
Abstract
Extreme heat and air pollution exposure are leading causes of adverse cardiorespiratory health outcomes. Exposure reduction strategies are often focused at the local level. This study examined critical challenges community leaders face in understanding and sharing environmental exposure and health information. We conducted interviews with 19 community leaders of two urban environmental justice communities in Massachusetts, United States. Using directed content analysis, we examined air quality and heat perceptions, information and data resources, and barriers to understanding and communicating relevant local information. Participants shared concerns about both poor air quality and extreme heat. They also expressed the opinion that exposure risk information about these topics is siloed; heat and air quality data can be hard to access, interpret, and effectively communicate with community members. Solutions recommended by participants included community engagement, open-data portals, and creative science communication. Increasing sustainable collaborations among academic, government, healthcare, and nonprofit sectors is recommended.
Background
Adverse health impacts of exposure to air pollution are well documented. 1 Decades of research indicate that, in addition to premature mortality, particulate matter (PM) is associated with the development of asthma, chronic obstructive pulmonary disease, cardiovascular diseases, and cancers. 1 Additionally, vulnerable subgroups such as children, the elderly, or people with pre-existing medical conditions may be at an increased risk for developing air pollution-related diseases. 1 In many cases, populations who are vulnerable to the health risks of poor air quality are also vulnerable to the risks posed by extreme heat. 2 Furthermore, extreme heat can exacerbate the negative health impacts of poor air quality. 3 High temperatures in warmer seasons and extreme heat events are associated with a variety of health conditions including heat stroke, cardiovascular disease, respiratory diseases, kidney disease, and diabetes.4–9 Lower-income communities and communities of color experience higher levels of air pollution, heat, and their associated health impacts.10,11 Systematic placement of major air pollution and heat sources (ie, highways, shipping ports, airports, and industrial areas) in these communities contribute to past and present environmental exposure and health inequities. 12
A growing body of locally oriented research has focused on air quality and heat exposure reduction strategies using both qualitative and community-engaged research methods.13–18 Community-engaged methods prioritize topics of importance to community stakeholders “with the aim of combining knowledge and action for social change to improve community health and eliminate health disparities.” 19 Qualitative data additionally enable a more contextualized understanding of stakeholder concerns and perspectives and may provide key insights for future targeted air quality and heat-related quantitative studies. 19 Within the last five years, researchers in the California San Joaquin Valley conducted qualitative interviews to examine local leaders’ perspectives on air pollution information sources, finding that there was a lack of clarity as to who was responsible for communicating air quality information, in addition to critical information on risk mitigation behavior and potential health impacts. 20 Authors concluded that providing local, real-time exposure information tailored to specific communities is necessary for appropriate environmental risk communication. Across and within different communities, it is important to assess the perspectives of community leaders, the resources that they access (or do not have access to), and their capacity for involvement in environmental health information sharing.
Through the analysis of semistructured interviews, we aimed to gain a better understanding of local community leaders' perceptions of air quality and heat-related data resources and opportunities for information sharing in two neighboring environmental justice (EJ) communities in Massachusetts (MA). In MA, an EJ population is a neighborhood where one or more of the following criteria are met:
The annual median household income is 65% or less of the statewide annual median household income. Non-White people make up 40% or more of the population, and 25% or more of households identify as speaking English less than “very well.” Non-White people comprise 25% or more of the population, and the annual median household income of the municipality in which the neighborhood is located does not exceed 150% of the statewide annual median household income.
21
The two communities included in this study, the city of Chelsea and neighborhood of East Boston, include 45,000 to 55,000 residents each and report some of the highest population densities in the United States (16,036 and 10,457 inhabitants per square mile, respectively).22,23 Approximately 67% of Chelsea residents and 58% of East Boston residents identify as Hispanic or Latinx, and around 50% of residents in both communities identify as foreign-born.22,23 While the poverty rate in East Boston is comparable to that of MA (10.5%), a significantly higher percentage of residents in Chelsea live below the federal poverty level (24%).
22
Residents of EJ communities have historically been excluded from environmental health decision-making and face structural inequities such as old housing stock, high rates of tenant-occupied multifamily buildings, high residential instability, poor air quality, economic pressures, or immigration-related stressors.
21
Given the multitude of environmental injustices faced by these communities, we situate this work under the Principles of Environmental Justice, ensuring research questions are informed by those most affected,24–26 and that community members are partners in all decisions about the research. We are committed to sharing results with study participants and the greater community and engaging in policy-relevant work.26,27 Prior to submission to journals for publication, a final manuscript draft was shared with each study participant for their feedback.
This study was influenced by the COVID-19 pandemic. In 2020, Chelsea and East Boston were hit hard by infection, record-breaking summer temperatures, and public attention on local air quality concerns.28,29 This analysis was a component of the Chelsea and East Boston Heat Study (C-HEAT), an established academic-community partnership between environmental health researchers at Boston University School of Public Health (BUSPH), and GreenRoots, Inc., a grassroots EJ organization in the City of Chelsea that is committed to the Jemez Principles of community organizing.30–33. The Jemez Principles advocate that work between community members and other working (ie, academic) partners should:
be inclusive; emphasize bottom-up organizing (listen to all levels of leadership); let all voices be heard (especially those most affected by an issue); be done consciously, acting together in solidarity and mutuality; treat all participants with justice and respect; and commit to self-transformation toward community-centered work (“walk the talk”).
33
C-HEAT previously engaged residents of Chelsea and East Boston in heat monitoring, qualitative and participatory research on extreme heat impacts, and mitigation actions applicable to local community leaders.24,25,34 Specifically, we engaged a total of 22 residents in monitoring their home environment, 12 of those 22 in one-on-one interviews, and the same 12 in a photovoice project that resulted in “calls to action” for city officials and community leaders.
25
Among many things we learned in this process, air pollution and heat are often perceived as two parts of a whole that comprise air quality. Here, we aimed to examine air quality and heat perceptions, data resources, and barriers to information sharing among Chelsea and East Boston community leaders. The research questions in the present study were informed by the results of the prior C-HEAT research.
Methods
BUSPH faculty (one of whom is also a Chelsea resident and GreenRoots board member) and students, and a subset of GreenRoots staff (the majority of whom are Chelsea or East Boston residents), agreed on the following categories and a list of individuals to recruit for interviews: Chelsea and Boston city government staff in Departments of Planning and Development, Climate Resilience, Health, Housing, Senior Services, and Public Works; elected members of the City Council; regional and/or local nonprofit nongovernmental organizations that work on climate resilience in Chelsea and East Boston; and local healthcare clinics. Within these categories, community leaders were also identified due to their engagement in heat and/or air quality improvement work.
To be eligible for the study, participants had to be age 18 or over; hold a leadership role that relates to serving Chelsea or East Boston residents in local government, nonprofit, or healthcare sectors; be able to consent for themselves; and have English language proficiency for speaking, reading, and writing.
Prospective participants were contacted via email by a BUSPH investigator inviting them to participate in an interview. Each received three email invitations. Those who did not respond to any of the three were removed from the contact list. Prior to beginning the interview, participants verbally consented to participate. The study protocol was reviewed and approved by the Boston University Medical Campus IRB (H-42851).
Semi-structured interviews took place in an agreed upon meeting space or through a secure Zoom at a time convenient to the participant. With participant permission, we audio-recorded and transcribed all interviews, and we took notes. Interviews included five domains: participant background, description of professional role, air quality perceptions, heat perceptions, and related work efforts (eg, policy writing, formation of climate action plans, and community organizing). The interviews were conducted in a manner designed to indicate the interviewer's desire to support each study participant's role and expertise as they relate to heat and air quality. In addition, interviews were designed to create the space for participants to think critically about their positional strengths and challenges. Using the approach described by Rubin and Rubin (2011), the interview guide kept conversations focused while allowing for exploration of new or emerging concepts. 35
Interviews were transcribed by Rev Transcription, a BUMC IRB-approved professional transcription service, and uploaded to NVivo 12 (Version 12.7.0). Three investigators reviewed and coded the transcripts (AM, LH, and MH), with at least two people coding each transcript. Our analyses followed the three stages of directed content analysis: preparation, organization, and reporting. 36 As part of preparation, we cross-checked inaudible or missing transcript content with our recordings for accuracy, completeness, and comprehension. For the organization stage, members of the research team categorized and abstracted the interview data using a codebook with 27 codes and 26 subcodes developed a priori using our interview guide domains and questions (see Supplementary Material). To improve intercoder reliability, the researchers met weekly to compare coded transcripts, discuss any emerging codes, and share written memos. We developed five emergent codes during this process. The entire research team collaborated to determine overarching concepts relating to each domain. For the reporting stage, we summarized the data under each domain with exemplary participant quotes. Finally, in our effort to promote data justice, the completed manuscript draft was sent to participants for feedback, and results have been and will be presented at community report-back events. 37
Results
Of the 25 community leaders in Chelsea and East Boston invited to participate, 19 consented and were interviewed. Participants worked in a variety of sectors, with most in government or nonprofit work. Ten participants both resided and worked in either Chelsea or East Boston. Participant ages ranged from 26 to 56 years, with a median age of 39 years. Sixty-eight percent of participants were female-identifying and White or Hispanic/Latinx (Table 1).
Participant Characteristics (N = 19).
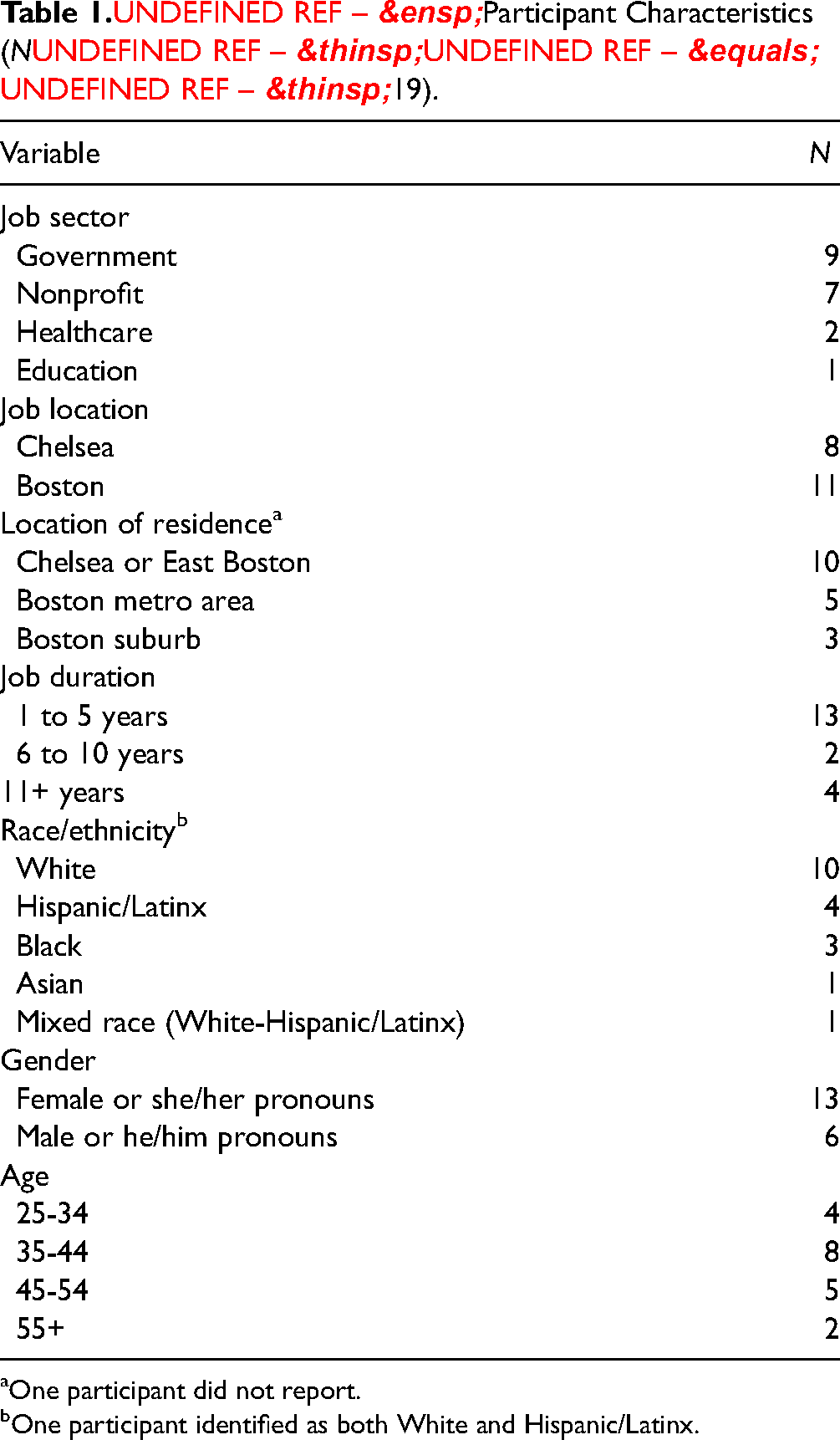
One participant did not report.
One participant identified as both White and Hispanic/Latinx.
When asked about their general perception of heat and air quality exposure in these communities, all 19 participants were concerned about heat exposure, while 15 were concerned about poor air quality. Pertaining to heat specifically, many community leaders described the more impervious urban surfaces of Chelsea and East Boston as a major contributor (Figure 1), with a nonprofit leader stating: My perception is that there's disproportionately higher extreme heat in Chelsea and East Boston since they are urban heat islands, meaning there's not that many trees or green space in the area compared to other more affluent and white areas in the surrounding areas.
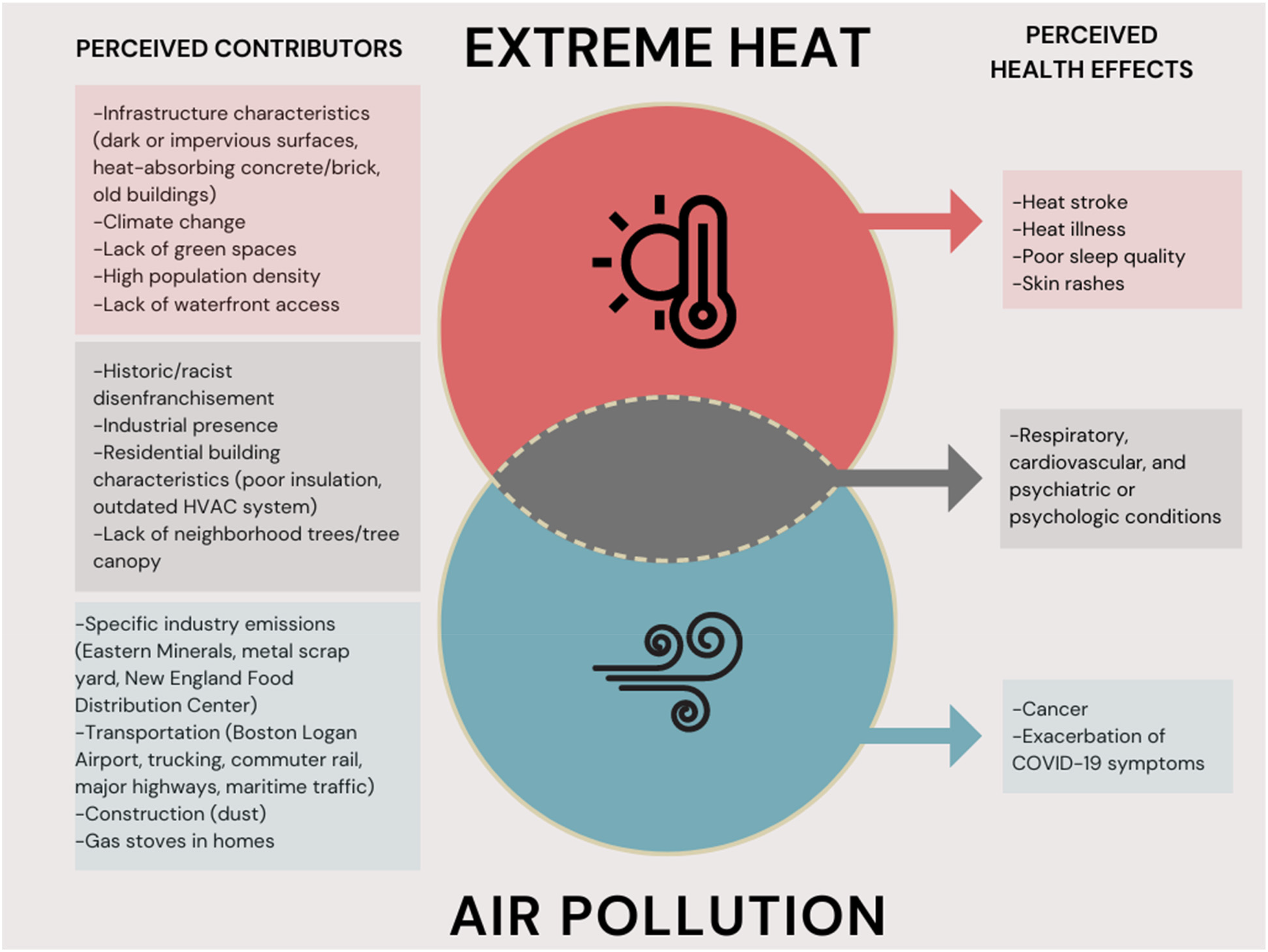
Perceived contributors and associated health impacts of extreme heat (red) and air pollution (blue) in Chelsea and East Boston, MA.
In terms of poor air quality, community leaders discussed transportation-related emissions and a large industrial presence as important contributors (Figure 1). A local government leader said that air quality was: Poor. We are adjacent to Logan Airport. Additionally, the Route 1 state highway bisects the city and it's compounded by the concentration of industrial uses, particularly industrial uses reliant upon the transportation of goods and equipment throughout the New England region.
Many community leaders mentioned health effects of heat including sleep disruption and health effects of poor air quality such as exacerbation of COVID-19 symptoms (Figure 1). Commonly mentioned health effects included cardiovascular and respiratory outcomes (Figure 1). Within more detailed discussions, three overarching concepts emerged: local capacity versus national regulations, environmental health knowledge and communication silos, and environmental health data access and interpretability.
Local Capacity Versus National Regulations
While participants described concerns over air quality and extreme heat, they identified gaps in their knowledge of national regulations, specifically air quality standards, and raised questions regarding their capacity to communicate related risk information in their role. Approximately 80% (n = 15) of participants were concerned about air quality in Chelsea and/or East Boston, while half were not familiar with air quality science or regulatory policy.
We asked participants whether they knew about the criteria pollutants. Each individual participant was able to name 1 (n = 7), 2 (n = 3), or 3 (n = 1) of the 6 criteria air pollutants (PM, NOx, SOx, CO, ozone, and lead) that are federally regulated in ambient air for their health risks. Two participants, one in the government and one working as a nonprofit leader, listed four criteria air pollutants. We probed further to understand what constituted as a “high” level of air pollution, specifically with regard to particulate matter: I couldn't give you the thresholds upon which [PM] is considered [high]. In my opinion, any exposure is too much exposure, and I know that there are thresholds that exist, but I think that there's the argument that they need to be lower, or again, any exposure is no good, said a nonprofit leader.
One participant, a leader in a local government, expressed the opinion that interpreting specific standards in their communities may be outside of the scope of their professional role altogether: I think I have enough level of understanding to know when I need to find an expert who can tell me whether or not something is dangerous in an emergency.
All 19 participants described concerns about extreme heat in the neighborhoods they serve. Five, in the government and nonprofit sectors, were aware that there are currently no national standards to protect people from extreme heat either at home or at work. Two of those five referred to the fact that the Occupational Safety and Health Administration (OSHA) is working on developing a heat standard that would provide protections to workers.
Though it may not be a part of their own job responsibilities, participants in local government and nonprofit fields also noted the need for specific and targeted risk communication from regulators at all levels of the government. They said that regulators should provide risk communication that is applicable to the communities that they serve. Regulatory bodies mentioned include the City of Boston Air Pollution Control Commission; City of Boston Office of Energy, Environment and Open Space; Massachusetts Department of Environmental Protection; Massachusetts Port Authority; US EPA; US Centers for Disease Control and Prevention; OSHA; and Agency for Toxic Substances and Disease Registry.
Regarding the need for dissemination assistance, a city councilor articulated: Just getting information in general [on air quality and heat], more information would be super helpful. And then also specific ways that the city council can utilize this information, where the city is falling short, and how to best work with community partners.
Environmental Health Knowledge and Communication Silos
When asked if community leaders consider extreme heat and air quality together, 14 participants in the government and nonprofit sectors discussed the fact that air quality and heat have shared characteristics. They mentioned perceived contributors to air pollution and extreme heat, including historic disenfranchisement (ie, redlining
1
), industrial land uses (eg, the airport and fuel storage tanks), building characteristics (eg, lack of weatherization), and a lack of trees (Figure 1). One participant, who is a leader in the nonprofit sector, commented on how these exposures may be perceived by residents: I don't think necessarily when you say, “air quality” you think of heat, but people tend to think about [air pollution and heat] the same when it's in terms of their comfort and their living environment and making themselves feel safe and having a healthy home.
Eleven community leaders described similarities between air pollution and extreme heat in terms of exacerbating pre-existing or contributing to new health conditions (Figure 1). Many also contextualized these health issues as occurring more frequently in vulnerable populations including children, the elderly, those with lower income, and those without health insurance or who have trouble accessing healthcare.
Despite the overlap between extreme heat, air pollution, and associated health outcomes, participants described how understanding and communicating related risks and mitigation solutions were often siloed: focusing on each environmental exposure separately, without noting potential relationships between the two. One reason for this phenomenon may be a lack of clear knowledge and guidance regarding environmental health content and communication responsibility. Two participants in the local government and nonprofit sectors reflected similar sentiments best summarized by this quote: We think about the two of those issues [air quality and heat], but I don't know if we've done enough to understand the relationship between the two.
One participant, who worked in the local government and healthcare, discussed gaps in knowledge related to the interplay of air pollution and extreme heat that can make communication challenging: I don't think the communication would happen with both of those [air quality and heat] at the same time, I think we tend to separate themes in general when trying to communicate with people … I don't think we're trained in the same way for air quality at all. … So, if it's cold you put on more layers. If it's hot, you'll try to stay cool … . But if the air quality is bad, we don't have an option associated with it. Do we wear a mask? Do we go outside? Do we avoid exercising outside? I don't think we have any type of action associated with air quality and I don't think we're trained to the same extent to look for it.
Environmental Health Data Access and Interpretability
Community leaders cited numerous sources they rely on for information and data on air quality and heat, although they described barriers to accessing and making sense of this information. As outlined in Figure 2, participants cited a wide variety of sources they reference for air pollution information: national government websites providing health and safety information, state of MA environmental departments and offices, and publicly available air quality monitoring networks. Specific sources for heat information included the National Oceanic and Atmospheric Administration (NOAA), Massachusetts Geospatial Information System (MassGIS), and various Boston City government-run resources. Key shared information sources included national government groups such as the EPA; the City of Boston Office of Environment, Energy and Open Space; the local nonprofits GreenRoots and Mystic River Watershed Association (MyRWA); and local universities involved in community-engaged research (Boston University and Northeastern University). Two specific Chelsea-based research efforts were mentioned (once each): the Center for Research on Environmental and Social Stressors in Housing Across the Life Course (CRESSH) and the Community Assessment of Freeway Exposure and Health Study (CAFEH); however, their academic institutional affiliations (Boston University, Harvard University, and Tufts University) were not mentioned.
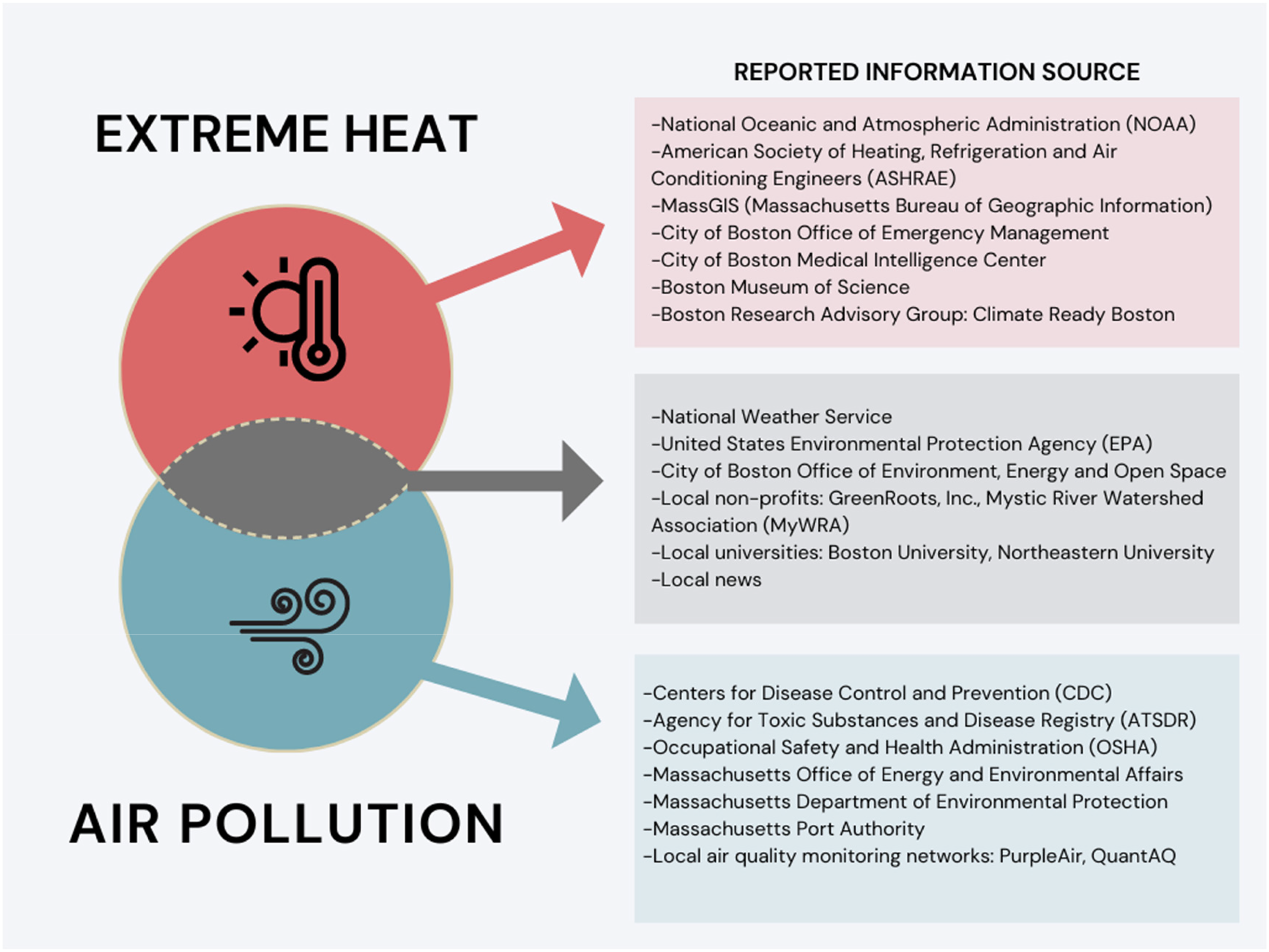
Participant-reported information sources for extreme heat, air pollution, and both.
Logistical challenges to accessing these resources in their day-to-day work and communications with residents are described in Table 2. They include difficulty interpreting government-run data dashboards, the absence of interpretable health and long-term climate information associated with local air quality and heat data, and a lack of community involvement in research on these topics.
Participant-Identified Challenges Matched with Potential Participant-Identified Solutions.
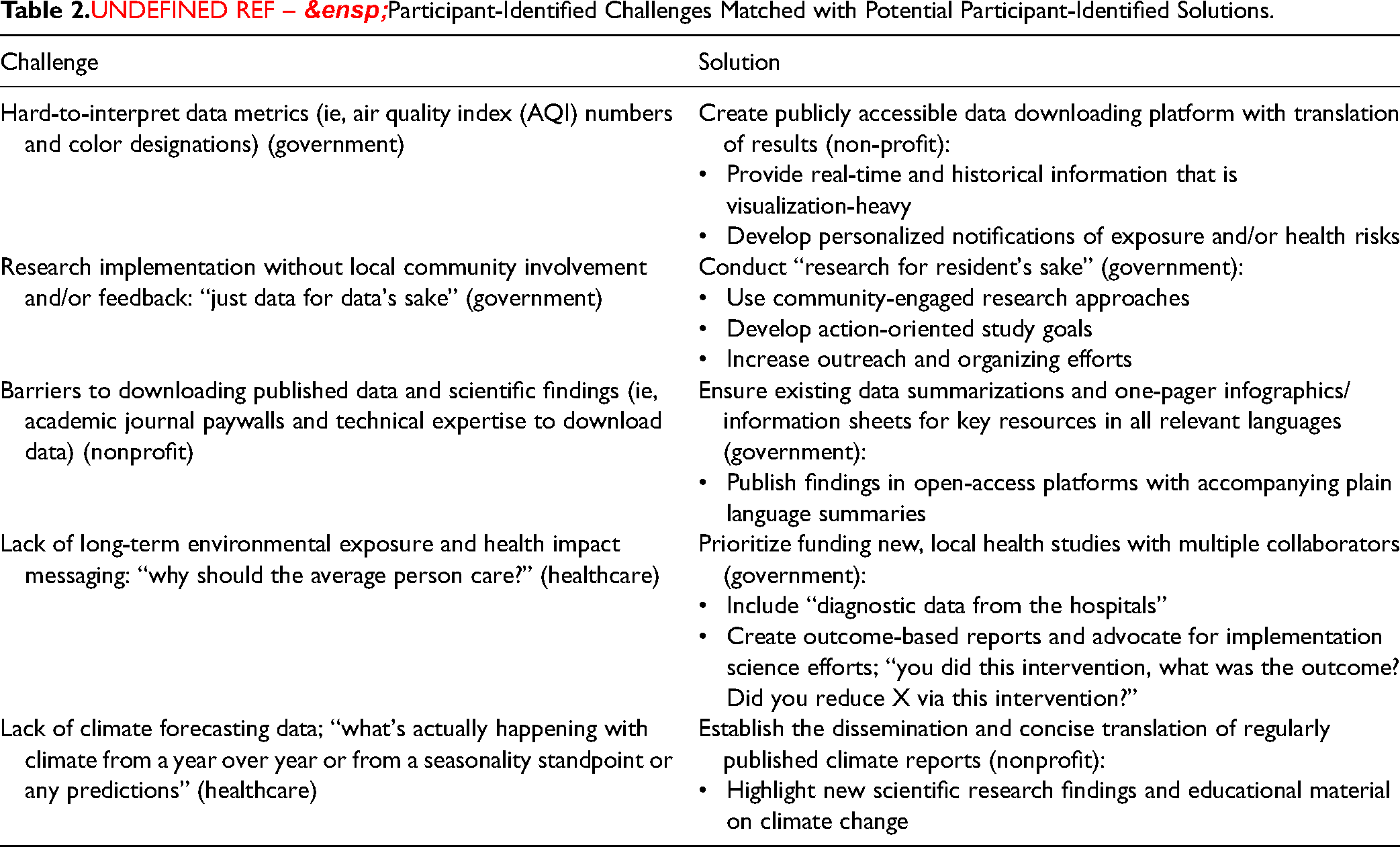
We heard from a participant working in the nonprofit sector on the difficulty interpreting government websites and summarizing data for their community members in an impactful way: When it comes to air quality, there's data out there, but it doesn't impact anyone's decision-making because they don't understand it. Some of these systems will give you a yellow, red coloring of like, “Oh, it's bad air quality out there.” But it still doesn't really connect to people….
A participant in the nonprofit sector reiterated barriers to adequate community involvement in the environmental health research process, specifically regarding academic-led projects in Chelsea: Academic institutions are intended to own their data and not share their data … your only access to that data is in publications which are behind paywalls for folks like us who don't have journal subscriptions.
Solutions to these barriers, proposed by participants, include developing publicly available and user-friendly data portals, requiring community outreach and education complete with research summarization materials, integrating community-engaged research approaches, and collecting more health data to support local environmental epidemiological research (Table 2). All solutions highlight a need for authentic and sustainable community collaboration across all job sectors, more than just “talking the talk” regarding community-engagement. A participant in the government sector summarized this idea: To envision it, and then to see it come alive, and allow them [residents] to be part of that process, be part of the meetings where engineers get together and speak about what's going to happen … When you're a part of something, you're going to care for that project.
As we were interested in the types of solutions that participants thought would be most helpful, we matched each challenge to a proposed solution presented by the interviewees (Table 2). The job sector belonging to each participant who reported a challenge or solution is indicated in parentheses. Our findings indicate shared challenges and solutions both between and within sectors.
Discussion
In this qualitative interview study, 19 community leaders in Chelsea and East Boston, MA, described their challenges in understanding and sharing air pollution and/or extreme heat information with the communities that they serve. Major barriers included a disconnect between information from federal regulations and monitoring programs and local capacity to interpret and share that information, siloed environmental health data and risk communication, and barriers to environmental health data access and interpretability. A potential example of the disconnect is the fact that in April 2021, state and federal authorities installed a federal reference monitor that measures criteria air pollutants and volatile organic compound in the City of Chelsea; community leaders did not mention accessing these data despite the placement of the monitor being a hard-one victory by city and grassroots leaders. 39 However, community leaders also discussed solutions to these challenges, including the use of community outreach and education, open-source data portals, and consistent science communication and report-back of results. Our findings on perceptions of both ambient air quality and extreme heat add to the limited body of literature that focuses primarily on air pollution; to the best of our knowledge, there are no similar studies that examine heat and/or high temperatures.14,18,20,40–43
Ramírez et al (2019) found that 10 regional community leaders in majority nonprofit or government fields in the California San Joaquin Valley were familiar with air pollution data sources applicable to their communities; however, they were unaware whether and how federal organizations such as the US EPA communicate air quality risks (ie, PM standards). These community leaders also felt that “the expert [government] sources were not used by the lay public, even though the sources are intended for the public, according to the agencies that produce those information sources.” 20 Local community leaders across the nation may face similar challenges in their capacity to identify who is responsible for increasing data accessibility and communicating environmental health risks to their residents. Future efforts could investigate the role of heat and air quality expertise and community leadership and activism.
Our study suggests that some of the challenges identified could be reduced by regular clear communications from federal and state regulators. Participants in a similar California-based study described feeling “overwhelmed and powerless” without receiving clear communication strategies to mitigate air pollution-related health impacts. 20 In terms of potential solutions, a study examining community leader perspectives (government, nonprofit, and research institute) on air pollution and health information in the Netherlands found that participants desired short overviews “ready for policy use” from regulators. 14 They also described the additional barrier of competing priorities: even if regulators did communicate expectations, there may be inadequate workforce to carry forward responsibilities. For example, one of their participants commented that a significant barrier was a “lack of time available to read and absorb all of the information.” 14 Although much of the current literature highlights the need for government regulators to improve environmental health communication, other entities must share this responsibility: academic groups and local public health institutions often hold valuable, community-specific knowledge and could collaborate between themselves and with governmental institutions to ensure accurate environmental health communication. 44
Major challenges to accessing air quality and heat data described by our study participants included difficulty interpreting available data and a lack of community involvement in the research process. Similar studies interviewing community leaders described the absence of health data related to existing exposure data as a major barrier.14,17,20,41 For example, in Spain, air pollution experts in government, nonprofit, and academic sectors shared how health information is “often provided by the local public health agency, but not always linked to information regarding air quality levels (eg, air quality indices).” 41 The opportunity to improve coordination of data across organizations and agencies is of global relevance. Many studies cite issues with data interpretability, challenging user interfaces, or lack of open-source design, many of which could be remedied by incorporating community feedback in the results dissemination process.14,20,27,41,45,46 For example, indoor and outdoor air quality are currently available for Boston Public Schools (including in East Boston) with a publicly available data dashboard—a data source like this, not mentioned by our participants, could be beneficial to them and many other community leaders. 47 Our study adds to the community-based participatory research conducted previously in Chelsea and East Boston 24 and highlights the continued need for development of successful communication strategies for reporting back of relevant data on both air quality and extreme heat.
Despite the overlaps between extreme heat, air pollution, and associated health outcomes, participants in our study described challenges both in considering and communicating combined risks and related solutions. The field of environmental health itself is generally siloed: environmental exposure science and public health can be uncoordinated across different organizations, departments, and leadership levels. 44 Relatedly, studies examining barriers to environmental information sharing among community leaders focus on one environmental exposure at a time.13,14,20,40–45 Numerous investigators have called for the examination of multiple exposures at once, or a cumulative impact approach: accounting for the “total burden of chemical and nonchemical stressors and their interactions that affect human health” to better integrate environmental health and environmental justice into our present systems.27,44,48,49 A cumulative impact approach can better support public health policy and decision-making. 31 However, as indicated by Chelsea and East Boston community leaders, it can be difficult to communicate cumulative impacts, and it can be difficult to incorporate them into policy implementation. This issue highlights the need for additional assistance in reporting back and communicating environmental health information tailored to specific communities. Although community-engaged research has been conducted on the issues of environmental health impacts, further work is needed to address sustainability and the infrastructure to support communications over time. The contributions of heat and air quality to cumulative impacts will continue to change and likely increase in the future; therefore, new efforts to fund and support data sharing in an accessible and multilingual manner will be paramount.
Policy-Relevant Summary of Recommendations
To bridge the gap between complex environmental data and actionable policy, the EPA and relevant state agencies should prioritize the development of concise, policy-ready overviews. As mentioned by a Chelsea community leader (Table 2), these overviews should distill critical information on air quality and heat exposure into easily digestible, visualization-heavy formats. By standardizing the creation and dissemination of these summaries, regulatory agencies can ensure that community leaders have the necessary insights to implement effective interventions. Additionally, if there is standardization for overview templates, protocols for data updates, and training for staff, state and local governments could more easily adopt processes tailored to their own regions and communities.
Relatedly, the underlying data summarized in these overviews should be available to all stakeholders, including community members and policymakers. This includes improving the accessibility and user-friendliness of data portals, especially updating data more frequently. For data that is more complex, training programs should be created and/or updated to help community leaders and/or public health officials interpret and utilize data more effectively. It would be important to enforce standards for data formats to ensure consistency across different platforms and users.
In addition to data accessibility and interpretability, government entities should expand policies and/or funding that facilitates collaboration between academic institutions, local public health organizations, and community groups. Key examples of programs that fund joint projects between academic researchers and community groups include the National Institute of Environmental Health Sciences (NIEHS) Community Outreach and Engagement Core (COEC) Grants and the EPA Environmental Justice Small Grants Program.50,51 Government institutions should work with training centers to engage local public health organizations. For example, the US Health and Human Services funds the New England Public Health Training Center, based at Boston University. The center engages public health and community-based organizations through assessments of workforce development needs and through publicly available learning tools such as webinars and workshops. 52 Future environmental health funding opportunities should require collaborative efforts such as building interdisciplinary task forces or shared data platforms.
Both public and private entities should mobilize to fund and support the dissemination of environmental health data in an accessible and multilingual manner. Future government funding in the environmental health field should explicitly require and support the development of resources in languages specific to the communities those resources serve. Additionally, private sector entities, including foundations or even technology companies, could invest in multilingual and community-oriented data-sharing solutions.
Strengths and Limitations
One of the strengths of our study was the use of qualitative information to characterize the depth and range of perspectives from community leaders working, and many living, in Chelsea and East Boston. We leveraged a strong, existing academic-community partnership with GreenRoots, Inc., to invite elected or professional community leaders across representative sectors. Our work supports a call-to-action to conduct exposure assessment in partnership with EJ communities. 27 This research offers an opportunity to integrate qualitative analyses in characterizing the air quality and heat burden in Chelsea with a policy-relevant lens. We also outline our limitations: although we aimed to have a diverse sample of participants depicting various job sectors and experiences, our 19 participants likely do not represent all community leaders or the lived experiences of the communities they serve in Chelsea and East Boston. Semistructured interviews were conducted over Zoom to allow flexibility but required strong internet connectivity and access to smartphones or computers. Virtual interviews may also mask certain body language, facial expressions, and/or emotional tone.
Conclusion
Identifying barriers and opportunities for air quality and extreme heat information sharing has the potential to outline avenues for collaboration and action-oriented work among Chelsea and East Boston community leaders and other community partners. Through this effort, we not only hope to support the City of Chelsea's and neighborhood of East Boston's future climate adaptation plans, but other community-based endeavors across MA and beyond.
Supplemental Material
sj-docx-1-new-10.1177_10482911241290557 - Supplemental material for Extreme Heat and Air Quality: Community Leader Perspectives on Information Barriers and Opportunities in Two Environmental Justice Communities
Supplemental material, sj-docx-1-new-10.1177_10482911241290557 for Extreme Heat and Air Quality: Community Leader Perspectives on Information Barriers and Opportunities in Two Environmental Justice Communities by Alina McIntyre, Leila Heidari, Michael Hagen, Roseann Bongiovanni, Bianca Navarro Bowman, Patricia Fabian, Patrick Kinney, and Madeleine Kangsen Scammell and in NEW SOLUTIONS: A Journal of Environmental and Occupational Health Policy
Footnotes
Acknowledgments
We thank the C-HEAT team: Boston University School of Public Health, GreenRoots, Inc., and C-HEAT Advisory Team members. We also express our gratitude to the study participants for their time and contributions.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a National Science Foundation Research Traineeship (NRT) grant (DGE 1735087), a National Institute for Environmental Health Sciences (NIEHS)/National Institutes of Health (NIH) grant (T32ES014562), a National Oceanic and Atmospheric Administration grant (NA21OAR4310313), and by a Barr Foundation Climate Grant (19-08038 and 22-34976).
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.