
Abstract
Purpose
This study examined the mediating role of resilience and living in care experiences between risk exposure (victimization by community and adverse childhood experiences) and psychosocial outcomes (housing instability, delinquency, and post-traumatic stress reactions) for youth receiving child welfare and community services.
Method
Two hundred and fifty-one youths (14–19 years old) who are receiving interventions from the Department of Community Services in Nova Scotia, Canada, were recruited. Multiple measures were administered to the youth.
Results and conclusion
Resilience and experiences of living in care significantly mediated the relationship between risk factors and outcomes, with youth demographic characteristics influencing the pattern of these relationships. Findings suggested that resilience and living in care experiences could reduce the effects of risk factors on psychosocial outcomes. These findings demonstrate a role for Child Welfare agencies in promoting youth access to the resilience-enabling resources necessary to sustain well-being.
Keywords
Introduction
Existing evidence-based research reveals that youth experience various developmental challenges even when they grow up in normative and benign family and community systems (Dimitrova & Wiium, 2021; Griesel & Hovinen, 2022). Experiencing heightened exposure to risk factors (e.g., victimization by community [VC] and adverse childhood experiences [ACEs]) may make these challenges even more complicated and create negative psychosocial outcomes such as delinquency (Leban & Gibson, 2020), housing instability (Davis et al., 2019; Heerde et al., 2020), and post-traumatic stress reactions (Anastas et al., 2021; Karatzias et al., 2020). Recently, an increasing number of studies have focused on the relationship between risk factors and these outcomes (Anastas et al., 2021; Garrido et al., 2018; Middleton et al., 2022; Rebbe et al., 2017) as well as the role of protective factors such as resilience (Herbers et al., 2020). Several studies have also addressed the impact of adolescents’ demographic characteristics such as age (Frederick et al., 2021), education (Alberton et al., 2020), gender (Crawford et al., 2015), sexual orientation (Ecker et al., 2020), or race (Forge et al., 2018) on these outcomes, most often with a narrow focus on the experiences of a homogeneous sample of youth who share a common set of risk exposures (LaBrenz et al., 2021).
Despite a body of literature exploring the role of protective factors (e.g., resilience) in reducing these outcomes for youth (Cronley & Evans, 2017; Grattan et al., 2022; Herbers et al., 2020), the relationships between risk and protective factors and outcomes for youth receiving community and child welfare services (CWS) across Canada, particularly in Nova Scotia, have not been studied. Moreover, the mediating roles of resilience and living in care experiences have not been well-studied for youth who are clients of community and child protection programs. Thus, this study aims to investigate the mediating roles of resilience and living in care experiences on risk factors and psychosocial outcomes for youth receiving community and CWS in Nova Scotia, Canada.
Background and Relevant Studies
Out of a total population of almost 40 million in 2022, 5.45% (N = 2,124,972) of Canadians are between 15 and 19 years of age (Statistics Canada, 2022). National surveys such as the General Social Survey—Canadians’ Safety (Victimization), the Population Census (Dionne et al., 2023), and the Canadian Housing Survey have been used by organizations such as the Children's Aid Foundation of Canada (CAFC, 2023) to estimate that approximately 300,000 children and youth are living with vulnerable or unstable families or experiencing different types of adversities and maltreatment that result in them requiring protection from a provincial or federal government agency. This includes the Department of Community Services (DCS) in Nova Scotia, a province of one million people in eastern Canada.
Conducting a thorough literature review on children and youth receiving CWS, Trocme et al. (2019) reported that over 230,000 child maltreatment investigations are conducted every year across Canada. At any one time, an estimated 59,000 children and youth are under a government-mandated protection order (CAFC, 2023). Furthermore, it was estimated that in 2019 the rate of children and youth who received CWS across Canada was between 7.46 and 8.16 per 1,000 (Saint-Girons et al., 2019).
Each province in Canada has the authority to administer community and CWS at its own provincial level. Nova Scotia's DCS provides children and youth with welfare services through 21 local child welfare offices located in each county. CWS for indigenous youth are also provided by Mi’kmaw Family and Children's Services for the 13 First Nations reservations in the province (Tremblett et al., 2021).
Services include but are not limited to individual and family therapy/counseling, clinical assessments, providing accommodations (e.g., foster families, extended family, or institutional settings), financial services, and educational support. Children and youth who have experienced or been at risk of a variety of ACEs (e.g., unstable families, parents with mental disorders, physical or sexual abuse or any other maltreatment, VC, etc.) are potential clients for these services (Tremblett et al., 2021; Trocme et al., 2019). In contrast to national averages, the rate of Nova Scotian children and youth who were placed in out-of-home care or used CWS was 5.64 per 1,000 children in 2019 (Black et al., 2022; Tremblett et al., 2021). However, it is estimated that a significant number of young people aged 15 and older in Nova Scotia are unsheltered or hidden homeless (2.9 and 17.3 per 1,000 people in 2022, respectively; Dionne et al., 2023; Uppal, 2022).
Though a large number of children receive services from government agencies in Canada, remarkably little is known about the impact on long-term developmental outcomes for children who are clients of DCS (Trocme et al., 2019). This limitation stems from scant attention to protective factors that are intended to enhance young people's resilience, such as living in care when under a child protection mandate. Indeed, the role of positive experiences (such as having a single caring person, having a stable living situation, and feeling like a part of a family) while living in care (e.g., foster care) and how these experiences prevent youth from later homelessness has been identified as an area of research requiring further study if housing stability after programming ends is to be improved for youth needing protection (Montgomery et al., 2006; Nunez et al., 2022). Given these limitations of the research, little is known about the factors that might help to prevent youth from experiencing precarious housing later in life or to buffer its covariates (post-traumatic stress reactions and delinquent behaviors). This has occurred despite the diverse literature that has shown that resilience has a positive role in buffering or reducing delinquent behaviors (Hodgkinson et al., 2021), post-traumatic stress reaction (PTSR; Cameranesi et al., 2023), and psychological problems in youth who are living in other challenging environments (Ungar & Hadfield, 2019) beyond those involved with CWS.
For this reason, the current study investigates the links between three outcomes (homelessness, delinquency, and PTSR) and the potential mediating role of time spent in care and resilience for a population of youth with histories of involvement with community and CWS in one Canadian province.
Links Between Outcomes (Housing Stability/Instability, Delinquency, and PTSR)
Apart from the types of housing instability (homelessness), worldwide studies show that homeless youth are over-represented among populations that engage in delinquent behaviors, such as drug dealing (Díaz & Patacchini, 2023), violent crime (Lussier et al., 2023), gang activity (Paredes & Navarrete, 2023), and trading sex for resources (O’Brien et al., 2022). In one study, Cutuli et al. (2020) found youth homelessness to be more pervasive and associated with delinquent behaviors than expected, with youth who experience homelessness being 196% more likely to struggle with alcohol addiction, 275% more likely to have used hard drugs, 115% more likely to report suicidality, and 95% more likely to engage in risky sexual behavior. Although the effect size of the relationship between youth homelessness and crimes (delinquent behaviors) varies across communities, both have a significant and positive correlation (Ee & Zhang, 2022). These associations were also verified for youth housing instability and PTSR (Jozefowicz-Simbeni & Israel, 2006). PTSR in children and youth is characterized by symptoms such as a sense of re-experiencing current events or intrusive memories of traumatic events (e.g., nightmares), hyperarousal (e.g., anxiety, irritability, and sleep difficulties), and avoidance of potential triggers (Maercker et al., 2022). These symptoms are typically experienced as comorbidities with homelessness and some types of delinquent behaviors, such as substance use (Cutuli et al., 2020; Davis et al., 2019).
Using symptom-driven and experience-driven models to examine how PTSR-related symptoms, substance use, and homelessness are related, Davis et al. (2019) found a strong association between these three constructs. That is the more days of homelessness, the higher the level of PTSR reported by youth. PTSR and delinquency were considered either the consequences of homelessness (Smith-Grant et al., 2022) or as the outcomes of psychosocial risk factors that occurred concurrently with homelessness (Barnes et al., 2021; Fallon et al., 2021; Gaetz et al., 2016). This can be observed in Smith-Grant et al.’s (2022) study where they found that youth who experienced homelessness were more likely to misuse pain medication prescriptions than stably housed individuals. They interpreted substance use as a consequence of housing instability. In this interpretation, there is a path from some risk factors to homelessness and from homelessness to other psychosocial problems such as substance use or PTSR. Although PTSR, delinquency, and homelessness have reciprocal relationships (Czaderny, 2020; Grattan et al., 2022), they may also be affected by other risk factors such as ACEs (Davis et al., 2019; Heerde et al., 2020; Middleton et al., 2022; Murran & Brady, 2022) and VC (Seon et al., 2022).
Links Between Risk Factors and Outcomes
Children and youth who receive CWS may have experienced different types of risk factors such as ACEs (Middleton et al., 2022) and VC (Seon et al., 2022), which could contribute to negative psychosocial outcomes such as PTSR (Davis et al., 2019), delinquency (Grattan et al., 2022), and housing instability ( Middleton et al., 2022). Being victimized by family, peers, or strangers in the community is one of the prevalent risk factors experienced by youth in Canada (Sutton, 2021). In 2019, children and youth reported being victimized by family members and non-family members at a rate of 311 and 659 per 100,000 children, respectively (Statistics Canada, 2023). The rate of young people in Nova Scotia which is the focus of the current study is approximately the same as for the rest of Canada (Statistics Canada, 2023).
Victimized children and youth may also experience housing instability as Flatley et al. (2022) demonstrated. In their study, they found that victimization was closely associated with different types of youth homelessness, such as living in shelters, relatives’ houses, campgrounds, or living with friends. Likewise, Fischer (1992) demonstrated that different types of victimization can directly lead to homelessness. That is, victimization can be considered one of the causes of homelessness when research assesses retrospective exposure to victimization. These risk factors are correlated with covariates of homelessness such as delinquency (Leban & Gibson, 2020) and PTSR (Anastas et al., 2021; Karatzias et al., 2020).
Experiencing victimization is also correlated with ACEs (Seon et al., 2022). This association was verified by other evidence-based studies in which ACEs were associated with various types of VC or social victimization, such as peer victimization (e.g., malicious gossip, friendship manipulation, and verbal and non-verbal exclusion by peers; Afifi et al., 2020; Rosen et al., 2017), cyberbullying (Nagata et al., 2023), sexual victimization (Thompson & Kingree, 2022), and physical and verbal victimization (Fagan, 2022). ACEs include a diverse range of childhood experiences linked with several outcomes, including mental health problems, delinquent behaviors, and experiences of homelessness later in life. With regard to youth who experience homelessness, ACEs include parental divorce or maltreatment by a caregiver, parents’ mental health problems, household incarceration, physical and sexual abuse, being emotionally ignored, neglected, and morally ridiculed during childhood (Afifi et al., 2020; Edalati et al., 2020; Karatzias et al., 2020). Generally, ACEs are a widespread risk factor that contributes to a higher likelihood of homelessness (Middleton et al., 2022), post-traumatic stress disorder (PTSD) symptoms (Anastas et al., 2021; Karatzias et al., 2020), and delinquent behaviors (Leban & Gibson, 2020).
Apart from the experience of homelessness (Barnes et al., 2021), youth who encounter complex adversity during their childhood are more likely to report some engagement in delinquent behaviors, such as criminal behavior, substance use, and risky sexual behaviors (Garrido et al., 2018; Rebbe et al., 2017). These behaviors are known to be prevalent among youth involved in CWS; however, they are not uniformly distributed across all CWS-involved youth (Rebbe et al., 2017).
Although the effects of risk factors (e.g., ACEs and VC) on these outcomes (homelessness, PTSR, and delinquency) have been partially verified by previous studies (Anastas et al., 2021; Karatzias et al., 2020; Leban & Gibson, 2020; Middleton et al., 2022), the mediating roles of resilience and living in care experiences have not been well-examined.
Mediating Role of Living in Care and Resilience
For our purposes here, a youth's experience of living in care refers to positive and negative experiences that children or youth have had during live-in caregiver programs, foster homes, or a private household provided by the government (e.g., CWS) or other non-profit organizations. Such programs aim to provide youth with positive, protective, and authentic experiences, facilitating the transition out of CWS. A systematic review by Montgomery et al. (2006) demonstrated that some living in care programs had protective effects on youth. These protective effects were mostly related to educational attainment, employment, housing stability, health, and other life skills. Considering that living in care is intended to create a stable placement for youth and provide them with access to protective and promotive factors and processes (Ungar & Theron, 2019), it is surprising that placement outcomes are so inconsistent.
Using an ethnographic methodology, Cudjoe et al. (2022) demonstrated that living in care programs such as foster care had difficulties providing care leavers with relevant and tangible support. Likewise, in a cross-sectional study, Stenason and Romano (2023) described how instability during living in care could create negative experiences for youth. Using hierarchical regression analysis to explore the data of 1,624 Canadian youth living in care, Stenason and Romano (2023) showed that caregivers and youth had unsatisfactory experiences when there were placement changes. They also found that youth showed more significant conduct problems, peer problems, and fewer internal assets (e.g., commitment to learning, positive values, and positive identity) when they moved placements. Burge (2022), meanwhile, found that living in care was associated with positive outcomes, but related those experiences to at least two factors: a safe and stable home and knowing one's history.
Although positive experiences during living in care could be considered a protective factor, resilience is a dynamic process through which youth navigate their way to psychosocial resources that buffer risk factors, maintain a sense of purpose and values in the face of adversity, and potentiate positive development under stress (Ungar, 2011). In line with Ungar's (2011) socioecological theory of resilience, Oppong Asante (2019) conducted a qualitative study of Ghanaian youth and found that three resources could explain the resilience of homeless youth. These resources were intrapersonal (e.g., humor and spirituality), interpersonal (e.g., friendship and social interactive activities), and socio-cultural (e.g., cultural norms, community-based care, and support). Using a similar methodology, Frederick et al. (2021) found that for youth in the United States, resources such as family empathy, skills mastery, and community relationships could enhance resilience and consequently buffer people's housing instability and its covariates. Finally, a systematic review of the literature on youth homelessness by Nunez et al. (2022) revealed that resilience was highly significant in explaining how youth deal with risk factors and complete a successful transition out of foster care into independent living.
Current Study
The main objective of the present study is to assess the associations between VC, ACEs, and the outcomes of housing stability/instability, delinquency, and PTSR when the mediating roles of resilience and living in care experiences are taken into account. This mediation study was implemented with Nova Scotian youth who have received community and/or CWS. Although the function of demographic variables (e.g., age, gender, race, etc.) are controlled in this study, the second objective is to investigate whether the exogenous and endogenous variables vary by the demographic characteristics of youth who receive services from DCS.
Method
Ethical Approval and Considerations
This research received ethical approval from the Nova Scotia DCS and Dalhousie University based on the adherence to the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans (TCPS 2, 2022) in Canada, which is a joint policy of Canada's three federal research agencies. After the detailed explanation of the research objectives to participants, their right to withdraw, the risks and benefits of the study were clarified. Consent to participate in the study was obtained by trained research assistants who engaged with the youth alone if they were at least 16 years old or the youth and a legal guardian if the youth was under the age of 16.
Study Design
This study was a cross-sectional design using path analysis to examine the links between the above-noted risk factors, mediating variables, and outcomes. Analogous to this research, many evidence-based studies have used path analysis within cross-sectional design to explore the significant associations between predictors and endogenous variables (see, e.g., de la Fuente, 2021; Kim et al., 2019; Melendro et al., 2020; Yeh & Waters, 2021).
Sample and Sampling
As Figure 1 shows, all youth (N = 653) between the ages of 14 and 19 receiving DCS services (e.g., foster homes, social assistance, voluntary supervision orders, kinship care, family support services, etc.) in the province of Nova Scotia during February 2022 were identified by DCS. Youth were read a short script and asked if they were willing to be nominated for the study. Youth who agreed were asked to share their contact information which was then forwarded to a member of the research team who contacted the youth to explain the study in more detail and seek their consent to participate. DCS staff were not informed which youth agreed to participate in the research. Youth under the age of 16 required the consent of a legal guardian such as a parent, caregiver, or in some instances, a social worker, when the child was under the care of the province (only in those instances where the guardian was the social worker would a member of the DCS staff knows that the child had agreed to participate in the study). Three hundred and sixty-five agreed to be contacted by a member of the research team to hear more about the study. Of the youth who were contacted by the research team, 258 agreed to be interviewed (Figure 1). Seven participants did not complete enough questions on the survey to be included in the final analysis. Participants were administered a survey by phone typically lasting between 45 and 90 min. A stipend (e.g., gift card) was provided in recognition of the youth's time spent on the research. Anonymized data were stored on a secure computerized platform for analysis.
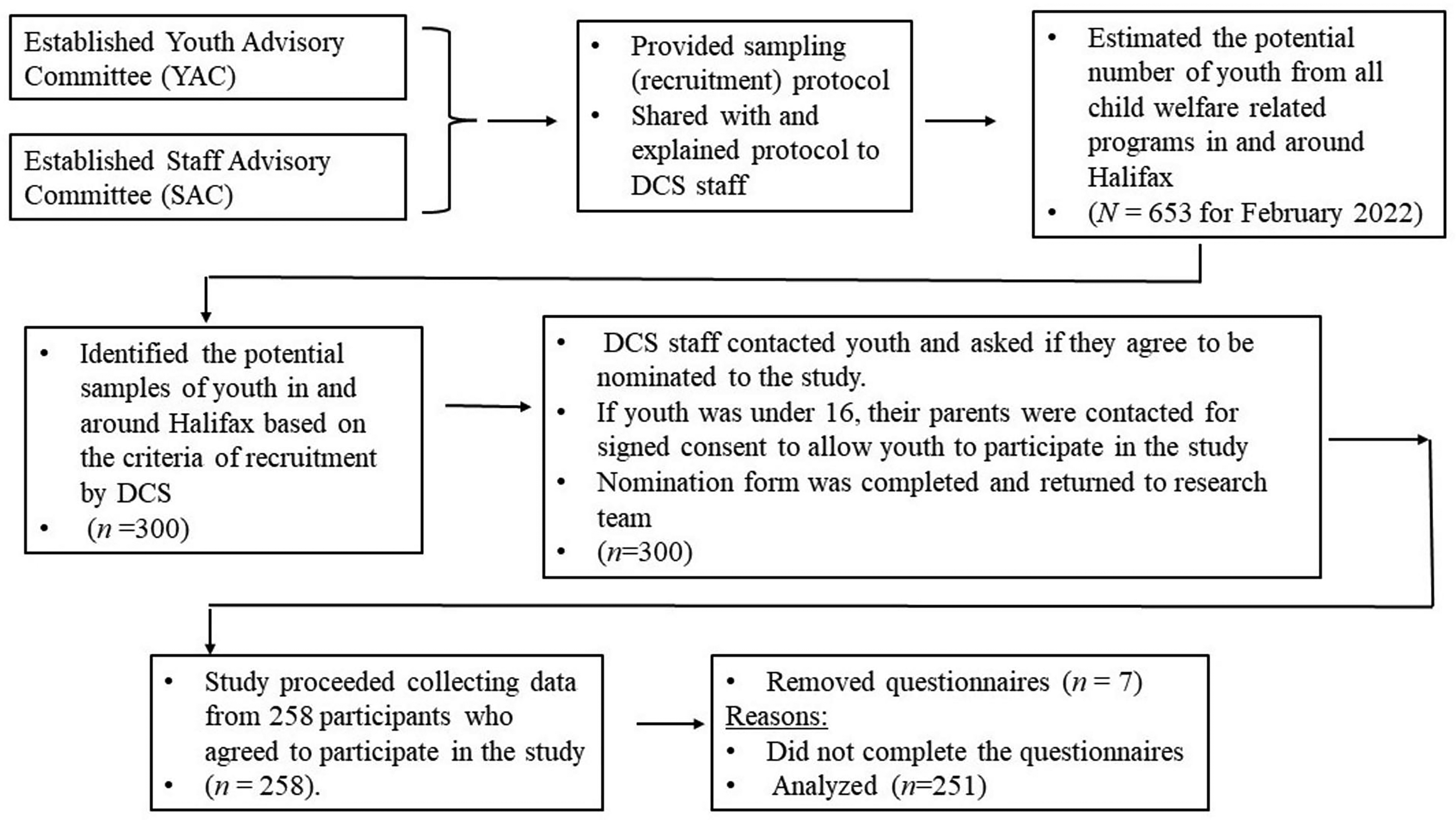
Samples recruitment process.
Participants’ Characteristics
Of the 251 participants, 83 (32%) were males, 144 (58%) were females, 23 (9%) were non-binary persons, and one participant declined to identify their gender. Ages ranged between 14 and 19 years old (M = 16.46, SD = 1.42), and were clustered into three categories for the purpose of analysis: 14–15 (27%, N = 70), 16–17 (43%, N = 107), and 18 and 19 (30%, N = 74). With regard to racial identity, 171 (69%) of the participants were white, 28 (11%) identified as mixed race, 13 (5%) black, 29 (12%) indigenous, and the remainder identified themselves as Middle Eastern, Latin American, and South Asian. At the time of the survey, 77% of the participants (N = 191) attended school. As per place of residence, 39% were residing in apartments with their families, 17% were living in foster care, 7% were in houses provided by child and youth caring programs, 6% were living with their friends or “couch surfing,” 6% were in shelters, 3% were in kinship placement, 3% were in boarding arrangements, 3% were in transitional housing, 3% had a semi-independent living arrangement, and 4% were living with relatives. The rest of the sample had a varied list of other housing arrangements, such as living on the street and in cars, or did not answer (8%).
Measures
Measures covered four topic areas: demographic characteristics, risks, mediating factors (resilience), and outcomes.
Demographic Measure
Demographic Scale: Participants were asked their age, gender (male, female, and non-binary), race (e.g., White, Mixed Race, Black, Indigenous, etc.), sexual orientation (e.g., straight, heterosexual, bisexual, etc.), education (e.g., attending educational classes or not participating in any educational classes), and their living arrangements.
Risk Factors Measures
VC Scale: The scale includes three items that measure the degree to which youth had experienced social victimization over the last 12-month period (e.g., During the past year, I have been chased by a group, gangs, or individuals). The items were selected from a related scale originally developed by Richters and Martinez (1993). Responses regarding youth experiences of victimization ranged from 1 (none) to 5 (10 or more times). The range of total scores was between 5 and 15, with higher scores indicating more victimization. The scale's internal consistency in the current study was α = 0.73, M = 5.24, and SD=2.64.
ACE Scale (ACES): The version used in this study was developed by Finkelhor et al. (2015) to measure the existence of emotional and moral maltreatment, physical and sexual abuse that youth experienced during their childhood (e.g., “At any time in your [childhood] life, did a parent, caregiver or another person ever slap you repeatedly, beat you, or otherwise attack or harm you?”). The internal consistency of the scale in the current study was α = 0.78, M = 2.46, SD = 1.89.
Mediating Factors Measures
Child and Youth Resilience Measure (CYRM-R): The scale was originally developed to assess culturally grounded experiences of resilience in youth aged 11–23 (Ungar et al., 2008; Ungar & Liebenberg, 2005, 2011). The scale measures the capacity of youth to navigate to the different psychological, social, cultural, and physical resources to maintain their well-being. The CYRM-R (Jefferies et al., 2019), a 17-item version of the measure, was used in this research. Questions included items such as “I feel supported by my friends,” and “I know how to behave in different social situations.” The measure uses a Likert scale with five options (e.g., “Not at all,” “A little,” “Somewhat,” “Quite a bit,” and “A lot”). Internal consistency using Cronbach's Alpha was satisfactory α = 0.84, M = 53.87, and SD = 9.11.
Living in Care Experiences Scale: Living in care experiences (positive or negative) were measured using a 7-item questionnaire with a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). The range of scores was between 7 and 35, with higher scores indicating more positive experiences. The scale was developed for this study following a literature review of youth experiences receiving different support for their social needs while living in care. Typical questions included “I felt like people [caregivers] cared for me” and “My caregiver(s) supported my spiritual needs (e.g., finding a higher power or life purpose).” Internal consistency was very good with Cronbach's Alpha α = 0.91, M = 26.15, and, SD = 7.49.
Outcomes Measures
Childhood Post-Traumatic Stress Reaction Scale (CPTSRS-5): Five items of the CPTSRS-5, originally developed by Frederick (1985a, 1985b), were used to assess youth's recurrent emotional and behavioral reactions to past traumatic events. Using a 5-point Likert scale from 1 (never) to 5 (most of the time), the measure focused on how frequently these reactions have recurred during the past month. Samples of items included “Do you get scared or afraid because you think about bad things that have happened to you?” and “Can you talk about bad things that have happened to you and how they made you feel?” The total score ranged from 5 to 25. The original scale had satisfactory convergent validity as it was highly correspondent with actual clinical diagnosis based on interviews (r = 0.91; Pynoos et al., 1993). Also, through a pilot study based on PTSD symptoms, Lack et al. (2008) validated this scale and reported high internal consistency (α = 0.84) and moderate 2-week test–retest consistency (r = 0.62). The internal consistency of the adapted Post-Traumatic Stress Reaction Scale-5 in the current research was acceptable α = 0.77, M =10.95, and SD = 3.96.
Delinquency Scale: Through a literature review of current delinquency scales (e.g., Bountress et al., 2021: Davis et al., 2019; Geldhof et al., 2014), a 6-item self-report scale was developed to measure the frequency of delinquent behaviors (e.g., substance use; being convicted of a crime). The total score ranged from 6 to 30 based on a 5-point Likert scale from 1 (never) to 5 (most of the time), with higher scores indicating more frequent delinquent behaviors. Items included “How frequently have you used opioid drugs (e.g., fentanyl, valium, heroin)?” and “How many times have you been convicted as a youth of a criminal offence?” The scale's internal consistency was good α = 0.73, M = 9.06, and SD = 4.24.
Housing Stability/Instability Scale: To measure housing instability, first, we considered the current definitions of “housing stability/instability” (Frederick et al., 2021) and “homelessness” (Cutuli et al., 2020; Forchuk et al., 2022; Heerde et al., 2020; Smith-Grant et al., 2022). Next, three conditions (current residency, frequency of changing living arrangements, and total times of being homeless during life) were determined and used to develop a scale to measure youth housing instability (homelessness). Using a 4-point Likert scale, the index of “current residency” characterized living places from not being stable (with a score of 0) to being stable (with a score of 3). For example, places such as vacant buildings, cars, outdoors, or living on the streets were scored 0, while places such as apartments/houses that the youth or their family own or rent and foster homes were scored 3. The index of “frequency of changing living arrangement in the past year” was defined based on the number of times the youth had changed their living arrangements. Changes six times or more indicated instability and were scored 0 (homelessness), while responses that indicated no changes in living arrangements were scored 3 (housing stability). The third condition, “total times of being homeless during life,” was defined as two or more years of being homeless (with a score of 0) to never being homeless (with a score of 3). Total scores indicated the degree of experiencing homelessness from 0, which indicated homelessness (housing instability), to 9, which indicated housing stability. Examining the internal consistency of the scale in this study was reasonable with α = 0.79, M = 7.05, and SD = 1.82.
Data Analysis
Three software applications including SPSS-24 (for data screening, examining main statistical assumptions, and multivariate procedures), Tableau-2019.4 (for the multivariate visualization of data), and AMOS-24 (for examining the effects of mediating factors on the paths from risks to outcomes) were used in this study. Before analyzing the hypotheses and research questions (RQs) using analysis of variance (ANOVA) and path analysis, a set of primary tests was used to explore data (Islam Khan & Hoque, 2020; Jakobsen et al., 2017). The essential statistical assumptions (e.g., homoscedasticity, normality, and lack of systematic missing data) were examined. Using a residual scatter plot, which refers to the difference between observed and predicted data (Nimon, 2012), the assumption of homoscedasticity was not violated. Also, all main factors had acceptable normalcy based on the skewness ranging from −0.026 to 0.74 and the kurtosis ranging from −0.07 to 0.49. Since the current research dealt with three to seven main independent variables in each analysis, the overall number of participants (N = 251) was adequate (Beshlideh, 2012; Hooman, 2010; Meyers et al., 2006). Beshlideh (2012) noted that there should be at least 15 participants per variable for linear regression and other statistical procedures. Likewise, the sample size was more than 10 times the total parameters used in the path model (Kline, 1998; Streiner, 2005). To test multi-collinearity, the variance inflation factor (VIF) was examined. The results showed that the VIF ranged from 1.39 to 1.71 with a tolerance between 0.58 and 0.72. Since VIF should be statistically below 10 to consider that there is no multi-collinearity between variables (Meyers et al., 2006), the range of VIF confirmed that no inflated correlations occur between variables.
In addition to examining essential statistical assumptions, the model fit indices for path analysis were calculated. The indices included chi-square, normed fit index (NFI), comparative fit index (CFI), Tucker–Lewis index (TLI), root-mean-square error of approximation (RMSEA), and HOELTER (for sample size). Of these indices, chi-square is a proper procedure to examine the differences between observed and expected relationships (correlations/covariances) among all variables in the path and adequately meet the expected criterion (x2 = 8.027, p = 0.05). Likewise, given that a value >0.95 for NFI, CFI, and TLI ensures a better model fit (Newsom, 2018), all above-mentioned indices CFI (0.98), NFI (0.98), TLI (0.92), and HOELTER (244) were well conceived. The last index, RMSEA, was 0.08, which once again indicated model fit.
Hypothesis and RQs
Based on the primary data analyses, the current research examined one hypothesis and six RQs to reach the research objectives.
Results
Descriptive Statistics
The mean scores and the standard deviation of risks and mediating factors and the outcomes were calculated, and the results revealed that the participants’ mean score in ACEs was M = 2.46, SD = 1.89. For VC, the mean score was M = 5.24, SD = 2.64. Also, the mean scores for resilience and living in care experiences were respectively M = 53.87, SD = 9.11, and M = 26.15, SD = 7.49. The mean scores for each outcome (PTSR, housing instability, and delinquency) were, respectively, M = 10.95, SD = 3.96, M = 7.05, SD = 1.82, and M = 9.06, SD = 4.24. Since RQ6 proposed whether there are significant patterns in all exogenous and endogenous variables across participants’ demographic characteristics, the means and standard deviations of the variables were calculated for each layer of demographic characteristics. The results are presented in Table 1. Based on the descriptive results, a general linear model (ANOVA) and data visualization were used to examine whether there are significant differences between the variables for each demographic characteristic.
Descriptive Statistics of Variables Based on Demographic Characteristics.
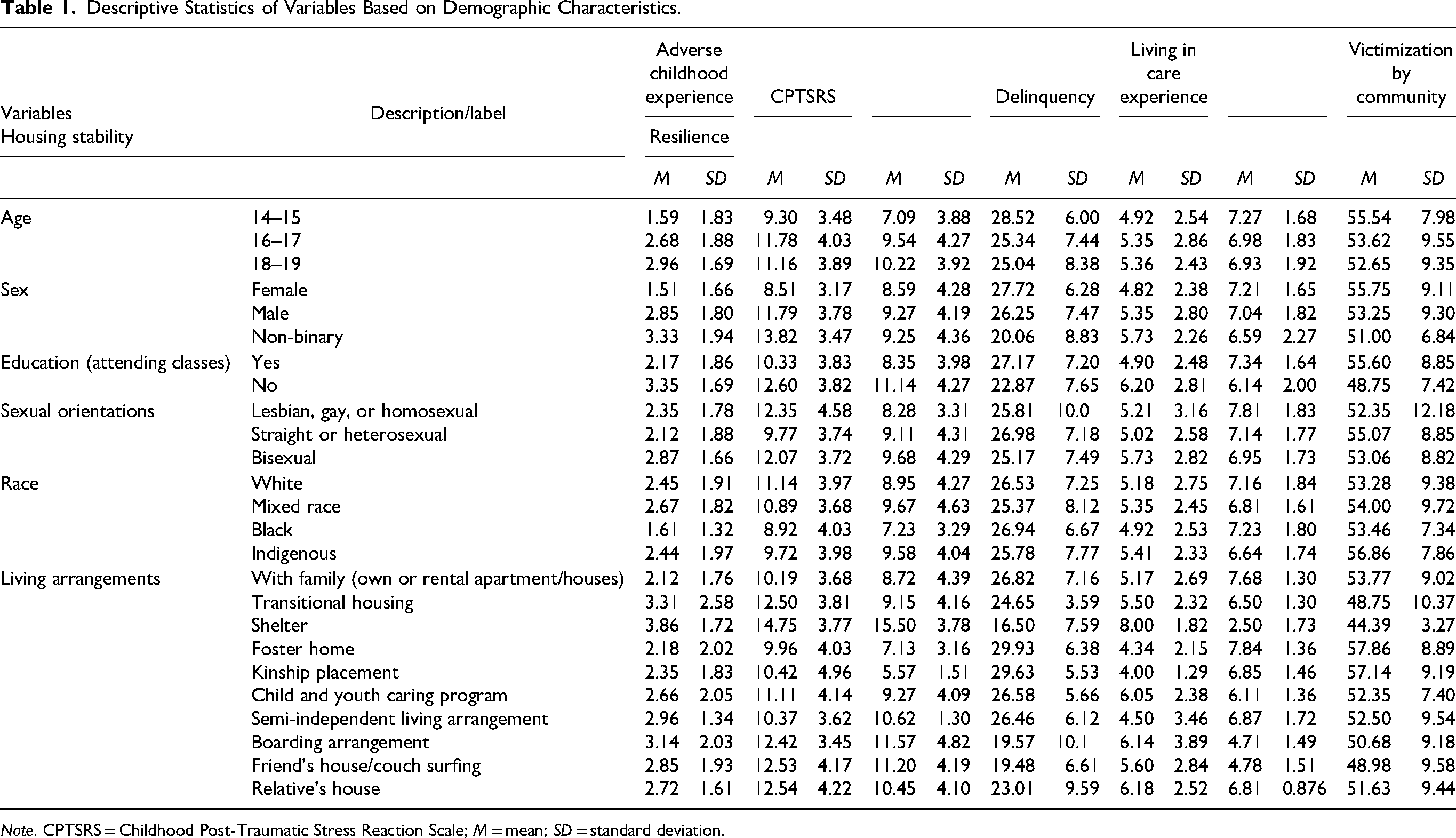
Note. CPTSRS = Childhood Post-Traumatic Stress Reaction Scale; M = mean; SD = standard deviation.
Testing the Hypothesis and RQs
As Table 2 shows, the hypothesized relationship between the variables was confirmed. All factors (risks, mediators, and outcomes) had significant correlations with each other at p < 0.001 with effect sizes ranging between 0.09 and 0.27. Specifically, ACEs were associated with PTSR (r = 0.53, p < 0.001), housing stability (r = −0.30, p < 0.001), and delinquency (r = 0.43, p < 0.001). The R-squared for these relationships are 0.27, 0.10, and 0.19, respectively. VC showed a significant correlation with PTSR (r = 0.44, p < 0.001), housing stability (r = −0.39, p < 0.001), and delinquency (r = 0.41, p = 0.001). The R-squared for these associations were 0.19, 0.15, and 0.16, respectively. These associations indicated that experiencing more risk factors is correlated with more PTSR and delinquency, and lower levels of housing stability. Also, both mediating factors (resilience r = 0.31, p < 0.01 and living in care experiences r = 0.37, p < 0. 01) had a significant positive association with housing stability. However, these mediating factors had a significant negative association with ACEs and VC (Table 2).
RQ1: Do the risk factors have significant direct effects on the outcomes?
Correlations (r) and Effect Size (r2) Among Risk, Mediating, and Outcome Factors.
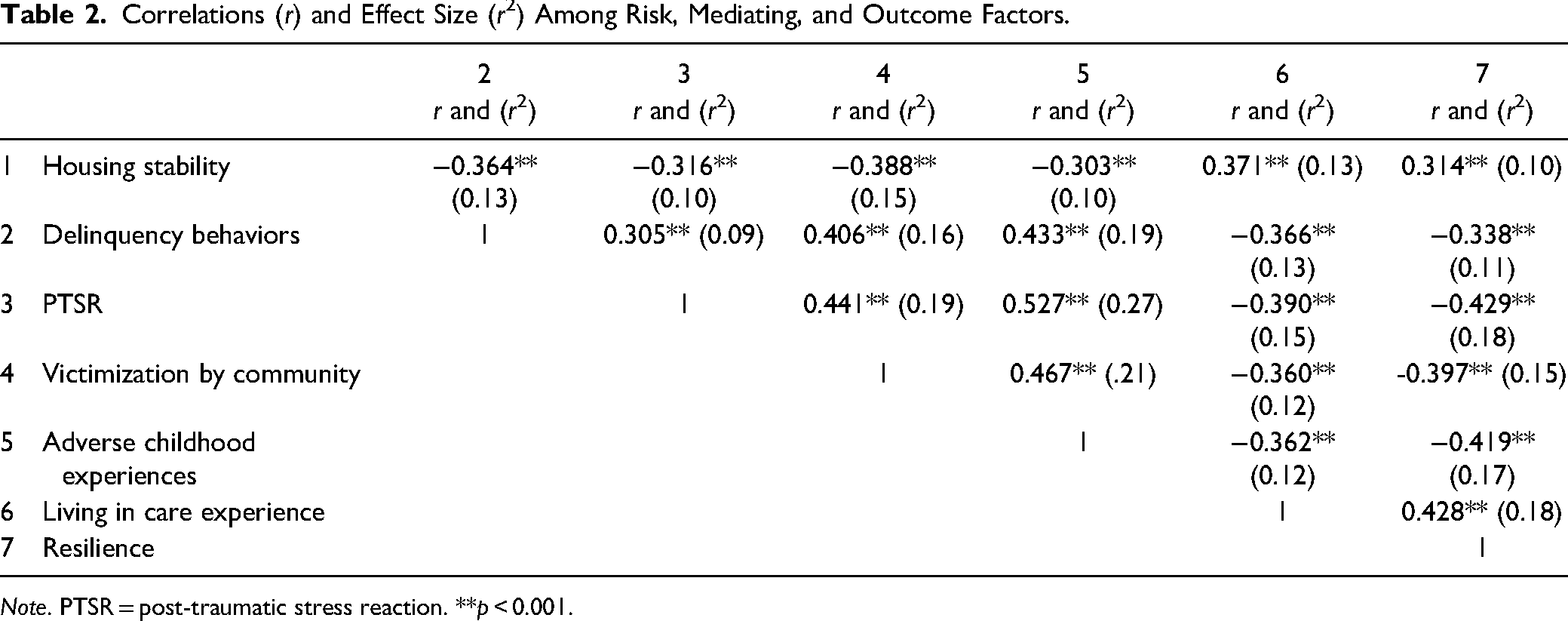
Note. PTSR = post-traumatic stress reaction. **p < 0.001.
Examining RQ2, ACEs showed direct significant effects on both PTSR (β = 0.32, p < 0.001) and delinquency behaviors (β = 0.23, p < 0.001). However, ACEs did not have any direct effect on housing stability (β = 0.06, p > 0.05). As Table 3 and Figure 2 show, the second risk factor, VC also had a direct and significant effect on all three outcomes, with an increasing effect on PTSR (β = 0.17, p < 0.001), a decreasing effect on housing stability (β = −0. 23, p < 0.001), and an increasing effect on delinquency behaviors (β = 0.16, p < 0.005).
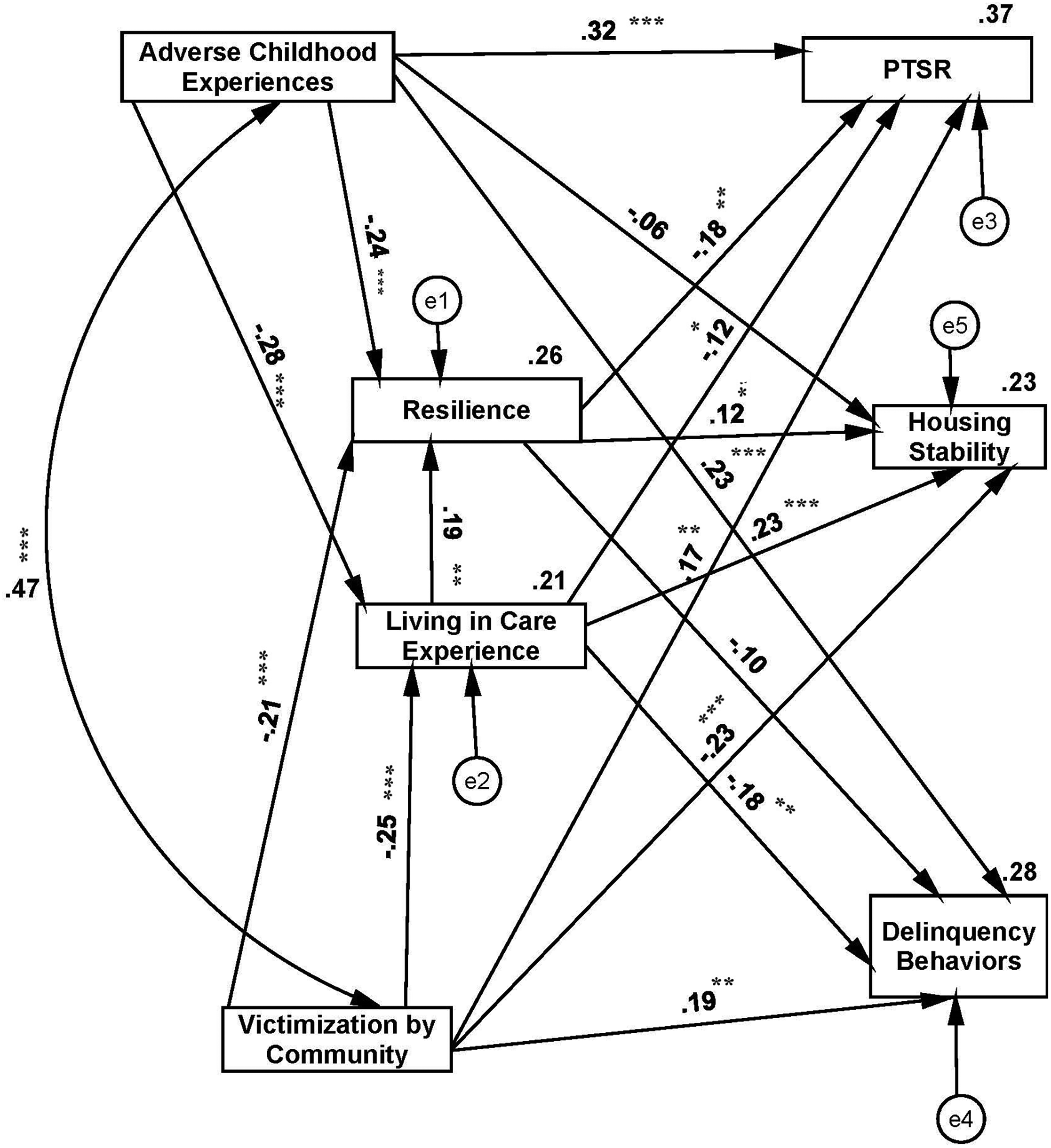
The standardized coefficients of paths in the observed (real) model
The Standardized Coefficients (β) of Direct, Indirect, and Total Effects.
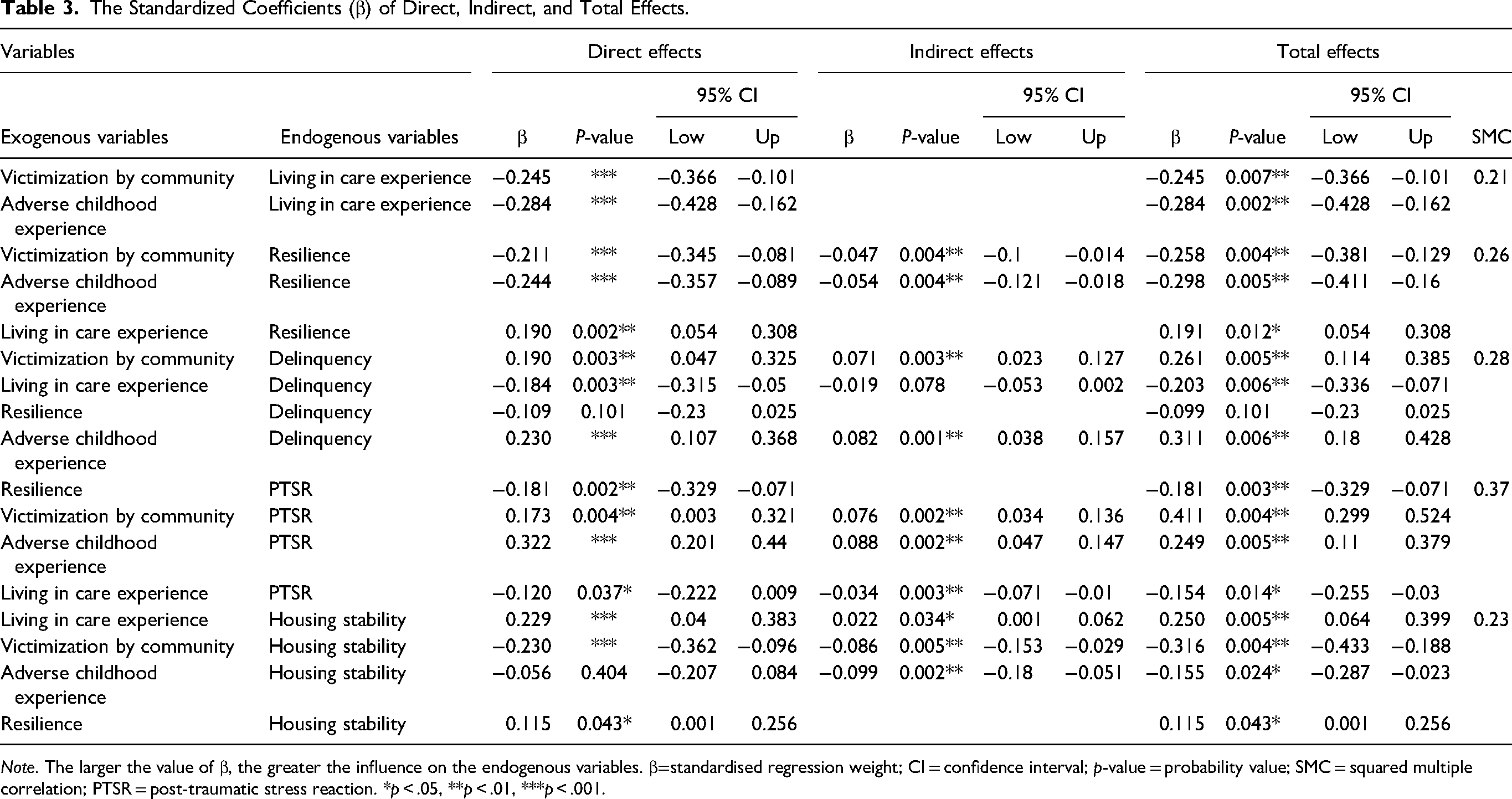
Note. The larger the value of β, the greater the influence on the endogenous variables. β=standardised regression weight; CI = confidence interval; p-value = probability value; SMC = squared multiple correlation; PTSR = post-traumatic stress reaction. *p < .05, **p < .01, ***p < .001.
The RQ2 was examined, and the results (Table 3 and Figure 2) revealed that resilience had significant direct effects on both PTSR (β = −0.18, p < 0.005) and housing stability (β = 0.12, p < 0.05). However, resilience did not have a significant effect on delinquency (β = 0.10, p > 0.05). Living in care experiences showed significant negative direct effects on PTSR (β = −0.12, p < 0.05), a positive direct effect on housing stability (β = 0.23, p < 0.001), and a negative direct effect on delinquency (β = −0.18, p < 0.005). The path from living in care to resilience showed that a positive experience of living in care could positively and significantly affect resilience (β = 0.19, p < 0.005).
Exploring the indirect effects of ACEs on the outcomes via each mediating factor revealed that ACEs could have significant indirect effects on PTSR, housing stability, and delinquency through the mediating roles of resilience and living in care experiences. In other words, both resilience and living in care experiences could significantly mediate the path of ACEs → PTSR, ACEs → housing stability, and ACEs → delinquency (Table 3).
For the path of ACEs → PTSR, the standardized indirect (mediated) effect of ACEs on PTSR is β = 0.088 (p < 0.01). That is, due to the indirect (mediated) effect of ACEs on PTSR, when the score of ACEs goes up by 1 SD, the score of PTSR goes up by 0.088 SD. For the path of ACEs → housing stability, the standardized indirect (mediated) effect of ACEs on housing stability is β = −0.099 (p < 0.01). This indicates that due to the indirect (mediated) effect of ACEs on housing stability when the score of ACEs goes up by 1 SD, the score of housing stability goes down by 0.099 SD. Likewise, for the path of ACEs → delinquency, the standardized indirect (mediated) effect of ACEs on delinquency is β = 0.082 (p < 0.01). These indirect effects are in addition to any direct (unmediated) effects that ACEs may have on PTSR, housing stability, and delinquency.
Examining the indirect effects of VC on the outcomes via each mediating factor revealed that VC could have significant indirect effects on PTSR, housing stability, and delinquency through the mediating roles of resilience and living in care experiences. Thus, both resilience and living in care experiences could significantly mediate the path of ACEs → PTSR, ACEs → housing stability, and ACEs → delinquency (see Table 3).
Exploring the specific indirect paths showed that the path ACE → resilience → PTSR (β = 0.093, p < 0.001) and the path VC → resilience → PTSR (β = 0.06, p < 0.005) could explain PTSR better than other paths. The path VC → living in care → housing stability (β = 0.038, p < 0.005) could reasonably explain housing stability. Also, the path VC → living in care → delinquency (β = 0.072, p < 0.005) could explain delinquency (Table 4). With regard to the effect size for each endogenous variable, 21% of the variability of living in care experiences, and 26% of resilience variability were explained by the ACEs and VC risk factors. Also, all risk and mediating factors could explain 37%, 23%, and 28% of the variability in PTSR, housing stability, and delinquency behaviors, respectively (Table 4 and Figure 2). Based on Cohen's (1988, 1992) and Lakens's (2013) views these effect sizes are between moderate to substantial; that is, the risk and mediating factors could meaningfully explain the variability of the outcomes.
Coefficients of Specific Indirect Paths
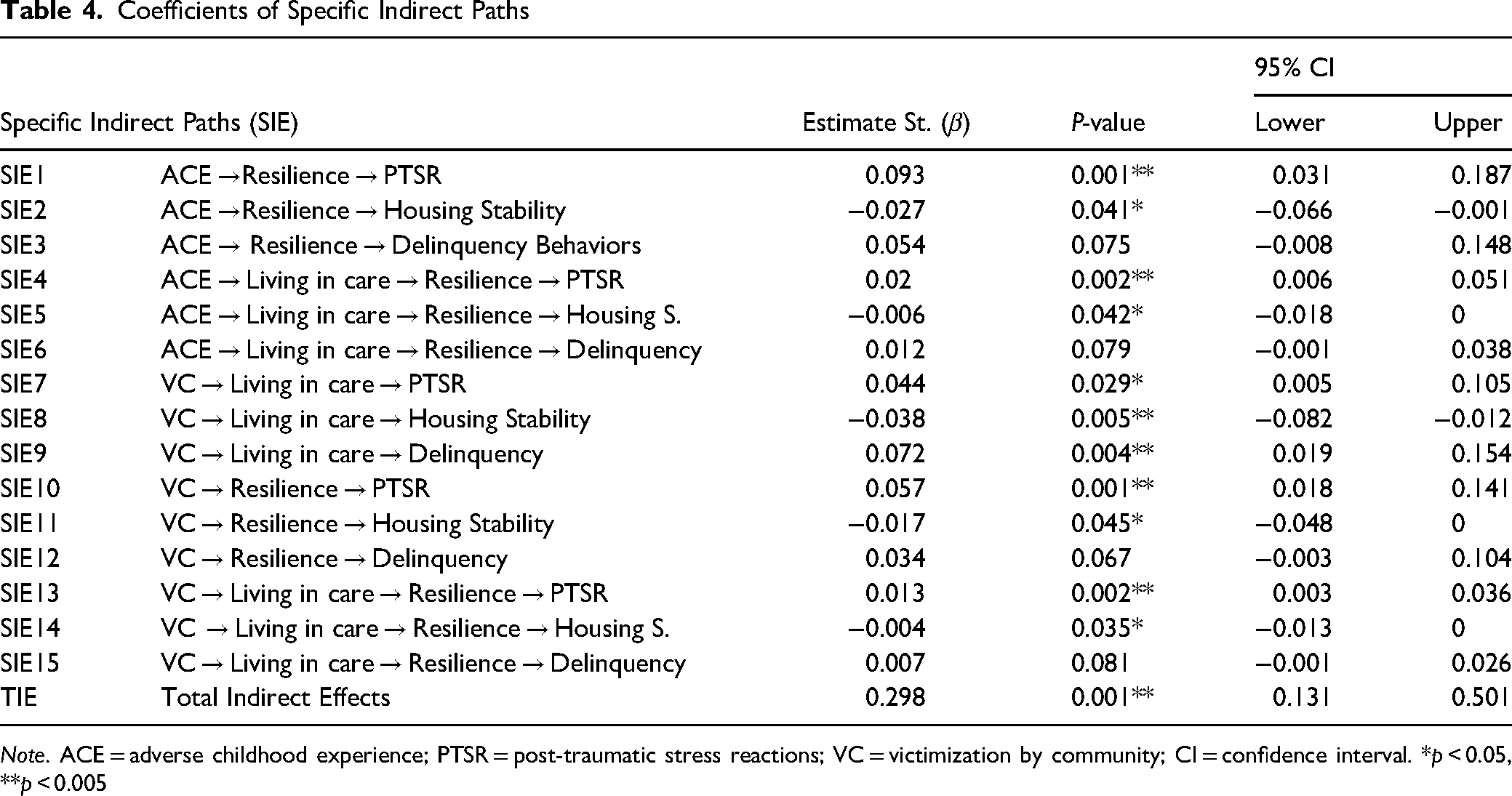
Note. ACE = adverse childhood experience; PTSR = post-traumatic stress reactions; VC = victimization by community; CI = confidence interval. *p < 0.05, **p < 0.005
ANOVA was used to investigate whether the risk, mediating factors, and outcomes varied by demographic characteristics of participants. Before using ANOVA, the homogeneity of variances for all measures (Levene's test) was examined. Results showed that this assumption was not violated (p-values were between 0.136 and 0.46). Next, age, gender, sexual orientation, education, race, and living arrangement were explored using ANOVA followed by Tukey post hoc (Table 5).
Summary of Analysis of Variance (ANOVA) for Demographic Factors and Measures
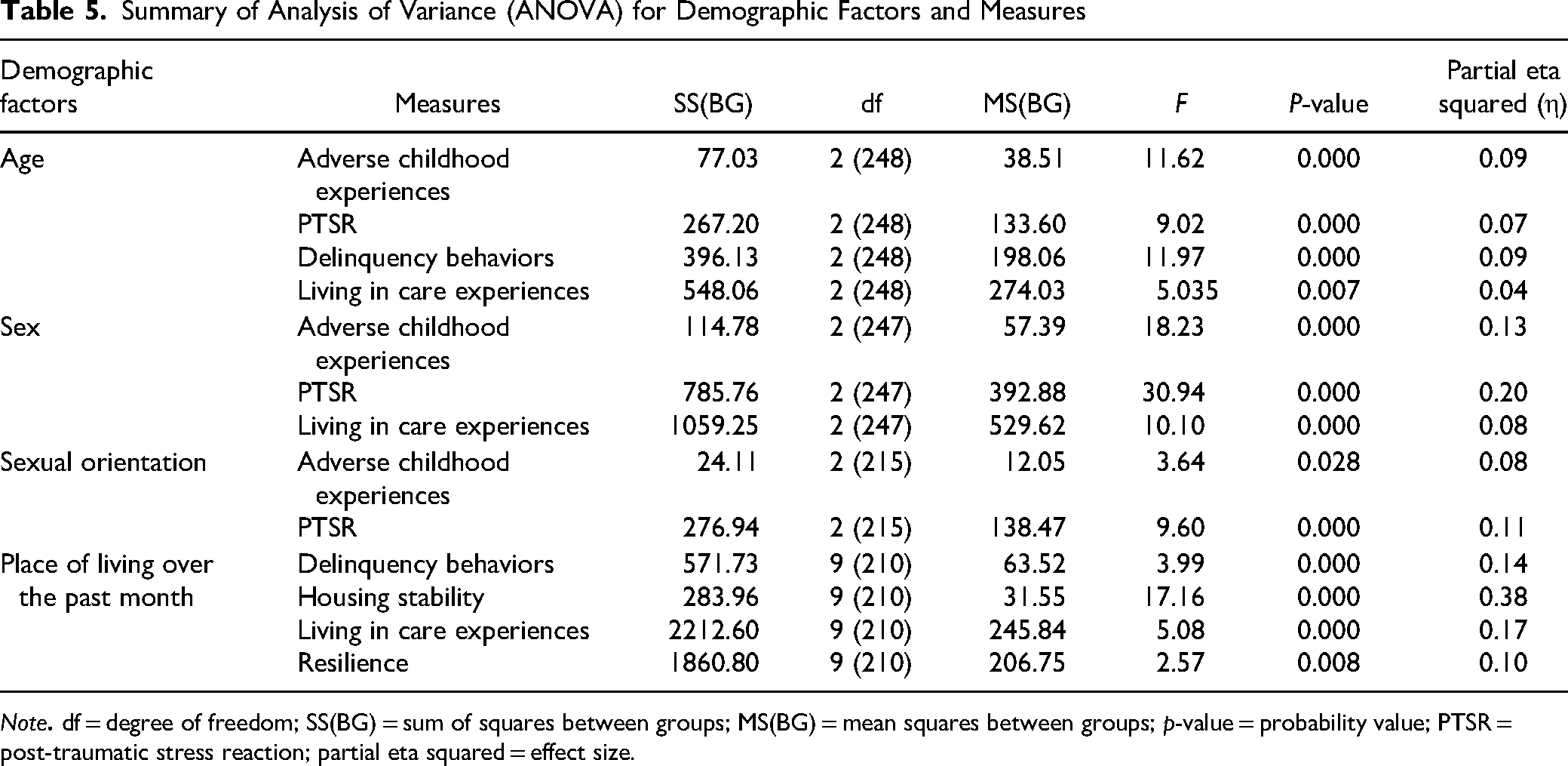
Note
Age
As Tables 1 and 5 show, three groups of participants, Group 1 (14 to 15 years old), Group 2 (age 16 to 17 years old), and Group 3 (18 to 19 years old) had significantly different patterns of ACEs, PTSR, delinquency behaviors, and living in care experiences. For ACEs, the results showed significantly different patterns in terms of age, F(2, 248) = 11.626, p < 0.001. Post hoc comparisons using the Tukey honestly significant difference (HSD) test indicated that the mean score of ACEs (M = 1.59, SD = 1.83) for Group 1 is lower than for Group 2 (M = 2.68, SD = 1.88) and Group 3 (M = 2.96, SD = 1.69), p < 0.001. Furthermore, there was no significant difference between Group 2 and Group 3. That is, both age groups (ages 16 to 17 and ages 18 to 19) had higher rates of adverse experiences than 14- and 15-year-old youth.
For PTSR, participants across age groups again showed significant differences, F(2, 248) = 9.025, p < 0.001. The Tukey HSD revealed that the mean PTSR scores for Groups 2 (M = 11.78, SD = 4.03) and 3 (M = 11.16, SD = 3.89) were higher than for Group 1 (M = 9.30, SD = 3.48), p < 0.001. Regarding the absence of a significant difference between Group 2 and Group 3, results showed that older adolescents (aged between 16 and 19) displayed more post-traumatic stress reactions.
Examining the delinquent behaviors across age groups revealed significant differences between group one and the other groups, F(2, 248) = 11.975, p < 0.001. Also, post hoc multiple comparisons showed an increasing pattern in the mean of delinquency behaviors (M = 9.54, SD = 4.27) for the second and third age groups (M = 10.22, SD = 3.92), p < 0.001. Taken together, the results suggest that the older adolescents in this research had more delinquent behaviors.
When living in care experiences were examined in terms of age, a significant difference between the three age groups was found, F(2, 248) = 5.035, p < 0.001. Also, comparing age groups by using Tukey HSD revealed that the younger adolescents (M = 28.52, SD = 6.00) had higher levels of positive experiences when living in care compared to older adolescents: Group 2 (M = 25.34, SD = 7.44); Group 3 (M = 25.04, SD = 8.38). However, there were no significant differences in resilience, housing stability, and victimization by the community in terms of age. Examining the effect size of age on the variables ACEs (η = 0.09), PTSR (η = 0.07), delinquency (η = 0.09), and living in care experiences (η = 0.04) revealed that age had weak to moderate effects on these variables (Table 5). Visualizing the relationships between age and the variables by using the Z score showed that youth aged between 17 and 19 had higher scores on delinquency than youth between 14 and 16 years old (Figure 3a). In contrast, youth aged between 14 and 16 had higher positive experiences during living in care compared with older youth (Figure 3b). Also, those youth who were between 14 and 16 years old had lower scores on PTSR and ACEs compared with the other ages (Figures 3c and 3d).
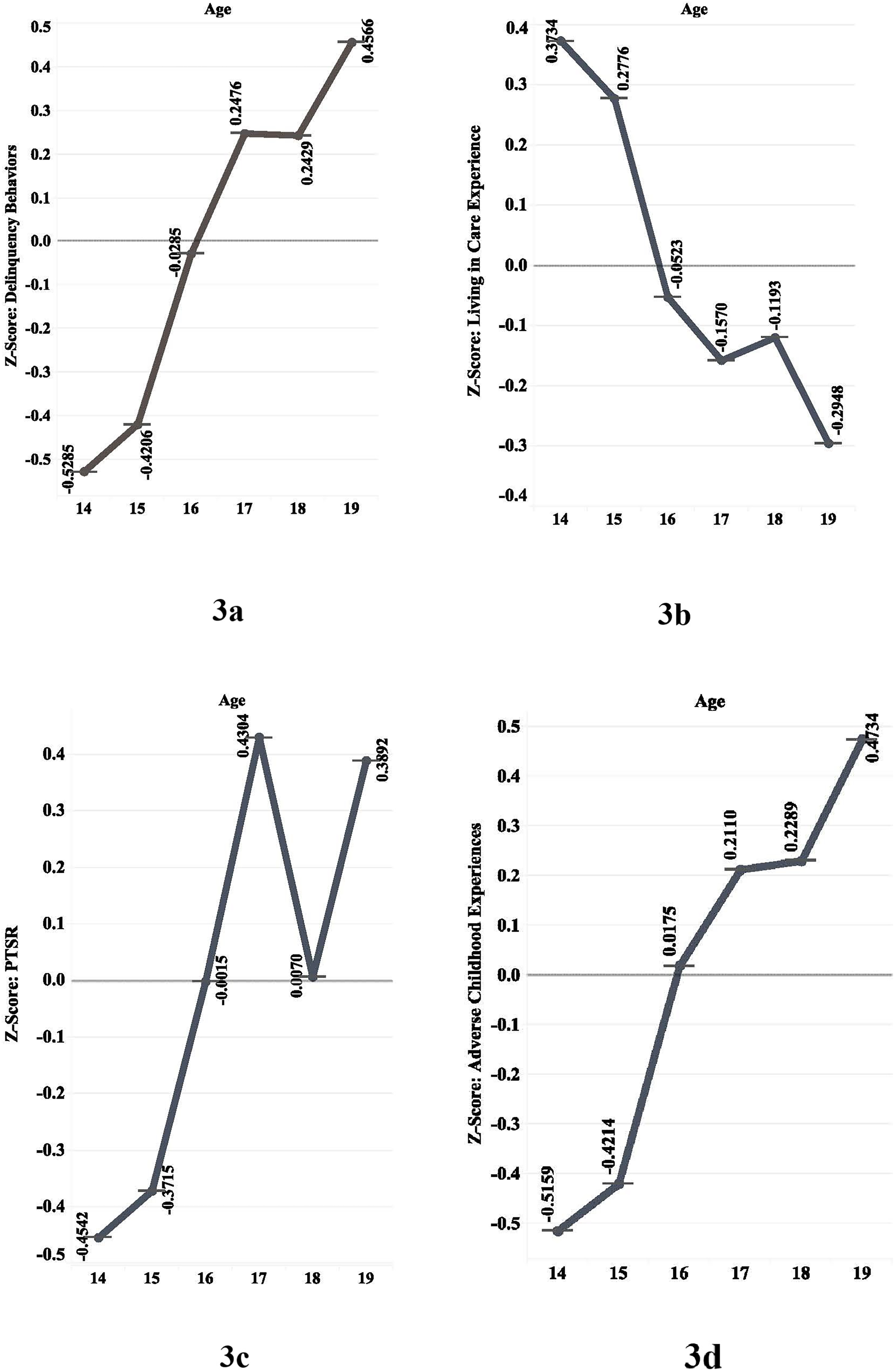
Patterns of changes in measures by age based on Z scores.
Sex
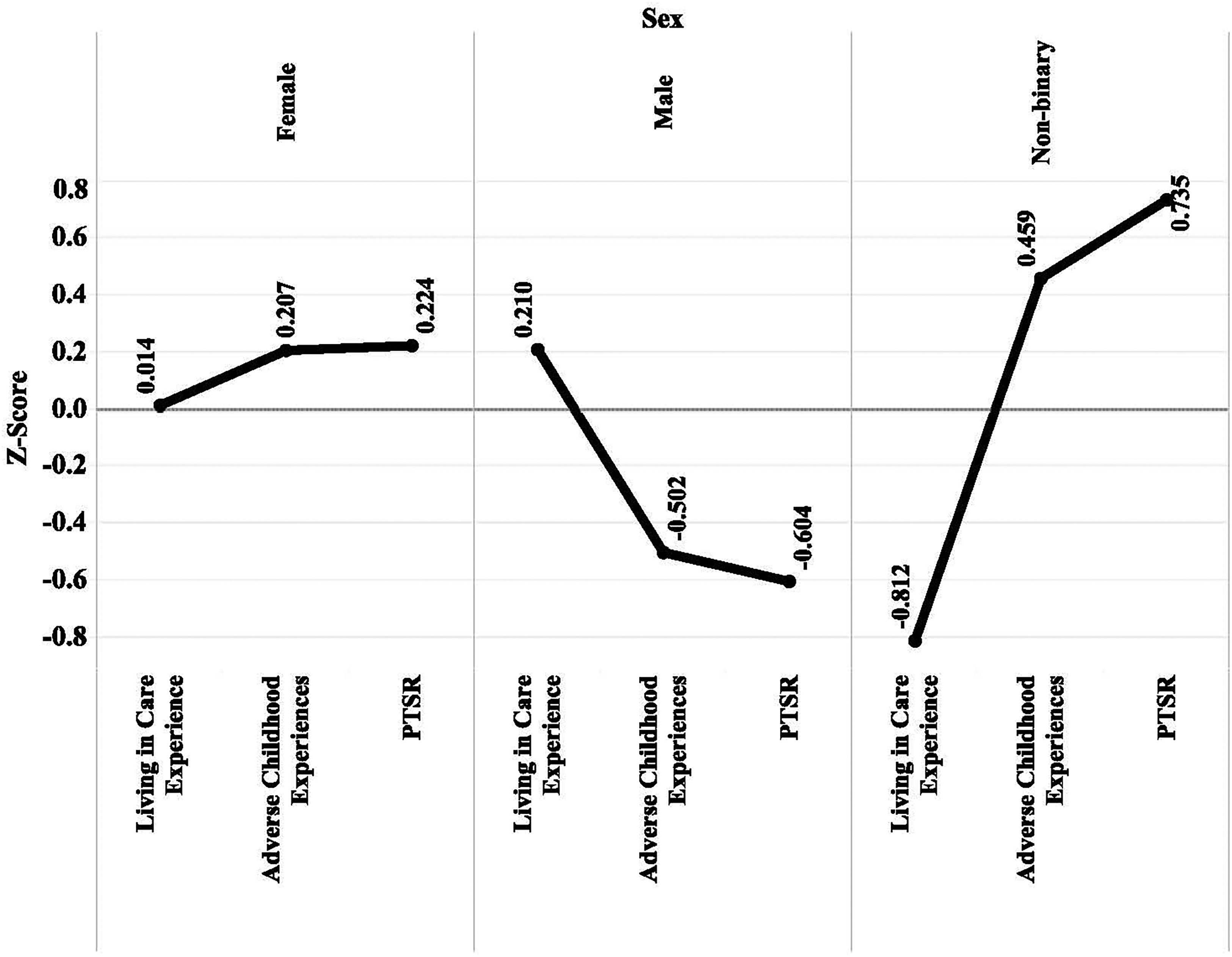
Three factors, including ACEs, PTSR, and living in care experiences showed different patterns of change in terms of sex. For ACEs, differences between male, female, and non-binary individuals were significant, F(2, 249) = 18.24, p < 0.001. The mean comparison between the three groups showed that male youth (M = 1.55, SD = 1.66) had significantly lower ACEs than female (M = 2.85, SD = 1.80) and non-binary youth (M = 3.33, SD = 1.94), p < 0.001. However, there was no significant difference between female and non-binary youth in adverse experiences.
The overall differences across sexes were also significant for the factor of PTSR with F(2, 247) = 30.95, p < 0.001. The test of mean difference (MD), using Tukey HSD, revealed that males (M = 8.51, SD = 3.17) had lower PTSR compared to females (M = 11.79, SD = 3.78), p < 0.001, and non-binary youth (M = 13.82, SD = 3.47), p < 0.001. Also, non-binary youth had a significantly higher score in PTSR than females, MD = 2.02, p < 0.001.
When youth living in care experiences were examined, the results revealed that both males and females had more positive experiences than non-binary youth while living in care. As Table 5 shows, sex had medium to large effects on living in care experiences (η = 0.08), ACEs (η = 0.13), and PTSR (η = 0.20). Also, Figure 4 shows that youth in the non-binary sex group had higher scores in ACEs and PTSR compared with male and female groups.
Patterns of changes in measures by sex based on Z scores.
Sexual Orientation
Of seven risk, mediating, and outcome-related factors, only two factors, ACEs and PTSR, showed significant differences based on the participant's sexual orientation, F(2, 215) = 3.64, p < 0.05 for ACEs, and F(2, 215) = 9.61, p < 0.001 for PTSR. The comparison of MD revealed that straight or heterosexual youth had significantly lower ACEs (M = 2.12, SD = 1.88) than bisexual youth (M = 2.87, SD = 1.66), p < 0.001. Also, PTSR was higher for lesbian and gay youth (M = 12.35, SD = 4.58) compared with straight or heterosexual youth (M = 9.77, SD = 3.74), MD = 2.58, p < 0.001. Taken together; the results showed that straight or heterosexual youth had fewer ACEs and lower rates of PTSR compared to youth with other sexual orientations. The effect size of sexual orientation on PTSR (η = 0.11) was medium (Table 5). There were no significant results for other variables in terms of sexual orientation.
Education
Since education was measured using a binary item (yes/no), a t-test was used to examine differences. with results showing that VC (MD = −1.30), ACEs (MD = −1.17), delinquency (MD = −2.78), and PTSR (MD = −2.27) were significantly lower for youth who attended educational classes compared to those who did not, p < 0.001. Also, participants who were attending school had a higher level of resilience (MD = 6.84), housing stability (MD = 1.20), and positive experiences during living in care (MD = 4.30, p < 0.001) than those who were not engaged with education.
Race and Living Arrangements
Although none of the factors showed any differences across the participants’ racial identity, the MD of four factors, including delinquency, housing stability, living in care experiences, and resilience were significant across the types of youth residency over the past month (Table 2). For delinquency, F(9, 210) = 3.99, p < 0.001, the Tukey HSD of MD (Table 6) revealed that those who had lived in their own or rental apartments, foster homes, and kinship houses had significantly fewer delinquent behaviors compared to those who were living in shelters.
For housing stability, F(9, 210) = 17.16, p < 0.001, the results of means comparisons (Table 6) revealed that those who lived in their own rental apartment, foster houses, kinship, and relative houses had more experiences of housing stability than those who lived in shelters, friends’ houses, or had boarding arrangements (Table 5). Regarding the positive experiences during living in care, the results, F(9, 210) = 5.08, p < 0.001, showed that youth who were living in their own or rental apartments or foster homes had more positive experiences than those who were living in shelters, friends’ houses, or had a boarding arrangement. Exploring resilience across the places of living revealed that youth who were living in foster homes had higher levels of resilience compared with youth who were living in other types of housing arrangements F(9, 210) = 2.58, p < 0.001. Using Z scores, patterns of difference were visualized in Figures 5a to 5d.
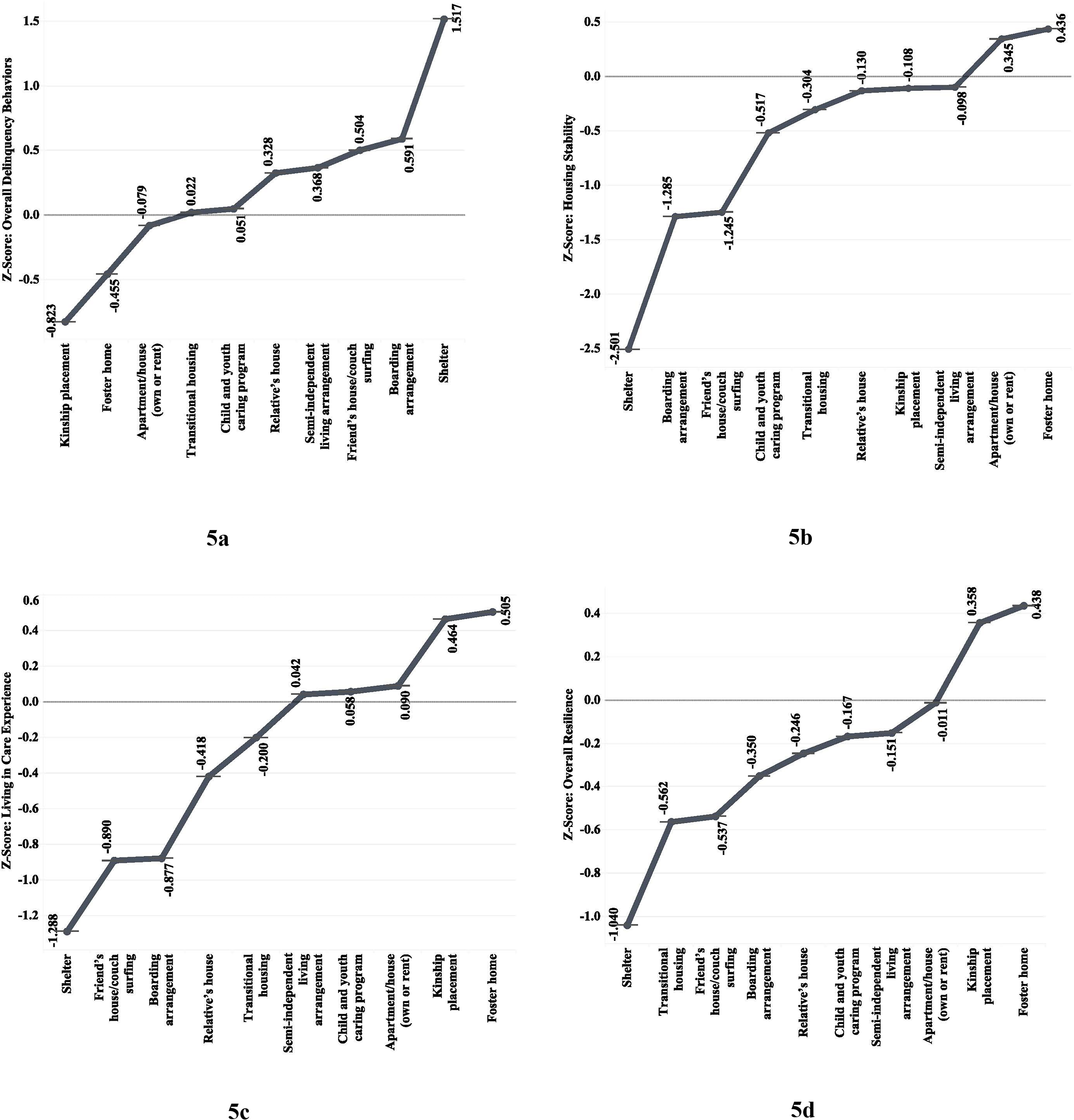
Patterns of changes in measures by living arrangements based on Z scores.
As Table 5 shows, the variable of living arrangements had a large effect size on housing stability (η = 0.38), living in care experiences (η = 0.17), and delinquency (η = 0.14). However, it had a medium effect on resilience (η = 0.10). Using Z scores, patterns of differences in delinquency, resilience, living in care experiences, and housing stability were visualized across living arrangements (Figures 5a to 5d). The results indicated that those who were living in shelters or had boarding arrangements showed more experience of delinquency and lower experience in housing stability and lower scores in resilience. In contrast, those youth who were living in foster homes or kinship placement had higher scores in resilience, positive experiences during living in care, and housing stability.
Discussion and Application to Practice
This research clarifies the paths between risk and protective factors and outcomes for a population of young people receiving child welfare and community support services. We were particularly interested in which constellation of factors and which statistically significant paths were associated with better outcomes in regard to PTSR, delinquency, and housing stability. Our cross-sectional data also generated several findings regarding how risk and mediating factors and outcomes vary across the demographic characteristics of adolescents.
Starting with risk factors, our results show that ACEs have a significant association with PTSR and delinquency, which is consistent with previous findings (Anastas et al., 2021; Barnes et al., 2021; Leban & Gibson, 2020; Rebbe et al., 2017). However, the model did not confirm an expected direct link to housing stability. This is the opposite of what Middleton et al.(2022) and Barnes et al. (2021) found. One interpretation for this heterogeny is that previous research studied adverse adolescent experiences (AAEs; Czaderny, 2020) instead of ACEs. When studying youth homelessness, it may be that AAEs are related to those adversities that were experienced concurrently by homeless youth rather than as conditions that preceded precarious housing. Accordingly, the immediacy of adolescent adversities may exert an acute impact on an adolescent's housing stability even though the ability of ACEs to influence other outcomes, such as PTSR and delinquency, remains strong. Further research is needed to explore the effect of ACEs during the period from childhood to late adolescence.
Unlike ACEs, VC did have a significant direct relationship with all three outcomes. The path from victimization to PTSR and other mental health problems was also studied by Flatley et al. (2022) and Fagan (2022) with similar results. Likewise, the relational path from victimization to homelessness was previously noted by Prock and Kennedy (2020) and Fischer (1992). Although Fischer (1992) believed that the relationship between victimization and homelessness should be interpreted causally, the likelihood of being victimized could be increased when homelessness occurs making it difficult to assert causality. This effect was also verified for delinquency in the current research, which was previously corroborated by Armstrong et al. (2018). Depending on their intensity and valence, risk factors may function individually or in combination with other risk factors to influence outcomes. Accordingly, the current research examined the co-variability between ACEs and VC. Both factors had 22% covariance (r = 0.74, p < 0.000). Since each risk factor could individually explain 10% to 19% of the variability of outcomes, it is inferred that these risk factors could both individually and together have a significant impact on outcomes.
Our results suggest that both resilience and living in care are mediating factors capable of influencing the link between risk factors and children's psychosocial outcomes for young people who are clients of CWS. Regarding resilience, we found that resilience can buffer the effects of ACEs on PTSR. Before taking resilience into account, ACEs had an effect size of β = 0.322, p < 0.001 on PTSR, but after considering the mediating role of resilience, the effect size was β = 0.093, p < 0.001. Resilience could also reduce the effects of VC on PTSR, from β = 0.17, p < 0.001 to β = 0.057, p < 0.001. These results showed that the relational paths amongst ACEs, resilience, PTSR, and also between VC, resilience, and PTSR are strong enough to define the mediating role of resilience. Several previous studies have indicated that resilience could assist individuals in coping successfully with different types of ACEs (Horn & Feder, 2018; Liu et al., 2020; Xi et al., 2020).
Similarly, living in care experiences influence the link between ACEs and PTSR and the link between VC, PTSR, delinquency, and housing instability. The positive impact of living in care on housing stability was previously reported by Montgomery et al. (2006). Although not all programs for youth living in care provide positive experiences, Montgomery et al. (2006) argued that living arrangements that provided protective experiences could successfully promote youth educational attainment, employment, housing stability, and health. Considering that the success of CWS depends on their capacity to provide youth with positive and authentic experiences (Burge, 2022), it seems that CWS were in large part a successful intervention for youth who participated in this study. When the mediating roles of living in care and resilience were examined cumulatively, both showed evidence of influence on the link between ACEs, PTSR, and housing stability; that is, these factors could buffer outcomes. Accordingly, higher resilience and positive experiences of living in care could be defined as protective factors that influenced PTSR, delinquency, and homelessness by lowering the likelihood of these outcomes.
Demographic characteristics (e.g., age, gender, sexual orientation, marital status, living arrangement, and race) are usually used to study whether psychosocial factors (e.g., ACEs and resilience) display differences or changes across diverse populations. Understanding these changes could inform CWS practitioners on how to deal with such differences in youth when providing services to adolescents. Well-documented studies have shown that adolescents who use welfare services are heterogeneous based on their levels of risk exposure, protective factors, resilience, and accessibility to services (Ungar & Ikeda, 2017). In addition, their abilities to navigate different protective resources vary by age, gender, sexual orientation, and living arrangements (Nunez et al., 2022). As our findings show, ACEs, PTSR, and delinquency varied based on age. That is, older youth showed more symptoms of PTSR, delinquent behaviors, and adverse experiences.
Our results also show that youth who were female and non-binary had more ACEs compared with male heterosexual youth. This result was consistent with previous research suggesting that non-heterosexual youth had more ACEs and other mental health challenges (Andresen et al., 2022). As found in previous studies (Ecker et al., 2020; Grattan et al., 2022), the current research demonstrated that non-heterosexual youth who are using CWS were more likely to show PTSR, housing instability, lower resilience and were less likely to have positive experiences when living in care. Notably, the capacity of resilience to buffer risk factors or reduce negative outcomes was lower for non-heterosexual youth than for heterosexual youth. These findings remind us that a child's sex and sexual orientation continue to put young people at greater risk for psychosocial and developmental problems.
We also found that youth not attending educational classes experienced more ACEs, VC, PTSR, and housing instability and had lower levels of resilience. As anticipated, these findings align with previous research in which homelessness was associated with lower levels of education or dropping out of school (Alberton et al., 2020; Grattan et al., 2022; Nunez et al., 2022).
Although previous studies displayed several differences in homelessness, ACEs, delinquency, and PTSR in terms of race (e.g., black, white, and indigenous youth; Alberton et al., 2020), the current research did not find such differences. This could be an artifact of the size of our sample or reflect efforts by DCS to offer children and families services that reflect equity, diversity, and inclusion principles.
We did, though, observe associations between young people's living arrangements, delinquency, housing stability, and living in care experiences. Youth residing in their own rental apartment, foster homes, or kinship homes had fewer delinquent behaviors, more housing stability, and more positive experiences when they were previously living in care. By contrast, youth living in shelters had more delinquent behaviors, negative experiences while living in care, and unstable housing with frequent changes. Although the positive attributes of foster homes were not studied here, previous studies have shown that foster homes can facilitate school engagement, intimate relationships, and the development of social skills (Mihalec-Adkins & Cooley, 2020; Nunez et al., 2022). More studies are needed, however, on the impact of diverse living arrangements (e.g., foster homes) and their possible benefits for youth resilience concurrent with their negative impact on delinquency and PTSR.
Though children come into contact with CWS because of their vulnerability, our findings suggest that CWS can serve a positive and protective function in children's lives. Clearly, earlier interventions and continuity of service (fewer changes to placement) are associated with better psychosocial outcomes, especially for young people with higher ACE scores and young people who identify as gender-diverse. Together, our findings indicate that good case management for children encountering government-mandated services may break patterns of risk exposure leading to mental health challenges and problematic behaviors such as delinquency. The data is especially interesting with regard to affirming the value of foster and kinship placements for youth with difficult pasts. While family reunification may be desirable, this study's findings show that when social workers prioritize placement stability it may be possible to mediate the relationship between exposure to adversity and negative developmental outcomes. This affirms the value of CWS interventions, especially when provided to younger adolescents before they are exposed to even more violence and neglect.
These findings also suggest that a more multisystemic approach to resilience is worthwhile (Masten & Cicchetti, 2016; Ungar & Theron, 2019) and that CWS are one of the institutional mechanisms that provide young people with the resources necessary to cope with adversity. When aspects of a child's social environment, including community-based violence and stigmatization, are addressed as part of case planning and intervention, there is evidence here that reduction of exposure to these macro- and mesosystemic problems could decrease negative developmental outcomes for populations referred to social services. In other words, the long-standing mandate of social work to focus attention on the person-in-environment (Kemp et al., 1997) is well-justified by the research reported here.
There are some limitations to this study. The study's cross-sectional design inherently prevents any definitive causal conclusions. The findings are a first step and indicate that further longitudinal research would be required to confirm the results. To achieve a causal interpretation, future studies should focus on longitudinal or experimental research.
Also, this study is focused on youth receiving services from CWS with limited diversity in the sample's racial identity. Though youth from racially marginalized populations tend to be over-represented in child welfare and community services, this was not the case for this Nova Scotian sample. It is therefore prudent to not generalize the results of this study to all CWS populations. Furthermore, although the measures used in this study were selected from original sources and their internal consistency was calculated, further studies are suggested to validate the scales for youth receiving welfare services.
Despite these limitations, this current study makes both theoretical and empirical contributions. From a theoretical perspective, this research extends our understanding of resilience and living in care experiences as buffers against risk exposure for young people receiving CWS. Empirically, our findings also suggest that resilience and positive experiences while living in care are important factors associated with decreased delinquency, preventing housing instability, and reducing PTSR. Additionally, this research advances our understanding of how risk and protective factors and outcomes vary across demographic characteristics. As this study showed, older youth (ages between 17 and 19) who are female, non-binary, less educated, and living in shelters are more vulnerable to risk factors and negative outcomes.
Conclusion
The present study deepens our understanding of the mediating role of resilience and living in care experiences on the risks for homelessness among youth receiving CWS. Our findings suggest that resilience and living in care experiences could mediate the relationship between homelessness and its covariates (delinquency and PTSR) in youth who receive CWS. Furthermore, resilience, as a significant multisystemic capacity, can act efficiently at different psychosocial levels (e.g., family, friends, and living in care systems) to decrease the risk of youth experiencing precarious housing and its covariates (post-traumatic stress reactions and delinquent behaviors).
Comparisons of Living Arrangements in Each Factor Using Tukey HSD.
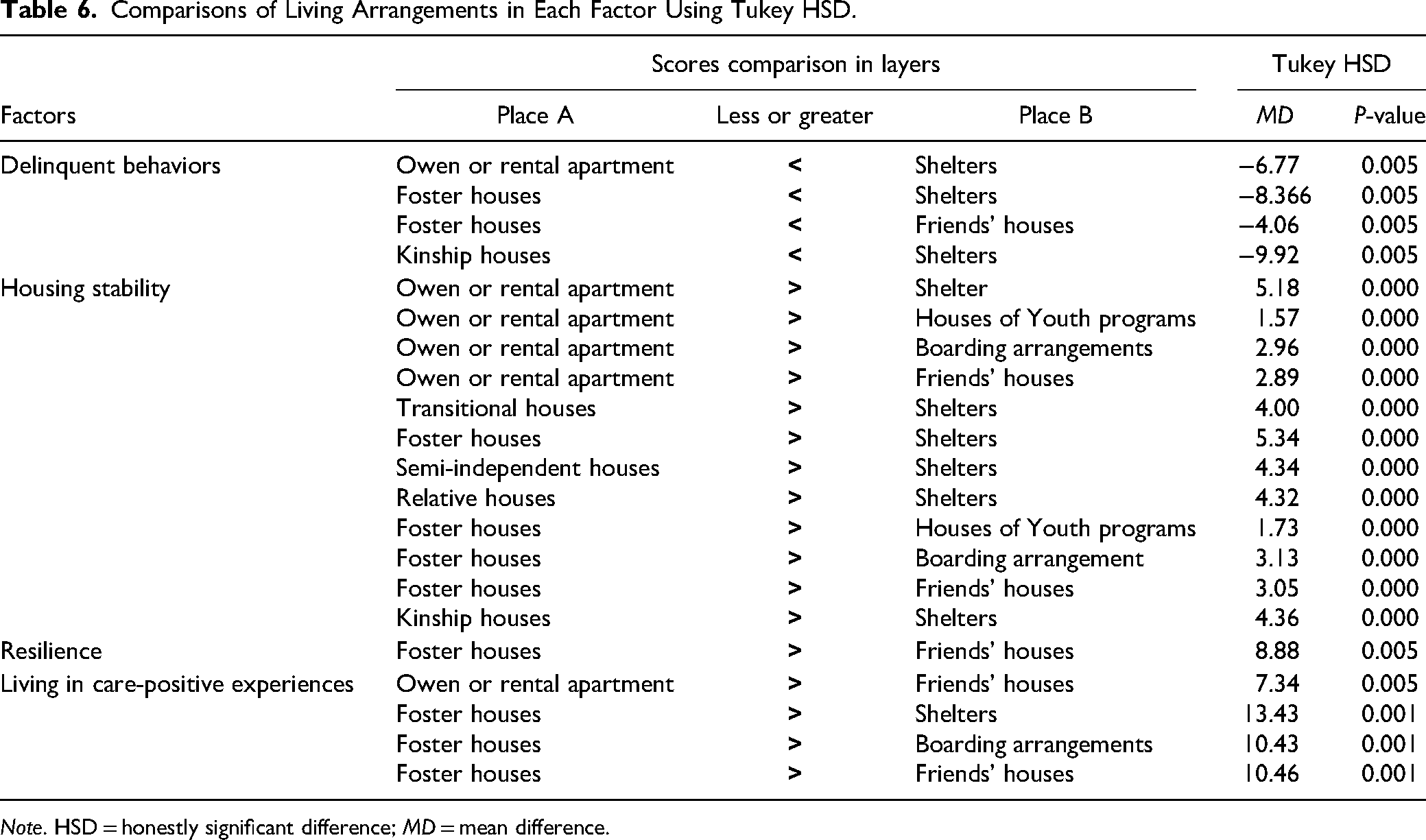
Note. HSD = honestly significant difference; MD = mean difference.
Footnotes
Data Availability Statement
Because of the protected and confidential nature of the data, and the vulnerability of the population (children receiving CWS), the data may only be reviewed for further analysis by contacting the Resilience Research Centre at Dalhousie University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Statement
The procedure followed by this study was approved by the Nova Scotia DCS (DCS-Child Welfare) and Dalhousie University, Canada (REB No. 2020-5103). Written informed consent was obtained from all participants and their caregivers (for those under the age of 16).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Making the Shift, which is a Government of Canada's Network of Centres of Excellence program.