
Abstract
Physical activity (PA) can help manage cancer treatment-related side effects and improve well-being following treatment; however, resuming PA after a period of inactivity due to cancer can be challenging. The purpose of this study was to explore adolescents and young adults (AYAs) experiences transitioning back into PA after a period of inactivity due to cancer treatment. Twelve previously active AYAs (Mage = 30 ± 5.8 years) were purposefully sampled and engaged in a semi-structured interview. The following four themes were generated through a reflexive thematic analysis: PA is described as important and valuable; navigating one’s appearance and fitness changes after cancer treatment within the PA context; supportive care is essential to successful PA transitions; and juxtaposed environments: fitness facilities, cities, and green spaces. Developing strategies aimed at gradually transitioning into PA should be a priority to improve AYAs’ well-being through survivorship.
Introduction
Adolescents and young adults (AYAs) diagnosed with cancer are defined as those who receive a cancer diagnosis between the ages of 15 and 39 years (Canadian Partnership Against Cancer, 2017). Physical activity (PA) is valuable during the survivorship trajectory wherein re-engaging in activity after treatment can be key to managing side effects, improving quality of life, and reducing recurrence and mortality risk (Adams et al., 2018; Bélanger et al., 2011; Brunet et al., 2018; Cormie et al., 2017; Murnane et al., 2019; Pugh et al., 2020). However, AYAs describe difficulties navigating the transition from a more sedentary lifestyle during cancer treatment to an active lifestyle after treatment (Wu et al., 2015), with approximately half of AYAs being insufficiently active after treatment (Adams et al., 2021; Barnett et al., 2016; Bélanger et al., 2011; Murnane et al., 2015). It is therefore important to understand AYAs’ PA experiences post-treatment to help increase PA re-engagement.
Since AYAs are in a life-stage where appearance is highly valued and social relationships are developing (Abrams et al., 2007; Epelman, 2013), body image and social support may be two especially important factors that impact this transition. Of particular interest, reported barriers to PA re-engagement after treatment among AYAs include body appearance and function changes and perceptions of low social support for PA (Brunet et al., 2013; Larouche& Chin-Peuckert, 2006; Pugh et al., 2018; Smith-Turchyn et al., 2020; Wu et al., 2015). Meanwhile, high perception of social support is cited as facilitating AYAs’ PA participation (Pugh et al., 2018; Rosenberg et al., 2014; Wu et al., 2015). Previous studies have used a quantitative design (Brunet et al., 2013; Rosenberg et al., 2014), did not have a sole focus on PA (Larouche& Chin-Peuckert, 2006; Pugh et al., 2018; Wu et al., 2015), and did not explore body image and social support in detail (Pugh et al., 2018; Smith-Turchyn et al., 2020), limiting an in-depth understanding of how body image and social support influence PA re-engagement among AYAs. Given the complexity of the decision to re-engage in activity, a qualitative methodology may foster exploration of the nuances of the PA transition and better elucidate the role of body image and social support within AYAs’ re-engagement efforts (Pearce, 2009).
Initiating PA after cancer treatment may be different between those who were previously active compared to those who were not. Previously active AYAs likely had an established exercise routine, may have differing expectations or goals for re-engagement, and may find treatment-related changes to their physical functioning especially troubling. In fact, one study qualitatively explored the effects of an exercise program during treatment using interviews with young adults who described themselves as pre-cancer athletes (Adamsen et al., 2009). Findings demonstrated that pre-cancer athletes had distinct challenges with identity and body appearance and function changes that were improved by participating in the exercise program. However, less is known about the post-treatment experiences of AYAs who are navigating re-engagement into PA in the absence of a structured exercise program. To our knowledge, researchers have not explored how AYAs who were meeting activity guidelines (i.e., 90 minutes of moderate-to-vigorous PA per week; Campbell et al., 2019) prior to treatment navigate the transition of re-engagement in PA post-treatment.
This qualitative interview study aimed to advance the existing literature by focusing on a subset of the AYA population who were active prior to their cancer diagnosis and to explore their PA transition experiences during the post-treatment trajectory. The primary research questions of this study were: (a) what are the experiences of previously active AYAs in their transition back into PA following cancer treatment?; and (b) do body image and social support play a role within the transition period? Understanding the experiences of this unique group of cancer survivors can provide valuable insight into the range of experiences that can influence the initiation and maintenance of PA after treatment.
Methods
Philosophical Position
A constructivist paradigmatic position was adopted, suggesting that AYAs each hold subjective perceptions of their experiences. We therefore focus on understanding the meanings that AYAs have created and attributed to their experiences (Guba & Lincoln, 1994; Lincoln et al., 2011). Aligned with constructivism, a relativist ontological position was held wherein we assumed that multiple realities exist, which are shaped by an individual’s interpretation of their experiences within various social contexts (Lincoln et al., 2011). Further, ascribing to a subjectivist and transactional epistemology, we assumed that knowledge is created through researcher-participant transactions and understood that our own realities, views, and experiences cannot be detached from the research process (Lincoln et al., 2011; Tamminen & Poucher, 2020). The researcher interacts with the participant in an attempt to understand their experiences from their point of view, lending to a co-construction of meaning (Davidsen, 2013).
Consistent with constructivism, qualitative description was used as the strategy of inquiry and semi-structured interviews as the data generation tool to describe and interpret previously active AYAs’ subjective experiences transitioning back into PA after treatment (Sandelowski, 2000). Qualitative description is well suited to address this research question as this approach can be used to provide a focused and rich description of AYAs’ perceptions and experiences of a particular phenomenon, the post-treatment PA transition. Furthermore, given the clinical and practical relevance of this topic, qualitative description is fitting to inform practice and intervention development (Neergaard et al., 2009).
Participants
Ethics approval from the appropriate university research ethics board committee (#39245) was obtained. To recruit AYAs, we contacted general and AYA-focused organizations and survivorship programs across Canada via email. Supporting organizations distributed study information to AYAs using email and/or social media. We also shared the recruitment poster on our social media accounts. Interested participants who contacted the research team via email were provided with a screening questionnaire and a digital copy of informed consent. Eligibility criteria included: (a) a diagnosis of cancer between the ages of 15–39 years regardless of cancer type, stage, time since diagnosis, and treatments received, (b) ability to understand and speak English, (c) self-reported engagement in approximately 90 minutes of moderate-to-vigorous PA per week before cancer treatment, and (d) access to a computer and internet.
Data Collection
All eligible participants were above 18 years of age, provided digital written consent, and were scheduled for an interview and sent a self-report questionnaire. The brief pre-interview self-report questionnaire was used to collect information about the AYAs’ demographics (e.g., age, relationship status), medical information (e.g., cancer type, treatments received), and PA information. The interviewer 1 reflected upon their positioning throughout the data collection and analysis phases. Virtual interviews (using Zoom) were conducted to abide by COVID-19 restrictions. Participants had the option of turning their video on. Interviews were conducted between September 1 and October 30, 2020.
Interviews were semi-structured and AYAs were first asked general questions about their PA history (e.g., “Can you describe your PA behavior during treatment for cancer?”). The PA transition period was defined for participants as any time following treatment when AYAs tried to or resumed activity. Next, the main questions explored (i) experiences transitioning back into PA (e.g., “What, if anything, made it easy [difficult] for you to transition back into PA?”), (ii) body-related experiences during their transition (e.g., “How did your body’s function, if at all, influence your PA transition?”), and (iii) support from others during their transition (e.g., “Tell me about the support you received from others during this PA transition”). Finally, AYAs were also asked questions related to their opinions regarding the PA transition for cancer survivors in general (e.g., “Based on your experiences, do you have any recommendations for smoothing this transition back into PA after cancer treatment?”). The interview guide was pilot tested with one AYA for relevance, clarity, length, and comprehension. Revisions were not made to the interview guide based on the pilot interview and this interview was not included in the analysis.
The semi-structured flexible interview guide (Supplemental file 1) provided researchers the opportunity to better understand the experiences of AYAs, while also allowing the responses of AYAs to shape the interview. Elaboration on participant’s accounts was encouraged using prompts (e.g., “How did that limit your willingness to be active?”; “Could you share an example of. . .?”). Interviews were audio-recorded and transcribed verbatim and then reviewed for accuracy. Immediately following the interview, the interviewer wrote notes on their thoughts and impressions to stimulate further consideration and organization of the interview data (Hermanowicz, 2002). Journaling was also used for self-reflexivity to challenge preconceived assumptions and acknowledge how their personal interpretations or characteristics may have affected the co-construction of meaning during the interview (Finlay & Gough, 2003; Rae & Green, 2016). Participants were provided with compensation in the form of a $20 CAD gift card. Although the number of participants was limited, following guidelines of information power (Malterud et al., 2016), our sample was deemed sufficient. Aspects relating to high information power include a narrow study aim, specific sampling of participants (i.e., previously active AYAs), and strong interview dialogue.
Data Analysis
A reflexive inductive thematic analysis was used to analyze the interview data, allowing for a flexible, iterative, and exploratory approach (Braun & Clarke, 2006, 2013, 2019). This approach is compatible with a constructivist paradigm and qualitative description, wherein AYAs’ PA transition experiences are described in detail, staying close to the data, yet also providing low-inference interpretations (Sandelowski, 2000, 2010). The analysis followed the six phases outlined by Braun and Clarke (2006). Following transcription, the interviewer read and re-read each transcript and listened to the associated audio recording to become fully immersed in the interview and atmosphere. This process facilitated a deeper familiarization of the meaning co-created in each interview. The interviewer noted their preliminary reflections and interpretations that were close to the data. Next, the transcripts were reviewed and initial codes (latent and semantic) were generated by identifying interesting bits of data and repeated patterns. As novel codes were generated, prior transcripts were reviewed and the list of codes was reorganized. NVivo 12 software was used to aid in the coding process (QSR International Pty Ltd, 2018).
Following the generation of a comprehensive set of initial codes, similar meaning units were clustered to generate themes and subthemes. Each theme was then reviewed in conjunction with the transcripts and codes to ensure that the generated themes provided a detailed and rich understanding of AYAs’ experiences and addressed the research questions. Specifically, each theme in conjunction with its associated codes and the transcripts were reviewed for consistency within themes and for uniqueness across themes (Braun & Clarke, 2006, 2013). A “critical friend” who was distanced from the interview process then reviewed the first author’s themes and interpretations (Smith & McGannon, 2018). The “critical friend” provided feedback and alternate interpretations, which were discussed among the pair. Based on the discussions, themes were re-ordered and refined yielding a final set of themes and subthemes, which were named and defined. The themes were richly described using everyday language and illustrative quotes.
Methodological Rigor
Aligned with a relativist approach, quality criteria (e.g., contribution of the work and rigor) were applied throughout the research process (Smith & McGannon, 2018; Sparkes & Smith, 2014). First, the interviewer displayed quiet concern and used probes during the interviews to encourage the opportunity for AYAs to provide detailed accounts of their experiences (Sparkes & Smith, 2009). Further, we engaged in reflexivity throughout the research process through self-reflections and discussions with a critical friend (Smith & McGannon, 2018). This encouraged her to recognize and challenge her preconceptions so as to not limit her interpretations of AYAs’ experiences and the meanings they ascribe to them (Sparkes & Smith, 2014). Finally, detailed descriptions of the themes and direct quotes from the transcripts were used for a rich and transparent illustration of the data (Smith & Sparkes, 2016).
Results
Demographics for the 12 AYAs are presented in Table S1 (Supplemental file 2). AYAs were diagnosed with a range of cancer types (n = 8), with the most common diagnosis of Hodgkin’s lymphoma (n = 4). The participants’ self-identified gender was woman (n = 7) or man (n = 5). At the time of the interview, AYAs ranged from 20–39 years, and time since treatment ranged from 2 months to 9 years. The interviews lasted 41–95 minutes in length (M = 55.96 minutes). Seven interviews were conducted with audio-only.
AYAs discussed a variety of experiences related to their post-treatment PA transition. Four themes were generated that demonstrate AYAs’ experiences navigating this transition: (a) PA is described as important and valuable, (b) navigating one’s appearance and fitness changes after cancer treatment within the PA context, (c) supportive care is essential to successful PA transitions, and (d) juxtaposed environments: fitness facilities, cities, and green spaces. The themes are presented in detail with illustrative quotes. Table S2 provides an overview of the themes, subthemes, and relevant quotes (Supplemental file 3).
PA is described as important and valuable
PA was described as essential for previously active AYAs, as exemplified through two subthemes: Comparisons to previous abilities challenge one’s active identity and The use of PA to regain control and feel “normal.”
Comparisons to previous abilities challenge one’s active identity
Most AYAs highlighted the value of PA through comparisons of their physical abilities pre- and post-cancer diagnosis. Prior to diagnosis, AYAs reported engaging in a variety of PA types (e.g., rowing, running, tennis, soccer) and levels of competitiveness (i.e., national sport teams to recreational). Many AYAs felt that being active and athletic was part of their pre-cancer identity. One AYA contemplated their athletic identity during treatment: . . .I was talking to someone, like professionally. . .and we were kind of on the topic of if it was my last day, to live what would I do. And I realized I would still work out on my last day. That was sort of the joke—because it feels good. . .thinking about that too it's just reinforced like active lifestyle, it's part of my identity.
After treatment, however, AYAs’ body changes and the associated reduction in abilities challenged their active identity. Since PA was integrated into AYAs’ previously active life, many AYAs described some degree of identity loss or change.
Being active after treatment was used to feel closer to their former sense of self. However, AYAs compared their current physical function abilities to their pre-cancer abilities, where they made upward comparisons that emphasized their reduced capabilities in terms of how intensely and how long they were able to be active. For one AYA, who was a former competitive kayaker that trained for an average of 20 hours a week prior to her diagnosis, shared: I struggled a lot with it and I think mainly because since I was so active prior to being diagnosed and then went the complete opposite direction to not doing anything at all—I found the motivation really difficult and the fact that I couldn’t just go out and do like a 6km run easily was very discouraging. So I think it’s that, it’s like ‘well I know I’m capable of doing this and I used to be able to do this quite easily and now I can’t’…
These feelings of discouragement and demotivation were intensified because of her expectations for post-treatment PA, “I think I expected to just hop right back into things and pretend life was OK again [laughs].”
The comparisons, in conjunction with PA expectations and a need to reconcile one’s identity, impacted AYAs’ motivation. As one AYA describes: . . .I felt more motivated to kind of get back to my high school self, where I actually had strength, I felt more proud of my body. And so, coming out of chemo, I wanted that again. And I had realized how weak I had become from chemo. So that was a big motivator to try to get my strength back.
However, when AYAs engaged in activity, their physical shortcomings resulting from cancer became more apparent, which triggered lower motivation for some of them. The contrast in physical abilities pre- and post-cancer treatment was portrayed by the same AYA, who further shared, “. . .it was hard when I went to the gym at first, because I didn’t have any strength left. I was doing such a little amount of weights [. . .] So, it was a little unmotivating seeing how weak I had become.” For most AYAs, making these upward comparisons to their previous abilities challenged their active identity and therefore, resulted in lower PA motivation. Alternatively, one participant’s motivation was rooted in the pressure to surpass their previous strength given his belief that he was a better version of his previous self: “. . .I have this whole kind of idea that I'm stronger because of this and like I'm a better person and a different person. So, for me personally I would like to surpass where I once was.”
Although rare, a couple of AYAs who were further out from treatment reflected on the progress they made in changing their expectations and reconciling their athletic identity issues. For one AYA, a diagnosis of cancer was what caused retirement from her sport 7 years ago and it took her awhile to come to terms with her new way of being active: I think not as much to keep up with what I used to be able to do. But um - just to have a routine and have that lifestyle where I do exercise regularly and feel good since it does, it can affect so many other aspects of life. But I don’t have to go, I don’t have to train like an athlete anymore and I know that now. [. . .] I think it took a year or so before I clued into that [pause] later after treatment.
The shift in PA expectations helped AYAs have a more adaptable relationship with PA as comparisons were made less often and they formed a new personal definition of active identity.
The use of PA to regain control and feel “normal”
A diagnosis of cancer and cancer treatment prompted AYAs to feel a loss of control and a drastic change in routine. The importance of PA was highlighted by participants’ reports of using PA as a means of resuming normality, creating routine, and regaining control. For example, one AYA described why she felt engaging in PA immediately after treatment was crucial, “…I think that physical activity is really important, like ongoingly and so, in the stages right after treatment, then you can start to build like a bit of a pattern for yourself, so that it stays a priority.” Creating a routine through PA was a main way that participants regained control and felt closer to normal: I would say [PA]’s fairly important [. . .] It’s a good way to feel good about yourself and also to feel like you’re moving on more in life. Because you can finish treatment and then still take time off, but you will still feel like you’re stuck in time, like when you were going through treatment. [. . .] It makes you feel good, because you’re working towards something. It may be small, but it’s something [emphasis]. And it’s one great way to help you feel like you’re moving on in life finally, after being stuck in time for so long.
Some AYAs described the importance of engaging in PA to help them move on and engage in meaningful activities that made them feel good after treatment. This was especially important for AYAs who were taking time off work or school as PA provided structure to their days and gave them purpose. Another AYA felt that having a PA routine facilitated a bridge to his prior routine: But I think in terms of getting back to any sense of normalcy, that was the most important thing. [. . .] And feeling ready to take on a day and being able to get up at a normal hour, not sleeping 11 hours a day. [. . .] Those all come hand in hand with the activity. [. . .] You’ve got to get back with how the rest of the world is living. And that was the one thing I think it helped me get back to that routine.
Notably, in contrast to some AYAs’ language use of “moving on,” this participant gave voice to the AYAs who felt that being active was a signal of hope indicating they were getting “back to normal” or back to “life as it was before.” Being able to engage in the same physical activities that were enjoyed prior to diagnosis and treatment was also described by AYAs as a way to feel “normal again.”
The need to regain control and normalcy was also exemplified when discussing mental health, as AYAs described using PA post-treatment to ease their mental health concerns. For instance, one AYA shared, “. . .for me, if I'm starting to feel really anxious I just know I have to go for a walk [. . .] it's my number one quick fix.” Later in the interview, this AYA went on to discuss the use of PA for managing fear of recurrence, “You can kind of forget about your troubles and try and not be afraid that it’s going to come back, you know, try and forget about those fears. . .” For these AYAs, mental health concerns (e.g., anxiety) were heightened after treatment and were not considered normal for their previous selves. And so, PA was used to manage their symptoms and feel closer to their “normal.”
Other AYAs underscored the importance of PA when they shared how they used PA to prevent the severity/occurrence of acute and late physical effects, recurrence, and secondary cancer. For instance, one AYA shared: . . .the goal is to do 30 minutes of [aerobic PA] so I can get blood flow going to my brain. [. . .] since my memory was taking a hit during the chemo I thought this would be the perfect opportunity for me to exploit this.
Meanwhile, other AYAs expressed that they exercised in an attempt to avoid future sickness and take back control of their health. Taken together, AYAs disclosed that PA was a strategy they used to control or manage their routines and mental and physical health, and PA contributed to feeling like they were resuming normality.
Navigating one’s Appearance and Fitness Changes after Cancer Treatment within the PA Context
AYAs experienced body appearance (e.g., scars, hair loss, body part removal, stretch marks), physical function (e.g., muscle atrophy, fatigue, pain), and weight (i.e., weight loss, gain, cycling) changes resultant from cancer and associated treatments. Overwhelmingly, AYAs described feeling unrecognizable, displeased, and disconnected from how they thought their body should look and feel, which impacted their PA experiences and behavior. Within this main theme, two subthemes were generated: Body appearance and function changes impacted PA behavior and experiences and Using physical activity as a means to change one’s body.
Body appearance and function changes impacted PA behavior and experiences
Changes to AYAs’ appearance and physical function impacted their ability and/or willingness to initiate and maintain a transition back into PA after treatment. Especially in the short-term, AYAs found that their physical limitations (e.g., muscle soreness, nausea) posed as a barrier to engagement. Discussing post-surgery recovery, one AYA stated, “From a physical standpoint it was pretty tough, because you're all sore and your muscles are all tight and you've been lying in bed for a while. . .mechanically it’s tough to get back into running or any physical activity right away.” As illustrated, changes to physical function and capacity acted as obstacles for AYAs when contemplating or attempting re-engagement.
The reduction in functional capacity also decreased AYAs’ confidence to perform PA. An AYA shared, “…I joined the gym, sometimes it was hard to go—because it was like, ‘OK, I'm going to go the gym and not be able’—you know, for a person my age, I'm going to feel completely incompetent and helpless…” Elaborating on this, another AYA who was treated with chemotherapy, provided a specific example of when she felt less confident in her abilities, “I feel that my stability, it's not the same. I'm not feeling comfortable with. . .if it's hiking on the trail, I'm not comfortable with going down or going up or going on a narrow path like I was before.” While the first AYA highlighted that her age did not match perceptions of her physical competence, the other AYA compared her current abilities to her previous ones in activity. Both descriptions underscore the unique experiences for previously active AYAs.
Many AYAs described how they responded to their physical function limitations. One AYA recognized her physical limitations and reframed the expectations she held for herself, “I couldn’t push myself but it doesn’t mean I couldn’t do the activity. That I can still do the same activities, but just have to reshape how far I can push myself in them.” Another AYA also found that they couldn’t exercise as intensely as he previously had, but had a harder time managing the inability of engaging in higher intensity PA, “In terms of endurance, the asthma and the lung problems that I’ve developed have definitely been frustrating. That’s the one annoyance. I used to like to play tennis in the summers and I can't really do that anymore.” In addition to discussions of reductions in intensity, AYAs also discussed duration limitations, “. . .if I were to do my hour workouts—I’d have to space it out, take rests, drink a lot more water. And yeah, I find I breathe a bit heavier.” And so, some AYAs had to change the type, intensity, and duration of their activities due to their physical side effects.
Changes in physical function caused some AYAs to feel embarrassed to engage in PA in public settings. For some, they went so far as to hide their physical limitations, as exemplified by one AYA: . . .it was hard because people don’t see you for what you’ve been through sometimes so they have no idea what you’re having a hard time with and think “Oh can’t you come do this or why?” You know? And then you have to explain “No, I’m not capable of that or that’s too much for me.” So sometimes because of those situations I think I held back or I didn’t participate whether it was a really big hike or volleyball. . .Anything that I really had to put my body forward for, I kind of tried not to do.
Other AYAs further highlighted the unease they had with displaying their physical limitations in front of others: I just felt puffy and uncomfortable in my clothes and it was hard to move and keep up with people, because I was always winded. . .it's not something I want people to see, it's embarrassing. So. . .I would tend to shy away from things. . .
AYAs who did engage in PA despite their discomfort and embarrassment described using purposeful actions to hide their limitations from others (e.g., using the stairs despite fatigue).
Appearance changes impacted AYAs’ PA experiences, with some avoiding or disengaging from public activities. One AYA considered whether he would have attended the gym after surgery if it were not closed due to the COVID-19 lockdown: . . .if the gym was open, I wouldn't feel ready going. . .I wouldn't feel comfortable. Because I lost a lot of weight after the surgery. . .and I was still dealing with the newness of the scar. So, I’d feel a little insecure going to a gym right away.
Meanwhile, another AYA discussed how her appearance changes impacted her avoidance of certain activities where her body would be on display: …friends you know going and playing beach volleyball and they want me to play. . .But I can’t play because I would have to be running around and they could see my body jiggling and if my scar doesn’t look nice then I don’t want them to look at it [. . .] it just stops you. . .you want to kind of do some of these things, but then you can’t [choking up] because your brain gets in the way. . .it’s definitely stopped me from doing all sorts of fun things because I haven’t been confident enough or too insecure or self-conscious.
In contrast, some AYAs described that due to the nature of the activities they engaged in, their appearance changes (e.g., scars) were hidden, which made them more willing to participate in PA in public. For instance, one AYA stated, “. . .if I was wearing a bathing suit, then it might have impacted my return to activity. But most activities that you do, you’re just in random clothes, so it doesn’t matter.” These sentiments underscore that participating in activities where the body is not on display yields greater comfort and engagement. Overall, physical function and appearance changes were barriers to PA participation after treatment, and when AYAs did participate, many worried about how their bodies looked and performed in front of others.
Using PA as a means to change one’s body
PA was used to “offset the damage to what the cancer did.” AYAs revealed that they engaged in activity for body function or appearance reasons, with most participants describing appearance as the key motivator for initiating PA. For instance, one AYA shared: How to accept myself again. . .how to know my body again, because it's changed, it's different now. So I feel that through sport and physical activity, I have more chances to reach my previous body again. . . I was active. . .So I believe that physical activity will help me to reach my old self again or even improve […] I am willing to participate in physical activity because of the weight gain, because I'm trying to stop gaining kilos.
When discussing appearance, many AYAs described engaging in PA to control or change their weight. Specifically, participants used PA to lose weight (“I gained a little bit of weight. So, just to, you know, trim down and look at yourself in the mirror and kind of be proud”), avoid weight gain (“. . .noticing the continuous weight gain so to try to keep that off”), maintain weight (“I’d like to maintain being at the weight I’m at now”), and/or increase muscle mass (“I’m working on muscles [. . .] try to get my strength back up”). Adding complexity, a treatment-induced weight change was a motivating factor for participation, yet weight changes also made it more difficult for some AYAs to engage in PA.
Some AYAs described a desire to use PA to change their bodies to get “in shape” and be attractive and desirable to others. One AYA stated, “I'm a woman and I would like to look great, so [laughs] I need to be in shape.” Another AYA shared, “Being a guy, there was a part of me that was thinking, I’d like to get back to the gym, because I want to get back in shape, because I’d like to meet somebody new.” They went on to say, “I like how things look when I look in the mirror. I like getting compliments from women.”
Success in the transition back to PA was often defined as changes in appearance (e.g., growing observable muscle) and function (e.g., feeling stronger). During treatment, AYAs noticed reduced muscle mass and increased fat mass, which left them feeling uncomfortable. As a result of this discomfort, feeling successful in PA was in part defined as increasing muscle mass and losing fat, “. . .feeling that fat change back into muscle was a great feeling. I just started to feel much more comfortable as time went by. . .and then you can do more things, you feel happier too.” Other AYAs echoed this feeling of success through weight loss: . . .I didn’t like that I couldn’t wear my old clothes. . .that I was using a different belt than I was using before. [. . .] I just felt uncomfortable in my skin and I felt physically uncomfortable all the time. And so it was nice to get rid of that feeling. . .I think that’s both a vanity standpoint and. . .getting your body back to kind of the shape it was before. [. . .] I can fully appreciate how silly it sounds, when you have a life-threatening illness . . .and you just went through that. But it’s kind of like once you're done with that, then you kind of want things back to how it was.
AYAs assessed their body changes by the physical feeling of their body, how their clothing fit, viewing their body in a mirror, and taking pictures to measure observable change over time. For instance, one AYA took pictures once a week, “. . .without [progress pictures], then I wouldn’t be able to look back on it. I wouldn’t see the progress change from where it was at initially to where I’m at. . .it helped my mind know that what I’m doing is actually changing stuff.” For many AYAs, observing and feeling the difference in their body was crucial to feeling accomplished in their PA efforts. AYAs also felt that seeing changes in their body’s appearance and composition helped them cope with other observable body changes: I guess I didn't like that I was all scarred up and missing a testicle and that's also kind of why I liked working out afterwards, because I could get into good shape and I could really like—[laughs] it sounds a bit vain—but I could admire my muscles. . .and take my mind off of the scars.
AYAs shared that activity-related body changes elicited positive thoughts and emotions: …because of the walking, I've recently lost about 50 pounds, so it's actually making me feel more confident, more energetic. I feel lighter, just both mentally and physically and I just, it makes me feel better about just what the future could hold, when I do physical activity. Because I'm not out of energy when I do it now.
Although AYAs reported appearance and weight change goals extensively throughout the interviews, it is important to note that other functional changes were also valued (e.g., activity-induced improvements in energy). For example, one AYA stated, “. . .it wasn’t really about looking good, it was about the exercise, 30 minutes a day, the cardio, to get that memory to ward off the cognitive stuff. That was the kind of priority for me.”
Supportive Care is Essential to Successful PA Transitions
AYAs expressed a need for supportive care in facilitating their transition back into PA, as illustrated through the subthemes: Do it yourself: Unmet support needs contribute to loneliness and Active connections: The critical role of others in supporting the PA transition.
Do it yourself: unmet support needs contribute to loneliness
AYAs described feeling too depleted to initiate PA alone, expressing a need for greater PA support. They explained feeling emotionally and physically exhausted after treatment, which contributed to a lack of motivation. One AYA described this sentiment and spoke how she was not prepared to create or enact a PA transition plan alone: . . .my body was destroyed essentially, so to try and bring it back is so much work, but I didn’t have the mental capacity or the motivation. [. . .] I had to do it myself. So I didn’t do anything for years and years and years.
AYAs further underscored the paucity of healthcare provider support, which compounded the barrier of motivation, “So, I feel like not getting guidance from the doctors [. . .] was part of what was challenging because I really just felt like I was alone by myself in trying to figure it out.” This feeling of lonesomeness in navigating the transition was shared among many AYAs, whereby participants discussed a lack of support and advice from healthcare providers. For instance, an AYA expressed confusion around the lack of PA support from healthcare providers: . . .my oncologist, my radiation oncologist, it was almost like after they had done their jobs that was pretty much it […] I think it’s important that the doctors actually say something. . .going back to my oncologist and he’s a bad ass. […] he’s such a good doctor. And he never ever mentioned physical activity and I'm just like—I just don’t know why.
AYAs described feeling surprised that their healthcare providers did not discuss PA with them.
The lack of support around PA forced many AYAs to take the initiative to seek out resources and advice from healthcare providers. When AYAs sought advice, the information received was inconsistent and oversimplified leading to confusion. For instance, one AYA was eager to get active after surgery, yet she was concerned about her limitations so she asked for advice from her healthcare team and received ambiguous and non-specific answers: I was trying to speak with my family doctor but their best advice was to do whatever feels good for me [. . .] The oncology team, they told me that there's no limitation. [. . .] The surgeon [laughs] was the most specific. He said that because of the surgeries, I shouldn't lift weight, I shouldn't do too much, not to push my muscles too much. So I was trying to read articles online, to search on social media.
Due to the varied and one-off advice, she turned to social media, and over 2 years later she remained unsure about her limitations and was afraid to engage in PA that may be unsafe for her. In addition, some AYAs felt that the advice they received was incompatible with their age and views of the self: . . .I was maybe hoping for a bit more resources from [hospital]. […] just everything in the occupational therapy and returning to work felt aimed at people 20 years older than me. And I felt it wasn’t really aimed for people that were coming from a good place. Not a good place, but like a good state of physical being and just wanting to get back to where they were and want to do things a little faster.
A lack of consistent and ongoing age- and ability-specific information heightened AYAs’ feelings of isolation.
On the rare occasions where healthcare providers initiated PA conversations, it was focused on the medicalization of exercise (e.g., to manage physical side effects) and did not cover the psychosocial benefits of engaging in PA after treatment. For example, one AYA experienced blood clots as a rare post-treatment complication, which led her doctor to recommend PA: . . .one of the doctors. . .he said to me ‘OK, [name] I need you to know if you don't want this to happen again you need to stay active your whole life, you can't be a couch potato ever.’ So I was ‘OK [cautious voice]’, you take that really seriously, so that was the biggest advice I got was stay active no matter what.
AYAs who recounted receiving direction on PA for combatting potential treatment side effects described that it encouraged ongoing participation motivated by concerns around future sickness.
Healthcare providers also provided unsolicited advice on PA based on AYAs’ weight. Healthcare providers who were concerned about AYAs’ weight loss did not encourage PA. In contrast, one AYA received recurrent unwelcomed instruction from healthcare providers: Doctors never give you advice about physical activity, they just literally say you need to lose weight. And I’m like no shit . . . I know that, this is not news to me […] . . .my weight 100% had a factor in them telling me to work out.
This participant’s experience was unique among the AYAs we spoke to and highlights the pervasiveness of weight stigma in medicine. Without the provision of proper assistance or resources, she was left feeling badly about herself, bitter towards healthcare providers, and isolated in her PA transition. Overall, the isolation of re-engaging in PA was prominent through AYAs’ narratives. For those that did receive advice, information, or direction, they found it to be inadequate or caused them to feel negatively, uncertain, and lonesome.
Active connections: the critical role of others in supporting the PA transition
AYAs who were able to access the support of exercise professionals (e.g., trainers, physiotherapists, physiatrists, kinesiologists) described them as helping them feel comfortable and capable of re-engaging and maintaining PA after treatment, “. . .I don’t think I could have done [transition back into PA] without having the trainer.” AYAs expressed a desire to be educated on their limitations and abilities by professionals who were equipped to support cancer survivors. Exercise professionals filled this role by providing informational support, which was useful after treatment (Table 1). However, the AYAs had varied opportunities to connect with professionals and emphasized the importance of having access to exercise professionals (Table S3, Supplemental file 4).
Physical activity support providers and support types with illustrative quotes.
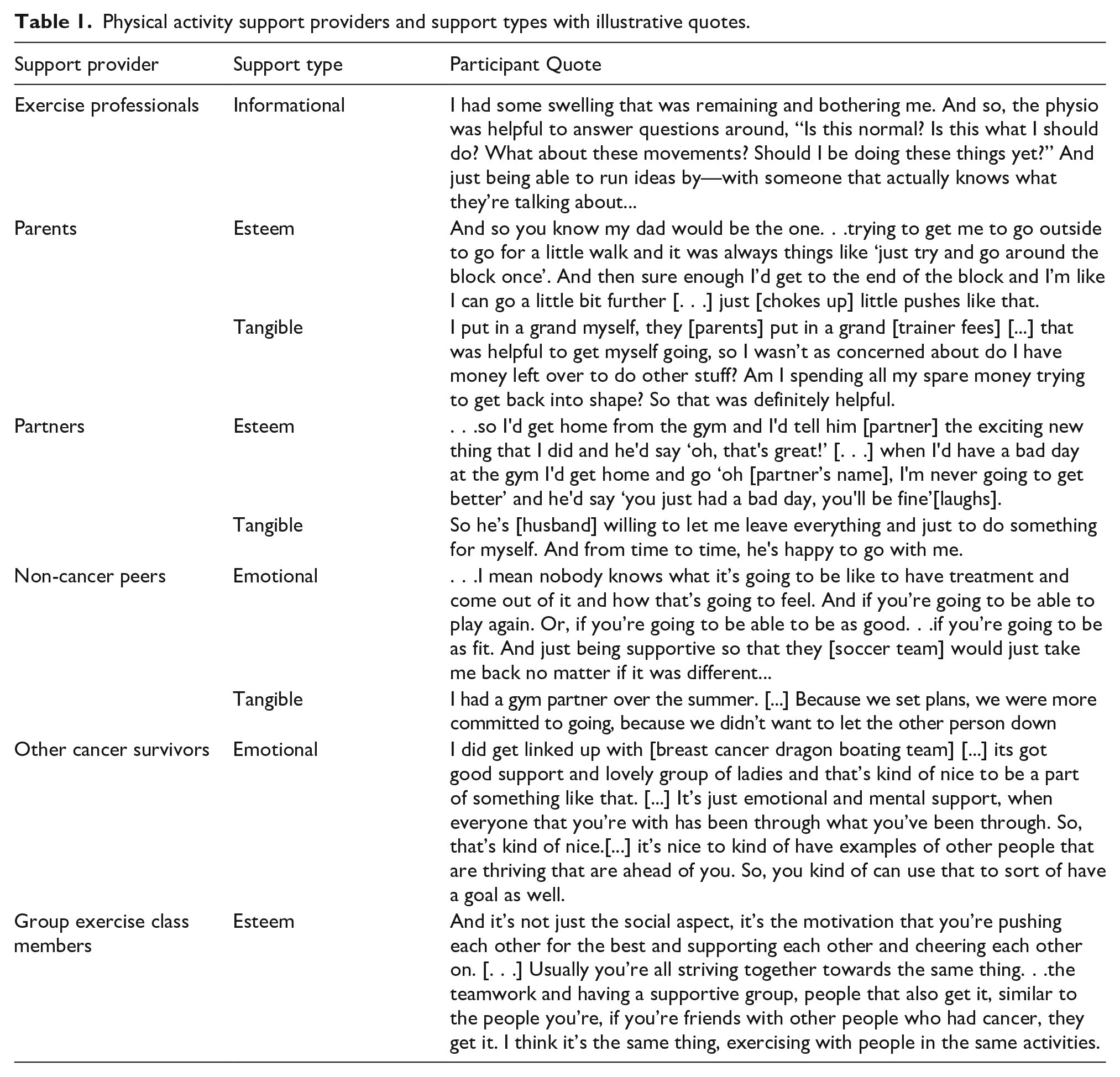
Family, partners, and non-cancer peers provided esteem support through encouragement to engage in PA and/or engaged in PA with the AYA, emotional support through unconditional acceptance regardless of performance changes, and tangible support by helping AYAs schedule their PA, set up virtual fitness applications, and offered financial (e.g., buy exercise equipment, training sessions) and childcare support (Table 1). However, a few AYAs felt that their families were overprotective in regards to their PA. One AYA felt that her family was “so, so overbearing and overprotective,” which hindered her resumption of PA as they encouraged her to rest, “It’s like, ‘Oh, let [name] not do this, let [name] not do that. Don’t walk, don’t move too much. Don’t lift anything heavy, don’t’. It was a lot of ‘don’ts’, because they were trying to, I guess, protect me.” As well, not all AYAs felt that they were accepted or understood by their non-cancer peers, “…I find peers my own age who didn’t have that experience [cancer] just don’t get it as much.” Some AYAs described feeling embarrassed when non-cancer peers did not understand their physical limitations and verbally expressed this misunderstanding, “. . .people don't understand that you can get tired from walking. They're like ‘. . .we didn’t walk very far, we just walked across school, and we didn’t walk that fast.’”
Meanwhile, other cancer survivors helped AYAs to feel understood and comforted, and provided them advice or shared their own PA experiences. AYAs described that hearing advice and experiences facilitated their own motivation for PA. A few AYAs also discussed how they connected with cancer survivors who were further out from treatment (Table 1). One participant was introduced to another AYA through her former coach and described the importance of their role in her PA re-engagement, “. . .being able to talk to somebody who gets it and who’s also young and is now well. I think she was almost 10 years out and very healthy. So it was very inspirational. . .” The connections with survivors further out from treatment provided an example of someone who was able to thrive after cancer. However, a couple of AYAs did not find connecting with other cancer survivors helpful and avoided these types of connections: I found any of the stuff where it was other people’s stories, I actually found it a bit kind of depressing a bit. It just didn’t work for me. […] sometimes people would say things like ‘oh I was upset about this’, or ‘this happened to me’ and it would be stuff I hadn’t even thought about. And I’d be like, ‘oh well now that you mention it, I'm kind of upset by that too’, or ‘this didn’t work for me either’. So I didn’t find that that motivating.
Exercising in a group setting was described as an enjoyable and preferred activity for a few AYAs. Regardless of whether the groups consisted of peers, strangers, or other survivors, they were perceived as supportive, made AYAs feel connected and motivated, boosted morale, and fostered a sense of camaraderie (Table 1, Table S2). While group-based aspects helped to improve AYAs’ perceptions of support, not all were financially accessible or age-appropriate (Table S3, Supplemental file 4). Overall, there were commonalities among the ways in which people provided support to AYAs. Yet, the accounts also illustrate the distinct support roles that others had in AYAs’ PA transition.
Juxtaposed Environments: Fitness Facilities, Cities, and Green Spaces
The ease at which AYAs transitioned back into PA post-treatment was greatly influenced by the environment. They were concerned of receiving negative attention in fitness facilities and did not want to be considered beginners. One AYA highlighted these concerns when he shared: I just felt silly. It just. . .sounds terrible to say it out loud, but it’s the weights too of that weight [two pounds], they're often pink weights. . .it’s kind of emasculating and it’s not very manly, if you will. I mean the guys that are at the gym during the daytime are typically more bodybuilder types. So it’s just—you know, everyone’s got to start somewhere, but it’s—you don’t want to be that person starting there.
Similarly, a couple of female AYAs also articulated discomfort with attending co-ed gyms because they are concerned about unwanted attention and staring. These concerns were exacerbated for AYAs who perceived themselves as overweight. Because of the anticipation of negative attention, AYAs had a difficult time attending the gym or exercising in public spaces.
Among AYAs who were active in fitness facilities post-treatment, some recalled receiving unwanted comments from others that were focused on their appearance and intensified their self-consciousness. For example, one AYA shared: . . .I would take myself to the aquatic center and try and stretch my limbs, I would try and move my body, I would try and help myself. And then. . .you have somebody who, well in this case was an older male who stopped me while I was swimming to ask me why I looked the way that I looked. ‘How come, you seem to have—you know’ [actions to breasts] and I’m like explaining to this gentleman at the edge of the pool, while everyone’s listening. ‘Yes, the reason I do look like a woman is because I am a woman. I’m on cancer treatment and I’m bald’ right. Like fuck [Crying]. As if this isn’t hard enough for me that I have to try and explain myself while I’m there. . .it was just not something I wanted to do. So I just hid.
Relatedly, another AYA revealed his experience with an owner of a private gym: I tried to find a private gym, because I felt less people, a little more focus might be better for what I need. So I go in and the manager sits down and he goes, ‘Let me guess, you just moved into the area, you walked past, see yourself as out of shape, you think we can help you out?’ And I was like, ‘Not exactly’. [. . .] And I felt like OK that’s how people might see me. . .it was a little disappointing [. . .] I feel OK enough with myself that I'm like whatever. . .But it’s still frustrating. . .I'm trying to do something, but this is where you're assuming I’m at versus what I’ve actually been through, what I'm trying to get to.
Some gym trainers also made uninformed comments regarding AYAs’ physical limitations (e.g., joint issues). AYAs recalled that trainers perceived them as young and therefore made assumptions on their capabilities, which contributed to poor gym experiences.
Similar to gyms, varying outdoor environments were contrasted, wherein urban areas were disliked and avoided, while rural areas and green spaces were highly valued and described as therapeutic. Cities were viewed as busy and unsafe due to the traffic and volume of people for AYAs who were immunocompromised after treatment. In contrast, participating in activity in rural areas, parks, and green spaces was enjoyed by AYAs. Aspects of these environments that made them enjoyable included, “the fresh air, the nature. . .it’s rare that you pass somebody else on a trail most days.” AYAs described that when engaging in PA in outdoor quiet environments, they felt better, were more relaxed, and found it difficult to worry. Living near green spaces and trails was beneficial for AYAs’ re-engagement in activity: . . .it's definitely something really positive and great just to be able to walk around and concentrate on nice things around, nature. . .it definitely makes me feel good […] It's a huge bonus and it. . .makes me to get out more because I know it's nice trails and hiking. . .with no huge crowds around.
Markedly, one AYA expressed, “I think that [exercising in nature] would be my top choice if I was exercising. If I can do something outside, that’s always going to be the better choice.” Overall, participating in PA in rural and green spaces was met with positive thoughts and emotions, whilst attending fitness facilities and engaging in activity in urban areas caused a range of mainly negative feelings for AYAs, and at times triggered behavioral avoidance.
Discussion
This study explored previously active AYAs’ experiences transitioning back into PA following cancer treatment. AYAs were motivated to be active for physical appearance and function reasons, and to regain control of their life and health. Factors that undermined a transition back to PA included experiencing identity issues, a lack of specific and ongoing support from healthcare professionals, negative PA experiences in fitness facilities and busy cities, low confidence in one’s physical abilities, and concerns around the body’s appearance and function. However, aspects that helped to facilitate this transition included access to exercise equipment and supports (e.g., exercise professionals and programs), access to natural settings for activity, and supportive others (e.g., family, partners, peers, other cancer survivors). Overall, PA re-engagement necessitated continuous attention and management at the individual level and would have benefited from greater system-level supports. Self-regulatory capacities are depleted through cancer and cancer treatment, increasing difficulties for re-engagement in meaningful activities, like PA (Arndt et al., 2014; Cummins et al., 2017). As such, greater supports at interpersonal and structural levels are needed for AYAs post-treatment.
Similar to previous work (Chisholm, 2020; Head & Iannarino, 2019; Petrella et al., 2020; Wu et al., 2015), AYAs described being motivated to engage in PA to manage changes in body appearance and function, physical and mental health, and one’s routine, independence, and sense of normalcy. Notably, the previously active AYAs were highly invested in their body’s appearance and weight, which was integral to their decision to be active after treatment. Yet, it is well known that exercising for appearance-related reasons is not a sustainable source of PA motivation (Chisholm, 2020; Ingledew& Markland, 2008). A preoccupation with managing one’s weight through PA engagement was common and reinforced by healthcare providers and society. The focus on weight, and appearance more broadly, highlights the pervasiveness of societal idealizations of slim, toned, and muscular bodies that are prominent for AYAs even after cancer treatment. Encouraging a functional body focus and compassion towards one’s appearance and weight changes may be useful individual-level strategies to improve PA maintenance and experiences (Alleva & Tylka, 2021).
Similar to previous reports (e.g., Petrella et al., 2020; Pugh, Petrella, Fisher, et al., 2021; Rabin et al., 2011; Wu et al., 2015), AYAs in the current study recounted worries around physical limitations and safety, dissatisfaction with fitness facilities, lack of support from healthcare providers, and body image concerns and anticipated negative body-related evaluations. The commonality in these reported barriers underscores the critical importance of addressing these issues in order to facilitate a smoother transition back to PA for AYAs. On this note, there are a number of modifiable factors that can be targeted through strategies and interventions (e.g., self-efficacy; body image). For instance, altering one’s capabilities through a PA intervention may help to improve confidence and competence in PA, which can improve body image (Sonstroem & Morgan, 1989). As well, AYAs that report significant body concerns and worries around exercising in public settings may benefit from the development of age-specific, private, and supportive PA programs to improve comfort and ultimately ease the re-initiation of PA.
There was also an unmet need for PA support from healthcare providers that is life-stage and age-appropriate, specific to the AYAs’ goals and needs, and continuously provided. In addition, there is a need for increased supports in the form of referrals to exercise professionals immediately after treatment and provisions of ongoing exercise plans and resources. Consultations with healthcare providers working with AYAs have revealed that they do not feel capable of providing PA advice due to a lack of knowledge and confidence (Pugh, Petrella, Pabary, et al., 2021). Further, healthcare providers have described limited referral pathways as a barrier to recommending PA to cancer survivors (Alderman et al., 2020). There are dedicated guidelines and supports that healthcare providers can consult (e.g., American College of Sports Medicine, 2019; American Council on Exercise, 2021; Schmitz et al., 2019); however, the development of AYA-specific guidelines is needed to appropriately support this unique group of cancer survivors (Adams et al., 2021). In addition, it may be worthwhile to strengthen available resource pathways and explore the benefits of integrating kinesiologists in AYA multidisciplinary cancer care teams (Santa Mina et al., 2018).
In the present study, some AYAs reported feeling uncomfortable when lifting lighter weights and being the target of appearance commentary from gym goers, trainers, and gym owners. These issues are not unique (Coen et al., 2020); however, the ubiquitous gym culture challenges participation, even for AYAs that had extensive previous gym experience. These accounts suggest that changes to the wider gym industry are needed, for example, weights should be gender neutral in color, body commentary should be banned, and front-facing staff including owners and trainers need sensitivity and inclusivity training. Although challenging gym culture will be beneficial for AYAs and beyond, AYAs may need additional support navigating these contexts and situations.
For the previously active AYAs in the current study, PA was important not only as a strategy to regain control and normalcy, but as part of their athletic identity as well. Similar results have been reported with previously active AYAs on treatment (Adamsen et al., 2009). AYAs had extensive prior PA experiences and were often expected to seamlessly re-engage in previously enjoyed activities and intensities. Managing PA expectations for post-treatment PA during treatment and promoting a more holistic view of activity may help with adaptability post-treatment and in turn, reconciling athletic identity issues. Further, supportive others (e.g., exercise professionals) should encourage AYAs to engage in previously enjoyed activities if possible, even if at a lower intensity. Focusing on enjoyable activities and holistic views of health may tap into intrinsic motivation for PA (Ryan & Deci, 2002), improving re-engagement and maintenance.
Aligned with previous literature with AYAs (Petrella et al., 2020; Wu et al., 2015), social support for PA was particularly useful for previously active AYAs to help streamline this transition. Based on this finding, it would be useful to leverage social connections by fostering a sense of community in interventions and programming. First, several AYAs noted the usefulness of connecting with other cancer survivors, especially those who were further out from treatment and were role models for PA. And so, future AYA program development should focus on group exercise programming (e.g., DeNysschen et al., 2020) or use a peer support model utilizing peer mentorship, as these types of programs may be especially useful for previously active AYAs. In addition, designing accessible age- and life-stage group PA programs and facilitating awareness of and participation in the programs would be worthwhile. One-day PA events for AYAs have shown to help increase confidence in engaging in further PA programs and may be great gateway to sustained group participation (Pugh, Petrella, Fisher, et al., 2021). Further, given the crucial role of supportive others, targeting the support people directly to provide them with education on the safety and benefits of PA for cancer survivors, as well as the ways in which they could support AYAs could be a helpful approach (Price et al., 2020). The current interviews indicate that education and tools could be especially valuable for supportive others who do not provide adequate PA support due to concerns around the safety and benefits of PA for AYAs.
The findings should be considered in light of the following limitations. Despite dedicated recruitment efforts, as is the case with many studies conducted with AYAs, the sample size was limited. Future research efforts should be aimed at recruiting larger samples. Although we attempted to recruit a heterogeneous group of AYAs, we had difficulties recruiting those with varying socioeconomic statuses and ethnicities. Given the additional barriers to PA for those who identify with minority ethnicities and lower socioeconomic statuses (Powell et al., 2004; Stalsberg & Pedersen, 2010), more work is needed to explore the PA transition experiences among diverse ethnicities and income statuses. The sample included AYAs who formerly engaged in competitive and/or recreational PA, as well as varied in the previous type, frequency, and intensity of PA. Whilst this provided variability in the accounts and experiences, it may be valuable to explore the differences in experiences based on former PA characteristics in future research. Although some participants who were further out from treatment (maximum = 9 years) provided rich accounts of their experiences, they may have described their experiences differently had they been closer to treatment. Thus, future research should consider limiting time since treatment. In addition, body image and social support were interconnectedly explored and discussed in the present study; however, a separate and thorough exploration of these topics would be a worthwhile endeavor for future research. Finally, the interviews were conducted with audio-only or audio and video, which may have impacted rapport building, level of comfort and disclosure, and duration of interviews (Irvine et al., 2013; Jowett et al., 2011). All participants shared in-depth accounts of their experiences, yet the extent of impact that the mode of interview had on the information disclosed and length of interviews is unknown.
Limitations notwithstanding, the present study contributes to the limited literature on AYAs’ experiences transitioning back into PA after treatment. In addition, our study describes the unique accounts of previously active AYAs. This research afforded this subgroup of AYAs the space to share their experiences and helped to uncover nuances that may have been otherwise overlooked by studying the PA transition experiences in AYAs more broadly. Deepening knowledge on this subset of AYAs is essential to informing tailored strategies and programming aimed at improving AYAs’ well-being through survivorship.
Supplemental Material
sj-pdf-1-qhr-10.1177_10497323221089855 – Supplemental material for “Your Body Is Not At All Where You Left It”: Adolescent and Young Adult Cancer Survivors’ Experiences Transitioning Back Into Physical Activity After Treatment
Supplemental material, sj-pdf-1-qhr-10.1177_10497323221089855 for “Your Body Is Not At All Where You Left It”: Adolescent and Young Adult Cancer Survivors’ Experiences Transitioning Back Into Physical Activity After Treatment by Madison F. Vani, Catherine M. Sabiston, Daniel Santa Mina and Linda Trinh in Qualitative Health Research
Supplemental Material
sj-pdf-2-qhr-10.1177_10497323221089855 – Supplemental material for “Your Body Is Not At All Where You Left It”: Adolescent and Young Adult Cancer Survivors’ Experiences Transitioning Back Into Physical Activity After Treatment
Supplemental material, sj-pdf-2-qhr-10.1177_10497323221089855 for “Your Body Is Not At All Where You Left It”: Adolescent and Young Adult Cancer Survivors’ Experiences Transitioning Back Into Physical Activity After Treatment by Madison F. Vani, Catherine M. Sabiston, Daniel Santa Mina and Linda Trinh in Qualitative Health Research
Supplemental Material
sj-pdf-3-qhr-10.1177_10497323221089855 – Supplemental material for “Your Body Is Not At All Where You Left It”: Adolescent and Young Adult Cancer Survivors’ Experiences Transitioning Back Into Physical Activity After Treatment
Supplemental material, sj-pdf-3-qhr-10.1177_10497323221089855 for “Your Body Is Not At All Where You Left It”: Adolescent and Young Adult Cancer Survivors’ Experiences Transitioning Back Into Physical Activity After Treatment by Madison F. Vani, Catherine M. Sabiston, Daniel Santa Mina and Linda Trinh in Qualitative Health Research
Supplemental Material
sj-pdf-4-qhr-10.1177_10497323221089855 – Supplemental material for “Your Body Is Not At All Where You Left It”: Adolescent and Young Adult Cancer Survivors’ Experiences Transitioning Back Into Physical Activity After Treatment
Supplemental material, sj-pdf-4-qhr-10.1177_10497323221089855 for “Your Body Is Not At All Where You Left It”: Adolescent and Young Adult Cancer Survivors’ Experiences Transitioning Back Into Physical Activity After Treatment by Madison F. Vani, Catherine M. Sabiston, Daniel Santa Mina and Linda Trinh in Qualitative Health Research
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This manuscript was prepared while MFV was supported by a doctoral scholarship from the Social Sciences and Humanities Research Council of Canada. CMS currently holds a Canada Research Chair in Physical Activity and Mental Health. This manuscript was supported by a Canadian Cancer Society William E Rawls award granted to CMS. Funding sources were not involved in the study design, data collection, analysis or interpretation, or the preparation of the manuscript for publication.
Supplemental Material
Supplemental Material for this article is available online.
Notes
Author Biographies:
Madison F. Vani is a Postdoctoral fellow in the Faculty of Kinesiology and Physical Education at the University of Toronto and is currently funded through a Social Sciences Research Council of Canada Postdoctoral Fellowship.
Catherine M. Sabiston is a Professor in the Faculty of Kinesiology and Physical Education at the University of Toronto and a Canada Research Chair in Physical Activity and Mental Health.
Daniel Santa Mina is an Associate Professor the Faculty of Kinesiology and Physical Education at the University of Toronto.
Linda Trinh is an Assistant Professor in the Faculty of Kinesiology and Physical Education at the University of Toronto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.