical practitioners during the pandemic caused distress and self-blame (González et al., 2021; Lesley, 2021). Furthermore, the lack of competency in performing professional responsibilities caused moral and psychological distress (Riedel et al., 2022).
The Context for the Study
In developing countries, including Indonesia, the pandemic worsened already vulnerable and constrained health systems (Ataguba & Ataguba, 2020; Ginanjar et al., 2020). Indonesia is experiencing prolonged shortages of general practitioners (GPs) and specialists, especially outside urban areas (Mahendradhata et al., 2017). Many medical practitioners, particularly GPs, are paid minimum wage or less (Haryawan et al., 2019; Nur, 2021). Medical residents have to accept unpaid placements in teaching hospitals, deterring many GPs who cannot afford training (Zainal-Muttaqin, 2020). The COVID-19 pandemic exacerbated these challenges by increasing practitioners’ workloads and revealing gaps in infrastructure and equipment for healthcare workers (Ginanjar et al., 2020; Sampe et al., 2021).
Method
To explain how medical practitioners in Indonesia adapt to pandemic-induced changes, we used constructivist grounded theory (CGT) (Charmaz, 2014). CGT is a research methodology well-suited to generating theory inductively and systematically when little is known about a phenomenon (Charmaz, 2014; Glaser & Strauss, 1967). Our study is also informed by the symbolic interactionist perspective (Charon, 2010) as we perceive that people think, act, and define meaning through interactions using language and symbols. Following Glaser and Strauss’ (1967) recommendation, we postponed our literature review on theories of professional identity until after our data collection and analysis.
Research Question
Like other CGT studies, we began with a general topic—Indonesian medical practitioners’ experience practicing during the pandemic—which we refined into a more specific research question as we collected and analyzed data. Specifically, “How did the COVID-19 pandemic in Indonesia affect medical practitioners’ professional identities?”
Interview Guide
Following Charmaz (2014), we developed an interview guide comprising open-ended questions to capture participants’ experiences. Applying our knowledge of the COVID-19 situation in Indonesia and the challenges faced by medical practitioners (the first Author was previously an Indonesian physician), we constructed questions to investigate participants’ experiences, challenges, resources, perceptions of the situation, and its effects on their lives. We routinely adjusted the interview guide based on the emerging findings.
Recruitment
To obtain broad insights from different settings and backgrounds, we recruited general practitioners (GPs), medical residents, and specialists, with diverse experience levels, in primary, secondary, and tertiary care settings, in both urban and rural areas. Recruiting lasted from August 2021 to December 2021 using advertisements in Indonesian medical practitioners’ social media forums and snowball sampling (participants referred others to the study).
Due to the extent of COVID-19 cases in Indonesia, most practitioners were involved with COVID-19 management in some way. Therefore, our eligibility criteria were simply medical practitioners in Indonesia, who were working/practicing during the pandemic. The screening for potential participants and the interviews were conducted remotely using end-to-end encrypted calls and adapted to the participants’ schedules.
Data Collection
We used in-depth, semi-structured interviews as our primary data collection technique, supported by document analysis. We interviewed 24 participants including 13 GPs (nine females and four males; two of whom are also hospital managers and one of whom is a hospital director), five medical residents (one female and four males; from ophthalmology, medical rehabilitation, surgery, and pediatrics), one general practitioner working with the district health office, and five specialists (four female and one male; one obstetric gynecologist, two pediatricians, one internal medicine specialist, and one radiation oncologist). Consent from all participants was obtained verbally. All interviews were conducted between September 2021 and January 2022. Interviews lasted between 45 and 90 min and were audio-recorded and transcribed verbatim by the first author. As a part of theoretical sampling and to follow up on the experiences of some practitioners, we did nine follow-up interviews, yielding 33 in total.
To ground and corroborate concepts emerging from interview data, we gathered government and non-governmental reports, government decrees, and organizational documents including two hospital employee COVID-19 screening pathways, the 2012 Medical Code of Ethics (PB IDI, 2012), Indonesian Laws (e.g., Law of the Republic of Indonesia Number 29 of 2004, on Medical Practices, 2009), Official Decrees (e.g., Decree of the Minister of Health on Medical License and Medical Practices, 2011), regulations (Indonesian Medical Council, 2012a, 2012b), official reports (Ginanjar et al., 2020; Mahendradhata et al., 2017, 2021), and news articles (Aditya, 2021; BBC News Indonesia, 2021; Zainal-Muttaqin, 2020). We coded relevant information and added it to the data we analyzed.
Data Analysis
Data for analysis included the interview transcripts and related documents. Coding was performed in Indonesian as the first author is a native speaker. Afterward, relevant quotations, concepts, and categories were translated into English by the first author. We wrote memos (in English) to guide us through the data analysis process by recording tentative ideas, gaps, and incomplete thoughts that needed to be pursued.
Open, line-by-line coding was performed following each interview. As a good CGT practice, we constantly compared statements and codes in the same interviews and from different participants (Charmaz, 2014). We began focused coding after nine interviews were coded and analyzed. A tentative model was constructed and used as the basis for theoretical sampling (Charmaz, 2014; Foley et al., 2021), which was used to obtain more data and saturate the grounded theory (Charmaz, 2014; Sinclair et al., 2018). That is, we updated the interview guide, interviewed more participants, and went back for follow-up interviews. We also did member checking with three willing participants to ensure our findings aligned with their experiences. We provided them with a two-paragraph summary of the findings and invited them to discuss their thoughts on the summary. The participants provided insights on the significant influence of socioeconomic status, financial burdens, work boundaries, and professional hierarchy on medical practitioners’ professional identity.
Rigor
To summarize, we ensured research rigor by embracing the core practices of constructivist grounded theory: delaying the literature review, collecting and analyzing data in interleaved rounds, theoretical sampling, line-by-line coding, constant comparison, memoing, continuing data collection until the emerging theory was saturated, and member checking. Moreover, when presenting our theory (below), we not only use direct quotations extensively to illustrate our findings but also re-integrate our findings with prior research.
Findings
Shifting professional identity emerged as our core category. A medical practitioner’s professional identity is formed through medical school, medical internships, and postgraduate training and reinforced by continuous knowledge updates, having an active medical license to practice, and memberships in one or more medical organizations. It emerges as a sense of competence to fulfill their societal roles as experts in medicine and health, and pride in holding their core values as medical practitioners: saving lives and social welfare. Interviewees showed a strong attachment to their professional identity as medical practitioners compared to other identities in their lives (e.g., student, manager, teacher, religious leader, spouse, child, and parent). Their professional identities as “doctors” are how they label themselves during social interactions; it is what they call themselves and what others call them.
Briefly, the situations and challenges of practicing during the pandemic, compounded by stigmatization as infection spreaders and government agents despite professionals’ contributions to their communities, led medical practitioners to lose their sense of professional competency (another in vivo theme we coded for during our data analysis). This triggered further losses of autonomy, public trust, social standing, and professional boundaries (deprofessionalization). Practitioners then followed one of two mutually exclusive pathways of professional identity shift (see Figure 1). Practitioners who had adequate protective factors and minimal secondary stressors tended to regain their knowledge and skills, leading to professional identity growth; that is, overcoming challenges strengthened their professional identity. In contrast, practitioners who experienced substantial secondary stressors and had limited primary protective factors tended to experience psychological and moral distress, and then either leave their job (attrition), cope by taking advantage of secondary protective factors (facilitated adaptation), or experience an enduring professional identity collapse. Pathways of professional identity shift.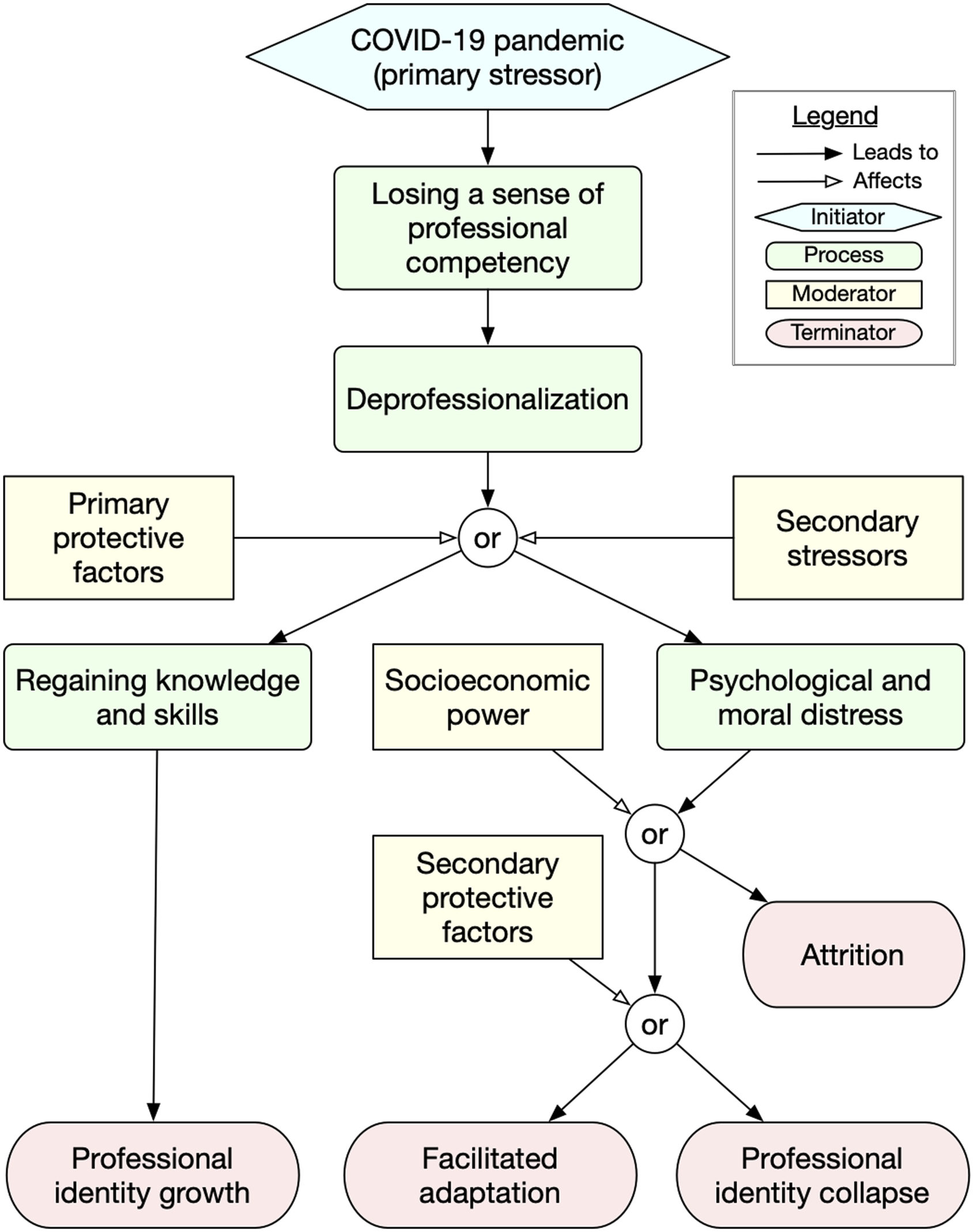
The two paths a medical practitioner can take constitute the main pattern that emerged from this study.
Shifts in Professional Identity
The COVID-19 pandemic created environmental challenges and shifted medical practitioners’ values, responsibilities, as well as society’s expectations of them. The novelty of the situation meant that participants had no previous knowledge or framework to treat their patients and no clear definition of work responsibilities or boundaries. The intensity of the pandemic and the constraints in the health system put constant pressure on the interviewees to work extra, sometimes outside their competencies. Participant-05 (General Practitioner, Male) described being overwhelmed working at the beginning of the pandemic: “I was overwhelmed, it’s like, we used to run 10 km/hour. Now we are pushed to run 150 km/hour. And we didn’t understand [what’s happening], didn’t know what to do….” Several other participants recounted being “stressed (P-04),” “scared (P-07),” “bewildered by constant changes (P-13),” and “confused (P-21).” Their struggle with the novelty, intensity, and limited knowledge of the situation upset their sense of professional competency.
Losing a Sense of Professional Competencies
With limited knowledge and experience, medical practitioners did not have adequate resources to perform their professional roles in society and thus experienced a decreasing sense of competence. Continuous changes in policies and treatment guidelines prevented them from sharpening particular competencies (e.g., in treating COVID-19 cases). They lost confidence in their ability to practice professionally, as recounted by Participant 4: There were no morning meetings at that time, which means no updates. We didn't know what to do, so when we [the residents] went in [to the COVID-19 isolation ward], especially the juniors, didn't know what instructions to give […] It is stressful, how the pandemic affected our services. (Participant-04, Pediatric Resident, Female)
This decrease in participants’ perceptions of their own competence made them feel they were underperforming, triggering deprofessionalization.
Deprofessionalization
Deprofessionalization arises from a practitioner’s inability to perform their roles competently as experts in medicine, having unclear expectations (e.g., constant policy changes), and performing additional responsibilities outside their competency. The feeling of deprofessionalization also led interviewees to reassess their identity as medical practitioners. To cope, interviewees redefined their positions in their workplace setting by comparing their situations and work environment to other medical practitioners and healthcare workers. They also compared responsibilities, resources, and privileges to other healthcare workers to rebuild professional boundaries that established their position as experts. For example, as a contract General Practitioner, Participant-01 (contract worker GP, Female) compared her work situation to an unskilled laborer: “Contract workers like us are forgotten… Like when helping C-section infants, I didn’t get standardized PPEs. I feel like an unskilled laborer.”
Other interviewees recounted feelings of deprofessionalization. However, as they worked in different settings, they faced distinct challenges and received diverse support. These differences led participants to experience one of two different outcomes: professional identity growth or professional identity collapse.
Pathway to Professional Identity Growth
Participants who followed the professional identity growth path found their professional identity not only restored but also enhanced. Interviewees experiencing professional identity growth overcame the feeling of incompetence and deprofessionalization. Their awareness of overcoming and thriving in this challenging situation reinforced their confidence and sense of competence as medical practitioners, leading to better definition of their roles and responsibilities and greater pride in their professions.
Regaining Knowledge and Skills
As scientists rapidly expanded their knowledge around COVID-19, medical practitioners in Indonesia continuously gathered information from various sources, for example, academic articles, government reports and recommendations, medical guidelines, and information updates from trusted colleagues. They also attended professional training (e.g., COVID-19 vaccine administration) to enhance and legitimize their skills in particular areas. As recounted by Participant-13: At morning meetings, we discuss new cases, talk them through, and debate the treatments. We got feedback and lots and lots of knowledge. We lost that at first [at the beginning of the pandemic], but now we are back to having the meetings via video conferences (Participant-13, Pediatrician, Female).
Professional Identity Growth
Medical practitioners who followed the professional identity growth path regained their sense of competence through training and knowledge updates. They rebuilt their status as experts by enhancing professional boundaries with other healthcare workers. They also decreased the knowledge gap between themselves and the public by performing as experts in their areas of expertise. They not only reconstructed their professional identities but also thrived in the face of these novel challenges, adding new competencies to those they held previously. Medical practitioners also exhibited stronger confidence in their performance and a sense of pride in their professions. Interviewees recounted these feelings as “growing into a better person” (P-21), “being able to provide better care” (P-15), “holding stronger values as physicians” (P-05), and “being a stronger doctor” (P-04). They exhibit better awareness of their professional responsibilities and boundaries. These positive outcomes were facilitated by several protective factors.
Primary Protective Factors
Interviewees described several factors that facilitated professional identity growth: religious beliefs, healthy boundaries, team collaborations, leadership, support from significant others, and acknowledgment. These factors protected against moral distress and helped medical practitioners regain and reinforce their professional identities.
Religious Beliefs
Many interviewees perceived their job as a religious calling, which provided them with strong core values and shifted the attribution of responsibility for both personal and professional outcomes to “God’s will.” As recounted by Participant-14 (Radiation-Oncology Specialist, Male), “Thanks to God’s grace, I’m always healthy even when practicing during the pandemic.” This view also helped participants cope when their current knowledge was insufficient to make meaning of the unknown and chaotic nature of the pandemic. Shifting the responsibilities to a higher being helped them cope with self-judgment and self-blame when they fail to save lives.
Healthy Boundaries
Maintaining boundaries between professional, social, and personal identities is crucial, as increasing work demands and professional responsibilities threatened to take over other aspects of participants’ lives. Maintaining boundaries also enhanced medical practitioners’ conception of their professional selves. At workplaces, well-defined work boundaries between medical practitioners and other healthcare practitioners were crucial for shaping the conception of professionals, with definite competencies, roles, responsibilities, and social status. Participant-02 (GP, Male) explained the importance of boundaries in this way: “The moment you step outside the hospital, your work is done...Working without limits will give you a headache and make you lose focus.”
Team Cohesion
A cohesive team fosters a sense of togetherness, which improved medical practitioners’ experiences practicing during the pandemic. Positive interactions reinforced medical practitioners’ social standing and their roles as professionals. For example, Participant-08 (GP, Female) realized her limitations as a medical practitioner and the benefits of working in teams: “We need everyone to be involved; we rely on allied health collaboration.”
Positive Leadership Styles
Medical practitioners working with organizations that support their professional development, consider their well-being, and see patient care as their core value reported better experiences and felt more empowered to perform their roles. Interviewees mentioned “full support from the department” (P-05), “management support in practicing” (P-15), and “good emotional support” (P-18). Organizational support (e.g., providing updates during morning meetings and arranging training sessions) was also necessary for medical practitioners to improve their skills and knowledge.
Connection to Significant Others
Shifting to different identities (e.g., parents, entrepreneurs, and children) provided interviewees with relief from the intensity of professional responsibilities. Moreover, positive interactions with significant others (e.g., spouses, parents, and close friends) outside the workplace gave interviewees different perspectives on themselves and their social standing, improving their self-worth. Significant others also help them cope with emotional distress, as recounted by Participant-13: “I talked to mom and dad; they always pray for me. My husband supported me, like ordering PPEs from overseas for me when the PPEs were scarce.”
Acknowledgment
Acknowledgment from society via formal government support (e.g., financial incentives) and informal support from the public (e.g., donations to hospitals or health centers and thank-you letters from the patients) reflected societal appreciation and approval of medical practitioners’ hard work during the pandemic. As recounted by Participant-21 (GP, Hospital Manager), “We got a lot of donations, not only PPEs and food but hand lotions and stuff! It’s so nice, you know.” This public appreciation enhances medical practitioners’ self-worth and confidence, cementing their identity as competent professionals.
Psychological and Moral Distress
While some interviewees successfully navigated the crisis and reforged their professional identities, others took less fortunate paths; they experienced psychological and moral distress leading to attrition or identity collapse. Interviewees who faced more secondary stressors without adequate primary protective factors experienced psychological distress due to difficulties in reconstructing their professional identity. Repeated or prolonged secondary exposures (e.g., problems at home and negative perceptions of doctors by the public at large) can lead to moral distress, leading to attrition or professional identity collapse. Some medical practitioners required facilitated adaptation to continue with their day-to-day work. Secondary protective factors facilitate their day-to-day adaptation and prevent identity collapse but do not deliver the same growth and self-worth as the primary protective factors.
Secondary Stressors
In Indonesia, COVID-19 patients and people with high-exposure risks are stigmatized as infection spreaders by the public (Saptarini et al., 2021). Some interviewees self-stigmatized and self-excluded from their significant others for fear of spreading the disease. Misinformation and fake news related to COVID-19 also turned public opinions on them (Saptarini et al., 2021). Interviewees also recounted how people deemed them as untrustworthy government agents or scammers trying to exploit the situation. Instead of being perceived as experts and appreciated for their hard work and sacrifices, they lost the public’s trust due to misinformation. And yet, they still felt responsible for educating and changing public perception, as recounted by Participant-07 (Internal Medicine Specialist, Female): [We] have to help with people who are exposed, have to tackle hoaxes too. It’s too much; it feels like we are ninja warriors; we have to do everything. But this [misinformation] was a mistake made by various players […] Like our medical community, we did not put the experts in COVID-19 as the spokesperson and ended up with blunders.
Practitioners reflected on their purposes, roles, and values as medical practitioners and the merits of their sacrifices. These reflections prompted them to reconsider their purposes and goals as medical practitioners. Stigmatization and conflicts, however, damaged the interviewees’ professional identity, causing psychological and moral distress.
Psychological and Moral Distress
Public distrust, lack of organizational and public support as frontline workers battling the pandemic, and deprofessionalization from having limited competencies to treat a novel disease engender psychological and moral distress in medical practitioners. Some interviewees experience self-judgment, guilt, remorse, emotional exhaustion, or shame, leading to anxiety, depression, compassion fatigue, and detachment. Participant-03 (Ophthalmology Resident, Female) described her conflicted feelings: “I got pandemic fatigue… Stressed, tired of the pandemic and the demand… But I am a healthcare worker, shame on me if I did not act like one.”
Interviewees who experienced psychological and moral distress lost their self-conception as medical practitioners and struggled not only to reconstruct their professional identities but also to maintain motivation to practice, thus losing the direction and purposes of their work—they became aimless. What happened next depended on practitioners’ socioeconomic power and exposure to two secondary protective factors.
Socioeconomic Power
Practitioners with socioeconomic power had the privilege to quit their current jobs or pursue residency or postgraduate programs. However, these options are privileges for practitioners who enjoy high socioeconomic status, are higher in the medical society hierarchy, or are not primary income earners—many Indonesian GPs and medical residents are poorly paid and have no such options (Nur, 2021).
Attrition
Being a medical practitioner is a prestigious position that is costly and takes years of effort; therefore, switching professions is not an option for most participants. However, participants with sufficient socioeconomic power did quit. For instance, Participant-11, a female General Practitioner, resigned from a public health center to enter a residency program: I resigned so I can go back to school. I have been working as a research assistant and I probably will look for a job as a public speaker or discussion moderator for the Medical Association if I can’t get into the program this year…. My sanity is more important.
Secondary Protective Factors
The fate of participants who stayed despite their psychological and moral distress depended on two secondary protective factors: mental health support and time off.
Mental Health Support
Mental health support (e.g., counseling and psychotherapy) helped interviewees in coping with their distress by supporting them as they identified new personal and professional goals. However, in Indonesia, mental health issues are not deemed crucial and accessing mental health support is disdained, even among medical practitioners. Moreover, few mental health services were known by the interviewees. As experts in medicine and health, they felt compelled to manage their issues themselves. As explained by Participant-22 (Pediatrician, Female): “I’d love to use the hotline… But if we use the hotline, it will be full. Better to give it to people that need it more.” Many interviewees only accepted support when provided by their organizations as part of their organizational policies and not those also meant for their patients. Others, however, were open to accepting any mental health services that were available. For example, Participant-03, an ophthalmology resident, recounted her experience attending mental health sessions from the psychiatric department: “It was pretty enlightening […] So, whenever I feel off, I will seek help, get counselling.”
Taking Time Off
Taking time off helped medical practitioners shift their focus and activities to themselves and explore other identities. Participant-16 explained: “I needed that three days off to sleep and go to the mall… That was so good.” During their time off, participants engaged in different activities which provide them with new perspectives and opportunities to reflect on their situations.
Exposure to these secondary protective factors facilitated practitioners’ day-to-day adaptation to the significant challenges they faced. In contrast, the absence of any secondary protective factors leads to enduring professional identity collapse.
Facilitated Adaptation
Taking enough time off or receiving mental health support facilitated interviewees’ adaptation to the psychological and moral distress they experienced. Participant-03, an ophthalmologist resident, recounted her experience attending mental health sessions from the psychiatric department: “it was pretty enlightening […] So, whenever I feel off, I will seek help, get counseling.” However, despite these efforts, they still did not exhibit the same self-worth and identity growth as those with strong primary protective factors and limited secondary exposures.
Professional Identity Collapse
Without socioeconomic power or secondary protective factors, interviewees have limited options but to stay in their positions with no clear direction, self-conception, or purpose. They chose to focus on their other identities (e.g., as entrepreneurs, parents, spouses, or religious leaders). Others exhibited detachment, decreasing professionalism, compassion fatigue, and lower regard for their identity as medical practitioners. As shared by Participant-02 (General Practitioner, Male), “I can’t even feel the stress anymore […] I’m stuck, not that I don’t want to move on. I have a family and my little ones are going to school. They are expensive.”
Discussion
The grounded theory presented in Figure 1 extends findings from previous studies by illustrating how significant stressors cause the reconstruction of medical practitioners’ professional identities. Our identity is the facade we maintain through social interactions (Monrouxe, 2010). Medical professional identity is formed through socialization and opportunities to perform professional roles and live up to the professional values (Cullum et al., 2020). Losing a sense of competency, increasing workload, and societal pressures during the pandemic caused significant stress to medical practitioners (Riedel et al., 2022).
We found that the COVID-19 pandemic shifted medical practitioners’ professional identities. As other research has shown, when experts lose their sense of competency, it triggers self-judgment and identity re-assessment (Pratt et al., 2006). Shapiro (2021) reported a similar finding among US medical residents who worked outside their competencies during the pandemic. Working outside professional competencies creates confusion regarding roles and boundaries, especially in semi-voluntary medical placements, which affects professional identity growth (Shapiro, 2021). Splichal (2020) defines the situation in which a professional loses conceptualization of their profession, autonomy, advantages and standing, and professional boundaries as deprofessionalization. Meanwhile, engaging in activities that increase professional and personal growth, application of one’s values and ethics, socializing in professional settings, and the ability to perform professional roles enhances professional identities (Öhlén & Segesten, 1998).
We theorize that crises trigger a mismatch between medical practitioners’ expected roles and the realities of practice in a stressful environment. Medical practitioners’ professional identities are constructed and reconstructed when there is a mismatch between role demands and current performance, triggering re-definition of a new identity through customization (e.g., through further training) or social validation which strengthens a previously held professional identity (Pratt et al., 2006). Pratt et al. (2006) studied the construction and reconstruction of professional identities of medical residents in the US without significant external stressors, while our grounded theory is based on the experience of Indonesian physicians facing an extremely stressful and under-resourced environment. We also extend Pratt’s theory with two different consequences of professional identity shifts (e.g., growth vs. facilitated adaptation or professional identity collapse) and several factors that have significant influences on the processes. As shown by our data, the pandemic was a primary stressor which triggered several secondary stressors (e.g., stigmatization and losing the public’s trust due to misinformation) and protective factors which influenced professional identity shifts. As a result, our constructivist grounded theory offers broader insights into medical practitioners’ professional identity maintenance and adaptation when faced with significant challenges.
Secondary stressors affected the pathway of medical practitioners’ identity shifts by eroding their roles as experts in society and excluding them from social interactions, worsening the feeling of deprofessionalization, and causing psychological disturbances. Losing the public’s trust and the decline in the profession’s prestige eliminate the gap between the professionals and the public, weakening the profession’s status and power in society (Splichal, 2020). Furthermore, failing to uphold their professional responsibilities to the public triggered ethical and moral dilemmas in healthcare practitioners (Wolf & Zuzelo, 2006). Kröger (2020) proposed various scenarios showing how high emotional strain against medical values and social exclusion triggers moral injuries (conflicts that are caused by performing actions that are not aligned with a person’s moral values) in healthcare practitioners while losing professional expertise shatters one’s professional identity. These two separate processes added to the medical practitioners’ daily traumatic experiences, contributing to various psychological disorders (Kröger, 2020). Williams et al. (2020) and Masiero et al. (2020) found similar stressors experienced constantly can turn into traumatic experiences leading to moral injuries in healthcare practitioners and other communities in the US, UK, and Italy. Psychological distress, along with a lack of recognition and bad leadership, led to attrition within healthcare during the pandemic (Simard & Parent-Lamarche, 2022; Tabur et al., 2022). Influenced by the socioeconomic environment in Indonesia, our study found that socioeconomic status and family needs impact medical practitioners’ ability to quit.
Fortunately, we identified several protective factors necessary for this process of professional identity reconstruction and growth, including religious beliefs, healthy work boundaries, team cohesion, good leadership, social connection outside the workplace, and acknowledgment. Creating supportive work environments and including medical practitioners’ well-being as a core value of medical professionalism (i.e., patient care, welfare, autonomy, and social justice) is crucial to prevent psychological distress and increase medical practitioners’ care quality (Goddard & Patel, 2021; Von Arx et al., 2018). Supportive leadership, too, proved to be one of the most important coping resources to reaffirm professional identity and prevent attrition (Von Arx et al., 2018). Organizations, for example, need to provide practitioners with adequate resources and an opportunity to take time off to grieve without any professional judgment (Funk et al., 2017). We also found that religion plays an important role by providing medical practitioners with motivation and a reason to practice. This finding is similar to Findyartini et al. (2020) who analyzed how medical students construct their values and ethics and prevent burnout, using their religious beliefs.
Furthermore, positive interactions inside and outside the workplace provide medical practitioners with opportunities to perform their professional roles. These interactions enhance a sense of togetherness, confidence, and self-worth, strengthening one’s professional identity. Positive role performances and in-group and out-group interactions affirm one’s social position, which enhances professional identity, while the opposite implies social rejection or faulty roles (Monrouxe, 2010). Day et al. (2020) found that acknowledgment and gratitude from patients intensify social ties, enhance practitioners’ quality of life, and reduce psychological disturbances.
As deprofessionalization can cause psychological and moral disturbances, another protective factor necessary to prevent psychological distress and enhance moral resilience during the pandemic was access to mental health support (Dean et al., 2020; Litam & Balkin, 2021; Williams et al., 2020). Litam and Balkin (2021) suggest dedicated mental health services for healthcare practitioners be made available outside of traditional work hours. Health organizations need to create dedicated mental health policies and programs for healthcare practitioners to ensure practitioners utilize mental health services (Dean et al., 2020). This aligns with our findings that medical practitioners hesitate to seek mental health support unless it is dedicated support provided by their organizations.
Another strategy to limit moral distress in healthcare practitioners during periods of extreme stress like a pandemic is to give them time and space to decompress through scheduled periods of leave (Roycroft et al., 2020). However, we found that mental health support and leaves of absence only help practitioners adapt to their work situations and do not foster the same self-esteem, life satisfaction, and identity growth as primary protective factors: religious beliefs, healthy boundaries, team cohesion, positive leadership styles, connection to significant others, and acknowledgment.
Recommendations
Better preparedness for future crises is needed. Based on our findings, we proposed the following recommendations.
Enrich professional competencies: (1) Send weekly knowledge updates (e.g., during morning meetings or via the organizations’ communication networks) that are focused, concise, and free of propaganda and (2) provide medical practitioners with opportunities to do short courses or training to enhance their skills and ensure they have sufficient time off to get the training.
Improve team cohesion: (1) Conduct team training to enhance a sense of togetherness and build a better definition of each member’s responsibilities and (2) ensure equity in financial incentives.
Optimize organizational support: (1) Provide all medical practitioners with standardized PPE and other instrumental supports relevant to the crisis situations they encounter; (2) create efficient patient admission and referral pathways; (3) allow non-medical practitioners to complete administrative work; and (4) provide dedicated mental health support for healthcare practitioners that allows them to have shorter sessions and sessions outside traditional work hours.
Limitations and Future Work
A CGT study should be evaluated using four criteria: credibility, resonance, originality, and usefulness (Charmaz, 2014). To demonstrate credibility, we thoroughly described our data collection and analysis and supported each concept in the proposed theory by direct quotations from participants representing various backgrounds, years of experience, and workplace settings. To assess and improve resonance, we cross-referenced the participants’ statements against our data from document analysis and compared and verified our ideas with the participants using member checking. To illustrate usefulness, we provided practical recommendations for decision-makers. Furthermore, our work is an original contributions in at least three ways: (1) we extend Pratt’s theory of professional identity with two different consequences of professional identity shifts (e.g., growth vs. facilitated adaptation) and have added several factors that influence these shifts; (2) we make several novel recommendations; and (3) we provide the first in-depth study of professional identity in the context of Indonesian medical practitioners.
As a qualitative study that focuses on a particular context, our work does not, however, support statistical generalization. Based on our limited understanding of differences across cultures and medical systems, protective factors and stressors may differ by context. This study was done in Indonesia, a country that emphasizes social cohesion (Jones, 2007; Mangundjaya, 2013) and strong religious influences (Ropi, 2017) despite social hierarchy. The context (i.e., the COVID-19 pandemic) was also specific, with distinct impacts on participants. Furthermore, our findings are based on the experience of a limited number of medical practitioners. Therefore, the proposed grounded theory needs broader validation, for example, by re-assessing it in different countries and with different professions.
Conclusion
This study has shown that the pandemic triggered a loss in medical practitioners’ sense of competence, and their public status and credibility. This deprofessionalization drove our participants down one of two paths: a more constructive path to growth in their professional identity or a path toward psychological and moral distress. We also found several factors—religious beliefs, healthy boundaries, team cohesion, positive leadership styles, connection to significant others, and acknowledgment—that help protect practitioners’ professional identity; two secondary stressors—misinformation and stigmatization—that worsen professional identity shifts; two secondary factors—mental health support and time off—that help practitioners adapt to damage to their professional identities; and that socioeconomic power allows attrition.
In summary, we advance a grounded theory of how medical practitioners adapt or reinforce their professional identities after experiencing deprofessionalization from external stressors. The proposed theory contributes to the body of knowledge around professional identity by showing the process of identity shifts after significant stressors.
Footnotes
Acknowledgment
We’d like to thank Dr. Paul Ralph for the technical input and general support in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study is approved by Dalhousie University Social Science and Humanities Research Ethics Board (REB # 2021-5523) and by the Health Research Ethics Committee of the Faculty of Medicine Syarif Hidayatullah State Islamic University Jakarta (Protocol No. 3674022P144202108160003) in Indonesia.