
Abstract
Background
Policy games can frame in silico interventions in public health. This study aims to map the WHO’s action framework for health equity, supported by social science theories, onto game components related to non-player characters in digital policy games. Embedded in social system theories, the WHO policy framework provides a robust knowledge base for designing policy games, highlighting the overarching problem and the social issues involved.
Method
Conceptual mapping is used to translate systems and agency challenges related to health equity into game components.
Results
Social system theories, with clarified subjective agency, are successfully used to map the WHO’s action framework to game components suitable for designing policy games aiming to improve health equity and how social determinants of health emerge and persist.
Conclusion
This study shows how a solid knowledge base can support the design and theoretical foundation of interventions in policy games addressing health equity. It focuses on configuring the game system and actions of non-player characters. This approach contributes to strengthening the development of non-character players in digital policy games and paves the way for future use of such games to explore and investigate how the structural determinants of health might be created, maintained, and disrupted, as well as revealing the unintended effects of interventions in simulated environments.
Keywords
Background
The health equity gap denotes unjust disparities in health outcomes within a country, arising from avoidable systematic disadvantages. The WHO’s action framework on health equity (Solar & Irwin, 2010) compiles decades of research to address these disparities. Whitehead and Dahlgren (2006; Dahlgren & Whitehead, 2006) highlighted how individual circumstances and national policies influence health. They introduced the term’ determinants of health,’ which includes living and working conditions, resource distribution, participation opportunities, and access to health services and social relationships.
The WHO framework (Solar & Irwin, 2010) can act as a knowledge base (Geurts et al., 2007) for simulating health equity interventions within complex social systems (Moore et al., 2019). The framework covers a wide range of determinants and their interactions, but often lacks operational precision, making it hard to identify how structural determinants function in specific contexts. It may obscure power dynamics, institutional practices, and historical contingencies. Emil Øversveen (2023) critiques its ambiguous use of ‘structure’, arguing that this reduces social determinants to static factors influencing health and overlooks how these determinants come into existence. The current perspective can underestimate how structures persist, evolve, or are disrupted through complex feedback mechanisms and agency. Øversveen’s reconceptualisation, rooted in social systems theories, offers a more nuanced analysis, recognising the bidirectional nature of structure and agency and the conditions for transformative change.
This enriched understanding broadens the scope for designing and evaluating interventions, as recommended by Moore et al. (2019). The reconceptualised approach adds mechanisms and processes underlying the enactment and transformation of health determinants. Thus, adopting this enriched WHO framework (Øversveen, 2023) as a knowledge base, this study aims to inform digital policy game interventions for health equity.
Studies highlight a persistent gap: while the impact of social determinants on health is well documented, tools to investigate how these determinants originate and persist within societies remain lacking (Øversveen, 2023). While games and simulations have advanced understanding of health behaviours (Squires et al., 2023) and policy effects (Boyd et al., 2022; Speybroeck et al., 2013), few studies incorporate structural determinants, with even fewer focusing on their shaping (Mudd et al., 2024).
This study proposes a digital policy game methodology, focusing on non-player character development to realistically simulate policy outcomes. This will enable the dynamic processes and mechanisms underlying the emergence and persistence of social determinants of health (Wilderink et al., 2022), as well as directly addressing the health equity.
Policy games address social complexity in analysis and planning (Mayer, 2009). They replicate real-world challenges in a simulated environment, helping stakeholders address specific problems (Mayer et al., 2014). Policy games enhance experiential learning, analysis, planning and decision-making about interventions or policies, such as municipal resource allocation prioritising the elderly over vulnerable children.
Policy game design begins with stakeholders constructing a shared knowledge base, which is then translated into game elements such as agents, rules, and environments (Geurts et al., 2007). Participants select and test interventions, with outcomes assessed by experts in live sessions or automatically in digital formats. For instance, a policy game may simulate a municipality facing economic inequality, where policymakers allocate resources to influence health outcomes and health equity.
In complex social systems, interventions aim to change the status quo by altering relationships, habits, and resource flows (Moore et al., 2019). Exploratory policy games accommodate uncertainty, providing a controlled environment for experimentation (Cureton & Coulton, 2024). This research focuses on digital policy games as experiential tools, emphasising the design of non-player characters to address health equity challenges and disrupt determinants of health.
The main research question is how a real-world policy framework, like the WHO’s, informed by social system theories (Øversveen, 2023), can be used in policy game design. The question is answered by diving into the design of non-player characters as citizens or policymakers in a digital experiential policy game. This study analyses how the game elements of agency, adaptation, and environment can be developed by mapping from a system-theory-informed knowledge base derived from the WHO framework. By reconceptualising a well-formed knowledge base as game elements with strong theoretical support, it is possible to build non-player characters that can help play out highly realistic digital policy scenarios.
The contributions of this study include:
Demonstrating how a policy action framework on health equity can be transformed into a knowledge base to guide policy game design, such as progressive taxation impacting non-player characters’ economic resources.
Illustrating how social system theories, like those of Giddens, Luhmann, Foucault, and Bourdieu, can inform non-player character design.
Translating elements from the knowledge base into game elements; agency, adaptation and environment, to construct non-player characters’ attributes and behaviour in policy games, such as rules for healthcare seeking.
The next section introduces the WHO framework and explains its integration with social system theories, creating a knowledge base for policy game design. It provides an overview of the game world and types of computational interventions. It then outlines how the framework can be systematically mapped onto three central game elements guiding NPC design: agency, adaptation, and environment, operationalising health determinants within digital policy games.
Methods
This study uses conceptual mapping to create matrices with game components on one axis and key elements from health equality and social system theories on the other (Geurts et al., 2007). Conceptual mapping as an epistemic instrument (Marcasite & Goodyear, 2017) of translation is used in the area of knowledge translation (Baker & Ødemark, 2024) to link knowledge to practice. In this work, a knowledge base is linked to game components to simulate real-life scenarios. The belief is that explicit labeling and linking of words describing everyday complexity improve understanding and communication, without claiming any reference to actual practices (Baker & Ødemark, 2024). Knowledge translation aims to bridge the gap between general and applied research, termed evidence-based by Schmitt et al., (2024), and policy practice goals (Marcasite & Goodyear, 2017; Rynes et al., 2001). WHO defines knowledge translation as the synthesis, exchange, and application of knowledge by relevant stakeholders to speed up the benefits of global and local innovation in strengthening health systems and improving people’s health (World Health Organization, 2005). Concept mapping is often the first step in knowledge translation.
The following sections present the WHO framework (Solar & Irwin, 2010) along with Øversveen et al. (2017, 2023) incorporation of structuration theory, drawing on Anthony Giddens and Pierre Bourdieu. To demonstrate the potential for including other theories, Niklas Luhmann and Michel Foucault are also considered. This section concludes with mapping the knowledge base into the game world and the game elements — agency, adaptation, and environment.
The Knowledge Base
The WHO framework for action on the social determinants of health (Solar & Irwin, 2010) have two conceptual layers. The first layer, health equity, is called structural factors. The second layer is the determinants of health, addressed as intermediary factors. While changes in the first layer change health equity, changes in the intermediary factors can increase inequalities, even if the health of the population improves. The WHO framework rests on a solid cluster of four major theories of social inequality in health, as the materialist, psychological, social determinants, and life-cycle explanations (Bartley, 2016; Marmot, 2015; Øversveen et al., 2017). A common denominator in this body of research is that socioeconomic status, or position, in a hierarchically oriented society, is believed to be the critical driver for health equity (Øversveen, 2023). The materialist approach focuses on access to resources as crucial for developing health. The psychological approach finds the personal experience of living with low social status or material or social deprivation as challenging to health. Social determinants are a cluster of structural elements that form humans and their material and immaterial environment. Within the life-cycle explanations, specific events in life are believed to follow and affect a person’s health later in life, such as exposure, stress or malnutrition in early childhood. The competition among the explanatory theories is small, leading to an agreement that they all contribute to a broader explanation of health inequalities (Øversveen et al., 2017).
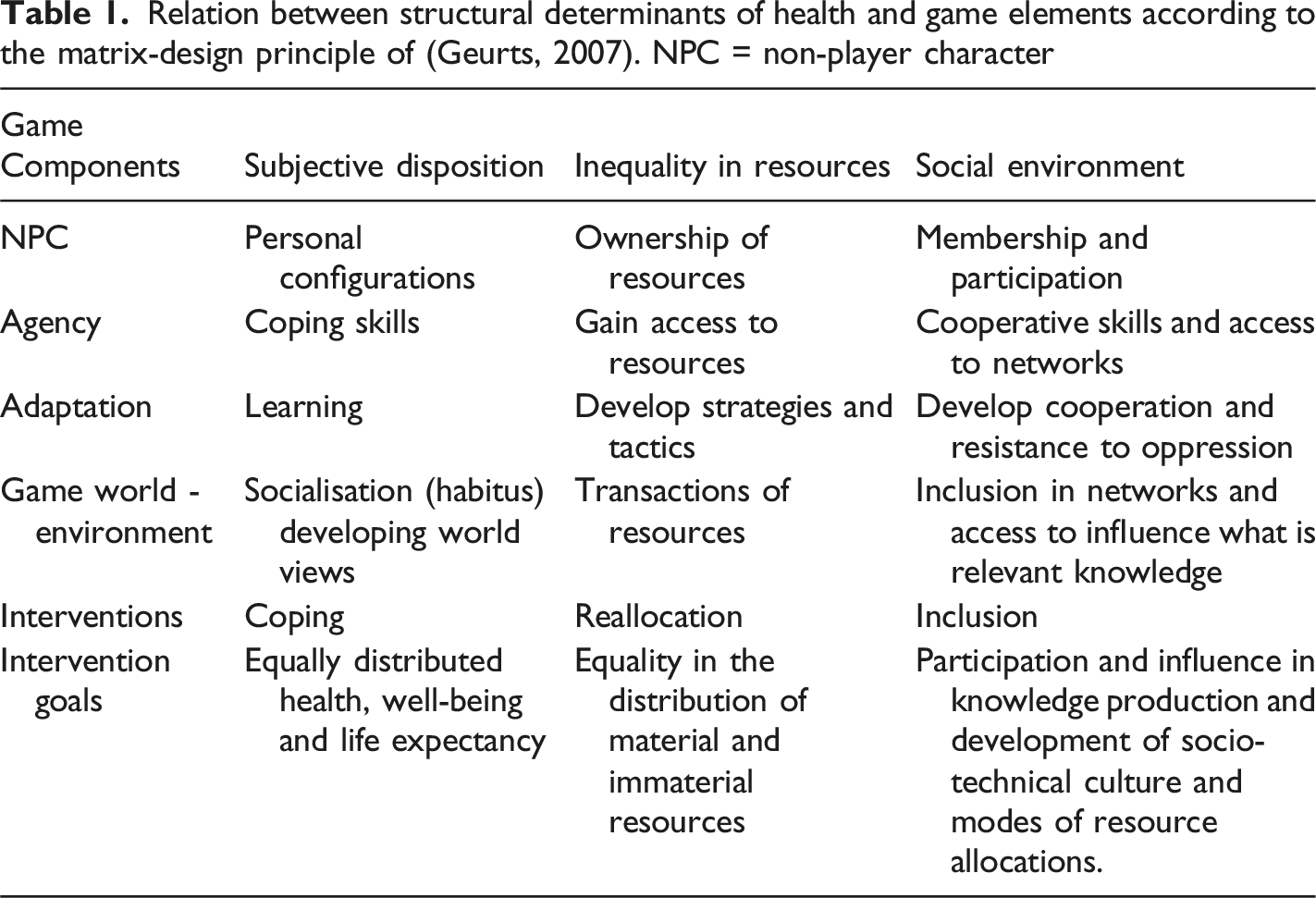
Øversveen et al. (2017) offer a major critique of the WHO framework (Solar & Irwin, 2010) and health inequality research highlighting inconsistencies in the use of the term structure and its relationship to the critical explanatory variable, social status. Øversveen (2023) claims structures are assumed in this body of research, missing out the focus on interventions able to disrupt the structural determinants of health themselves. His point of view is consistent with the turn to complex systems thinking in current social epidemiological interventions on health equity (Boyd et al., 2022). Øversveen (2023) identifies two significant branches of interpretation of structure in health equity research and the WHO framework. The first is inequality-as-structure, and the second is structure-as-components. To mitigate the divide, Øversveen (2023) suggest using three distinct structural determinants: (a) subjective disposition as the social embedded in our mental states and physical bodies, (b) the resource inequalities as distribution of material and immaterial resources and (c) the social environment embracing the social hierarchies. The three types of structural determinants are next embedded as part of a triad with practice and health outcomes as outlined in Figure 1. Structural determinants establish the objective and subjective conditions of social practices. Triad of process, determinants and outcomes in WHO framework as re-conceptualised by Øversveen (2023)
The Wrapping in Social System Theory
Øversveen (2023) uses Giddens (2004) structuration theory to clarify the concept of structure in the WHO framework (Solar & Irwin, 2010). Øversveen (2023) suggests that according to structuration theory, we should focus on the social practices that create, recreate or disrupt the social determinants, and not only treat them as causes of health. Giddens (2004) defines structure as rules and resources involved in the reproduction of social systems, existing as memory traces, and instantiated in action (Øversveen, 2023). According to Giddens (2004), a social system is the patterning of social relations across time and space, understood as reproduced practices. In structuration theory (Giddens, 2004), structural determinants come to life through these practices in which persons reflexively engage. Reflexivity involves a person’s belief in the connections between causes and effects of events. The core of structuration theory is these reflexive practices in which actors produce, distribute and consume material and immaterial resources according to subjective dispositions, thereby either reproducing or disrupting the structural determinants of health.
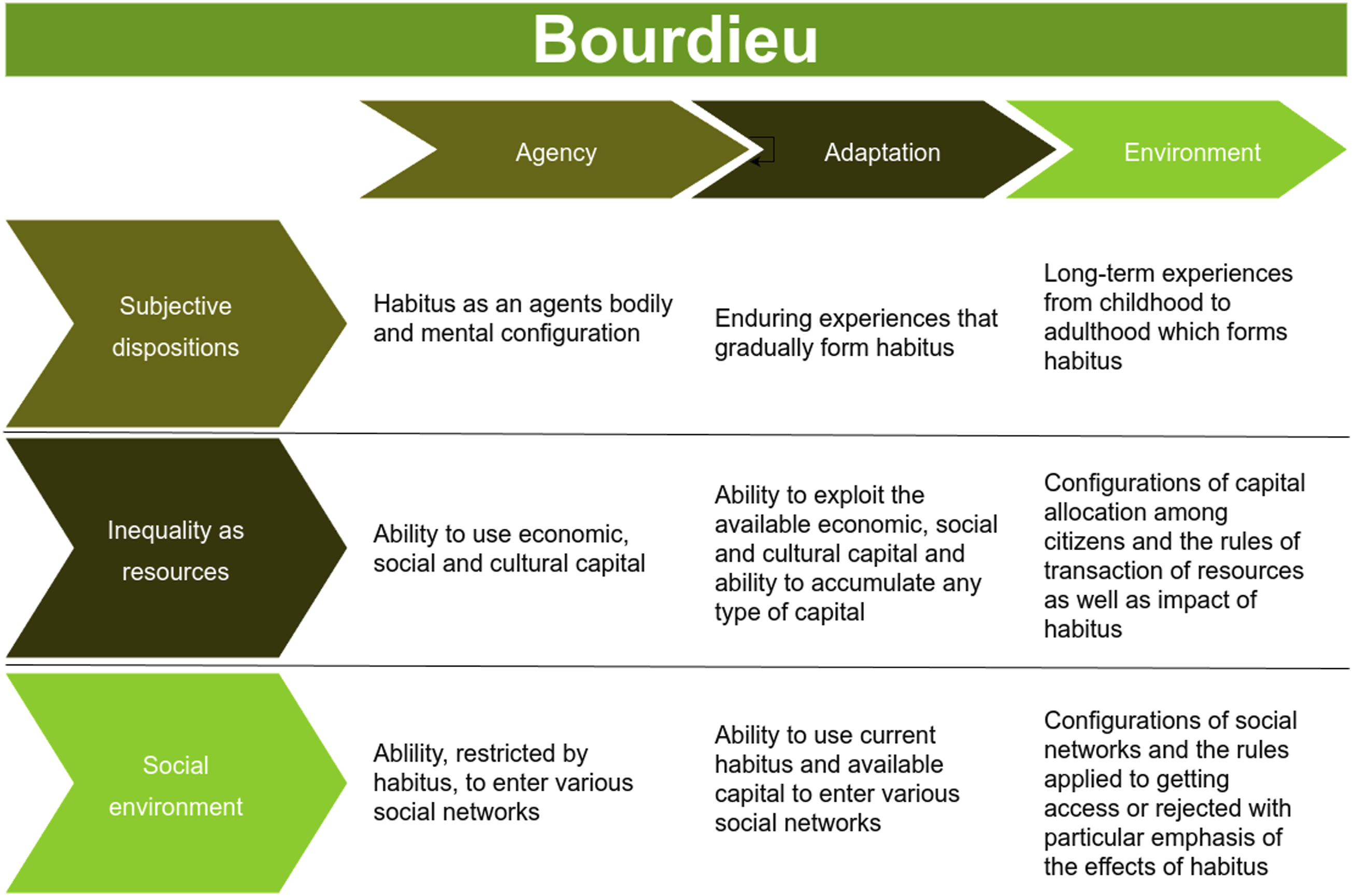
Øversveen (2023) also uses Bourdieu (2016) term habitus to embrace the concepts of subjective dispositions and the economic, social and cultural capital to describe the concept of inequality in resources. Habitus refers to an individual’s physical and mental configuration, including habits, skills, and perceptions of their environment. Social capital refers to the resources embedded in supportive networks and a person’s position whitin certain social hierarchies. Cultural capital is education and mastering the symbolic spaces of social life, like speaking foreign languages and having knowledge of the arts. Both social and cultural capital are acquired through lifelong social interactions and used to accomplish tasks. Economic capital is money and ownership of any material resources.
The structural determinant of subjective dispositions involves reflexivity, where agents learn from past actions and apply new strategies to utilise available resources to accomplish a task. Subjective dispositions, seen as habitus, encompass the mental and physical skills developed within a social environment. Health is a mental and physical attribute linked to this determinant.
Resource inequality is established through the long-term circulation of material and immaterial resources. Transaction and distribution rules can produce, reproduce or disrupt the configuration of resource inequality. The concept of capabilities in structuration theory (Giddens, 2004) refers to an agent’s ability to use material and immaterial resources to achieve goals. Effective resource use is also intertwined with subjective dispositions.
The structural determinants of the social environment are the configuration of involved networks and social hierarchies. According to Bourdieu (2016), habitus and possession of capital place people in social hierarchies. Institutions are formalised networks created through long-term practices. Social position, key to theories on health equity, refers to people’s placement in roles in different networks. To attain a position, one needs a suitable habitus, sufficient capabilities, including resource access, and entry into the relevant networks.
The Other Theories on the Social
Niklas Luhmann and Michele Foucault’s theories demonstrate the applicability of various theories for policy game intervention design. Here is a brief introduction to their core ideas on agency and adaptation.
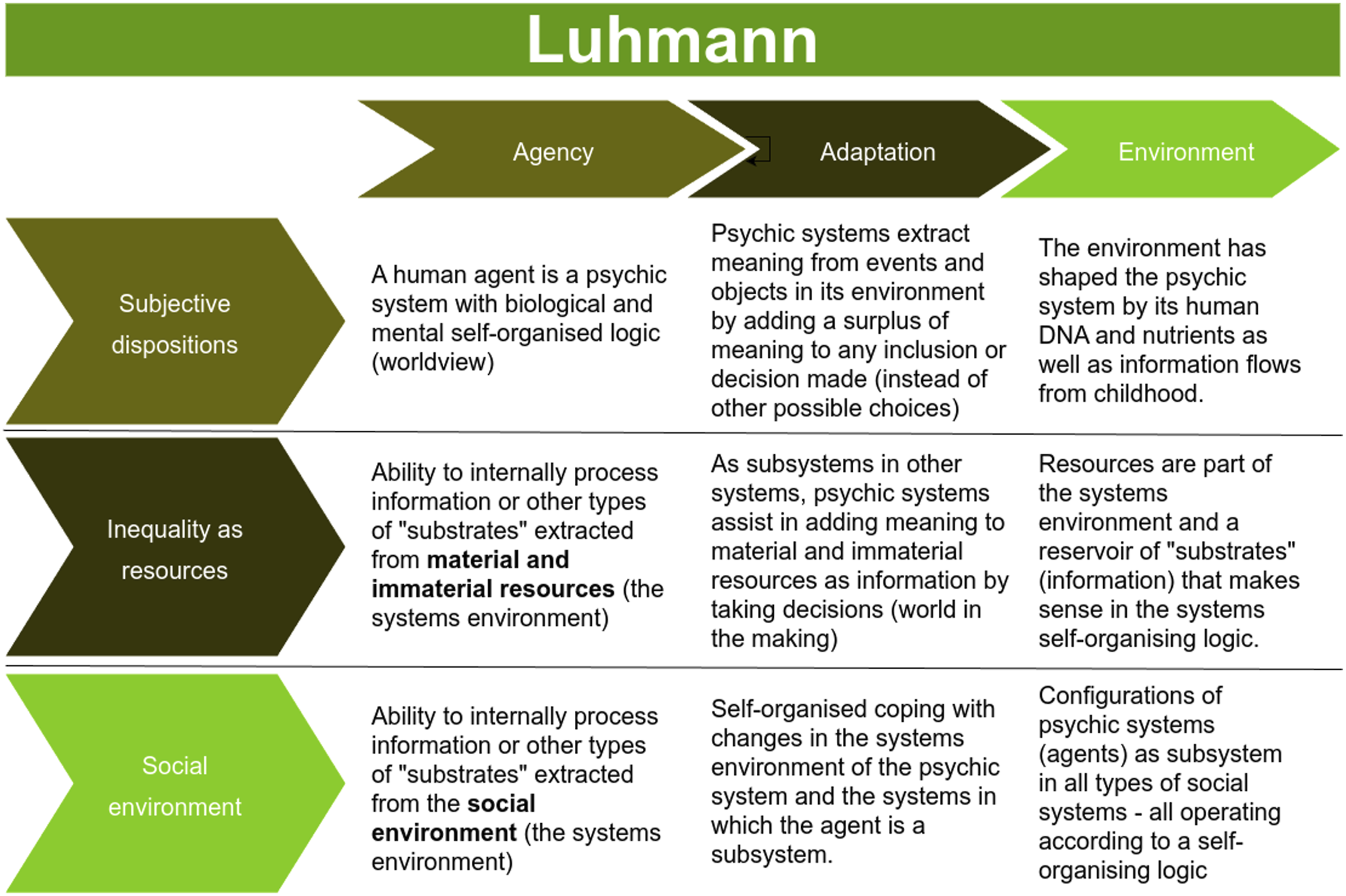
Luhmann (1995) views a social system as a self-organised entity inspired by Maturana and Varela’s concept of autopoeisis (Maturana & Varela, 1980), an organism’s internal self-organising system of maintaining life. Systems adapt to digestible substrates from the environment; in social systems, this substrate is information, which only makes sense internally within the system.
A social system cannot observe itself, but has control over its internal processes. Luhmann argues that humans are psychic systems, including their physical bodies, functioning as a subsystem in other social systems. Humans extract surplus meaning by selecting one decision instead of any other possible decisions. The produced meaning establishes what makes sense in the world. Luhmann’s social system theory centres on information flow, rather than human interactions.
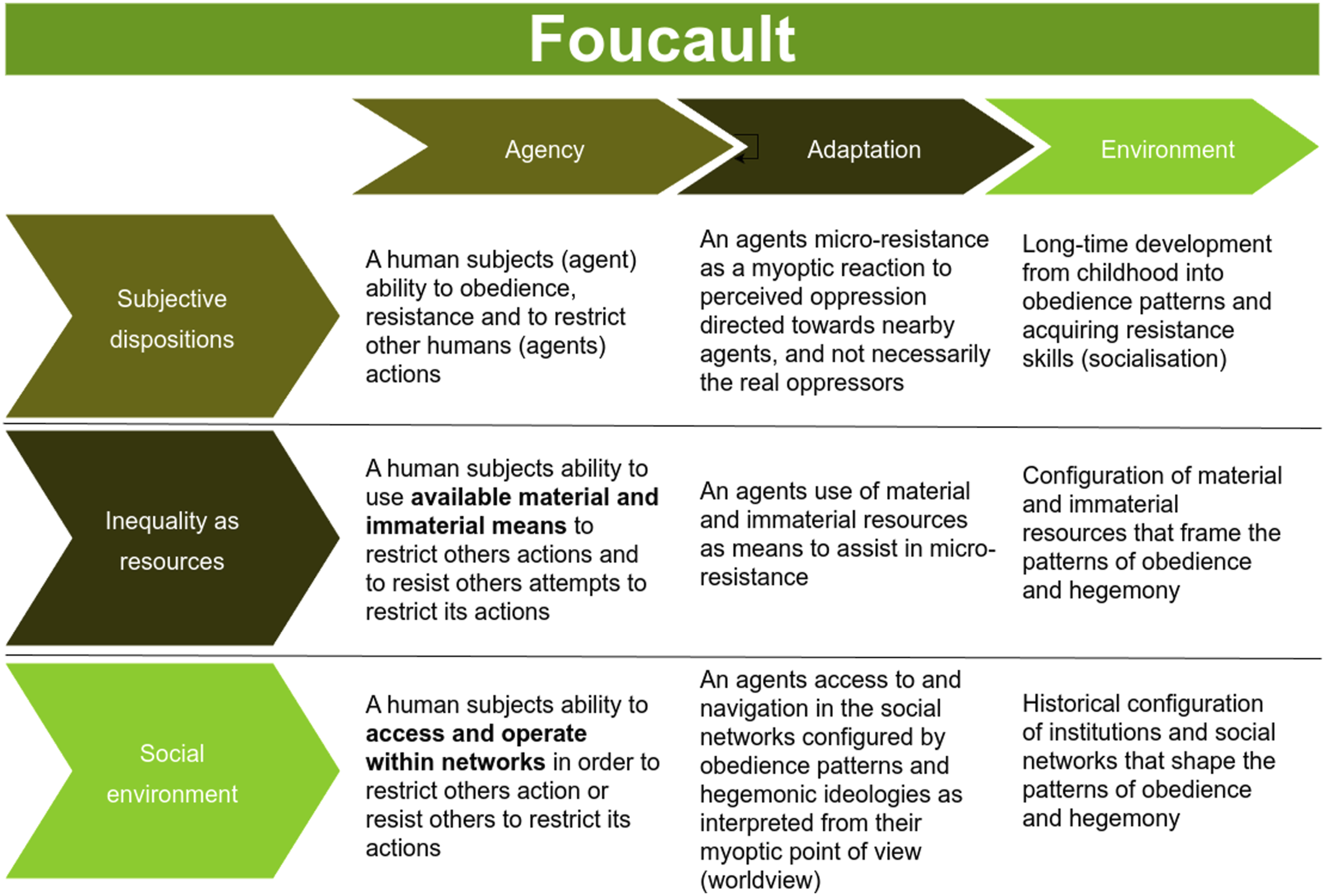
Foucault (1982) views social structures as emerging over historical times from actors preventing other actors’ actions, a process he calls micro-power - the primary driver of human agency. According to Foucault, actors often focus on perceived oppressors nearby, engaging in myopic power struggles rather than countering true oppressors. Instead, actors focus on actors close to them and whom they, often wrongly, perceive as oppressors. He is concerned with hegemonic knowledge, created through these myoptic micro-power battles and the often subtle methods of imposing disciplinary actions on others. The most efficient method is to get actors to voluntarily restrict their actions by means of imposing religion or other hegemonic knowledge. Actors who resist tend to use myopic counteractions, which usually fail to defeat real oppressors.
Øversveen (2023) strengthens the WHO framework by incorporating Giddens’ structuration theory and Bourdieu’s concepts of habitus and capital, creating a stronger knowledge base for game design. Suggesting other applicable theories not only informs and expands design options but also strengthens the explainability of simulated interventions. The knowledge base, at this stage, depicts the “big picture” of health equity in line with the policy game development framework of (Geurts et al., 2007). A knowledge base is an organised database of technical, scientific, and procedural knowledge for developing, simulating, and evaluating policy interventions. Game design (Brathwaite & Schreiber, 2009) are used to extract the logic, narratives, and adaptive mechanisms embedded in knowledge bases (Geurts et al., 2007) such as the WHO’s social determinants of health to mimic real-life policy-making and its impacts.
The following section describes the game world and computational evaluation of interventions in a policy game, followed by a dive into the three game components; agency, adaptation and environment.
The Game World and Policy Interventions
The gameworld is a fictional environment populated by players and non-player characters (Cureton & Coulton, 2024; Fernandez-Vara, 2019). Brathwaite and Schreiber (2009) note that game world design involves creating the game’s backstory, setting, and theme, while system design involves creating rules and mathematical patterns essential for gameplay. Actions allowed or restricted for players or non-player characters define the nature of the game world (Cureton & Coulton, 2024; Fernandez-Vara, 2019). Although the game world does not need to reflect the real world, policy games often do (Cureton & Coulton, 2024). Conceptual mapping can be used to connect game design and the real world.
A policy game intervention uses a chosen player strategy or simulation setup to feed certain conditions and actions into the complex adaptive system, exploring how it plays out. Policy game interventions are guided by what-if questions posed to the knowledge base (Pettit et al., 2015). A digital game evaluates an intervention computationally, presenting results in summaries of analysis. Detailed techniques for simulating interventions are documented elsewhere (Ansoms & Geenen, 2012; Duchatelet et al., 2022; Hofstede & Pedersen, 1999; Lukosch et al., 2018; Mayer et al., 2014; Moore et al., 2019; Szczepanska et al., 2022). A brief example is the heterogeneous treatment effect analysis (Wager & Athey, 2018), a machine learning algorithm that calculates health outcomes from observational data, suitable for evaluating health equity and socioeconomic impacts in the game world.
Agent-based social simulations explore agents’ practices – used for driving non-player characters in games like SimCity (Cureton & Coulton, 2024), which create, maintain or disrupt structural determinants (Boyd et al., 2022; El-Sayed et al., 2012; Galanis & Hanieh, 2021; Silverman et al., 2021; Tolk et al., 2022; Wilderink et al., 2022). These models replicate and analyse emergent results agents’ interactions with micro-level rules (Gilbert, 2006), acting as tools for investigating how practice shapes the structural determinants. Formalised social agent-based models can be seen as configurations of a social system theory (Antosz et al., 2023). Since the 1960s, social agent-based models have simulated cooperation, diffusion of norms, cultural dynamics, and health behaviours (Bianchi & Squazzoni, 2015; Elsenbroich & Polhill, 2023; McAlpine et al., 2020; Squires et al., 2023; Will et al., 2020). Polhill et al. (2021) discuss computing limits when agents’ actions affect subsequent agents, a core aspect of the micro-power interactions suggested by Foucault (1982). Szczepanska et al. (2022) discuss how social agent-based models currently are and can be implemented in games. Applying agent-based models to the non-player characters’ actions can assist in calibrating the game mechanics to real-world data to ensure relevance for policy planning (McCulloch et al., 2022; Yiannakoulias et al., 2024).
While computational social simulations have explored aspects of Luhmann’s theory on social systems (Barber et al., 2006; da Silva et al., 2008; Leydesdorff, 2009; Lukosch et al., 2018), and a combination of Luhmann and Giddens (Leydesdorff, 2009), similar works on theories by Bourdieu and Foucault are less known. These theories offer potential for computational exploration within policy interventions and gaming, enhancing social science insights to computational social simulations.
In the next section, the knowledge base on health equity is used to develop game elements particularly relevant to non-player characters desig, agency, adaptation, and environment.
The Game Elements
Consider the perspective of a policymaker navigating a game world designed to reflect real-life complexities. The objective is to improve decision-making, answer what-if questions (Pettit et al., 2015), and examine both intended and unintended consequences in realistic scenarios. This raises a key question: how can we design non-player characters whose traits (Falck, 2025), behaviours (Klinkert & Clark, 2021; Babichenko et al., 2020), and constraints authentically mirror those of real people (da Silva & de Souza Ribeiro, 2021)?
Assume a municipality facing a dilemma in allocating resources to either elderly sick or young people. The citizens vote for national government, which influences progressive taxation policies based on political views. Economic inequalities, one of the social determinants of health, can be disrupted in this scenario if sufficient political support for strong progressive taxation. If we wanted to place this scenario in a visual environment world, the game mechanics and customisability in urban development game City Skyline can be a point of departure. However, simpler user interfaces like a dashboard can also suffice. When such comprehensive overall game design is outside the scope of this text, the next section will elaborate on the non-player characters. In the next sections on agency, adaptation and environment design suggestions derived from the WHO knowledge base linked to this scenario are outlined.
Agency
In a game, agency refers to situations where non-player characters (NPCs) access resources or use their capabilities to cope (see Figures 2–5). This agency considers citizens as non-player characters, not players acting as policymakers. However, players can be both citizens and policymakers, equipped with capabilities, like any other citizen of the game world. NPCs, like elderly and young citizens in the municipality have roles defined by societal and social group expectations. An NPC ‘s social position, impacting health inequality, is influenced by collectively valued attributes like education, wealth, and status. Simulations examine how an agent’s health, capabilities, and roles evolve. Health affects an agent’s ability to fulfil roles, access resources, and ultimately their position in society. An NPC typically has multiple social roles, such as family member, friend, employee, and voter with roles carrying action rules. An NPC’s subjective dispositions can modify general role behaviour, a central mechanism of social inclusion or exclusion according to Bourdieu (2016). Giddens (2004) theory of structuration translated into a game matrix of structural determinants of health and game elements agency, adaptation and environment Bourdieu (2016) theory of the social translated into a game matrix of structural determinants of health and game elements agency, adaptation and environment Luhmann (1995) theory of the social systems translated into a game matrix of structural determinants of health and game elements agency, adaptation and environment Foucault (1982) theory of social structures translated into a game matrix of structural determinants of health and game elements agency, adaptation and environment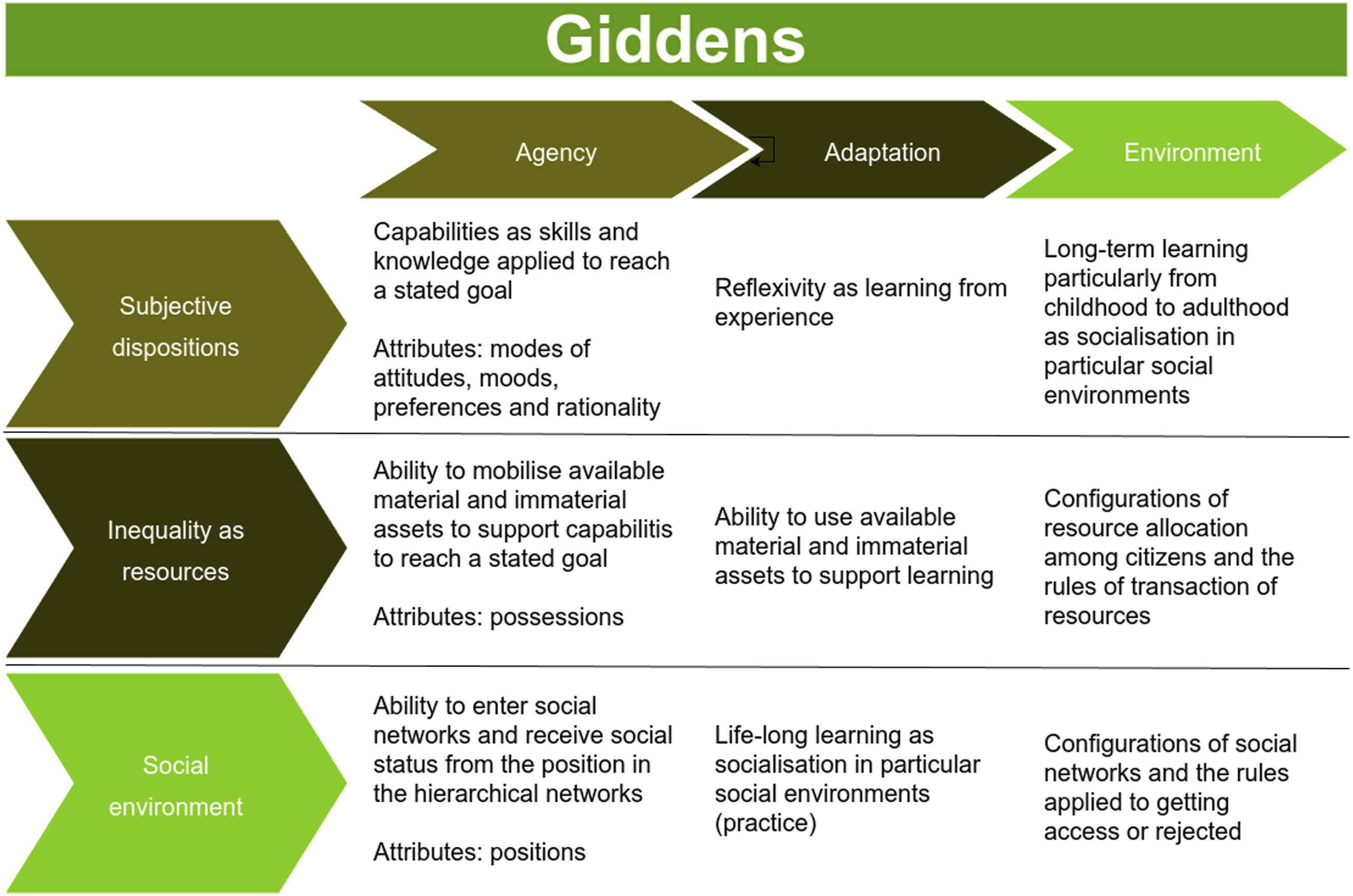
Giddens (2004) views agency as capabilities and reflexivity, inviting NPCs learn from experiences and exploit resources. Young NPCs that seeks education, not only collects cultural capital, but then also skills to obtain high paid jobs in the future. Elderly NPCs with health issues not seeking health care, either because of lack of knowledge, money, access or beliefs of social stigma, have a chance to die earlier.
Luhmann (1995) theory focuses on the prodcution of meaning and the exchange of information within a system. Agency, as an exchange of information, accumulates meaning, influencing future decisions. NPCs engaging in dialogue, produce meaning resulting in either propensity for seeking or refusing education, health care, engage in community activities or to vote for particular party.
Foucault (1982) describes NPCs’ strategies as micro-power, where resistance occurs within their immediate sphere, though the actual source may be elsewhere. NPCs struggle to identify the true source of oppression due to a restricted, myopic horizon. Elderly NPCs not getting necessary health care might blame their family members and local politicians or the young NPCs, while the municipality’s overall economy, restricting services, mostly are caused by other external factors like global recession or state taxation policies. The latter is not easily observed. Foucault suggests analysing NPCs’ actions that prevent other NPCs’ actions to understand power plays. In the dilemma of either funding the elderly NPCs health care or supporting the young NPCs a policymaker NPC (or player) do prevent the loosing NPCs room for action. In non-player character design, such analysis could inform rule construction and their relation to chosen interventions.
Bourdieu (2016) focuses on the young NPCs’ long-term learning or socialisation as not only upbringing and education, but also peer learning, resulting in an NPC’s habitus and its impact on accumulation or loss of economic, social and cultural capital. Habitus affects access to economic, social, and cultural capital. Bourdieu explains interactions between NPCs through habitus, emphasising access it as a ticket to acces networks and capital.
To address disruptions of social determinants of health described in the WHO knowledge base, agency in policy games should be viewed through both NPCs health outcomes and their contribution to disruptions or subsistence of the structural determinants (Øversveen, 2023). The disruption can be staged by i.e. NPCs actions of voting, educational choices, access to influential networks, and civic engagements.
Adaptation
Adaptation refers to how NPCs respond to changing environments and past strategies, learning to handle similar future tasks. This process includes coping with new situations and accessing external resources, such as other NPCs for support (see Figures 2–5). Giddens (2004) describes capabilities as a combination of NPCs ' subjective disposition (Klinkert & Clark, 2021; Uludagli & Oguz, 2023) and access to material or immaterial resources (the structural determinant inequality-in-resources), which indirectly affect their status in hierarchical social networks by either facilitating or hindering access to resources. Reflexivity, the ability to learn from experience, relies on these resources to develop successful strategies.
Foucault (1982) is less optimistic than Giddens, arguing that NPCs often have a limited view of their environment, making it difficult to adapt strategies to counteract oppression from their positions in social hierarchies. NPCs hence, should operate in restricted areas of the environment. A young NPC does not know much about the situation for the elderly in the municipality, and might not be aware of the dilemmas of local policy makers and politicians or the impact of state taxation programs on his or her situation. To gain awareness, NPCs must communicate, and a few may help others become aware of their situations. Foucault (1982) emphasises that the major driver is hegemonic knowledge, an emerging phenomenon shaped by the often uncoordinated collective actions of the NPCs and players over long periods. In a policy game the hegemonic knowledge can translate to the historically selected policy interventions and the common tendencies these policy choices represent. Measured on the level of NPCs in our scenario example this manifests as i.e., voting patterns and young NPCs choices of education.
Luhmann (1995) theory sees NPCs as sub-systems in social systems, with learning understood as a self-organised adaptation to changes. The NPCs subjective disposition, can be interpreted as such self-organising entity, prone to reproduce actions according to their psychological profile (Klinkert & Clark, 2021). Changes in the self-organising logic of the NPC is less and less likely as the NPC grow older.
Learning, or adaptation, occurs over different game timescales, from hours to generations. Structural determinants of health are persistent (Wilderink et al., 2022), and usually change slowly over historical time but can occasionally shift rapidly. In the scenario above a 20-30 year span embrace the young NPCs adaptive voyage from childhood to working age, through socialisation, education and ending up with socially stratified jobs or unemployment, placing them in the social hierarchies of their artificial society. The pattern emerging from placing NPCs in the social hierarchy is postulated by the WHO knowledge base to be one of the strongest predictors of health inequality. A quest in a policy game can be to find the paths to hierarchic structures with strong and persistent health equality.
Environment
In a game, the environment encompasses the game world’s visual and structural elements, mirroring i.e., the WHO knowledge base. For health determinants, the environment includes the socially ordered, material and immaterial elements.
NPCs experiences and histories. As the main focus in this paper is the design of NPCs and not the complete game world, the relevant issues related to environment is what kind of feedback NPCs receive from the environment in response to its actions. This can be boiled down to another NPCs reaction. However, social norms, national laws and other rules of transactions like progressive taxations are above the NPCs level and needs to be dealt with in the game. Each NPC has a limited perception of the environment, similar to a worldview or pre-understanding in real life. Over time, new experiences can reshape worldviews (Gadamer, 2003). Bourdieu’s concept of habitus describes how experiences shape NPCs ' subjective dispositions. Luhmann’s theory equates NPCs ' self-organising logic to their worldview and subjective dispositions. However, the NPC gets input from the environment and its actions feedback to the environment. If the inputs from the environment, like lack of necessary health services, occurs, the NPC might die. Likewise, if a young NPC operates on its self-organised logic resulting in failed education, it might later not obtain sufficient income to maintain its well-being. Foucault, like Bourdieu, recognises how experiences are embodied in obedience to authority. NPCs with habitus, or subjective dispositions without the necessary capabilities (Giddens, 2004) to resist against i.e., municipality’s denial of health care services or lack of educational support, will suffer, while NPCs with strong capabilities can get to the denied services through other pathways. In these situations the environment poses challenges to the NPCs that they need to deal with. These can be challenges that feedback from i.e., NPCs voting for parties that promote policies increasing economic inequalities. The NPCs voting can be influenced socially by other NPCs, and later the effects turn out counter productive. Game world rules involve algorithms for the distribution and transactions of knowledge and resources, the historical context serving hegemonic knowledge, and the demographic profiles. The game environment comprises the spatial distribution of NPCs, their subjective dispositions, resource allocation, and social hierarchies, forming the initial state of the game world.
Results
The main research question is how the game elements of agency, adaptation, and environment can be conceptualised through the WHO knowledge base. The previous section dived into the details of these game elements and outlined suggestions to power the design of non-player characters. The WHO knowledge base have three main pillars: subjective disposition, resource inequality and social environment that are translated into the three game components referring to four major sociological theories (Giddens, 2004; Bourdieu, 2016; Luhmann, 1995; Foucault, 1982), all of them grounded in agency driven social systems. The approach can design non-player characters for policy games to explore health equity, both from a traditional point of view -- regarding the social determinants of health mainly as causes, and from the radical point of Øversveen (2023) -- namely mechanisms disrupting the social determinants of health themselves. Designing non-player characters from the WHO knowledge base support both developing digital policy games as planning tools (Pettit et al., 2015; Mayer, 2009), research tools (Olejniczak et al., 2018) and as experiential learning tools (Mayer, 2009).
Relation between structural determinants of health and game elements according to the matrix-design principle of (Geurts, 2007). NPC = non-player character
Each theory is matched with the game’s components—agency, adaptation, and environment—in Figures 2–5. These figures suggest how to translate the extended knowledge base into game design approaches for setting up policy games or simulations to explore health equity challenges.
Discussion
Driving non-player characters in a health equity policy game should achieve two objectives. First, non-player characters must appear credible (da Silva & de Souza Ribeiro, 2021). Second, their agency and adaptation strategies should be tailored to the game’s specific tasks or interventions for validity. This study maps the WHO knowledge base onto non-player characters using four theories that link human actions to complex social systems; other theories can also be used. This approach connects directly to the three main pillars of the WHO knowledge base: subjective disposition, resource inequalities, and social hierarchies. Øversveen (2023) suggestion to include research on changing the social determinants of health themselves is also accounted for in the design proposal for non-player characters. However, the design suggestions do not cover other aspects, such as emotions (Klinkert & Clark, 2021), ranging from strong emotional intelligence to uncontrolled rage. Another limitation is that the theories do not cover the cognitive motives behind specific actions or pathways — crucial for human decision-making. Nonetheless, aligning the WHO knowledge base with game or simulation components helps explore and communicate the potential real-world impact of policy interventions, under certain assumptions.
Conceptual mapping does not capture all elements of translating knowledge into practice, such as in a policy game. Knowledge translation, as understood in evidence-based medicine (Schmitt et al., 2024) and science and technology studies, is often criticised for being too rigid and not reflecting real-life complexity (Baker & Ødemark, 2024). However, without guaranteeing validity in policy games when the WHO knowledge base powers non-player characters, conceptual mapping is valuable for making explorations explicit and for setting up games and simulations to better analyse complex adaptive systems.
The mechanisms for implementing the suggested non-player character design in digital games are not addressed, nor are the computational challenges it entails. This is a huge, largely unexplored area left to game developers and researchers.
Lastly, the purpose of digital exploratory policy games is only briefly suggested, as the current proposal for designing non-player characters for policy games on health equity can be applied to any purpose. Of particular interest for future research is how digital policy games grounded in health equality can serve as research tools to investigate the disruptive mechanisms suggested by Øversveens' structuration theory approach. Such studies can only be conducted through longitudinal cross-national case studies or meta-studies. Games or simulations can serve as in vitro laboratories to study such phenomena. Digital exploratory policy games have been suggested as research tools (Olejniczak et al., 2018), planning tools (Pettit et al., 2015), and combined educational tools (Mayer, 2009). It is left to future investigations to implement and validate the WHO knowledge base-derived design ideas for non-player characters in operational digital policy games.
Conclusion
Non-player characters in digital policy games on health equity is designed by mapping the core game components agency, adaptation and environment with the WHO framework (Solar & Irwin, 2010) turned into a knowledge base by strengthening the frameworks theoretical embedding. The suggested methodology paves the way for developing future policy games for research, planning or education.
Footnotes
Declaration of Conflicting Interests
The author affirms that there are no potential conflicts of interest related to this article’s research, authorship, and publication.
Funding
The author received no financial support for this article’s research, authorship, and publication.
Informed Consent
This study does not include any informants or study subjects.