
Abstract
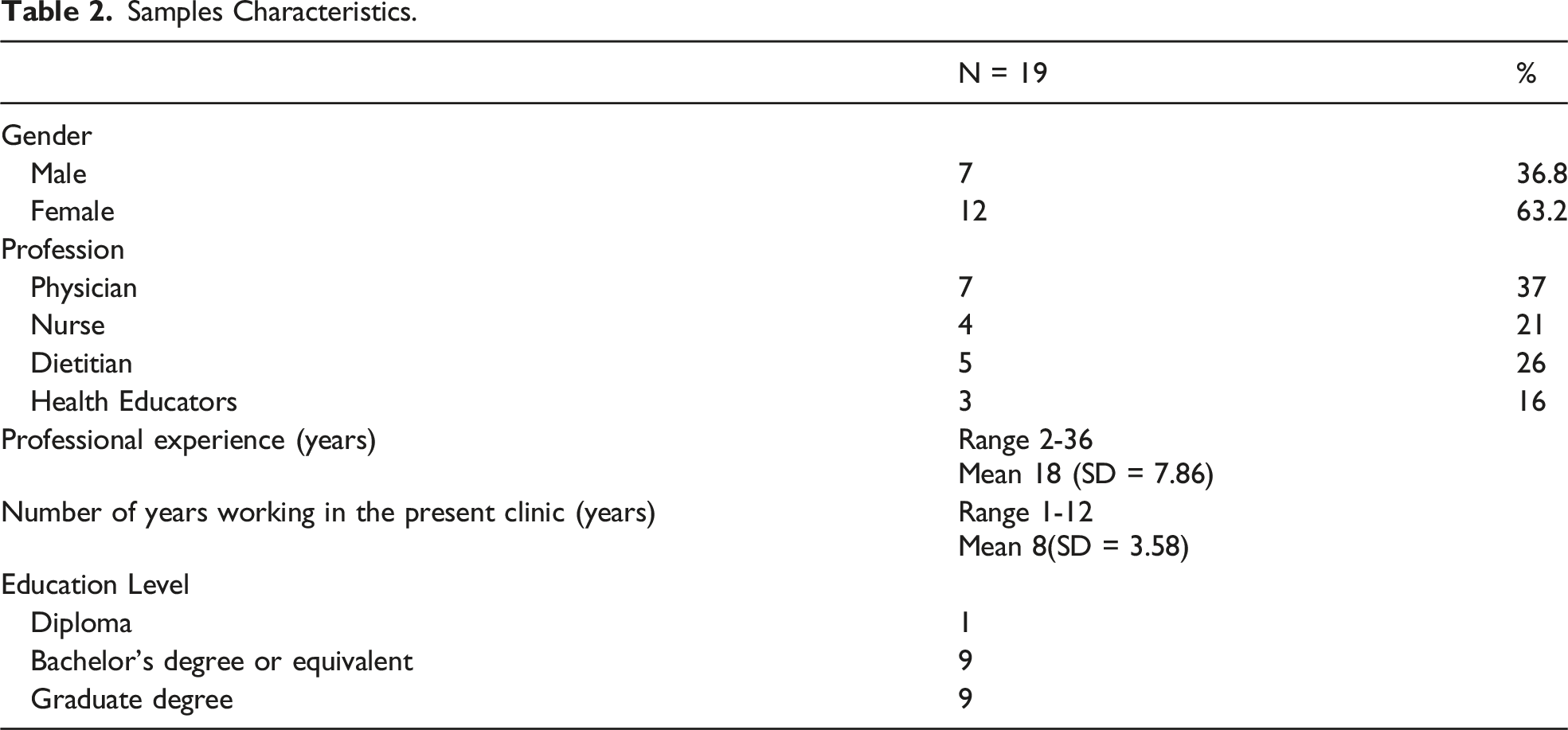
Nigeria struggles to reframe its traditional acute-care disease approach to health care to accommodate rising needs for chronic disease care. This interpretive descriptive study explored Nigerian healthcare providers’ (HCPs) perspectives, experiences, and practices related to self-management support (SMS). Observational and experiential data were gathered from 19 HCPs at two urban hospitals in Southeastern Nigeria (seven physicians, four nurses, five dietitians/nutritionists, and three health educators). There were four themes: (a) compliance-oriented medical model, (b) SMS as advice, informal counseling, and education, (c) navigating the sociocultural terrain, and (d) workarounds. Nigerian HCPs perspectives and SMS practices were characterized by attempts to foster compliance with healthcare instructions within a traditional biomedical model. Participants enhanced patient support using specific strategies to bypass structural system obstacles. These findings demonstrate the need to reevaluate the current understanding of SMS in Nigeria and its practice.
Introduction
Self-management support (SMS) is a prerequisite for effective diabetes self-management (Beck et al., 2019). While there is no cure for type 2 diabetes mellitus (T2DM), it can be managed through various lifestyle measures, including carbohydrate-limited diets, increased physical activity, blood glucose self-monitoring, and medications. Implementation depends on the patient’s diabetes knowledge, attitudes, skills, and capacity for self-care behavior. In this regard, self-management is the foundation of diabetes management (Diabetes Canada Clinical Practice Guidelines Expert Committee et al., 2018; Schulman-Green et al., 2012). SMS refers to the diverse support HCPs provide to help individuals with chronic diseases manage their condition. Diabetes SMS has been associated with significant health benefits among individuals living with diabetes in various settings (Van Hecke et al., 2017; Sheridan et al., 2017), specifically including positive outcomes such as increased knowledge of the health condition and its management, reduced HbA1C, higher patient-reported quality of life, better self-efficacy, and behavioral improvement (Attridge et al., 2014).
Despite the pivotal role of SMS in diabetes care, little is known about SMS practices in Nigeria. Meanwhile, Nigerians living with T2DM tend to have insufficient knowledge about diabetes, poor self-management, and increased morbidity/mortality (Osuji et al., 2019; Stephani et al., 2018). For example, up to two-thirds of individuals with diabetes in Nigeria have uncontrolled blood glucose (Attoye et al.,2020; Oluma et al., 2021), and there are high rates of stroke, limb amputations, blindness, and premature death (Adeloye et al., 2017; Ojobi et al., 2016). As for patient-related factors, these complications and deaths have been attributed to low education levels, poor health literacy, diverse cultural beliefs, poverty, inadequate knowledge of diabetes, and poor self-management (Bosun-Arije et al., 2019). Nonetheless, there is a paucity of evidence on the initial and continued professional SMS practices offered to people in Nigeria and several African countries. Therefore, this study aimed to explore HCPs’ perspectives, experiences, and practices of SMS in Nigeria by focusing on two outpatient diabetes clinics in Southeastern Nigeria.
Background
PRISMS Components of SMS.
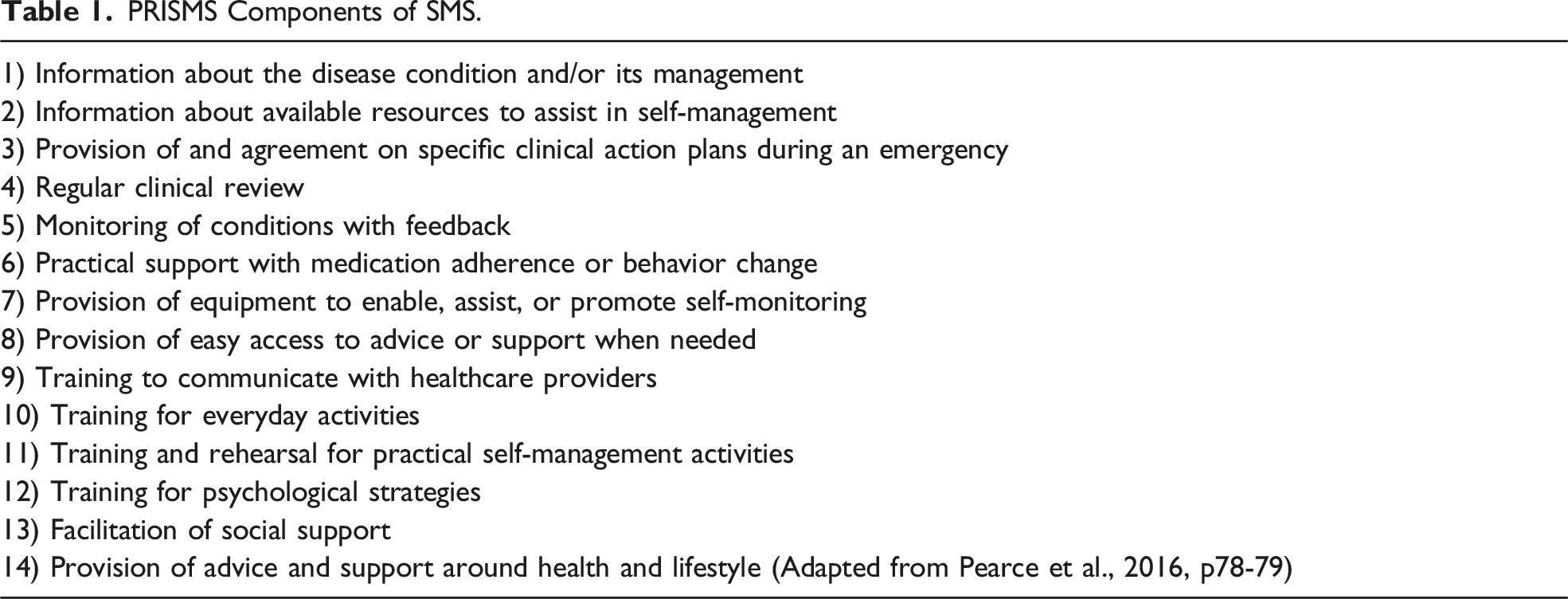
HCP support is pivotal for diabetes patients (Chrvala et al., 2016; Sheridan et al., 2017). It prepares and equips patients with knowledge and skills to navigate the clinical, educational, and psychosocial needs associated with living with diabetes (Powers et al., 2020). Unfortunately, there is a considerable gap in diabetes care knowledge and practice among HCPs in Southeastern Nigeria (Ugwu et al., 2020). HCPs are more likely to provide SMS if they understand what it entails and have the requisite expertise. It also depends on their predispositions toward and beliefs about the usefulness/feasibility of SMS interventions and their ability to provide relevant support (Alvarez et al., 2016; Schulman-Green et al., 2016). However, few studies have explored the worldviews, knowledge, and SMS practices of HCPs who care for persons with T2DM patients in Nigeria. Kumah et al. (2021) conducted a scoping review of diabetes self-management education (DSME) interventions in the WHO African region and documented the presence of few individualized, group-based, and technologically based DSMEs in Africa. Only two of those studies were conducted in Nigeria (Afemikhe & Chipps, 2015; Essien et al., 2017). Essien et al. (2017) and others (Fasanmade & Dagogo-Jack, 2015; Nwankwo et al., 2015) described diabetes education in many Nigerian hospitals as a random and unstructured provision of didactic information, often in public waiting areas during follow-up visits. The content, processes, and structures of such education remain unclear. Moreover, T2DM patients who do not receive support from HCPs may fail to manage or perpetuate poor self-management due to insufficient knowledge, skills, and confidence. As such, this interpretive descriptive study addressed the following research questions: Q1: What perspectives (experience, knowledge, values, and beliefs) do Nigerian HCPs hold toward diabetes SMS? Q2: How do these perspectives inform the practices of Nigerian HCPs? Q3: How do Nigerian HCPs support or facilitate self-management for T2DM patients?
Methods
The study design was interpretive description (ID), a qualitative research approach developed by Sally Thorne, primarily for nursing and other practice disciplines (Thorne et al., 1997; Thorne, 2016). Its primary focus is to explore complex experiential human problems while adhering to the disciplinary logic of the profession where the findings will be applied. Hence, ID employs flexibility in the use of design strategies.
Epistemologically, ID assumes that truth is subjective and that knowledge is co-constructed between a researcher and participants (Thorne, 2016; Thorne et al., 2004). Hence, researchers using ID must interact with study participants to access the multiple versions of reality while also acknowledging and situating the experiences within the context (Thorne, 2016). We used ID to explore diabetes SMS as practiced and articulated in the accounts of Nigerian HCPs providing care to persons with type 2 diabetes in 2 diabetes clinics in Southeastern Nigeria.
Setting and Sample
Hospital 1 and Hospital 2 were in a major city and an urban periphery, respectively. Both were government-owned and provided outpatient diabetes care. These sites were selected based on the scope of service and the availability of different HCPs in their diabetes clinics. Both hospitals were also referral centers for nearby hospitals. The study protocol was reviewed and approved by the Academic Research Ethical Review Board (PRO Pro00081155) and ethics committees/administrations at each hospital. All staff members were aware of the researcher’s presence and purpose. Written consent was obtained from all participating HCPs, while verbal consent was obtained from patients and family members. The PI was a registered nurse in Nigeria. Other team members included qualitative researchers in diabetes and a researcher experienced in ID. The conceptual approach was to identify participants’ emic SMS perspectives based on constructivist assumptions.
Samples Characteristics.
Data Generation
The data sources included (a) interviews, (b) participant observations, and (c) document reviews. There were formal and informal interviews, both face-to-face and telephonic. The formal interviews were semi-structured via interview guide and audio-recorded (23 total interviews with 19 participants). Informal conversations were brief and generally pertained to observations in the clinic; field notes were handwritten as soon as possible. Concurrent data generation and analysis allowed the interview protocol to evolve contemporaneously. Data generation was concluded after obtaining sufficient in-depth data to answer the research questions (Thorne, 2016). All participants spoke in English. The primary researcher is a native speaker of the Igbo language and took notes in cases where patients used Igbo.
Participant Observations
One hundred and twenty hours of participant observations were conducted at Hospital 1 and 58 hours at Hospital 2. The PI followed one HCP or patient through various consultations. No data were retrieved via medical records. Instead, patients were engaged in informal conversations to inquire about their understanding and feelings about present care.
Document Review
During observations, it was noted that two key patient education documents were used for SMS: a two-page diabetes overview pamphlet and a diabetes diet guide. These documents were examined for content, depth of information, and the Flesch reading ease index.
Data Analysis
Data generated from interviews, participant observation, and clinic SMS document review were analyzed in a complementary manner. Clinic SMS documents were examined to extract information about the self-management education content and the Flesch reading ease index.
Data generation occurred concurrently with data analysis, with emerging findings guiding further data generation and new data informing the analytic process. Data were managed in Quirkos© (Quirkos, Version 2.3.1). Consistent with the ID approach, data analysis was inductive (Thorne, 2016). Initially, the primary researcher immersed herself in the data by reading and re-reading the transcripts and field notes to develop an in-depth global understanding. Then, she used descriptive coding to assign titles to phrases, sentences, or paragraphs to capture particular meanings. Similar codes were grouped into categories. We used strategies from the constant comparative approach (Glaser, 1965), including open coding and in vivo coding, to compare similarities and differences within and across cases. The second analysis phase involved determining the relationship between the different categories, including their properties and context. This phase also involved an iterative reasoning process between the field and data; developing ideas or patterns were clarified, explored further, or challenged by analyzing existing and new data while allowing minor adjustments in the probing questions. The first author led the data analysis, and regular team discussions provided debriefing and opportunities to consider alternative interpretations. Descriptive and interpretive analysis discussions continued until consensus was achieved among the team. The last phase of the interpretive analysis involved experimenting and aligning the categories in various ways to develop the most feasible explanation (Thorne, 2016). We utilized both processes of immersion in data and distancing ourselves from the data to consider the different possibilities the data presented (Thorne, 2016). The resulting categories and their relationships were combined to form a narrative that became the study findings.
Trustworthiness:
The PI used reflexive journals and memos to record contexts across various stages of the study, including the decisions made and the rationale behind those decisions. As a result, the interpretation of data went through a check and balance process (Morse et al., 2002). Using different data sources such as interviews, field notes, document reviews, and reflexive journals also helped to ensure that the data upon which findings were based existed beyond a single angle of vision or perspective; thus, strengthening the trustworthiness of the analysis (Thorne, 2016).
Results
Four central themes describe the perspectives, experiences, and practices of Nigerian HCPs: (a) compliance-oriented medical model approach, (b) SMS as advice, informal counseling, and education, (c) navigating the sociocultural terrain, and (c) workarounds.
Theme 1: Compliance-Oriented Medical Model Approach
The compliance-oriented medical model approach was perceived to ensure that patients complied with medical instructions. Subthemes included (a) prioritizing standard blood glucose, (b) focusing on compliance, and (c) HCPs as experts.
A. Prioritizing Normal Blood Glucose Levels and Other Physiological Values
All participants perceived that SMS aimed to reduce blood glucose levels and prevent complications. They based their support on each patient’s biomedical results. For example, only patients with abnormal test results received brief lectures on diabetes management during follow-ups. By contrast, HCPs assumed that patients with normal blood glucose managed well and did not require self-management education. They rarely explored how their patients felt about diabetes and most often redirected conversations toward symptoms and the need to take prescribed medications, as in the following field note excerpt: The patient was a woman in her late 50s with visual impairment in one eye, which she continually wiped with a handkerchief due to emerging tears. She sat down and said: Patient: “My husband’s brother’s wife told me four years ago, while quarreling, that I will go blind. Now I am having problems with my eye.” Doctor: “Which drugs are you on? Any fever?” Patient: “No, but I have headaches. They say it is ‘Okiri-mgbawa-isi” [an Igbo name for a severe headache supposedly inflicted on one by evil people or power]. Doctor: “Your BP is very high, 190/100 mmHg; when last did you take your antihypertensive?” Patient: “Last two Weeks.” Frowning, the doctor faced the patient and said, “Go and see what is happening in the casualty [Emergency unit]; that is where people that do not take care of themselves end. Then, that money you do not want to spend will come out by force… stroke does not know that you have an eye problem. Your blood sugar and blood pressure are high; this combination comes with stroke.” (Hospital 1 field note) The HCP barely acknowledged the patient’s viewpoint, instead focusing on symptoms and medical treatments over “unimportant” matters such as health beliefs. There was no structure for providing self-management education (SME) to patients with T2DM, either periodically or incrementally. Instead, provisions were reserved for cases of abnormal laboratory results. The focus on biomedical parameters and compliance was dominant across HCP-patient interactions.
“Our goal is to make the diagnosis, confirm the diagnosis, then harness a management plan for the person. When you start the management plan, monitor the patient by giving an appointment. The patient’s role is to adhere to the instructions.” (Endocrinologist)
HCP–patient conversations were not interactive but entailed a one-way informational flow from HCPs. Patients were expected to accept this and strictly adhere to medical instructions: they should be ready and willing to follow orders from HCPs, who were to be fully trusted: “It becomes a challenge when patients do not do what they are supposed to do, [or] not do what they are told to do. We are not happy because we are not achieving our aim. The solution is that, if a patient is coming to the hospital, let the patient make up their mind that anything he is told in the hospital to do, he should do it.” (Resident doctor)
Patients who refused to follow instructions or asked too many questions were described as “difficult,” especially those with differing opinions or who offered personal anecdotes: “Our challenge here is that sometimes they will not agree with you. When you say what they should do, they will say, ‘no, I cannot do this.’ That is our challenge here, a diabetic patient that is so difficult to handle will be asking questions and questions; some will start telling you stories, [and] time will go [to waste].” (Dietitian)
Education was not considered an interactive process at either clinic, where participants interchangeably used the terms “compliance” and “adherence,” connoting obedience.
“We have a guide, a written guide given to them (patients) individually, which contains the individual measurements and quantities of food. In the guide, you will see the dos and don’ts, the foods to eat, and what not to eat.” (Dietitian, Hospital 1)
Dietitians believed patients required diet guides that listed different food items and quantities for each meal. Neither clinic provided practical meal planning tools that would give patients tolerable flexibility in their dietary choices. The dietitians considered it unnecessary to provide diabetic food exchange lists because they were too complicated for poorly educated patients. Instead, they believed they should solve these problems directly, not the patients or their families. Dietitians enforce compliance with strict dietary plans that some patients perceive impossible to follow. Patients questioned the diet guide due to the small portion sizes stipulated, with little or no room for maneuver. I observed patients struggle to accept restrictive diet guides at both clinics, as manifested through facial expressions or remarks such as “O gakwa ekwe omume?” [Is what you are asking me to do possible?]. Some would outright refuse: “I saw the dietitian only once. She showed me how to measure what I would be eating, but what she showed me was too small. I would die of hunger if I went by that, so I manage my diet on my own.” (Field note)
Participants assumed their superior knowledge rather than acknowledging patients as experts on their bodies or circumstances, nor did they believe them capable of informed choices. Thus, SMS experiences and practices were shaped by compliance perspectives. The themes below reflect strategies that HCPs used to support patient self-management.
Theme 2: SMS as Advice, Informal Counseling, and Health Education
While there were various opinions on SMS, many HCPs fundamentally viewed it as provision of information, assuming that any such knowledge (the basis for effective management) would automatically translate into self-management behaviors. The nurses, dietitians, and health educators adopted broader views, perceiving SMS as education, informal/spiritual counseling, and advice. By contrast, the physicians focused on education and instruction, providing medical information about the signs and symptoms of diabetes, complications, and modes of treatment. Participants referred to their opinions as “advice” (e.g., encouraging patients to comply). They described their activities as counseling when helping patients accept or come to terms with diabetes. The primary message was that diabetes was not a death sentence but could be managed for many years if instructions were followed. One dietitian described how they provided counseling and the conditions under which patients were counseled at the clinic: “Some of them will be very sad as if they are dying today or tomorrow. Then we start counseling them; we tell them this is not the end of the world. Some people have been with the disease for 30 years… It is when you are not under control that you face problems; we start telling them that they will live a long life, just for them to know that diabetes is not dangerous like other diseases.” (Dietitian) Most counseling was provided early after diagnosis, as noted below: “When I was newly diagnosed, I nearly died. I was depressed, but the doctor helped me by counseling me and telling me that diabetes is not a death sentence and that once I keep to my drugs and diet, I will be fine. I benefitted from the doctor’s counseling and the dietitian’s counseling.” (Field note, Hospital 2)
HCPs believed that instilling hope helped patients accept their condition. They thought patients needed to accept their condition due to the cultural beliefs associated with chronic illness. Here, their primary strategies were reassurances and repeated assertions that diabetes was not invariably fatal and could be managed well. Participants believe that SMS’s counseling, advice, and education are essential components. “SMS is education, nah [certainly]. Adequate health education, then, whatever you tell the patients, the patients should try to carry out those things. So, the doctor’s primary role is to give instructions and educate the patients.” (Endocrinologist)
Two forms of health education were practiced at Hospital 1: a) general health talks for all patients and relatives the morning before clinic consultations and b) individualized talks during HCP–patient consultations. General health talks did not occur in Hospital 2.
General Education
At Hospital 1, health educators (individuals with general health science degrees employed to reduce health illiteracy among patients) gave daily general health lectures to all persons in the clinic waiting room. However, during the eight-week observation period, no diabetes topics were addressed: “What we usually do is talk to them generally. We do not pay attention to a particular group of patients and their condition, like those with diabetes… it is usually a summary; we have to be brief.” (Health educator)
Health talks occurred while nurses called patients to obtain their vital signs. The clinic was usually busy and noisy. It was difficult to hear the health educator, and no audiovisual aids were employed.
Individualized Education
Patients sometimes received one-on-one diabetes education from different HCPs. The scope and extent depended on the HCP, available time, and specific laboratory results. Sessions typically lasted about 10 minutes for nurses and physicians and about 30 minutes for dietitians. Physicians mainly educated patients on the first visit after initial diagnosis and in cases of abnormal laboratory values. They focused on basic diabetes facts (causes, complications, medical instruction adherence, and follow-ups). The HCP decided on an education topic unless the patient had a specific question. Upon first contact, the education aimed to provide patients with an overview of diabetes. The following exchange involving a young man chronicled an individualized education session following a T2DM diagnosis: The doctor asked, “do you know about diabetes?” The patient replied, “I have been hearing about it.” The doctor then briefly explained diabetes, its causes, possible complications, and the need for adequate glucose control. He instructed that the fasting blood sugar should not exceed 110mg/dl [6 mmol/L], while RBS should not exceed 160mg/dl [8.8 mmol/L]. He continued, “There is a test you do from time to time every three months, HbA1c, that will give us an idea of your glycemic control. We encourage you to get a glucometer. We will start you on oral medications first; if there is inadequate control, we will put you on insulin.” This talk lasted approximately 10 minutes. After the patient left, I asked the doctor if the patient would receive any other form of education on diabetes self-management, as he was newly diagnosed. He replied, “Some health educators come here in the morning to give education, but we do not really have diabetes educators, so we just do [what] we can.” (Field note)
Education sessions for patients with new diagnoses typically lasted about 10 minutes. In follow-ups, additional provisions of diabetes education were dependent on specific FBS/RBS results and the number of waiting patients. For example, patients may not receive more education if their blood sugar levels are normal or if the clinic is busy, which is typical. Patient education invariably consisted of basic biomedical information about diabetes and instructions on maintaining normal blood glucose levels, delivered via quick-paced lectures. HCPs did not usually request verbal feedback from patients. The explanations were minimal or entirely omitted when other patients were waiting or near closing, even if patients did not understand their condition or its management.
All diabetes education was provided verbally, typically without visual aids or models. Hospital 1 did provide a two-page diabetes tip pamphlet. However, its Flesch reading-ease index of 42/100 was best suited to university graduates. The document was written in formal English with medical jargon, which was inappropriate for those with low levels of health literacy. The pamphlet listed information on the types of diabetes, risk factors, signs/symptoms, and management/control. However, it did not provide detailed information for patients who required more than a superficial knowledge of diabetes and diabetes self-management.
Participants believed that a combination of health education, counseling, and advice could help patients understand their disease, accept it, and comply with medical instructions. Despite the medical compliance approach that dominated SMS, HCPs attempted to integrate specific cultural values and practices to make their care acceptable to patients.
Theme 3: Navigating Sociocultural Terrain
HCPs at both hospitals practiced in contexts where many patients thought that diabetes had supernatural causes and had similar beliefs about the efficacy of herbs and spirituality in treating diabetes. Moreover, the local culture entailed a strong family orientation which meant that family members were intimately involved in the patient self-management of their diabetes, including providing financial assistance, assistance with dietary management, and self-care decision-making. These cultural practices influenced how patients approached diabetes care and the SMS attitudes/practices adopted by HCPs. Navigating sociocultural terrain has three subthemes: (a) involving God and prayer in patient care, (b) allowing the judicious use of herbs, and (c) family involvement. HCPs allowed the integration of cultural and medical practices if there was no potential harm. As individuals and community members, participants shared many of the same beliefs and values prevalent in this context, including a firm reliance on God. Their advice on continuing/discontinuing cultural practices depended on whether they were medically harmful.
Involving God and Prayer in Patient Care
In traditional Igbo culture, chronic diseases are thought to have supernatural origins (e.g., evil spirits or curses). These beliefs coexist with dominant Christianity. During counseling, HCPs leveraged shared Christian spiritual beliefs to support and encourage patients while offering a biomedical model of care as the primary standard. For example, physicians encouraged patients not to abandon their prescribed medications but to combine prayers and medications instead: “We tell them that, even if you have such beliefs [believe that praying will heal you], try and combine it with the orthodox way of treating this condition. We still pray because God cures them, and God also gives the knowledge and wisdom to discover those drugs being used.” (Endocrinologist)
Belief in God was employed to encourage patients to endure distress caused by their physiological condition. However, reference to God did not occur at the expense of worldly care: “Some of us physicians are spiritually inclined. We also talk to them on that note, using spiritual tactics, but that will not be at the expense of the actual physical thing they have come to know. Somebody like me knows that there are spiritual aspects of many things, almost everything, but these are things you cannot prove physically; it is by faith. You can try to explain to people that some things have a spiritual relationship, but they, as humans, have a role to play.” (Endocrinologist)
Spirituality was used to maintain hope and promote overall well-being, as some participants considered spiritual well-being essential for overall health, even though the disease was physical: “I encourage people. I give them hope and tell them what we usually say, that medical people care, but God heals… God can heal anybody, so when we talk to people, we encourage them. Even if they are not physically healed, spiritually, and psychologically they will be encouraged.” (Endocrinologist)
HCPs incorporated prayer into clinical activities. For example, health educators regularly sang Christian songs and prayed with patients before initiating education.
Allowing the Judicious Use of Herbs
The use of herbs or vegetables was not uniformly encouraged due to the lack of scientific evaluation and unknown side effects: “The first one I told you is onugbu, the bitter leaf [Vernonia amygdalina]… We tell patients that those herbs even have side effects. They can even affect their liver, their kidney, and things like that, and even if those things have effects on lowering blood sugar, they do not know the appropriate dose to use, so it is better to use the drugs that are already tested rather than herbs and be coming for their checkup so that medical personnel will monitor them.” (Endocrinologist, Hospital 1)
Some HCPs discouraged usage, as the benefits were unknown. However, cultural practices were not always outrightly integrated or refused but modified at the practitioner’s discretion. At times, HCPs altered prevailing practices to harness potential benefits or prevent harm. For example, dietitians believed that some vegetables and herbs (e.g., bitter leaves and scent leaves; Ocimum gratissimum) were safe but instructed patients on modifications before consumption; instead of washing herbs and drinking herb juice, they encouraged blending the vegetables and herbs and drinking the juice with fiber. This was permitted due to the benefits of fiber on blood sugar rather than any juice benefits, as patients widely assumed: “They squeeze out the water [juice] from onugbu and nchanwu and drink them. I tell them they should grind the onugbu with the fibers, and they can eat them in small quantities. So when they come, we tell them that it is incorrect; they have to wash it very well, grind it together, and not remove anything.” (Dietitian, Hospital 1)
All participants actively discouraged patients from abandoning medical treatments for cultural reasons. Many believed in God and God’s infinite power alongside their medical training and freely discussed religion with patients when desired. They also acknowledged other cultural practices (e.g., individual-family interdependence) and openly encouraged family involvement in patient care.
Family Involvement
Participants actively encouraged patients to visit the hospital with relatives and talked to all parties, as this was thought to help in self-management. At times, they also educated relatives on self-management tasks (blood glucose checks, insulin injections, and dietary management). Family members were assumed to encourage patients and reinforce any teachings at home. As traditional gender norms in the Nigerian Igbo context entailed that female relatives were responsible for meal preparation, HCPs also educated families—especially female members—about dietary requirements and encouraged them to help patients adhere: “Some people come to the hospital alone, and I feel such people should be accompanied to the hospital by a family member. When they come alone, I tell them to come with their relatives. Then we educate the relatives, tell them that the patient needs help.” (Endocrinologist)
It was common to see a patient come in with one or two relatives. Such relatives usually go in with patients to see the physician, nurse, or dietitian. Some patients were reluctant to administer insulin or check their blood glucose levels, in such cases, family members were taught how to assist with these self-management tasks. They were also invited to help make important decisions about managing the patient’s condition, especially when the proposed treatment was expected to cause emotional distress.
On the other hand, some family members advocated for their loved ones by refusing treatments they perceived as distressing. Although HCPs involved families in obtaining consent to ensure that all parties agreed, this was mainly achieved through persuasion. HCPs used their expert positions to persuade that the chosen course of action was in the patient’s best interest. As discussed in the following section, HCPs also used various strategies to circumvent structural barriers at their diabetes clinics.
Theme 4: Workarounds
At both clinics, diabetes management was hindered by social and structural barriers, including the absence of health insurance for most of the patient population and insufficient resources for managing the educational and psychosocial needs of patients with diabetes. For example, there were neither diabetes educators nor sufficient time/resources dedicated to diabetes education. In general, hospitals and communities were not equipped to offer ongoing support, making implementing SMS challenging. Theme 4 highlights the different approaches that participants used to bypass various organizational challenges in this regard. Specific strategies included providing personal phone numbers to patients and exercising flexibility in drug and laboratory prescriptions. To provide support to patients beyond clinical hours, some HCPs at both hospitals gave their private phone numbers to patients in case they encountered problems at home or were confused about taking or interpreting their blood sugar results: “Yes, we give them our numbers; they call to tell me their blood sugar… suppose the patient feels that the blood sugar is enormously low. In that case, you reassure the patient by saying, ‘that is the level we want, and there is no cause for alarm; continue your medications at that level.’” (Endocrinologist)
Although this could avert emergencies or complications, it was unclear how many patients sought support in this way, nor was this practice directly observed. HCPs also tried to reduce the financial burden of diabetes management by tailoring prescriptions to each patient’s financial status and soliciting free drugs from drug companies: “For patients of low socioeconomic status who require insulin, it might be difficult to prescribe the necessary type of insulin, and you might go with what the patient can afford… some of our patients with cost constraints may have to do with less monitoring… we tailor the treatment towards the patient’s peculiar case…” (Endocrinologist)
Discussion
The current findings add to our understanding of Nigerian HCP views and SMS practices for individuals with T2DM. As characterized by the four identified themes, participants enforced compliance and integrated cultural values/practices. The conceptualization of SMS and the underlying assumptions identified in this study differs from the Western world’s current approach. The current conceptualization of SMS in the West, particularly in North America, has focused on power sharing between HCPs and patients (Aujolat et al., 2008; Lorig & Holman, 2003) by enhancing patients’ self-efficacy and problem-solving skills. This practice is a significant contrast to the findings in this study, where HCPs assumed effective control while patients and families took a subordinate and passive role of listening and carrying out HCPs’ instructions. This practice is traditionally conceptualized as compliance (Anderson, 1985). The study participants’ interactions with clinic patients focused on HCPs’ desire for patients to comply with medical instructions. Developing SMS from this stance involves a shift from expecting compliance to promoting patient autonomy and empowerment; this shift is possible when patients are enabled to develop the knowledge, skills, confidence, and capacity for self-management (Powers et al., 2020; Thille et al., 2014). The compliance orientation is evident in many studies conducted on diabetes in Africa. Many researchers in Africa who have conducted studies on adherence (used interchangeably with compliance) found that instructions and treatment goals were usually established with little or no input from patients and assumed that SME and SMS were in place for patients (Abrahams et al., 2019; Adejoh, 2014; Watermeyer et al., 2019). Unfortunately, this assumption does not seem to be borne out, given the findings of this and other studies.
The problem with compliance orientation is that rigidly applied instructions may not reflect or apply to the patient’s changing circumstance. Moreover, compliance fosters a feeling of powerlessness on the part of the patient, who must entirely depend on the providers’ knowledge and goodwill. Major principles inherent in modern SMS approaches include patient autonomy and empowerment, patient-centeredness, and collaboration between patients and HCPs (Aujoulat et al., 2008; Kawi, 2012; Morgan et al., 2015). Patients should play an active role in making decisions about their health (Fumagalli et al., 2015; Funnell, 2016). In turn, SMS must shift from a disease-focused approach to more holistic care because diabetes, like many chronic illnesses, affects not just the patient’s body but every aspect of the patient’s life. This requires the health provider to forego the sole decision-maker role and instead provide ongoing support and guidance, addressing the clinical, educational, psychological, and behavioral aspects of care needed for daily self-management of diabetes (Powers et al., 2020). This requires a partnership between a multidisciplinary team of HCPs and patients (Bain et al., 2019) to identify patients’ health needs jointly, set priorities, establish goals, and create treatment plans that consider individual knowledge/expertise as well as personal and social contexts (Anderson & Funnell, 2010).
Although HCPs in this study believed that education is a crucial component of SMS, SME was minimal because there was little or no time to squeeze in diabetes self-management education during the official consultation time. This was compounded by the absence of dedicated diabetes educators. Poor SME is a recurring finding in much diabetes research conducted in different African nations (Alaofè et al., 2021; Chepulis et al., 2021; Steyl & Philips, 2014; Suglo, & Evans, 2020; Werfalli et al., 2020). In a study carried out to outline the obstacles encountered by individuals with diabetes in South-African primary healthcare settings, Steyl and Philips reported patients not getting enough information because staff had many patients waiting and did not have enough time to provide diabetes education. In Alaofè et al.‘s (2021) study, patient-participants complained of insufficient information about their condition and its treatment, while the provider participants complained of not having enough time to explain or allay concerns about medications and other treatments. Without SME, patients may not have the required knowledge and skills to self-manage. Moreover, diabetes education, when provided in this study, was a one-way flow of information from the clinician to the patient. DSME should incorporate interactive and collaborative teaching tailored to individual needs (Fan & Sidani, 2009). The content and skill-training components of SME are individualized according to the patient’s ability, barriers, culture, literacy level, and available resources (Powers et al., 2016); this can only be realized when both the expert knowledge of the clinician and the experiential knowledge of the patient are brought to the table.
The only diabetes educational resource available in one of the hospitals was deficient. Similarly, the diet guide was inadequate. Patients in both hospitals often perceived using the diet guide as akin to starving. In fairness to the patients, the guide stipulated small portions for everyone without considering sex, age, or activity level. Given that dietary management is a key component of diabetes care and one that patients often find challenging, as noted in this study and reported by other researchers (Suglo & Evans, 2020; Uchenna et al., 2010), there is a need to review the diet guide used in the management of diabetes in Nigerian hospitals emphasizing the food pyramid, exchange list, carbohydrate counting, and glycemic index (Nwawuba et al., 2019). Dietary counseling should also be patient-centered, acknowledging patient preferences while allowing for flexibility (Cheng et al., 2016). To achieve this, SME should include information about matching insulin dose with carbohydrate content, the impact of physical activity on blood glucose, and recognizing and treating hypoglycemia (Munshi, 2017).
While there is an urgent need to make significant changes to diabetes management in Nigeria, this study also reported positive findings. For example, HCPs facilitated social and spiritual support by incorporating existing cultural values (e.g., prayers and family involvement in patient care). As a workaround, they also provided their personal phone numbers to assist patients with urgent concerns (e.g., hypoglycemia). A particularly critical activity was combatting social beliefs that diabetes was a death sentence, therein addressing spiritual needs and providing hope. Integrating knowledge about patients’ cultural beliefs, values, and practices is associated with improvements in diabetes-related knowledge, perceived competence in managing diabetes, quality of life, and ultimately reduced HbA1C levels (Attridge et al., 2014; Gucciardi et al., 2013). Some of the participants’ activities meet the criteria for SMS according to the comprehensive descriptive taxonomy of SMS interventions (Pearce et al., 2016). For example, the participants facilitated social support by encouraging family participation. Like this study, others have reported both supportive and discouraging effects of family involvement in diabetes management in Africa, and other parts of the world (Abdulrehman et al., 2019; Bross et al., 2022; Chepulis et al., 2021; Mogre et al., 2019; Othman et al., 2022; Suglo, & Evans, 2020; Werfalli et al., 2020), necessitating the need for not only involving families in patient education but also educating them on how to prevent diabetes for themselves, as well as how to support a family member living with diabetes (Thirsk & Schick-Makaroff, 2021).
The practice of providing personal phone numbers to patients filled the gap created by the absence of a formal channel for continual support. HCPs also prescribe cheaper generic medications to help patients. Similarly, innovative practices are being integrated into chronic illness management in resource-constrained areas to improve patient outcomes. For instance, medication adherence clubs (MAC) were developed in South Africa to manage stable patients with HIV and were associated with good patient outcomes (Luque-Fernandez et al., 2013). These MACs were adopted in Kenya and extended to include stable patients with diabetes and hypertension; the clubs were nurse-managed, and patients could go in for drug refills and SME (Khabala et al., 2015). In a retrospective study to assess the care of persons with hypertension, diabetes, and HIV enrolled in 47 different MACs in Kenya (each MAC having 23–25 stable patients), Khabala et al. found that the program was successful in offloading 2208 consultations from the regular clinic. Moreover, patients were satisfied with the care received, and the loss to follow-up from MACs was only 3.5%.
Other countries have explored using volunteers and peer-to-peer support in chronic illness SMS. Angwenyi et al., (2019) found that community health volunteers and “expert patients” provided health information, emotional support, and shared life experiences, which greatly helped persons with HIV in their self-management. Using non-physician and non-medical persons to provide SMS may alleviate time constraints, and the lack of diabetes educators reported in this study and others and could improve the care of persons with diabetes in Nigeria.
Nonetheless, the workarounds described in this study were not uniformly implemented but relied on individual HCP discretion. Evidence-based and sustainable approaches are needed to enhance SMS. Urgent efforts are required to improve diabetes SMS knowledge/practices in Nigeria. Structured DSME programs are also imminently needed for diabetes patients in developing countries.
Limitations
This study had some limitations regarding the sample and setting. First, both hospitals were government-owned and attracted middle/lower socioeconomic groups due to their cheaper rates. Future studies should therefore include private hospitals in Nigeria where patients with higher socioeconomic status attend. Not all HCPs in Nigeria were represented, as this study was localized in one Nigerian state. In addition, the study sample may not represent other diabetes clinics, as health educators were also included. However, the findings may apply to similar resource constrained areas. Researchers should explore other cultural groups in differing geographic areas in Nigeria.
Conclusion
This study examined SMS for T2DM patients in Nigeria based on the perspectives, experiences, and practices of HCPs. These findings provide an opportunity to reflect on the current nature of provided support and how it contributes to the poor state of diabetes care. In particular, the traditional biomedical approach to treatment has influenced the Nigerian healthcare system to perpetuate an SMS approach that focuses on formal control. Despite the desire to support T2DM patients and their families, HCPs are rarely equipped to provide effective and sustainable support, thus emphasizing the need for change.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.