
Abstract
Purpose
This study evaluated six abbreviated versions of the DASS-21 in adult male survivors of sexual abuse to identify valid, reliable, and efficient tools for trauma-informed assessment.
Method
Secondary data from 534 male survivors were analyzed using confirmatory factor analysis to assess model fit, reliability, and construct validity.
Results
All forms showed acceptable reliability (α ≥ .70). After modification, all models fit the data well. The two-factor DASS-10 was statistically superior (CFI = .996, RMSEA = .025, nonsignificant χ²). The three-factor DASS-12a also demonstrated excellent fit (CFI = .987, RMSEA = .040) and met all convergent validity criteria (all AVEs ≥ .50). Discriminant validity between anxiety and stress was not supported.
Discussion
The DASS-12a is the most sound three-factor option, while the D-10 offers a more robust, two-factor measure of general distress ideal for rapid screening. Generalizability is limited.
Accurate assessment of mental health symptoms is essential for effective practice, especially when working with individuals affected by trauma. Brief, standardized self-report measures have increasingly been recommended in clinical, community, and counseling settings to monitor client progress, support timely intervention, and inform collaborative decision-making (Barkham et al., 2023; Lambert & Shimokawa, 2011). Instruments that are concise, easy to administer, and capable of capturing multiple domains of psychological distress—such as depression, anxiety, and stress—are particularly valuable in service environments where time and resources may be limited. Widely used tools like the PHQ-9 (Kroenke et al., 2001), GAD-7 (Spitzer et al., 2006), and BDI (Beck et al., 1996) often address one or two domains of emotional distress, but frequently overlook stress as a separate construct. The Depression Anxiety Stress Scales (DASS; Lovibond & Lovibond, 1995a, 1995b), by contrast, were developed to measure these three related constructs within a unified framework and have shown strong utility in mental health contexts.
Trauma-specific symptomatology highlights the relevance of these domains for survivors of sexual abuse. Hyperarousal symptoms such as irritability, tension, and sleep disturbance are well captured by the DASS stress subscale (Antony et al., 1998; Clara et al., 2001). Panic, fear, and physiological arousal map onto the anxiety subscale (Clark & Watson, 1991; Lovibond & Lovibond, 1995a). Similarly, depressive cognitions such as hopelessness, anhedonia, and diminished self-worth correspond closely to the depression subscale (Beck et al., 1996; Crawford & Henry, 2003). These alignments suggest that the DASS domains are particularly suited to indexing the multifaceted distress common among trauma-affected populations (Zanon et al., 2021).
Despite its strengths, the DASS—particularly its short forms—has not been validated for use with adult male survivors of sexual abuse, a population that remains underrepresented in both research and assessment. Masculine norms often discourage emotional expression and help-seeking, which can inhibit assessment and service engagement (Easton, 2014; Javaid, 2015). Validating brief and accessible assessment tools for this group is a crucial step toward trauma-informed and gender-responsive care. This study evaluates six abbreviated versions of the DASS-21 to determine which are most psychometrically sound and practically applicable for assessing emotional distress in adult male survivors of sexual abuse.
Literature Review: Psychometric Abbreviations of the DASS
The DASS was originally developed as a 42-item measure assessing depression, anxiety, and stress, with 14 items per subscale rated on a 4-point Likert scale (0 = Did not apply to me at all to 3 = Applied to me very much or most of the time; Lovibond & Lovibond, 1995a). Psychometric evaluations confirmed a strong three-factor structure and excellent reliability, with Cronbach's alpha ranging from .95 to .97 for depression, .89 to .92 for anxiety, and .93 to .95 for stress (Antony et al., 1998; Clara et al., 2001; Crawford & Henry, 2003). To reduce respondent burden, the DASS-21 was developed by selecting seven items per subscale. Confirmatory factor analyses (CFA) have consistently supported its three-factor structure in both clinical and nonclinical populations (Henry & Crawford, 2005; Sinclair et al., 2012; Soria-Reyes et al., 2024). A systematic review by Dwight et al. (2024) reported internal consistency ranging from acceptable to excellent: α = .72–.93 for depression, .77–.90 for anxiety, and .70–.94 for stress. As of January 9, 2025, the DASS-21 has been translated into 60 languages and is widely used as a validated tool for assessing emotional distress (University of New South Wales, 2025).
To orient readers to the central trade-off between brevity and measurement coverage, I summarize short forms in descending item count (from 20 items to 8 items), then discuss their factor structures and psychometric findings; Table 1 is streamlined to enhance readability while preserving comprehensive details for reference.
Summary of Psychometric Studies on DASS-21 Short Forms (DASS-20 to DASS-8).
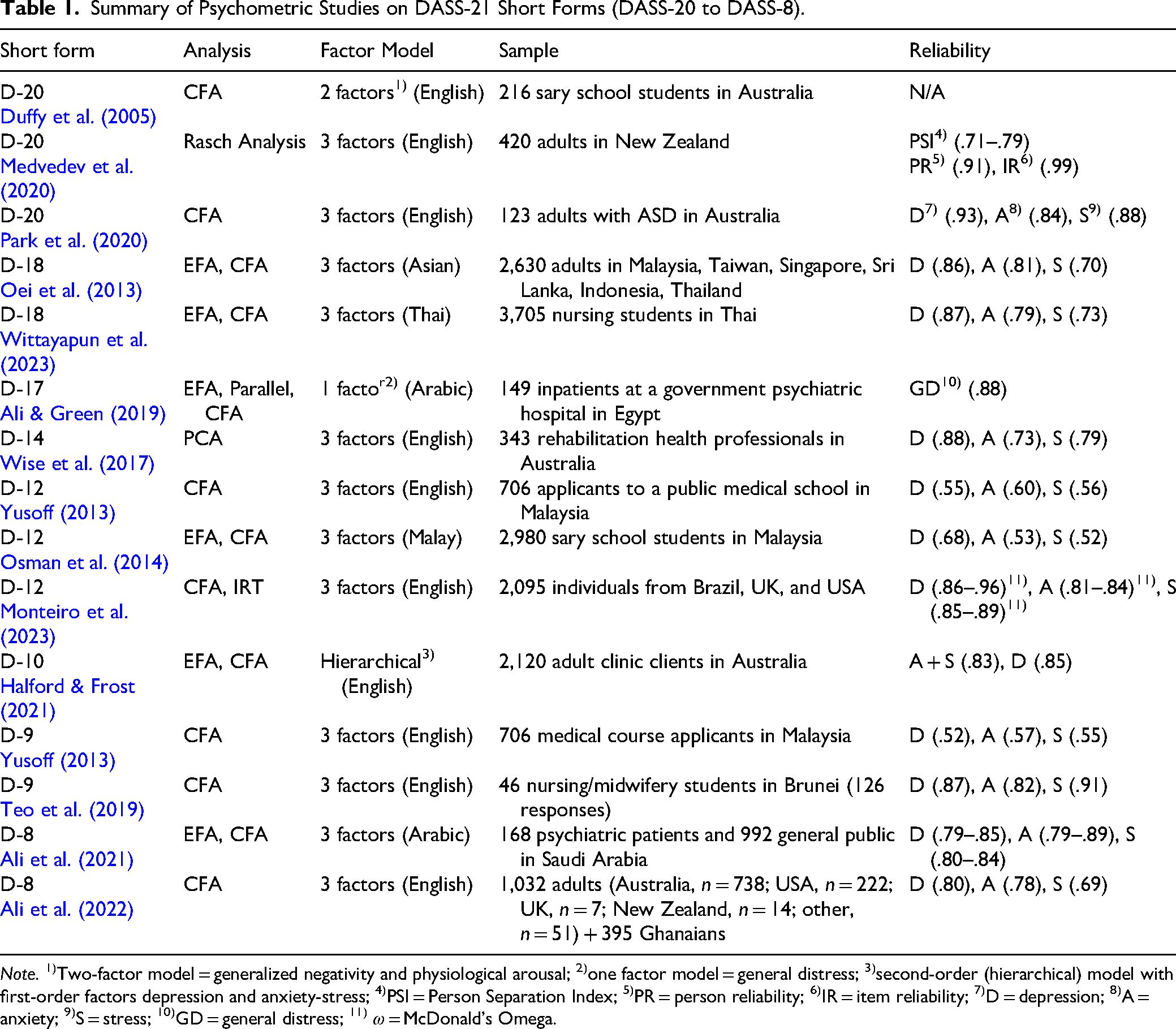
Note. 1)Two-factor model = generalized negativity and physiological arousal; 2)one factor model = general distress; 3)second-order (hierarchical) model with first-order factors depression and anxiety-stress; 4)PSI = Person Separation Index; 5)PR = person reliability; 6)IR = item reliability; 7)D = depression; 8)A = anxiety; 9)S = stress; 10)GD = general distress; 11) ω = McDonald's Omega.
Emergence of Shorter DASS Versions
To further enhance efficiency, researchers have developed abbreviated DASS forms (8–20 items) using exploratory factor analysis (EFA), CFA, item response theory (IRT), and Rasch analysis. This review summarizes 15 such short forms (see Table 1), focusing on their development, psychometric properties, and suitability for adult male survivors of sexual abuse.
DASS-20 (20 Items)
Several studies proposed 20-item DASS versions by removing one item from the DASS-21 to improve psychometric properties. Duffy et al. (2005) tested the DASS-21 in 216 Australian adolescents, finding a two-factor structure (generalized negativity and physiological arousal) with acceptable fit (χ²(168) = 296.63, p = .144, GFI = .88, CFI = .90, RMSEA = .06). However, internal consistency was not reported, and the two-factor model deviates from the tripartite DASS framework, limiting its theoretical alignment. Medvedev et al. (2020) applied Rasch analysis to the DASS-21 in 420 New Zealand adults, removing one item and creating super-items to address local dependencies. The resulting DASS-20 retained the three-factor structure with good fit (χ²(15) = 20.28, p = .161) and acceptable subscale reliability (PSI = .71–.79), with excellent total scale reliability (person reliability = .91; item reliability = .99). Park et al. (2020) evaluated the DASS-21 in 123 Australian adults with Autism Spectrum Disorder, supporting the original three-factor structure and –after removing the “dryness of mouth” item and allowing correlated residuals—reporting a modified 20-item three-factor model with acceptable fit (χ²(165) = 284.4, p < .001, CFI = .924, RMSEA = .077, SRMR = .060) and good-to-excellent internal consistency (α = .93 for depression, .84 for anxiety, .88 for stress). The DASS-20 offers marginal brevity over the DASS-21, with inconsistent adherence to the original three-factor model. Duffy et al. (2005)'s two-factor structure sacrifices theoretical coherence, as it fails to differentiate depression, anxiety, and stress as distinct constructs (Lovibond & Lovibond, 1995b). Medvedev et al. (2020) and Park et al. (2020) maintain the tripartite framework but achieve only modest reductions in respondent burden. Because the DASS-20 removes only one item relative to the DASS-21, the reduction in respondent burden is negligible and offers limited practical advantage in clinical or routine-monitoring contexts (Boateng et al., 2018; DeVellis, 2016; Streiner & Norman, 2015).
DASS-18 Short Form (18 Items)
Oei et al. (2013) developed a DASS-18 by removing three stress items from the DASS-21 in 2,613 employees across six Asian countries. EFA (52.21% variance explained) and CFA supported a three-factor structure (7 depression, 7 anxiety, 4 stress) with good fit (χ²(116) = 552.01, p < .001, CFI = .94, RMSEA = .06, GFI = .95, NFI = .92) and internal consistency (α = .86 for depression, .81 for anxiety, .70 for stress). Wittayapun et al. (2023) validated a Thai DASS-18 in 3,705 nursing students, using split-sample EFA (n = 2,000; KMO = .965, 71.31% variance) and CFA (n = 1,705; χ²/df = 3.08, CFI = .98, GFI = .98, NFI = .99, RMSEA = .032). Internal consistency was strong (α = .87 for depression, .79 for anxiety, .73 for stress), with good convergent and discriminant validity. The DASS-18 maintains the three-factor structure and demonstrates strong psychometric properties across diverse populations. However, its development in non-English contexts (Asian versions) raises concerns about linguistic equivalence for English-speaking populations (e.g., Streiner & Norman, 2015).
DASS-17 Short Form (17 Items)
Ali and Green (2019) evaluated the DASS-21 in 149 Egyptian inpatient drug users, finding poor fit for the three-factor model. Exploratory, partial confirmatory, and parallel analyses supported a unidimensional structure. After removing four items, the resulting DASS-17 showed good unidimensionality, strong internal consistency (α = .88), and convergent validity (r = .417–.495 with affective stigma). The DASS-17's unidimensional structure diverges significantly from the tripartite theoretical framework of the DASS (Lovibond & Lovibond, 1995b), making it less appropriate for studies requiring distinct subscale scores, such as those assessing specific symptom profiles in trauma survivors. Its validation in an Arabic-speaking, substance-using sample further limits its applicability to English-speaking trauma survivors, as cultural and clinical differences may affect symptom expression (Oei et al., 2013; Teo et al., 2019).
DASS-14 Short Form (14 Items)
Wise et al. (2017) developed a DASS-14 in 343 Australian health professionals using principal components analysis, selecting five depression, five anxiety, and four stress items to minimize construct overlap. The three-factor structure showed good internal consistency (α = .88 for depression, .73 for anxiety, .84 for stress) and concurrent validity with related constructs. The DASS-14 balances brevity with psychometric robustness, retaining the three-factor structure and acceptable reliability. However, the anxiety subscale's marginal reliability (α = .73) falls below the preferred threshold for applied use (Nunnally & Bernstein, 1994), and nonclinical validation limits generalizability to trauma-exposed groups—particularly adult male survivors of childhood sexual abuse, who frequently report heightened internalizing distress (Easton, 2014). Consistent with best-practice guidance, short forms should therefore be revalidated in the intended clinical population (Boateng et al., 2018; DeVellis, 2016).
DASS-12 Short Form (12 Items)
Yusoff (2013) tested a DASS-12 in 706 Malaysian medical school applicants, reporting excellent model fit (χ² = 63.16, p = .118, CFI = .989, GFI = .985, RMSEA = .024), but poor internal consistency across subscales (α = .55 for depression, .60 for anxiety, .56 for stress). Osman et al. (2014) similarly developed a Malay-language DASS-12 using data from 2,980 Malaysian secondary school students. While their model also demonstrated good fit (χ²(57) = 132.94, p < .001, CFI = .96, GFI = .98, RMSEA = .04), reliability coefficients were similarly low (α = .68 for depression, .53 for anxiety, .52 for stress). Monteiro et al. (2023) validated a DASS-12 (Mini-DASS) across 2,096 adults from Brazil, the United States, and the United Kingdom, reporting good fit (e.g., Study 3: χ²/df = 3.59, CFI = .97, TLI = .96, RMSEA = .072 [90% CI = .055-.089]; SRMR = .041) and strong reliability (McDonald's ω = .86–.96 for depression, .81–.84 for anxiety, .85–.89 for stress). The DASS-12 offers significant brevity, but reliability varies widely. Yusoff (2013) and Osman et al. (2014) report low internal consistency, suggesting limited symptom homogeneity in their samples (Nunnally & Bernstein, 1994). Monteiro et al. (2023) demonstrate superior psychometric properties and cross-cultural invariance, making their version a stronger candidate for diverse populations. However, its performance in trauma-specific contexts remains untested.
DASS-10 Short Form (10 Items)
Halford and Frost (2021) developed the DASS-10 using two Australian clinical samples (n = 1,036 and n = 1,084). CFA supported a hierarchical model with two first-order factors—depression and anxiety–stress—and a higher-order general distress factor, with acceptable fit (χ²(34) = 218.83, CFI = .959, RMSEA = .072). Internal consistency was good (α = .85 for depression; α = .83 for anxiety-stress), and the scale demonstrated discriminant validity and sensitivity to therapeutic change. Its ability to capture both general distress and specific depressive symptoms makes it a valuable clinical tool. However, combining anxiety and stress into a single factor may limit its ability to differentiate these constructs—an important consideration given that survivors often exhibit complex internalizing presentations (Easton, 2014) and that the original DASS was theoretically designed to separate depression, anxiety, and stress (Lovibond & Lovibond, 1995a, 1995b; Zanon et al., 2021).
DASS-9 Short Form (9 Items)
Yusoff (2013) proposed a DASS-9 in 706 Malaysian medical students, with excellent fit (χ² = 26.11, p = .348, GFI = .992, CFI = .997, RMSEA = .011) but poor reliability (α = .52 for depression, .57 for anxiety, .55 for stress). Teo et al. (2019) validated a DASS-9 in 126 responses from 42 Brunei nursing students, reporting good fit (χ² = 57.1, p < .001, CMIN/DF = 2.38, SRMR = .037) and good reliability (α = .87 for depression, .82 for anxiety, .91 for stress). While the DASS-9's brevity is appealing, Yusoff's (2013) version demonstrates inadequate reliability, limiting its use in applied settings (Nunnally & Bernstein, 1994). In contrast, Teo et al.'s (2019) version shows promise, with strong reliability and good model fit. However, its small sample size (42 participants providing 126 responses) and reliance on repeated measures raise concerns.
Repeated assessments from the same individuals may inflate reliability by reflecting within-subject consistency rather than true population-level stability, warranting cautious interpretation (Tavakol & Dennick, 2011). Further validation in larger, more diverse samples—including trauma-exposed populations—is recommended to establish generalizability (Boateng et al., 2018; DeVellis, 2016).
DASS-8 Short Form (8 Items)
Ali et al. (2021) developed a DASS-8 in Saudi Arabia (n = 1,160), with excellent fit (χ² = 16.5–67.0, p = .420–.001, CFI = .998–1.000, RMSEA = .013–.059) and good reliability (α = .79–.85 for depression, .79–.89 for anxiety, .80–.84 for stress). Ali et al. (2022) validated an English DASS-8 in 1,032 adults (primarily Australia and the United States), reporting excellent fit (χ²(15) = 44.96, p < .001, CFI = .99, RMSEA = .04) and acceptable reliability (α = .80 for depression, .78 for anxiety, .69 for stress). Although the DASS-8 offers maximal brevity and demonstrates strong model fit, its two-item stress factor falls below the commonly recommended three-indicator benchmark for latent factor identification and stable estimation (Brown, 2015; Kline, 2015). Moreover, the stress subscale's reliability is marginal (α = .69), falling below thresholds typically recommended for applied use (Nunnally & Bernstein, 1994).
Inclusion Criteria for Selecting DASS-21 Short Forms
Four criteria guided the selection of short forms for the present study.
English-language development: To ensure linguistic fidelity and avoid translation-related biases that could alter item meaning or psychometric properties (Streiner & Norman, 2015), short forms must be developed using the English-language DASS. Restricting the sample to English-based validations minimizes the risk of translation-induced distortions in factor structure or item functioning due to cultural differences in symptom expression. Theoretical alignment: To ensure item reduction reflects theoretical intent rather than statistical convenience, short forms must align with the DASS's conceptual foundation (Lovibond & Lovibond, 1995a, 1995b). Preserving content validity is especially important when reducing items for complex constructs like emotional distress (DeVellis, 2016). Minimum three items per subscale: Each subscale must include at least three items to ensure stable factor estimation, as fewer items risk under-identification and unreliable construct measurement (Brown, 2015; Kline, 2015). This criterion, linked to theoretical alignment, safeguards the ability to measure distinct constructs reliably. Substantial item reduction with psychometric integrity: Short forms must significantly reduce items from the DASS-21 (21 items) while maintaining reliability (Cronbach's α ≥ .80 preferred; Nunnally & Bernstein, 1994) and factorial validity (e.g., good CFA fit). This balances brevity, critical for reducing respondent burden, with accurate measurement.
Based on these criteria, the DASS-18 (Oei et al., 2013; Wittayapun et al., 2023), DASS-17 (Ali & Green, 2019), and DASS-12 (Osman et al., 2014) were excluded due to non-English development. The DASS-8 (Ali et al., 2022) was excluded for having only two items in the stress subscale, and the DASS-20 was excluded due to minimal item reduction. Selected short forms for the present study are the DASS-14 (Wise et al., 2017), DASS-12 (Monteiro et al., 2023; Yusoff, 2013), DASS-10 (Halford & Frost, 2021), and DASS-9 (Teo et al., 2019; Yusoff, 2013). Table 2 outlines the specific items included in each of these six short forms.
Item Composition of Selected DASS-21 Short Forms Selected for Validation in This Study.
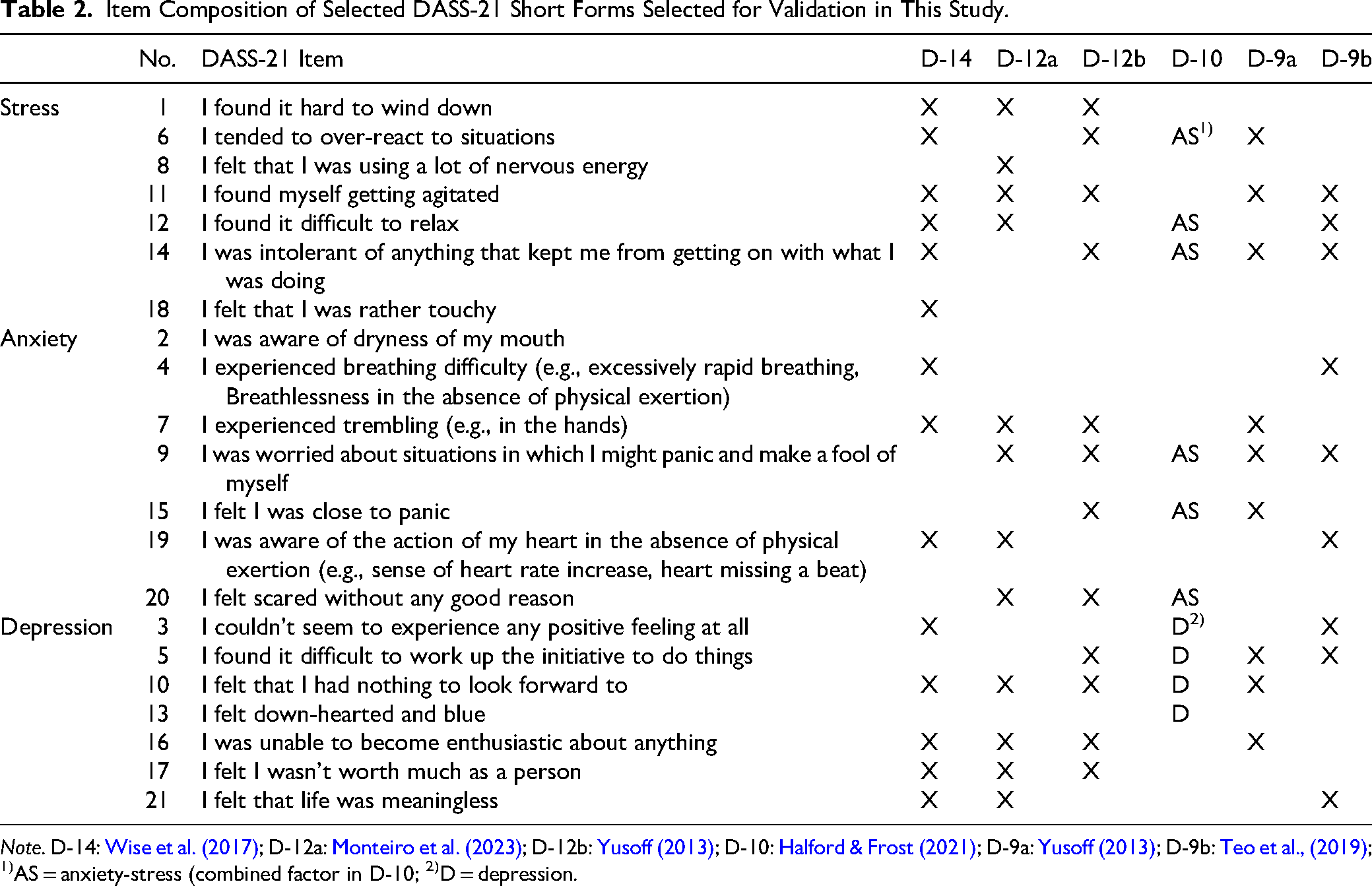
Note. D-14: Wise et al. (2017); D-12a: Monteiro et al. (2023); D-12b: Yusoff (2013); D-10: Halford & Frost (2021); D-9a: Yusoff (2013); D-9b: Teo et al., (2019); 1)AS = anxiety-stress (combined factor in D-10; 2)D = depression.
Research Question
The research question guiding this study is: Which English-language DASS short form demonstrates the strongest psychometric properties—reliability, factor structure, and construct validity—when applied to adult male survivors of sexual abuse?
Method
Research Design and Participants
This study utilized a quantitative, cross-sectional design, analyzing secondary data from publicly funded trauma support programs for male survivors of sexual abuse in Ontario, Canada. The data were collected by the Sexual Assault Crisis Centre of Essex County (SACC), the Lead Agency for 18 government-funded male survivor programs across 12 county regions in western Ontario. SACC coordinated intake assessment using the DASS-21 (Lovibond & Lovibond, 1995b) as part of routine service delivery and program monitoring. The dataset comprised de-identified intake records collected between January 5, 2010, and May 17, 2022, for administrative and service delivery purposes.
From 2,986 original records, cases were excluded if participants were not adults or had more than 10% missing responses on the Depression Anxiety Stress Scales (DASS-21), the key variable in this study. This yielded a final sample of 534 adult male survivors of sexual abuse. Participants ranged in age from 18 to 85 years (n = 501; M = 40.14, SD = 11.9). Approximately 67–94% of participants provided demographic data. Among respondents (n = 367), 45.2% had high school education, 25.6% college, 12.5% university, and 4.9% graduate studies. Employment status (n = 361) included 40.7% unemployed, 35.5% employed full-time, 9.7% part-time, and 2.8% students. Marital status (n = 366) comprised 41.8% single, 22.4% married, 13.7% common-law, 10.4% separated, 8.7% divorced, and .3% widowed. Primary language (n = 364) was English for 95.3%, French for 3.6%, and other languages for .8%. Indigenous identity (n = 358) was reported by 6.1% with 83.8% identifying as non-Indigenous. Ethical approval for secondary data analysis was obtained from an institutional Research Ethics Board prior to conducting the analyses.
Measure
The Depression Anxiety Stress Scales-21 (DASS-21; Lovibond & Lovibond, 1995a, 1995b) is a 21-item self-report measure assessing depression, anxiety, and stress, with seven items per subscale rated on a 4-point Likert scale (0 = Did not apply to me at all to 3 = Applied to me very much or most of the time). In this sample, internal consistency exceeded the recommended threshold (α ≥ .80; Nunnally & Bernstein, 1994), with Cronbach's α of .92 for depression, .85 for anxiety, and .86 for stress. Details of the DASS short forms are provided in the Literature Review.
Preliminary Analyses
Data were screened for quality and suitability prior to CFA. Items with less than 10% missing data were imputed using regression-based methods, consistent with standard approaches for low missing data (Enders, 2010). Skewness and kurtosis values were within acceptable limits (|skew| < 2.0; |kurtosis| < 7.0), supporting univariate normality (West et al., 1995). Mahalanobis distance flagged 20 multivariate outliers (3.75%). As Kline (2015) notes, the presence of a small proportion of outliers is not uncommon in large datasets and may be retained if they do not exert undue influence on model fit or parameter estimates. Variance inflation factors ranged from 1.25 to 2.86, below the threshold of 5.0 (Menard, 2002), indicating no multicollinearity.
Statistical Procedure
Preliminary analyses, internal consistency (Cronbach's α; see Table 3), and descriptive statistics were conducted using SPSS Statistics ver. 30. CFA was performed using AMOS ver. 30 to evaluate the factorial validity of the DASS-21 and six short forms. Model fit was assessed using chi-square, Goodness-of-Fit Index (GFI), Comparative Fit Index (CFI), Tucker-Lewis Index (TLI), Incremental Fit Index (IFI), Normed Fit Index (NFI), Standardized Root Mean Square Residual (SRMR), and Root Mean Square Error of Approximation (RMSEA), along with its 90% confidence interval. Model modification indices were examined; additional covariances between error terms were added sparingly and only when theoretically justifiable (e.g., within-factor error correlations) to improve fit. These modifications are reported alongside the results.
Cronbach's Alpha Coefficients for the DASS-21 and Selected Short Forms.
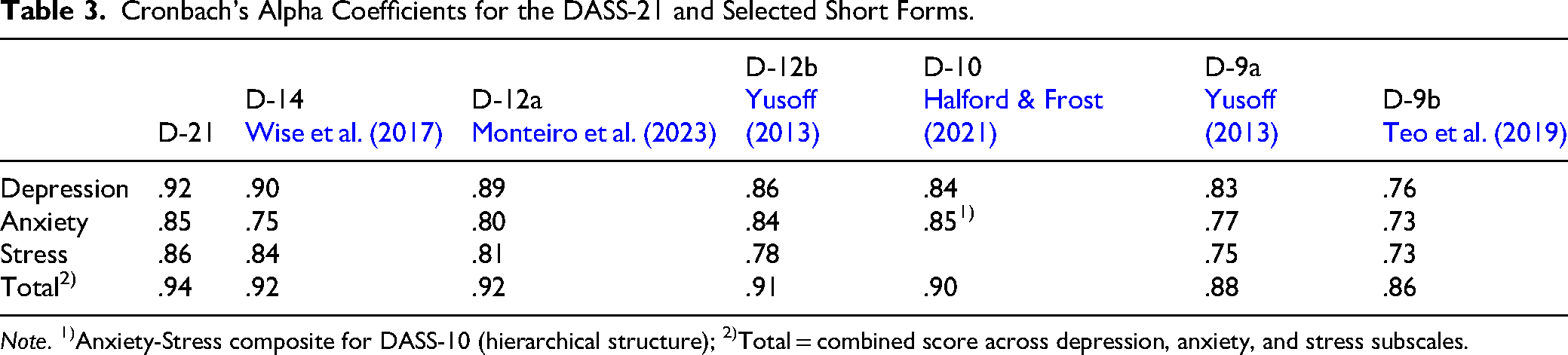
Note. 1)Anxiety-Stress composite for DASS-10 (hierarchical structure); 2)Total = combined score across depression, anxiety, and stress subscales.
The adequacy of the sample size was evaluated according to widely cited guidelines for CFA. Kline (2015) recommended samples of N ≥ 200, and Hair et al. (2019) noted that 10–20 participants per estimated parameter are generally sufficient. With N = 534, the present study exceeded these recommendations, providing stable parameter estimates. A formal a priori power analysis was not conducted, but the sample size is consistent with established standards in SEM research.
Per Hu and Bentler (1999) and Kline (2015), a close model fit is typically indicated by RMSEA ≤ .05. Good fit is generally reflected by CFI, TLI, IFI, NFI, and GFI ≥ .95 and SRMR ≤ .08, while acceptable fit corresponds to values ≥ .90 and RMSEA and SRMR ≤ .08. Although the CFI and TLI are generally considered more robust and are preferred, other indices such as the GFI, IFI, and NFI continue to be commonly reported in the literature. Thus, these indices are also used for comparative purposes. Convergent validity was assessed using the average variance extracted (AVE), with values ≥ .50 indicating adequate convergence (Fornell & Larcker, 1981). Discriminant validity was supported when the AVE for each construct exceeded the squared inter-construct correlations (r²), consistent with the Fornell and Larcker (1981) criterion. To assess the precision of the inter-construct correlations, a bootstrapping procedure with 2,000 resamples was used to generate bias-corrected 95% confidence intervals (CIs) for each latent factor correlation.
Transparency and Openness
This study's design and analytic plan were not preregistered. Deidentified data, analytic code, and research materials are not publicly available due to secondary data use agreements with the original data providers. However, descriptive item compositions for all six DASS short forms evaluated in this study are included in Table 2 to support transparency. Data were analyzed using IBM SPSS Statistics (Version 30.0) (2023a) and IBM SPSS Amos (Version 30.0) (2023b). Both software packages and version numbers are cited in the reference list.
Results
Results are presented in three stages: Internal consistency (Cronbach's α), model fit indices, and factor loadings with construct reliability (CR), convergent, and discriminant validity.
Internal Consistency Reliability
Cronbach's alpha was calculated for the DASS-21 and six short forms (see Table 3). All scales demonstrated acceptable reliability (α ≥ .70), with most ≥ .80. Among the short forms, the DASS-12a and DASS-10 consistently showed the strongest reliability across all subscales (α ≥ .80), while the DASS-9b was comparatively weaker for anxiety (.73) and stress (.73).
Model Fit Indices
Confirmatory factor analyses were conducted to evaluate the model fit of the DASS-21 and its six abbreviated forms. Each model was evaluated both before and after being modified according to modification indices. The fit statistics for all models are presented in Table 4.
Model Fit Indices for the DASS-21 and Selected Short Forms Before and After Modification.
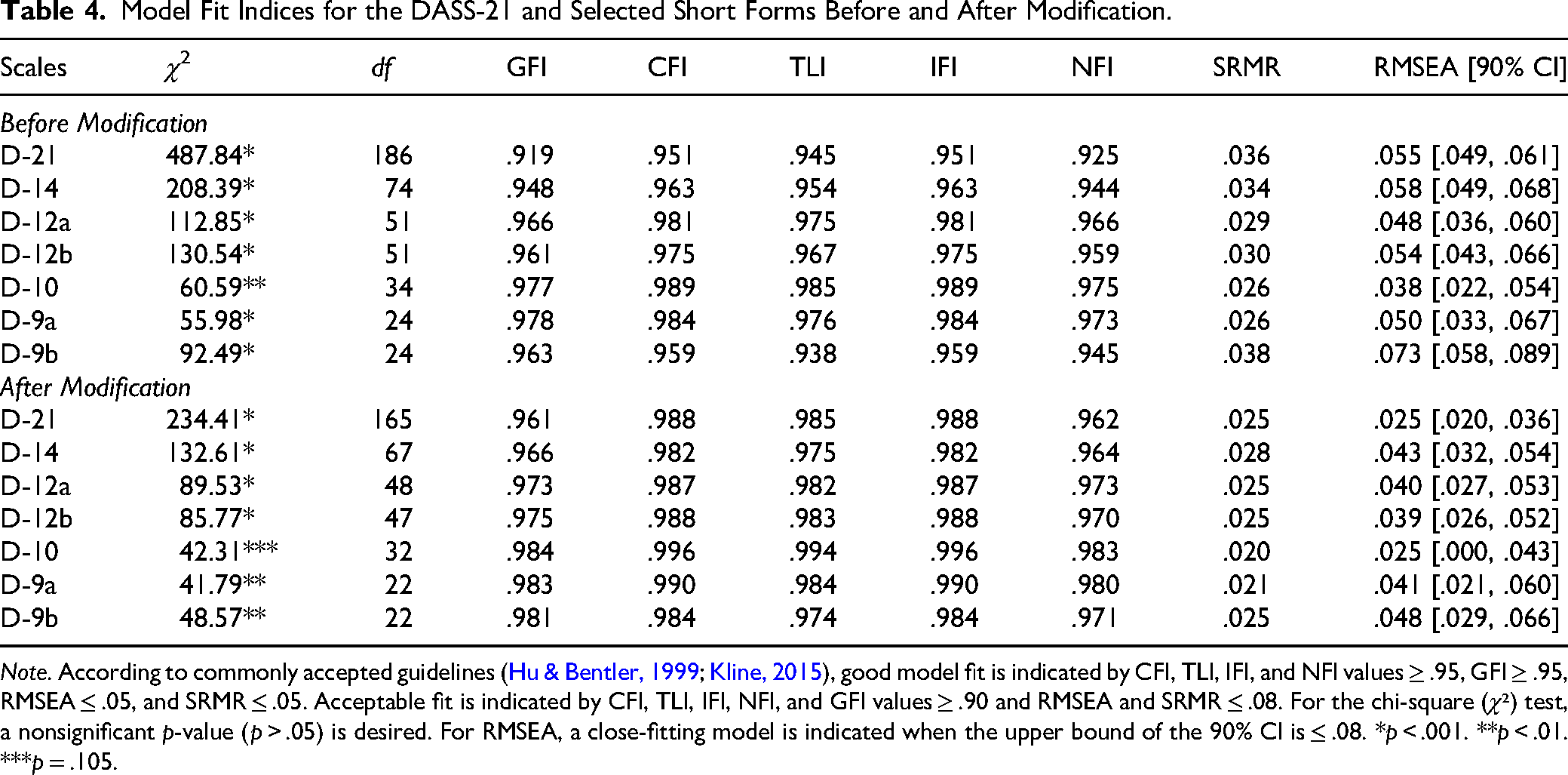
Note. According to commonly accepted guidelines (Hu & Bentler, 1999; Kline, 2015), good model fit is indicated by CFI, TLI, IFI, and NFI values ≥ .95, GFI ≥ .95, RMSEA ≤ .05, and SRMR ≤ .05. Acceptable fit is indicated by CFI, TLI, IFI, NFI, and GFI values ≥ .90 and RMSEA and SRMR ≤ .08. For the chi-square (χ²) test, a nonsignificant p-value (p > .05) is desired. For RMSEA, a close-fitting model is indicated when the upper bound of the 90% CI is ≤ .08. *p < .001. **p < .01. ***p = .105.
Prior to modification, the initial models demonstrated a range of fit from acceptable to good. Several short forms, notably the DASS-12a and DASS-10, showed strong initial fit, meeting the conventional criteria for good fit on indices such as CFI, TLI, and RMSEA. Other models, such as the D-9b, showed a weaker initial fit, with a TLI value below .95 and an RMSEA above .07.
Following the application of modification indices, primarily through correlating error terms, all seven models showed a substantial improvement. After modification, every model met the criteria for good to excellent model fit according to the guidelines presented in the table note. The two-factor D-10 model emerged as the strongest performer, demonstrating outstanding fit indices (e.g., CFI = .996, RMSEA = .025) and was the only model to achieve a non-significant chi-square value (χ²(32) = 42.31, p = .105). The precision of this fit was underscored by the narrow 90% confidence interval for RMSEA [.000, .043], with its upper bound well below the .05 threshold for good fit. Other short forms, including the DASS-12a, D-12b, and D-9a, also provided an excellent fit to the data, with all their key indices well within the recommended ranges for good fit and their RMSEA confidence intervals indicating a high degree of precision.
Factor Loadings, Construct Reliability (CR), and Convergent and Discriminant Validity
All standardized factor loadings exceeded .50, ranging from .59 to .84. The vast majority of construct reliability (CR) values were ≥.70, indicating acceptable internal consistency (Fornell & Larcker, 1981; Hair et al., 2019), with only minor shortfalls for the anxiety (.68) and stress (.69) subscales in the D-9b model. Table 5 provides details on both convergent and discriminant validity. Convergent validity was generally supported; DASS-12a, D-12b, and D-9a demonstrated strong convergent validity, with all their AVE values exceeding the .50 threshold. In contrast, marginal shortfalls were observed for the anxiety (.49) and stress (.47) subscales in DASS-14, and for both the anxiety (.42) and stress (.43) subscales in DASS-9b. In the second-order model (DASS-10), the first-order anxiety–stress factor fell slightly below the AVE threshold (.48). However, the overarching second-order distress factor demonstrated excellent convergent validity (AVE = .85) and internal consistency (CR = .92), supporting its robustness as a measure of general psychological distress.
Convergent and Discriminant Validity of DASS-21 Short Forms.
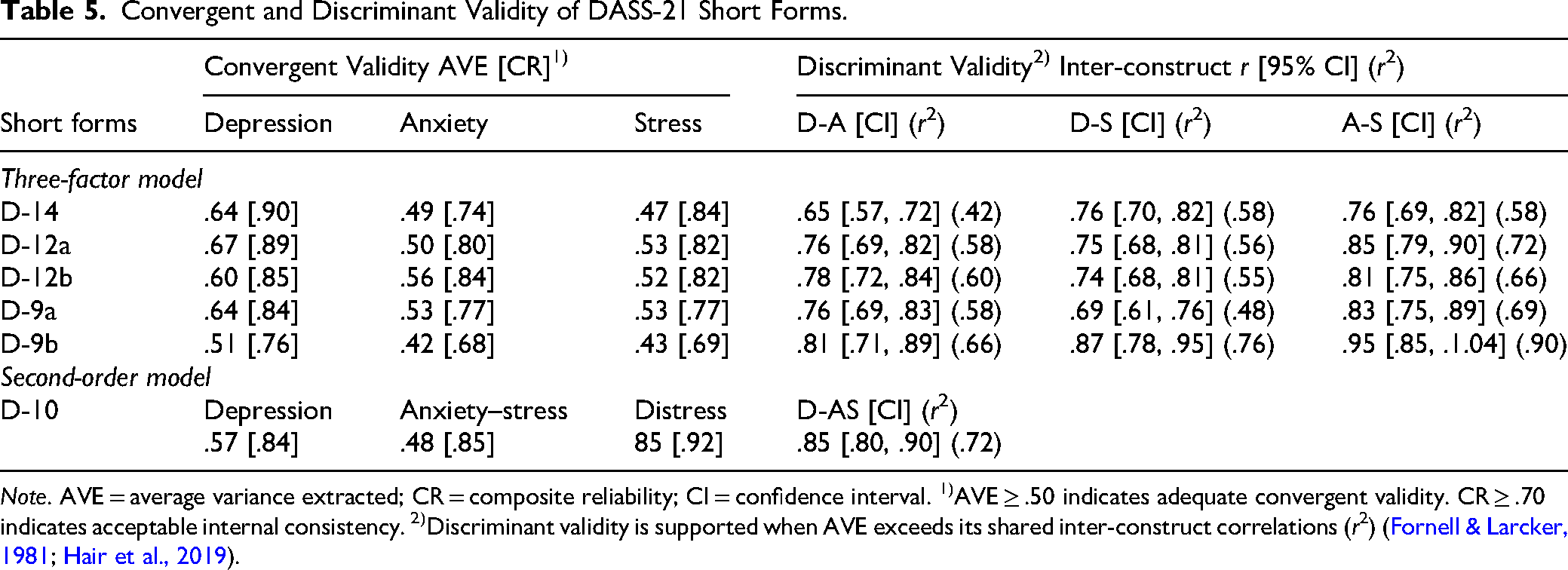
Note. AVE = average variance extracted; CR = composite reliability; CI = confidence interval. 1)AVE ≥ .50 indicates adequate convergent validity. CR ≥ .70 indicates acceptable internal consistency. 2)Discriminant validity is supported when AVE exceeds its shared inter-construct correlations (r2) (Fornell & Larcker, 1981; Hair et al., 2019).
With respect to discriminant validity, the interfactor correlations were consistently high across all models, and their precise 95% confidence intervals provided strong evidence of empirical overlap. Consequently, the Fornell–Larcker criterion was generally not met, with only two pairs across all models meeting the strict test for distinctness: the depression–anxiety pair in DASS-14 and the depression–stress pair in D-9a. In all other cases, the shared variance between constructs exceeded the AVE of at least one of the factors. For example, in the DASS-12a, the shared variance between anxiety and stress (r = .85, r² = .72) substantially exceeded the AVEs of both anxiety (.50) and stress (.53). Similar patters were observed across the other three-factor models, with only a single pair in the DASS-14 (depression and anxiety) meeting the criterion. The second-order DASS-10 model also failed to demonstrate discriminant validity, as the shared variance between its depression and anxiety–stress factors (r = .85, r² = .72) was considerably higher than the AVE for either factor (.57 and .48, respectively). Taken together, these findings strongly indicate that the constructs, particularly anxiety and stress, were not empirically distinct in this sample.
Discussion and Applications to Practice
This study evaluated the psychometric properties of six abbreviated versions of the DASS-21 in a clinical sample of adult male survivors of sexual abuse. Across all models, internal consistency was acceptable, and convergent validity received at least partial support. However, discriminant validity—particularly between anxiety and stress—was consistently limited. Despite these challenges, two short forms—the DASS-12a and DASS-10—emerged as the most psychometrically robust options. Both exhibited strong reliability and excellent model fit, but they offer distinct strengths: the DASS-12a demonstrated the cleanest profile of convergent validity across three factors, while the D-10 achieved a statistically superior model fit that pragmatically addresses the overlap between anxiety and stress. The DASS-10, while collapsing anxiety and stress into a single factor, maintained excellent internal consistency, a finding consistent with prior evidence of empirical overlap between these constructs in the broader DASS literature (Antony et al., 1998; Zanon et al., 2021). For clinical purposes, the DASS-10 should be interpreted as providing two indices: a Depression score and a combined anxiety–stress score, which may serve as an indicator of generalized arousal or physiological tension.
Convergent validity was generally supported. The DASS-12a, D-12b, and D-9a demonstrated strong convergent validity, with all their AVE values exceeding the .50 threshold. In contrast, marginal shortfalls were observed for the anxiety (.49) and stress (.47) subscales in DASS-14, and for both the anxiety (.42) and stress (.43) subscales in D-9b. Importantly, convergent validity was evaluated only through internal CFA-based indicators; external validation against measures such as the PHQ-9, GAD-7, or BDI will be necessary to confirm these results.
Discriminant validity, however, presented a consistent challenge. The inter-factor correlations were consistently high across all models, and their precise 95% confidence intervals provided strong evidence of empirical overlap. Consequently, the Fornell–Larcker criterion was generally not met, with only two pairs across all models meeting the strict test for distinctness: the depression–anxiety pair in DASS-14 and the depression–stress pair in D-9a. These findings align with prior research showing that anxiety and stress are difficult to disentangle empirically (Osman et al., 2014; Zanon et al., 2021). In trauma-exposed populations, overlap between the DASS anxiety and stress subscales may reflect co-activation of autonomic arousal and tension/irritability (Clark & Watson, 1991; Henry & Crawford, 2005), and trauma-affected men often show elevated internalizing distress (Easton, 2014). Thus, while the lack of discriminant validity represents a psychometric limitation, it also reflects the lived symptom experience of survivors, where trauma responses often transcend conventional diagnostic boundaries. For practice, this indicates that anxiety and stress subscales should be interpreted with caution, and in many cases, a combined distress index (as represented in the DASS-10) may provide a more pragmatic reflection of client functioning.
Taken together, these findings support the DASS-12a and DASS-10 as promising short forms for trauma-affected populations. The DASS-12a preserves the original three-factor structure of the DASS and is well-suited for contexts where distinguishing between depression, anxiety, and stress is clinically meaningful, particularly given its strong convergent validity for all three distinct factors. In contrast, the DASS-10 offers a statistically superior and time-efficient alternative, particularly useful in frontline or resource-limited settings where rapid screening for a single, robust measure of general distress is needed. Its brevity makes it especially appropriate for digital applications, such as electronic intake systems and mobile mental health platforms, which rely on real-time scoring and feedback to support timely intervention (Barkham et al., 2023). Integrating these short forms into routine outcome monitoring (ROM) can enhance trauma-informed care by reducing client burden while supporting practitioners in tracking symptoms over time.
Several limitations should be acknowledged. This study focused exclusively on adult male survivors of sexual abuse in Ontario, Canada. While this population is clinically significant and underrepresented in research, the absence of female and gender-diverse participants restricts broader gender-based assessment implications. Accordingly, this study cannot directly address gender comparisons in scale functioning; future research should examine whether abbreviated DASS forms perform equivalently across diverse gender identities. Moreover, most participants identified as White and English-speaking, with only a small proportion identifying as Indigenous. These demographics reflect the client base of the participating agencies but limit the generalizability of findings to other cultural or geographic groups. Race and ethnicity data were also incomplete, restricting a fuller examination of cultural variation in symptom presentation. In line with equity-informed frameworks, race and ethnicity are best understood as proxies for broader social and structural determinants—including systemic racism and economic marginalization—rather than as essentialist categories.
Another limitation concerns sample attrition. Although the original database contained records for 2,986 clients, only 534 cases met inclusion criteria for this analysis. This substantial reduction occurred because the dataset was not designed for research but rather compiled for administrative and service delivery purposes between January 5, 2010, and May 17, 2022. As a result, the dataset contained considerable missingness, and only participants with complete DASS data could be included. While the final analytic sample remains clinically meaningful, attrition may have introduced bias by disproportionately excluding clients with incomplete records. Future studies should employ prospectively designed research protocols to minimize missingness and enhance representativeness.
Methodological considerations also warrant caution. The cross-sectional design precluded assessment of test–retest reliability and sensitivity to change; longitudinal studies are needed to evaluate stability and responsiveness in applied settings. Convergent validity was assessed using CFA-based indices only, without external validation against independent instruments. Furthermore, cutoffs for indices such as RMSEA and AVE remain debated in the literature and should be interpreted cautiously. Finally, the recurring challenge of discriminant validity, especially between anxiety and stress, highlights the need for alternative modeling strategies, including bifactor or network models, to capture the dimensional nature of distress more precisely.
Applications to practice flow directly from these findings. Both the DASS-12a and DASS-10 offer brief, psychometrically supported options for identifying distress among male survivors. The DASS-12a is most useful in contexts requiring differentiation among depression, anxiety, and stress, such as comprehensive clinical assessments or detailed treatment planning. The DASS-10, by contrast, is particularly valuable for efficient screening in frontline practice, including crisis intake, community-based services, and digital platforms. Its brevity may also reduce barriers to disclosure among male survivors who experience stigma and socialized constraints on emotional expression (Javaid, 2015). In practice, the use of these tools can support trauma-informed engagement by offering less confrontational entry points into care. Training for practitioners will be essential to ensure accurate interpretation, particularly given that many are more familiar with the DASS-21.
Future research should move beyond replication to address key gaps. In addition to validating these short forms in larger and more diverse samples, studies should evaluate their longitudinal stability, sensitivity to change during treatment, and predictive utility for trauma recovery outcomes. Research should also explore whether distinct clinical cutoffs are required across gender and cultural groups and test advanced modeling frameworks (e.g., bifactor or network analyses) to clarify the structure of distress. Such efforts will ensure that abbreviated DASS forms evolve into both scientifically rigorous and practically responsive tools that can advance social work research and strengthen equitable, trauma-informed practice.
Footnotes
Author Note
Sung Hyun Yun is now at School of Social Work, University of Windsor. The author has no known conflict of interest to disclose. Data are not publicly available due to REB-approved ethical restrictions. This study involved secondary analysis of de-identified data previously collected by partnering agencies. This study is approved by the University of Windsor Research Ethics Board (# 12-080).###
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Canadian Institutes of Health Research (CIHR; #392373) and Social Sciences and Humanities Research Council (SSHRC; #892-2023-3003 and #890-2024-0022).
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.