
Abstract
Health coaching is a novel population intervention to support self-management but it is untested in people with mild disease. People with chronic obstructive pulmonary disease with mild dyspnea are a population excluded from supported self-management and whose illness might progress without intervention. We explored participants’ experiences about how health coaching motivated behavior change. Interviews were conducted with 21 intervention and 10 control participants at 6 months, and 20 intervention participants at 12 months. Participants were identified from a randomized controlled trial of telephone health coaching. Data were analyzed using the framework method. Participants positively enacted behavior change to become more physically active. Participants took advantage of environmental affordances to pull themselves toward activity targets, or relied on being pushed to be more active by the health coach or significant others. Behavior change was maintained where efforts to be more active were built into the everyday lifeworld of participants.
Keywords
Introduction
Over the past two decades, the global burden of disease has significantly shifted away from communicable to noncommunicable long-term conditions with more years lost to disability from cancers, cardiovascular diseases, musculoskeletal disorders, chronic respiratory diseases, digestive diseases, and diabetes, especially among older adults (Murray et al., 2012). Reorganizing health care systems to respond to these epidemiological and demographic challenges is a critical feature of health policy in high-income countries, and increasingly in low-and middle-income countries too (Coulter, Roberts, & Dixon, 2013). Supporting people with long-term conditions, such as chronic obstructive pulmonary disease (COPD), to engage in self-managing their illness is a key strategy to improving the quality and outcomes of health care for this growing population. Provider-based approaches to supporting self-management draw on health service architecture, such as clinical information systems and decision support aids, to support practitioners to monitor symptoms, undertake medication reviews, and give lifestyle advice (Bodenheimer, Lorig, Holman, & Grumbach, 2002; Department of Health, 2005). In the United Kingdom, such an approach has been incentivized by the Quality and Outcomes Framework (QOF), which is a pay-for-performance contract that rewards general practitioners (GPs) for effectively managing long-term conditions in line with evidence-based quality indicators (Doran et al., 2006). By contrast, patient-based approaches to supporting self-management look to equip patients with the relevant skills, confidence, and knowledge to self-manage their condition. For example, the Expert Patient Program is a lay-led educational intervention designed to encourage and instill self-care skills through goal setting, participative techniques, and task-oriented approaches to problem solving (Foster, Taylor, Eldridge, Ramsay, & Griffiths, 2007). However such programs can have limited reach and target only people who are educated, affluent, and previously engaged with their health (Ryan, Wilson, Taylor, & Greenfield, 2009).
Health coaching has emerged as a model of care that has the capacity to support self-management at scale and reach a higher proportion of people with unmet need. This is especially true of telephone health coaching which has been defined as a regular series of phone calls between patient and health professional to provide support and encouragement to the patient, and promote healthy behaviors such as treatment control, healthy diet, physical activity and mobility, rehabilitation, and good mental health. (McLean, Protti, & Sheikh, 2011)
There is emerging evidence that telephone health coaching can effectively promote health behaviors and improve self-efficacy and health status in people with a broad range of long-term conditions (Dennis et al., 2013; Kivela, Elo, Kyngas, & Kaariainen, 2014). Telephone health coaching might also be associated with wider engagement with health services and uptake of planned services but reductions in unscheduled care, making it potentially cost-effective at conventional willingness to pay thresholds (Panagioti et al., 2018). However, there is less certainty about how health coaching brings about these outcomes and for whom it is most effective and in what settings (Hutchison & Breckon, 2011; McLean et al., 2013). Understanding how complex interventions such as telephone health coaching are delivered and exploring mechanisms of impact and contextual factors external to the intervention are an essential component of evaluations that aim to identify and characterize factors critical to post-trial implementation (Moore et al., 2015).
People with COPD with mild symptoms of dyspnea are a key exemplar population who might be disengaged or excluded from self-management interventions and potentially reached by telephone health coaching. COPD is a progressive lung disease and medical management is currently unable to reverse decline in lung function (Vogelmeier et al., 2017). Despite falling rates of smoking in high- and middle-income countries, the prevalence and burden of COPD is rising worldwide and it is the third most common cause of death globally (Burney et al., 2014).
Structured self-management interventions facilitated by practitioners that include goal setting and practitioner feedback and combinations of smoking cessation, action plans for exacerbations, an exercise or physical activity component, advice about diet, advice about medication or coping with breathlessness, can improve health-related quality of life (HRQoL), dyspnea (breathlessness), and reduce respiratory-related and all-cause hospital admissions in people with COPD (Zwerink et al., 2014). However, trials of self-management support interventions have tended to only include patients with moderate or severe symptoms making it difficult to draw conclusions about the relevance of these approaches to people with mild COPD who are mainly managed in primary care population (Haughney et al., 2014). Identifying candidate interventions that can be rolled out at scale to prevent the progression of COPD in patients who present with early signs of the disease and mild symptoms is a priority (Csikesz & Gartman, 2014; Department of Health, 2011).
The Patient Self-Management for COPD (PSM-COPD) randomized controlled trial was conducted between March 18, 2014, and February 5, 2015 (Jolly et al., 2018). It tested the effectiveness of telephone health coaching delivered by a nurse to support self-management in a primary care population with mild symptoms of COPD. It was hypothesized that compared with usual care, telephone health coaching would lead to improved HRQoL, and also improve dyspnea, physical activity, smoking cessation, psychological health and self-efficacy for managing COPD and undertaking physical activity. The trial found no significant difference between the telephone health coaching and usual care arm for HRQoL. There were also no significant differences in the EuroQoL 5 Dimensions 5 Levels, Hospital Anxiety and Depression Scale, Stanford self-efficacy scale, or level of breathlessness. At 6 months, total self-reported physical activity, walking, moderate, and vigorous intensity activity were all significantly higher in the intervention arm but the difference was not significant at 12 months. There was also no difference in smoking cessation rates at 6 and 12 months. Self-reported self-management activities targeted by telephone health coaching (medication adherence, inhaler checks in past 6 months, having written advice about what to do if symptoms worsened and having an antibiotic rescue pack) did improve in the intervention group at 6 months and many of these differences remained at 12 months.
We report here the findings of a qualitative study that was conducted alongside the PSM-COPD trial that aimed to explore why, how, and in what contexts people with mild COPD engaged in self-management activities following exposure to the telephone health coaching intervention. We also aimed to explore the ways in which self-management activities were maintained or discarded over the longer term.
Method
The PSM-COPD Trial
Full details of the protocol for the PSM-COPD trial have been published (Sidhu et al., 2015). Participants for the PSM-COPD trial were recruited from 71 general practices across England. Patients were eligible if they were aged 18 years or above, on the general practice register for COPD with mild dyspnea (Medical Research Council [MRC] Grades 1 [only breathless on strenuous exercise] or 2 [only get short of breath when hurrying on level ground or up a slight hill]), and had a Forced Expiratory Volume in 1 second/Forced Vital Capaity (FEV1/FVC) <0.7 after post-bronchodilator spirometry (Vogelmeier et al., 2017). Patients were only excluded from the trial if they self-reported that their level of dyspnea was MRC ⩾3, or if their GP reported that it would be inappropriate for the research team to invite them to take part in the trial (e.g., terminal illness, severe psychiatric disorder).
Health Coaching Intervention
The intervention targeted four health behaviors associated with optimal self-management of COPD: medication management and adherence, smoking cessation, physical activity, and action planning. Intervention components were delivered by telephone and by post over 24 weeks. The telephone components were delivered by eight specially trained study nurses. The nurses received 2 days of training and were able to practice telephone coaching sessions with the research team.
In Week 1, participants received an initial 35- to 60-minute telephone consultation that focused on discussion of timing of last check of inhaler technique and where relevant setting a goal to get inhaler technique checked in general practice. Where relevant medication adherence was also discussed. Participants were given memory prompts and advice about restructuring their environment and getting support from their partner to maximize mediation adherence. Participants who were still smokers were given opportunities to discuss smoking behaviors, quit attempts and barriers to quitting, and encouraged to set a goal to contact a smoking cessation service and get social support to help them quit. Current levels of physical activity and breathlessness were discussed in the context of setting goals to increase duration and/or intensity of physical activity and how to use a diary to record activity. Finally, participants were given time to discuss action planning as part of how they managed exacerbations. Nurses identified whether participants had a written action plan and whether participants were confident about using such plans. Participants were prompted to discuss action planning at routine appointments in general practice if they lacked understanding or confidence about using these plans. In Week 1, participants also received by post a physical activity diary and a booklet that included information on the benefits of activity for COPD and how to overcome barriers. A pedometer with instructions and an inhaler technique instruction leaflet were also sent by post. Participants who smoked received a smoking information booklet that included the contact details of smoking cessation services.
Participants received a further three 15- to 20-minute telephone contacts at approximately 3, 7, and 11 weeks after randomization. The second call at Week 3 focused on discussing progress and barriers to achieving goals set in the first session and reviewing physical activity levels and setting new goals. Smoking cessation and medication management and action planning were discussed as required. Participants received by post information about opportunities for physical activity in their locality and information leaflet titled “What are SMART goals?” along with a SMART goals sheet.
During Weeks 7 and 11, the telephone contacts focused on discussing progress and barriers to achieving goals set in previous sessions and reviewing physical activity; smoking, medication management, and action planning were discussed as required. By post, participants received a SMART goals sheet. A further SMART goals sheet was sent by post at Week 16 and the final contact by post at Week 24 included information about opportunities for physical activity in the locality and a leaflet on tips for sustaining physical activity.
The physical activity element of the intervention was underpinned by Social Cognitive Theory (Bandura, 1986). This is a reciprocal causation model which proposes that behavior is driven by a combination of personal (cognitive, affective, and biological) and environmental factors (social norms, culture, media).
Qualitative Study Design
We used a parallel mixed-methods design whereby qualitative data were collected concurrently with trial data (but blind to trial outcome) between baseline and 12 months post-randomization (Nastasi et al., 2007). This approach underpins well-established methods to achieve convergence between different sources of nonoverlapping data, starting with a confirmatory and quantitative data analysis phase, followed by qualitative analysis and inference (Tashakkori & Teddlie, 1998).
Recruitment and Selection of Participants for the Qualitative Study
After ethical and research governance procdedures were complete the research team invited participants who had consented to take part in the trial to also consider being approached for a qualitative interview. 1 Once permission to contact was given, the researchers obtained consent to interview from willing participants at the first follow-up assessment at 6 months. There were 267 participants in the intervention group and 287 participants in the control group eligible for interviews at the 6-month assessment. Researchers ran a query in MS Access to identify eligible participants based on the following sampling characteristics likely to affect engagement with the intervention: baseline HRQoL, geography (urban or rural location), age, and gender. HRQoL was determined using a single item of the St. Georges Respiratory Questionnaire (Jones, Quirk, Baveystock, & Littlejohns, 1992), which aims to characterize patients’ functional limitations in relation to their ability to do the things that they want to do on a daily basis (Part 2, Question 7). 2 We invited the 58 participants drawn evenly from the four regions involved in delivering the PSM trial to take part by letter; of which, 48 agreed.
Data Collection
Semi-structured interviews were conducted by a researcher with a health psychology background or researcher with a community nursing background and were recorded and transcribed verbatim. Recruitment to the trial began in March 2014 and ended in February 2015; between January and September 2015, participants in the intervention arm were interviewed at 6 and 12 months post-randomization; participants in the control group were interviewed only at 6 months post-randomization. The 6-month interviews were conducted face-to-face in participants’ homes or at another location identified by them as convenient. The majority of 12-month interviews were conducted over the telephone.
Topic guides were used to guide interviewers and prompt participants. Table 1 describes the topics discussed with participants in the intervention group at 6 and 12 months. The control group version excluded items about the role of coaching in the process of behavior change (Supplementary File 1). Only participants in the intervention group were interviewed at 12 months as these follow-up interviews were principally aimed at exploring how exposure to the intervention had supported maintenance of behavior change over the longer term.
Topic Guides for the 6- and 12-Month Interviews With Participants in the Intervention Group.
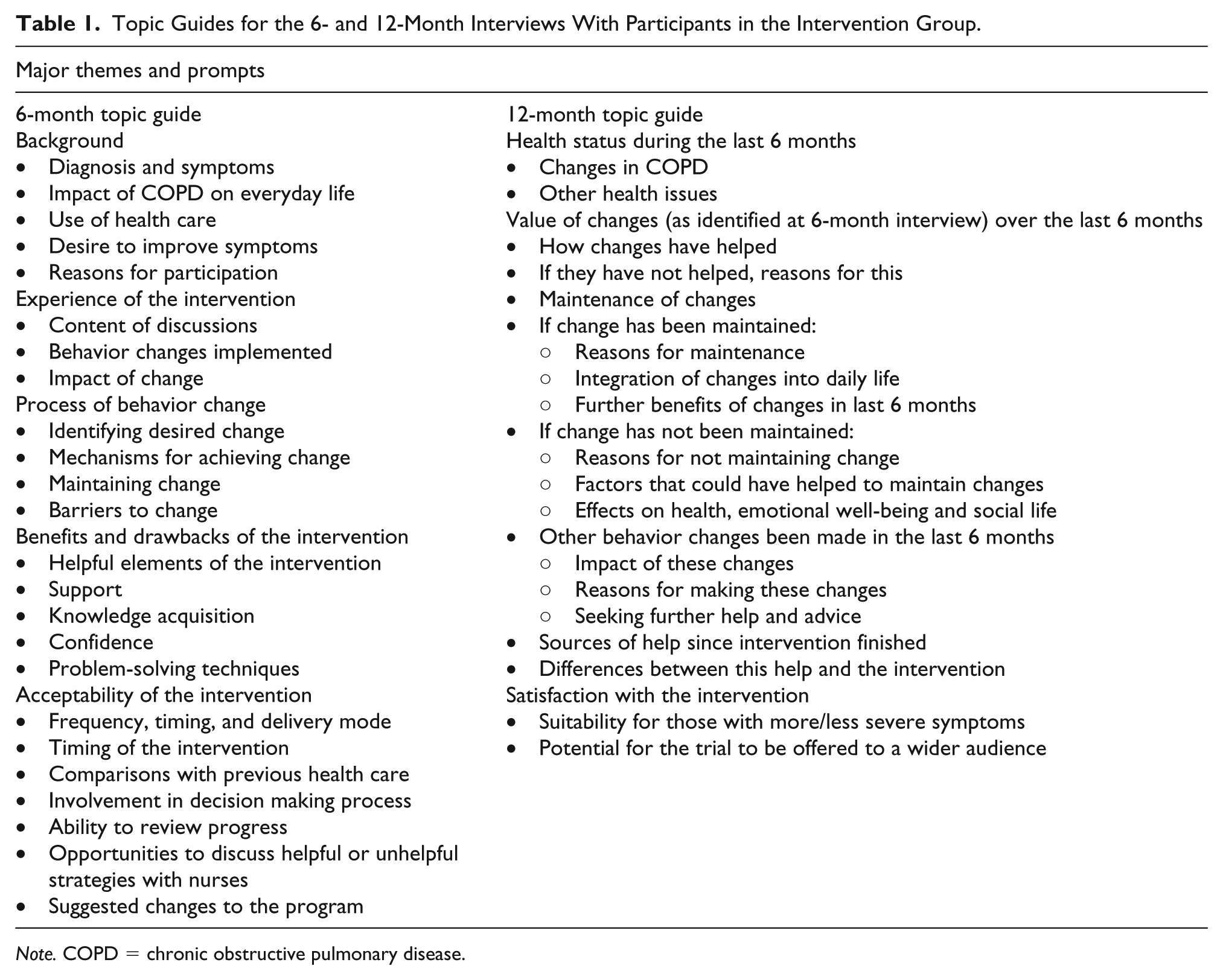
Note. COPD = chronic obstructive pulmonary disease.
The 6-month interviews were conducted with 31 participants across the intervention (n = 21) and control groups (n = 10); 20 (95%) participants from the intervention group were interviewed at 12 months. The 6-month interviews lasted between 27 and 64 minutes; the 12-month interviews were between 20 and 48 minutes. The age of interviewees ranged from 50 to 85 years and 21 participants (67%) were male; there was no difference in the mean age of participants who agreed to be interviewed (70.6 years) and the mean age of participants in either the intervention group (70.7 years) or control group (70.2 years). All were either retired or semi-retired. Twenty-four (77%) were ex-smokers and six were still smoking at the time of their baseline interview. All participants self-reported that their COPD was mild (MRC Grade 1/2) and that their COPD symptoms either did not stop them from doing anything that they wanted to do, or stopped them doing only one or two things that they wanted. Participant characteristics are shown in Table 2 in Supplementary File 2.
Data Analysis
Data were analyzed with the framework approach (Ritchie & Spencer, 1994). We followed five steps that are core to using framework: (a) Familiarization—researchers blind to the trial outcomes familiarized themselves with the data by reading transcripts and/or listening to the recordings to identify key themes; (b) developing a thematic framework—an initial thematic framework was developed in Excel and refined and, where necessary, expanded to take into account emerging themes; (c) indexing—themes were labeled and indexed; (d) charting—a matrix by participant and theme was compiled for the intervention and control group interviews; (e) mapping and interpretation—the data were mapped across participants and between groups to support interpretation and synthesis. Data derived from the 12-month interviews were incorporated within the 6-month matrix for the intervention arm: new codes were added to capture themes that spoke to data about maintenance of behavior change. In this sense, longitudinal data were not used to construct narratives about individual participants, rather it contributed to the properties of themes previously identified in the 6-month interviews (Calman, Brunton, & Molassiotis, 2013). Trustworthiness of the analysis was increased by a process of discussing the framework matrix with the wider team drawn from different disciplinary backgrounds (Henwood & Pidgeon, 1992). This process was completed before trial outcome data were known. Interpretation of the qualitative findings as presented in the discussion was undertaken after the trial outcome was known and shared with all members of the qualitative team.
Results
We encountered data 3 that spoke to three core themes that described the processes by which participants engaged with or enacted over time. Data saturation was apparent in the data from both control and intervention groups for Theme 1; saturation was apparent in the data from intervention participants for Themes 2 and 3 but not from control participants who were not exposed to the same opportunities to undertake self-management activities.
The three themes are the following:
Motivation: which focused on unpicking participants’ pathways to self-management in the context of their prior understandings and experiences of COPD.
Mechanisms: which sought to explain how participants’ motivations to engage in self-management underpinned choices about which behaviors to engage with and how these choices were translated into action.
Maintenance: which centered on understanding factors that enabled or constrained longer term engagement with self-management after exposure to the health coaching intervention.
Motivation: From Diagnosis to Self-Management
Motivations to engage in self-management behaviors were foregrounded by participants’ desire to offer countervailing and more positive narratives about their illness that broke with their previously held negative attitudes about COPD. Many participants recalled feeling “shocked” and disbelieving when first given a diagnosis of COPD. This was especially true among those who had no prior understanding that they might have a chronic lung problem, as recalled by this female ex-smoker: Oh yes I didn’t know anything about it before. When I was first told what the COPD stood for I was horrified and then the other name for it was emphysema and I thought oh my goodness.
In instances where “. . . unless you know what it [COPD] is, you just brush it off, it seems to bounce over your head . . .,” participants had been less likely to take stock of the impact of COPD and consider options about self-management. This was true also for participants who were persuaded by their GP that their declining physical health was associated with aging rather than specifically with COPD, as this male participant from the control group in his early 70s explained: No. He [the GP] just said, go and see the asthma nurse. When you get to 65, they say to you, how old are you? Over 60. Oh, are you, right, you better go and see the asthma nurse, go and see her.
For some, again, especially ex-smokers who had no prior warnings about their illness, being dismissive of COPD was also a by-product of their mistrust about the motives that lay behind the diagnostic process: Well, it seemed to catch all situations, it wasn’t specific. And I just got that impression, it was just a case of form filling on the part of the GPs, where they get an extra from the Government for doing this, that was it.
More rarely, but particularly pertinent in the case of younger participants, shock about being given a diagnosis was compounded by overly blunt communication on the part of their GP, often typified by rushed and pithy discussions about self-management: . . . it was the look on the nurse’s face I think, and the way he [GP] delivered it, I just thought oh my god. Then he gave me a website to look it up. So he gave me the NHS medical website, is it? Or WMD Medical website I think it was. Yeah. Actually I think it was the way it was delivered. It was very doom and gloom.
These early encounters with COPD meant a sense of fatalism had rapidly taken hold among many participants. For this group, the chance to engage in self-management was wrapped around altruistic notions of wanting to be in a position to help others if not themselves. There was a strong perception that COPD was “self-inflicted” and that the prospect of good health as being “too late for me.”
However, even in the face of a near universal belief that “the damage has been done,” some participants were motivated to engage in self-management to positively fend off further decline, such as this male participant who experienced more shortness of breath: All you can do is maintain the level. It’s not going to get . . . well it is going to get worse but you can make it as slow as possible don’t you? Well, that’s the idea. That motivates you a bit. Well it should motivate everybody.
For others, across both the control and intervention groups, maintaining function was similarly a strong motivating force to self-manage but their motivations to do this were underpinned by fear of becoming incapacitated “. . .walking round with this bottle of oxygen” and losing their independence. This determination to not succumb to the effects of a progressive illness was typified by this female participant: Because I want to stay independent as long as I possibly can I really do and I think well so long as I keep doing it I don’t want to finish up in a wheelchair and gasping for oxygen. It’s the thought of what it might turn to if I don’t keep going is what really gets me . . . motivates me.
Narratives about exerting a sense of personal control over COPD by becoming better self-managers were also underscored by a desire among some participants to distance themselves from what they perceived to be an overly medicalized existence: Well . . . what I thought I might learn, was extra skills in doing that, and I’m all for doing that if I can possibly help it, manage it. So yeah, I think that was the reason, the emphasis on, yes, almost de-hospitalizing, de-doctoring, de-medicating this.
Mechanisms—Pathways to Change
The key finding about what elements of the intervention participants engaged in centered on their overriding preference to increase their physical activity. The majority were ex-smokers having given up in the immediate aftermath of their diagnosis; those who still smoked felt inclined to “buy a packet occasionally” or had cut back as far as they were prepared or able to, smoking “between 5 and 10 a day.” The role of action planning to support moments of respiratory crisis and learning about inhaler use were relegated as minor themes, and as such, the findings here offer insight into how participants were enabled and enabled themselves to increase activity.
Goal setting was the principal tool at the disposal of nurses to encourage participants to increase physical activity. Although there was some evidence that goal setting took place, either mutually or in more self-directed ways, there was an overriding ambivalence or, in some instances, outright resistance to using this technique to increase activity. This was partly because some relatively active participants had made the judgment that setting explicit goals was unnecessary because “. . . most of the stuff, I was really already doing, you know.” Or, for others, goal setting was an unhelpful reminder of the chore of achieving targets in previous roles while employed and, as this retired male participant explained, “once you’ve got rid of it [goal setting] you don’t want to do it again, even if it is for your own good possibly.”
More central to how participants enacted goals was the way health coaching acted as a spur for participants to avail themselves of environmental affordances to adopt more active ways of doing routine tasks such as shopping. Here, affordances are conceived as the range of latent action possibilities that are perceived by an actor in the presence of an object or an environment (Gibson, 1979). The extent to which such environmental affordances can be translated into action is contingent on the observer’s capabilities and intentions, and as such, affordances are relational and dynamic. Sometimes, for those who became breathless less often, the use of environmental affordances was expressed in strategic terms, for example, by clearly indicating a move to take advantage of opportunities to walk more and use the car less: In other words, don’t get the car out when it’s only a few minutes’ walk. Make that walk a bit longer. I can go up to the village to do the shopping, by going up the road. I can also go down the road, and along the bottom, and up, and turn it into a fifteen minute walk rather than . . . yeah. And it was a consciousness, I think, that stayed with me.
For others, particularly those living in urban areas, changes in their immediate built environment coincided serendipitously with the advent of the health coaching intervention, bringing about a change in behavior not previously thought possible. Here, as with this male participant, the offer of health coaching afforded participants opportunities to establish new routines off the back of changes to their environment: So it was quite fortunate in a way, it [intervention] coincided with . . . we’ve always had our daily paper delivered for god knows how long, 30, 40 odd years. But the newsagents we use were closing down and I took that as an opportunity to go and walk for the daily paper. Now, I don’t for a minute think I . . . well, I wouldn’t have done it if it hadn’t have been for this [closure]. Absolutely no way.
Affordances were also identifiably present in the shape of pet dogs. Dog walking featured strongly in this theme, with participants pointing to the needs of their dogs to be exercised as instrumental in themselves becoming active: They do get me out because they go and stand by the front door because they want to go out and I’ll take them out for ten minutes or so.
Among those who were already active, such as this female participant, dog walking was also presented as a means to increase the intensity of daily exercise: . . . so I thought I already exercise with the dogs walking and it’ll give me more incentive to try and speed up what I can do.
By contrast, accounts in which the health coach figured as a spur to either continue or increase activity reflected a sense in which participants were also reliant on being pushed to engage in behavior change. For participants who were “pretty motivated anyway,” the scheduled contact with the health coach represented “an extra push” to be more active. This was especially relevant to those participants who identified the health coach as an authority figure with the capacity to bestow upon them a sense of positive affirmation about making changes to their daily activity. One male participant who was trying to be more active eagerly anticipated the moment when he could declare to the health coach that he had become more active: Well it was just in me own mind and I felt like she keeps asking me so next time I’m going to tell her I’m still doing it and I’m doing more . . . You know what I mean? Cos I thought she’d be impressed if I did a bit extra.
In other instances, participants felt morally obligated to honor commitments made to the nurse because the nurse was seen as a surrogate significant other who deserved to be told the “truth.” Here, there was a sense among participants that the nurse performed a quasi-disciplinary role and prompted positive behavior change because “. . . somebody was relying on me to do it” and because “. . .I was doing it for somebody else rather than just me.”
Outside the context of the health coaching calls, participants used pedometers and diaries to enable them to either maintain or increase activity levels. For participants who regularly achieved the widely recommended 10,000 steps a day, the function of pedometers and diaries was analogous to the health coach as they positively reinforced their efforts to change their behavior: . . . because I was doing well at the time, most days I was getting up to 10,000 steps a day on the pedometer, so I was . . . and I kept a record of it, which I don’t think I’ve got now, but yes, it was getting a little smiley face on it. So I was quite pleased.
Whereas for others, pedometers exerted a sense of disciplinary control over their efforts to be more active and determined by pushing them to do extra activity as illustrated by this male participant in his early 60s: . . . By six o’clock at night I’d done 6,593, so I went out and I did a walk at six o’clock and I knocked it up to 10,000. Yeah, at the end of the day it was 11,000. So I had to set out from under seven, and did another 4,000 steps purposely.
This was true even if the prospect of achieving 10,000 steps was remote, for example, because of bad weather or fatigue. Here, self-monitoring activity with pedometers pushed participants to attain a level of activity that approximated target levels and gave them a sense of achievement even in the face of obstacles: It’s easy to pack up and say I’ve had enough now, but if you’ve got that [the pedometer], you look at it and you say, oh, I’ll do another 1000 . . . I’d go . . . while I’d got the weather, if it started to pour with rain I would stop. I’d regularly get around 7000, if I didn’t make the ten.
Maintenance—Embedding Behavior Change in Everyday Settings
In line with the accounts from the previous section, data are presented here thematically rather than within participants. By using data that were common across participants, we explain links between initiation and maintenance of behavior change.
Participants who had remained active cited how they had continued to remodel the way they interacted with their local environment to take advantage of opportunities to walk more: Oh, she [health coach] thought “park in the farthest place in the car park and walk if the weather is good.” I still do things like that. Constantly, I’ll park in the farthest place in the car park and then walk.
The weather was seen as critical to the success of implementing such a strategy. In the presence of bad weather, health coaches had encouraged participants to remain active by walking indoors, such as in covered shopping centers. However, as described below, for participants living in rural areas without a car or public transport, staying active by driving to local shopping centers was not a feasible solution to staying active in bad weather: There are people living up here and people living far away from places who don’t have a car. I mean we don’t have a bus up here, so you know, it’s quite difficult for people like that, it wouldn’t work for them.
Dog walking also remained a key resource for participants to stay active, especially among those who, amid the daily toil of caring for themselves, found it difficult to engage in additional physical activity: . . . I mean you’re supposed to pace yourself but I found that to me not a good idea, because the way you live, as I’m on my own, it was difficult to pace yourself because you’re living in a life where things have to be done, unless you’re a very wealthy person. So I decided then I would get my dog and it would have to go out and it would give me that push.
Whereas the external environment was an important factor for facilitating the maintenance of activity among many participants, others drew on an internally derived sense of self-determination to stay active. This trait was often expressed by female participants in the context of seeing the health benefits of staying active and being able to support their children: She’s got three flights of stairs, my daughter, and I go and help her and clean-up for her when they’ve gone to work and things like that, keep the house tidy for her. So that’s one of the things that made me realize I had a battle. By the time I’d climbed one floor I was like oh gosh, I feel tight in my chest. But now [after the intervention] I can go up and down, go from the cellar up to the attic, up three floors and down again without feeling breathless.
Internal drivers to stay active were also evident among participants who continued to use a diary or a pedometer long after the intervention period was over. Although these resources were often characterized as props or prompts that reminded participants to remain active, they were used in the context of a broader commitment to self-improvement: I’ve found it quite useful. I’ve found it a good idea. I think that is the thing that you do it for yourself, you’re not doing it to hand into somebody to check that you’ve done alright. It’s the fact that you can look at it and see how you are doing.
It was however recognized that some participants who had maintained their newly active lifestyles pushed back against using pedometers after completing the intervention, even if they recognized the merit of self-monitoring: I continued with it for a while and then stopped because a bit like the Fitbit, you get fed up with having to look at figures all the time. I know it’s a good philosophy. I react against it in the end.
Resistance to self-monitoring was twinned with the emergence of a more relaxed attitude to not achieving recommended weekly targets. Participants were minded to calibrate their daily activity to what they felt could be achieved. Abandoning rigid targets was seen as liberating and freed participants to carry on doing what they had done before without fear of failure. This approach was typified by this female participant who recognized that trying to over achieve was an unhelpful attitude to hold onto when trying to stay active: Once I stopped this sort of thinking oh I must get there, I must get there, then I realized that I do quite a lot of walking anyway, so it was easier to keep it at a reasonable level.
That participants had developed a keen sense of the importance of being at least moderately active was particularly apparent among those who encountered illness or injury during the course of the trial. After suffering from a virus and without the availability of health coaching, this participant felt less motivated and capable of maintaining previous activity levels: . . . I’ve deteriorated a bit and trying to get the enthusiasm to go for a mile walk now is . . . I probably could do it, it’s just it’s one of those things, well it’s one of the things that this condition is renowned for, you know, get the exercise but it’s hard work doing the exercise.
Equally, even participants who were physically capable and motivated to maintain higher levels of activity sometimes had less capacity to do so, especially in the context of competing demands to participate fully in family life. However, in these instances where participants were geographically and socially stretched, there was an appreciation that while they may have stopped logging steps, they were able to remain relatively active in ways that fitted their particular lifeworld: . . . I’m not doing what I was doing before. But then I’ve been doing a lot of running around, because I’ve been helping [Daughter] out and helping my son out, because he’s split up with his partner, so I’ve been going and getting him his shopping on a Friday and filling his fridge, and then popping round and giving it a bit of a once over clean.
Discussion
Using this longitudinal qualitative study, we showed that people with mild COPD perceived telephone health coaching as a means to distance themselves from negative experiences of being diagnosed with COPD and to develop motivational attitudes commensurate with avoiding further functional decline and maintaining independence, potentially leading to greater personal control over their illness. Translation of these motivational attitudes into action was mainly achieved by participants either electing to continue being physically active or by building on existing physical activity; most participants were ex-smokers and, as such, did not need to engage in smoking cessation advice and there was also little evidence of engagement in behavior change to support inhaler technique and medication adherence and action planning. Mechanisms to change included taking advantage of environmental affordances, including dog walking. Other salient mechanisms included doing activity to attract positive affirmation from the study nurse and significant others, and using pedometers and diaries to bolster commitments to pursue activity goals. Behavior change was most likely to be maintained where changes were embedded in and fitted with the routines and settings of participants’ everyday lifeworlds. This was especially challenging in the face of illness, injury, or competing demands on time from social groups such as family. It was also acknowledged that resources to sustain physical activity were not evenly distributed, for example, between rural and urban areas, making it difficult for some participants to make use of environmental affordances.
Interpretation of Findings
The PSM-COPD trial aimed to identify a cost-effective intervention for people with mild dyspnea in the context of increased screening and case finding for COPD in primary care. The trial did not show benefits for HRQoL, dyspnea, quit behavior for smoking, self-efficacy, or confidence in using antibiotic or steroid rescue packs; participants who received health coaching were more active at 6 months, but this effect waned and was not significant at 12 months. Similarly, in Australia, Walters et al. (2013) showed that a telephone mentoring intervention that used negotiated goal setting for people with moderate to severe COPD improved participants capacity to self-manage by being more active, but did not improve HRQoL or symptoms (Walters et al., 2013). Qualitative evaluation of this Australian trial showed that mentoring increased awareness of COPD and supported participants to develop and personalize behavior change strategies. However, because the qualitative findings were published prior to the trial findings, the analysis does not explicitly address why the mentoring intervention did not improve HRQoL.
In PSM-COPD, it is possible that the failure of the intervention to achieve its primary aim can be partly explained by a disconnect between the implementation of the health coaching model and its partial adoption by participants. Although theoretically coherent and plausible, social cognition theories upon which health coaching interventions draw on are based on normative assumptions about humans as rational actors, motivated and capable of behavior change through goal-oriented and problem-solving strategies (Sanders & Rogers, 2011). By contrast, sociological work in chronic illness has highlighted the complexity and plurality of responses to chronic illness and shown that these responses are rooted in patients’ historical and existing coping strategies and should also take into account their prior experiences and contact with health services (Gately, Rogers, & Sanders, 2007; Taylor & Bury, 2007). Far from operating at a purely instrumental and rational level, we similarly found that participants displayed a variety of motivations for engaging with opportunities to self-manage that were articulated in the context of recursive and ambiguous relationships between their encounters with primary care, their diagnosis, and their everyday lifeworlds. Indeed, bar smoking cessation, being given a formal diagnosis of COPD prior to the intervention, had not previously prompted participants to fully enact self-management practices expected of them, further highlighting the tension between the aims and outcomes of pay-for-performance case finding policies in primary care (Daker-White et al., 2015). In the context of the PSM-COPD trial, participants’ historically ambivalent attitudes toward self-management continued, with the exception that telephone health coaching played a role in supporting participants to make some positive changes to self-management behaviors.
Motivations to change behavior to be physically active were especially apparent where the availability of environmental affordances intersected with participants’ desire to stay or be more active. Here, we endorse the notion that environmental affordances are not just action possibilities latent in objects in the environment, but are perceived by individuals in relation to their attributes and characteristics, which are dynamic and change over time and space (Clark & Uzzell, 2002). In PSM-COPD, participants’ needs and intentions in relation to environmental affordances were expressed in the different ways they remodeled their interactions with their environment to be physically active, for example, by taking stairs not escalators, or parking further way from shops. Dogs were also perceived as action possibilities whereby participants co-opted their pets in opportunities to be physically active. This extends the idea that animals can be critical components in how people achieve practical elements of illness work associated with living with a long-term condition (Brooks et al., 2013).
Goal setting was largely unpopular among participants. There is an emerging understanding that interactional styles of health professionals can play an important role in setting the parameters of goal setting with the use of less directive language and more flexible and less biomedical approaches being more effective (Franklin et al., 2018). In our study, the extent to which health coaches were instrumental in eliciting participants needs and preferences to be active and supporting them to be active can be explained in relation to a push–pull system used in supply chain management. Push–pull describes the movement of a product or information between the distributor and the consumer; distributors typically push the product downstream to the consumer who can sometimes demand more by pulling. The interface between these two subjects is known as the push–pull boundary (Harrison, Lee, & Neale, 2003). In PSM-COPD, the goods to be moved were information and motivational strategies and participants sometimes relied on these being pushed by the health coach to encourage them to be active, whereas other participants pulled themselves along to enact self-management behaviors. Pedometers and diaries were usefully deployed by participants to help move the push–pull boundary closer to themselves allowing them to calibrate the extent to which they felt inclined to be pushed by coaches to be active, or were capable of pulling themselves along to be active. Of note here was the sense that while goal setting was resisted, pedometers were embraced as a means to navigate this push–pull boundary. Pedometers and tracking devices are ubiquitous features of what might be best understood as the quantified self (Lupton, 2016). Their prominent use by participants in this study can be in part explained in relation to Foucault’s notion of biopower, which speaks to how the way people manage their bodies on a daily basis is intertwined with monitoring and promoting the health and well-being of populations (Foucault, 1990; Lupton, 2016). Self-management in this context could be construed as a means to exert bodily discipline and control in ways that are socially and morally prescribed and there were allusions to this ontological proposition in our findings about monitoring physical activity. Equally, this proposition resonates with evidence from qualitative meta-ethnography that among the most valued activities of daily living among people with COPD are ones that offer opportunities to exert a sense of control and to effectively manage the way they care for themselves (Lindenmeyer, Greenfield, Greenfield, & Jolly, 2017).
Maintenance strategies were most successful when participants adapted activity goals set during the intervention period to fit with their existing capabilities and took in account the availability of environmental affordances, including dogs. Pedometers provided participants with the tools to ascertain whether they were being sufficiently active and judgments were often made independent of any normative assumptions about what makes a “good self-manager” (Ellis et al., 2017). For some, this meant being satisfied with achieving activity levels that were less than recommended targets, reflecting that the experience of living with a long-term condition involves balancing illness self-management with social roles and commitments (Vassilev, Rogers, Kennedy, & Koetsenruijter, 2014). Here, it is perhaps also possible that the limits of individual agency were exposed where participants’ social contexts made it difficult to maintain behavior change. In these senses, it is possible that activity levels waned at 12 months because participants adopted self-management practices that were less goal-oriented and instead were sufficiently flexible to meet their needs and capabilities and fitted with their particular contexts, an attitude to self-management that has proven to have some salience among people with diabetes (Gomersall, Madill, & Summers, 2011).
Strengths and Limitations
By conducting two interviews 6 months apart, we were able to capture data that explored the impact of the intervention on self-management practices over a longer time period, thereby giving participants an opportunity to discuss how behavior change was maintained. Analysis was undertaken concurrently with interviews and this enabled researchers to build into the follow-up interviews at 6 months tailored prompts that focused on eliciting information about what enabled or impeded behavior change over time. In this sense, the follow-up interviews were partly driven by empirical findings from the first interviews and facilitated interpretation of how self-management trajectories were shaped by prior and ongoing experiences of living with COPD in the context of participants’ lifeworld. Giving participants an opportunity to discuss their experiences of self-management twice over 6 months may also have minimized the impact of recall bias, although we cannot rule out the possibility that findings were affected by this bias. In addition, by conducting this qualitative study in a trial, we were able to use the qualitative analysis to determine whether participants’ experience of the intervention mapped to the results of the main trial evaluation. Separation of the analysis of qualitative from quantitative outcome data allows for less biased interpretations of participant experience of interventions (Oakley et al., 2006). By ensuring that the qualitative data were analyzed before trial outcomes were known, the findings in this study are likely to offer less biased interpretations about the merit of telephone health coaching for people with mild COPD. However, we acknowledge that because the interviewers were not blinded to allocation or the trial hypothesis, there is a chance that the ontological assumptions and prior knowledge of the interviewers affected the validity of the findings. But we would also highlight that by maintaining analytical separation between the qualitative and quantitative findings facilitated inductive analysis of data giving rise to the concept of a push–pull boundary as a heuristic device to point up the significance, use, and place of health coaching in the lifeworlds of participants. Although, in some respects, this concept is adjacent to internal and external locus of control, we opted to use the concept of a push–pull mechanism as an analytical lens because it featured in the data and in this sense it resembles a first-order construct not shorn of contextual meaning. However, because trial populations tend to be highly selected groups with characteristics not always shared by the general population, we cannot be confident that the findings presented here generalize to all people with mild COPD in contact with telephone health coaching interventions. On a different methodological note, we recognize that the comparative utility of this study was potentially reduced by interviewing fewer participants in the control group and limiting these interviews to the 6-month time period. In this sense, opportunities to compare, like-for-like, experiences among participants in the intervention and control group were reduced. However, because the primary objective of this qualitative study was to explore the experiences and perceptions of participants exposed to the intervention, the control data were used in a way that is analogous to deviant case analysis, whereby disconfirming evidence helped to confirm emerging themes from the interviews in the intervention group. By undertaking a limited number of interviews in the control group, we were able to more readily identify what impact the intervention had on participants and thereby develop more solid themes about how behavior change was enacted among participants in the intervention group. Finally, because we analyzed and presented data from the 6- and 12-month interviews thematically using framework, we were not able to identify and articulate how self-management behaviors may have been maintained on a case-by-case basis, limiting the value of the longitudinal design. It is possible that the use of narrative forms of qualitative analysis would have been more sensitive to capturing changes and critical moments pertinent to individual accounts compared with thematic analysis, which can tend to emphasize the reporting of cross-sectional data at each time point (Calman et al., 2013).
Implications for Self-Management Policy and Research
Deploying population-level interventions such as telephone health coaching following case finding for mild COPD is unlikely to be a successful way to promote wholesale adoption of self-management practices, especially those associated with symptom management. Whole system interventions that seek to embed self-management of long-term conditions in the day-to-day activities of practitioners through provider training and facilitation have not added value to the existing care of people with long-term conditions (Kennedy et al., 2013), and are also possibly ill-suited to supporting implementation of risk-mitigating strategies that can delay disease progression in people with mild COPD. By contrast, telephone-guided access to community-based assets and interventions has proven to be a novel way to improve HRQoL and self-management behaviors in people with chronic kidney disease (Blakeman et al., 2014) and this approach, along with social prescribing, might hold promise for supporting self-management in people with mildly symptomatic long-term conditions. There is also scope to better understand how health coaching models might be adapted to support people with milder disease to be physically active. Self-management interventions for people with chronic disease are known to benefit service users where they build in opportunities to offer support in a holistic and flexible fashion (Stenberg & Furness, 2017). Key here is the need to personalize coaching so as to make it meaningful and responsive to the everyday experiences and psychosocial needs of people living with a long-term condition such as COPD (Russell et al., 2018). One possible option is to develop and test ways to move the push–pull boundary closer to the individual so health coaches and patients alike can work in more dynamic and less static ways to develop and implement more personalized self-management goals. Digital solutions that include web dashboards that allow patients to communicate with health coaches or other health professionals and log their activity, for example, by using electronic diaries, may be ways to implement more flexible and data-responsive self-management interventions for people with mild and presymptomatic disease (Coventry et al., 2016; Patel, Jones, Adamson, Spiteri, & Kinmond, 2016).
Conclusion
This longitudinal qualitative study showed that people with mild COPD only partially engaged with a telephone health coaching intervention that aimed to promote self-management. Participants were less inclined to focus on behaviors associated with managing respiratory symptoms but they did respond positively to opportunities to adopt active lifestyles, especially in the presence of environmental affordances, including pet dogs. Pedometers and activity diaries also helped shape the extent to which they needed to be pushed or could pull themselves along to be active. There was considerable variation in the ability of participants to maintain active lifestyles reflecting that self-management of long-term conditions is played out in the context of people’s routines and everyday lifeworlds. It remains a challenge to develop interventions that can flexibly support people with long-term conditions with mildly symptomatic disease to self-manage.
Supplemental Material
Supplementary_file_2 – Supplemental material for The Push and Pull of Self-Managing Mild COPD: An Evaluation of Participant Experiences of a Nurse-Led Telephone Health Coaching Intervention
Supplemental material, Supplementary_file_2 for The Push and Pull of Self-Managing Mild COPD: An Evaluation of Participant Experiences of a Nurse-Led Telephone Health Coaching Intervention by Peter A. Coventry, Amy Blakemore, Elizabeth Baker, Manbinder Sidhu, David Fitzmaurice and Kate Jolly in Qualitative Health Research
Supplemental Material
Supplementary_material_1_control_topic_guide – Supplemental material for The Push and Pull of Self-Managing Mild COPD: An Evaluation of Participant Experiences of a Nurse-Led Telephone Health Coaching Intervention
Supplemental material, Supplementary_material_1_control_topic_guide for The Push and Pull of Self-Managing Mild COPD: An Evaluation of Participant Experiences of a Nurse-Led Telephone Health Coaching Intervention by Peter A. Coventry, Amy Blakemore, Elizabeth Baker, Manbinder Sidhu, David Fitzmaurice and Kate Jolly in Qualitative Health Research
Footnotes
Acknowledgements
We would like to credit all membrs of the Patient Self-Management for COPD (PSM-COPD) collaborative group for supporting this qualitative study: Peymane Adab, Khaled Ahmed, Elizabeth Baker, Amy Blakemore, Peter A. Coventry, Amanda Daley, Lee Dowson, David Fitzmaurice, Carl Heneghan, Catherine A. Hewitt, Natalie Ives, Kate Jolly (Chief Investigator), Rachel Jordan, Sue Jowett, Tosin Lambe, David Nunan, Manbinder S. Sidhu, Sally Singh, and Jinu Varghese.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article summarizes independent research funded by the National Institute for Health Research (NIHR) School for Primary Care Research and the NIHR Collaborations for Leadership in Applied Health Research and Care (CLAHRC) West Midlands. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health and Social Care.
Notes
Supplemental Material
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.