
Abstract
Introduction:
The aim of this scoping review was to synthesize and summarize existing evidence for implementing and evaluating Cultural Safety initiatives in Australian hospitals for Aboriginal and Torres Strait Islander peoples. The rationale for this work was to establish guidelines for best practice in providing culturally safe care across hospital and health services.
Methodology:
A systematic search guided by PRISMA Extension for Scoping Reviews was conducted across five databases: CINAHL, Scopus, MEDLINE, Embase, and Informit. Reference lists and citations of eligible studies were also examined. Studies were eligible for inclusion if they were in English and discussed the implementation and/or evaluation of Cultural Safety initiatives in Australian hospitals. Evaluations assessing both health care staff and patient perspectives were included. Studies were excluded if they presented future implementation protocols or initiatives among health care students. No date limiters were applied due to the small body of available literature.
Results:
Nine studies met the criteria and were included in this review. Five themes emerged: (a) process of implementation; (b) process of evaluation; (c) change in health professional’s behavior; (d) change in patient behavior; and (e) future recommendations.
Discussion and Conclusions:
Validated implementation frameworks and evaluation tools are needed for integrating Cultural Safety initiatives into Australian hospital settings. This review has highlighted that despite the availability of evidence-based tools, their use was lacking. This scoping review also highlighted that evaluation of Cultural Safety initiatives is primarily focused on the attitudes and knowledge of health professionals, rather than patient experience. As Cultural Safety is determined by recipients of care, future evaluation of initiatives should prioritize patient perspectives.
Keywords
The strengths of Aboriginal and Torres Strait Islander peoples, embedded in culture and kinship, endure today despite the profound impact of colonization (Bourke et al., 2018). However, intergenerational trauma resulting from colonization continues to have significant influence on the health and social and emotional wellbeing of Aboriginal and Torres Strait Islander Australians (Smallwood et al., 2021). The impacts are perpetuated by ongoing racism and a lack of Cultural Safety in government systems and services, particularly hospitals (Durey et al., 2012; Parter et al., 2021). Consequently, the actions and responses of health care professionals who engage with Aboriginal and Torres Strait Islander people are critical to ensuring Cultural Safety in hospital settings. This requires attention to clinician knowledge and attitudes in relation to Aboriginal and Torres Strait Islander Australians as well as adoption of strategies that are known to deliver high-quality, culturally safe care. There is an existing strong body of evidence surrounding the development of potentially effective strategies, protocols, and models of care promoting Cultural Safety, such as the Daalbirrwirr Gamambigu (Safe Children) model (Flemington et al., 2022).
However, this body of evidence must be supported by knowledge about the implementation, evaluation, and sustainability of these models of care (Elvidge et al., 2020). Valid and sensitive evaluation tools used within robust implementation frameworks are needed. With this in mind, the objective of this scoping review was to provide insights from the available literature for the implementation and evaluation of Cultural Safety initiatives in Australian hospital settings. The research question was “How have initiatives aimed at improving Cultural Safety for Aboriginal and Torres Strait Islander people been implemented and evaluated in hospitals in Australia?”
Method
To answer the research question, a scoping review was undertaken guided by the PRISMA Extension for Scoping Reviews (PRISMA-ScR) (Tricco et al., 2018). A scoping review allowed for an adequately comprehensive overview of the recent literature to appraise implementation and evaluation strategies, as well as identify any significant gaps in the knowledge base (Tricco et al., 2018). The search strategy was formulated with librarian input. The protocol was not registered.
Eligibility Criteria
Studies were eligible for inclusion if they were in English and discussed the implementation and/or evaluation of Cultural Safety initiatives in Australian hospitals. Evaluations assessing both health care staff and patient perspectives were included. Studies were excluded if they presented future implementation protocols, as these have not yet been evaluated, or initiatives among health care students, as implementation of these differed significantly from hospital settings. No date limiters were applied due to the small body of available literature.
Information Sources
A systematic search was conducted across five databases in June 2023: Cumulated Index to Nursing and Allied Health Literature (CINAHL), Scopus, MEDLINE, Embase, and Informit. Reference lists and citations of eligible studies were also examined.
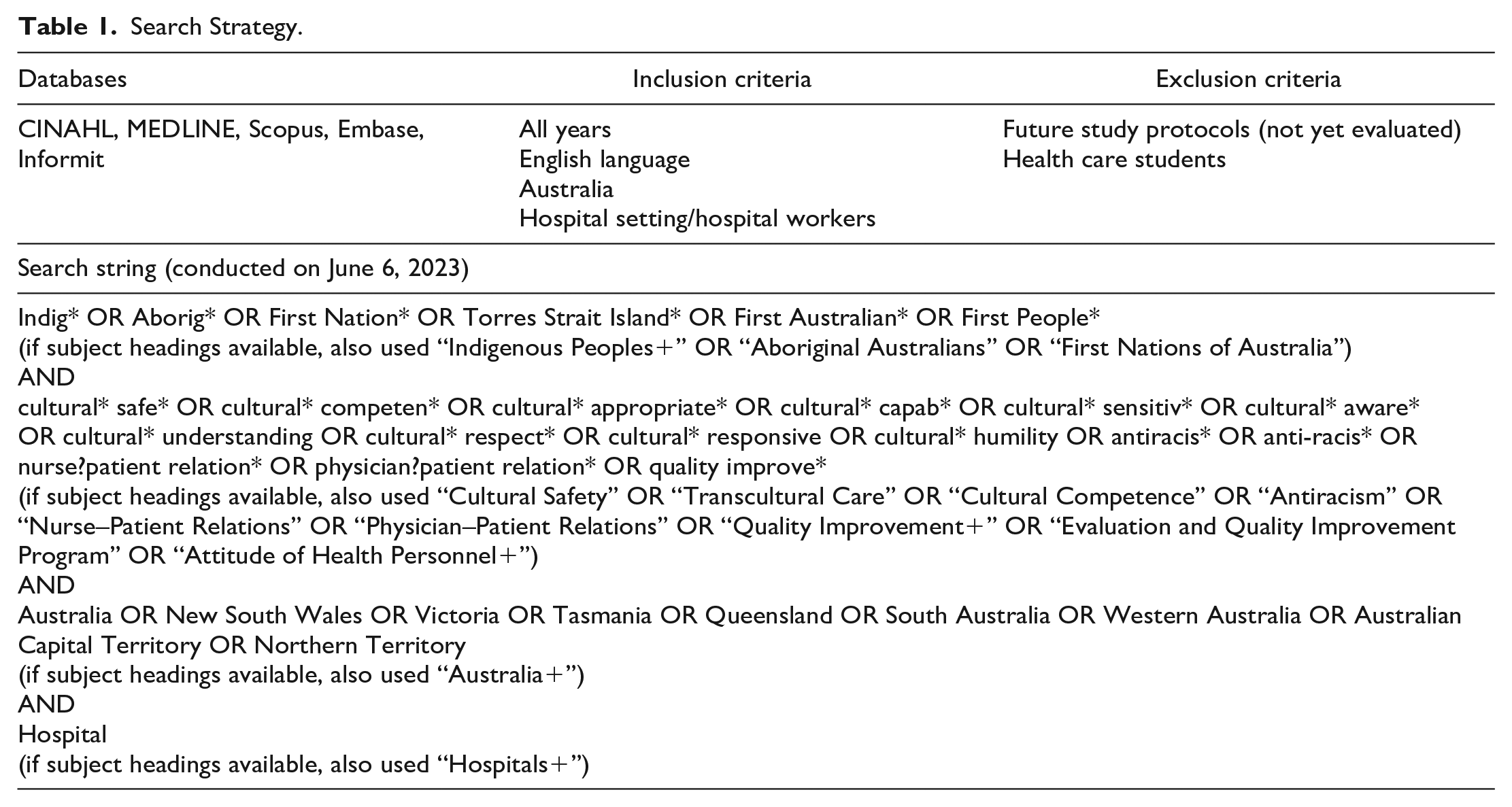
Search
The initial search was undertaken by the first author (B.C.). An example of the full electronic search strategy is provided in Table 1. The referencing program Endnote was used to save search results and remove duplicates (The Endnote Team, 2013).
Search Strategy.
Selection of Sources of Evidence
The titles and abstracts of search results were screened for relevance, followed by reading the full text of promising studies. Screening was undertaken by the first author (B.C.), under the guidance of her supervisory team. Any studies that prompted uncertainty regarding their inclusion in the review were read and discussed by all team members.
Critical Appraisal of Evidence
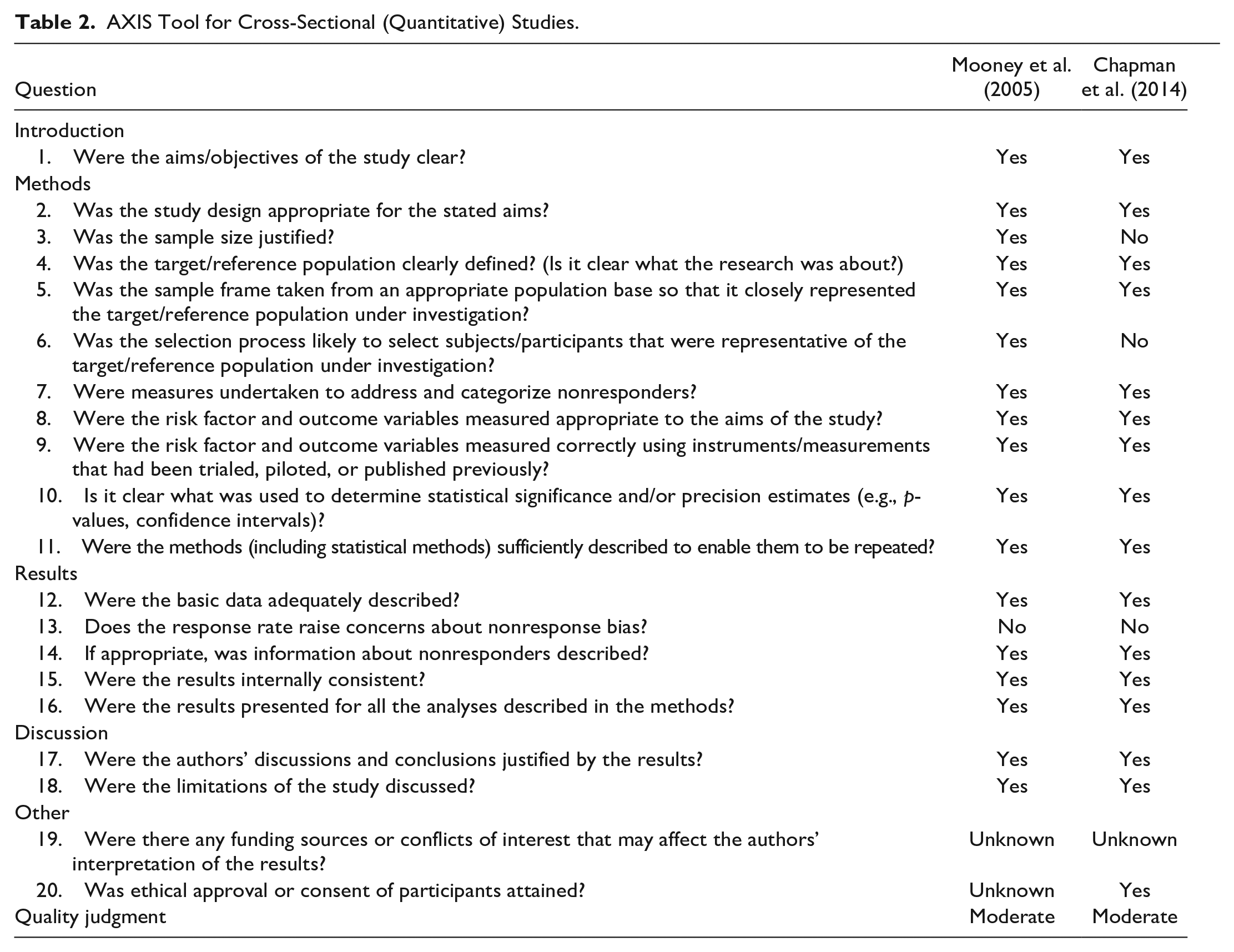
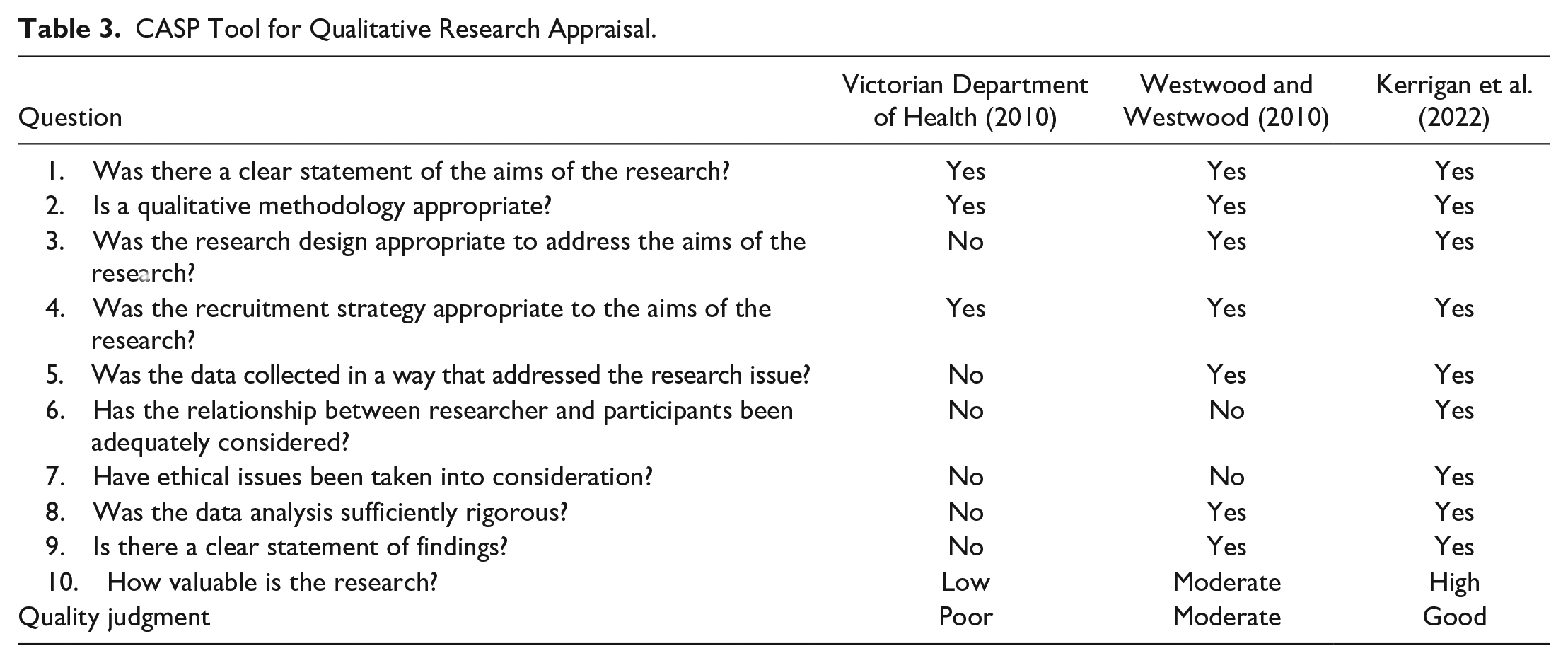
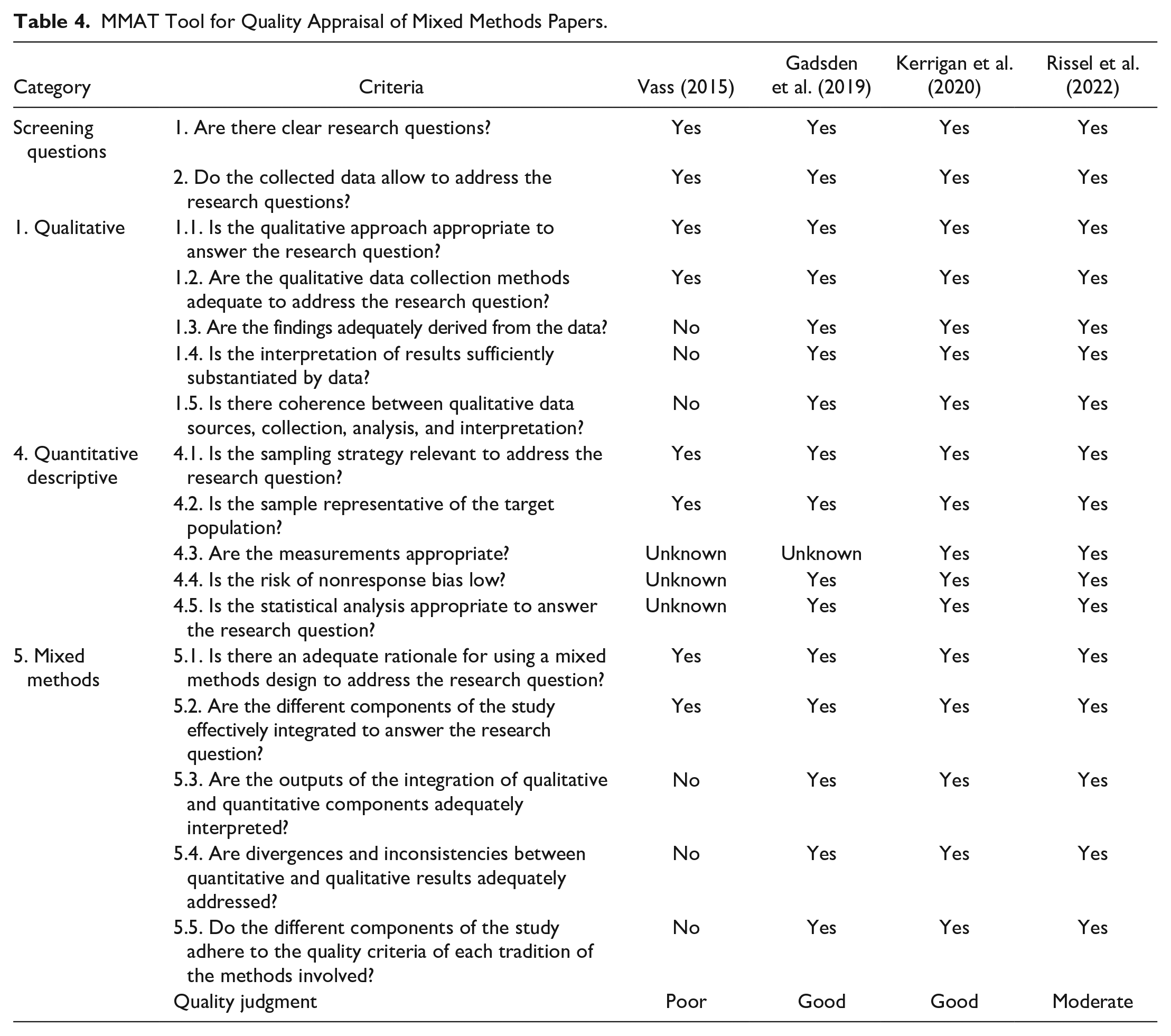
Studies were subject to quality appraisal utilizing the appropriate checklist for each study type, as depicted in Tables 2–4. Quality varied across the studies, although the majority were deemed to be of moderate or good quality. However, all results were included in the review regardless of quality due to the insights they could offer regarding the research question.
AXIS Tool for Cross-Sectional (Quantitative) Studies.
CASP Tool for Qualitative Research Appraisal.
MMAT Tool for Quality Appraisal of Mixed Methods Papers.
Results
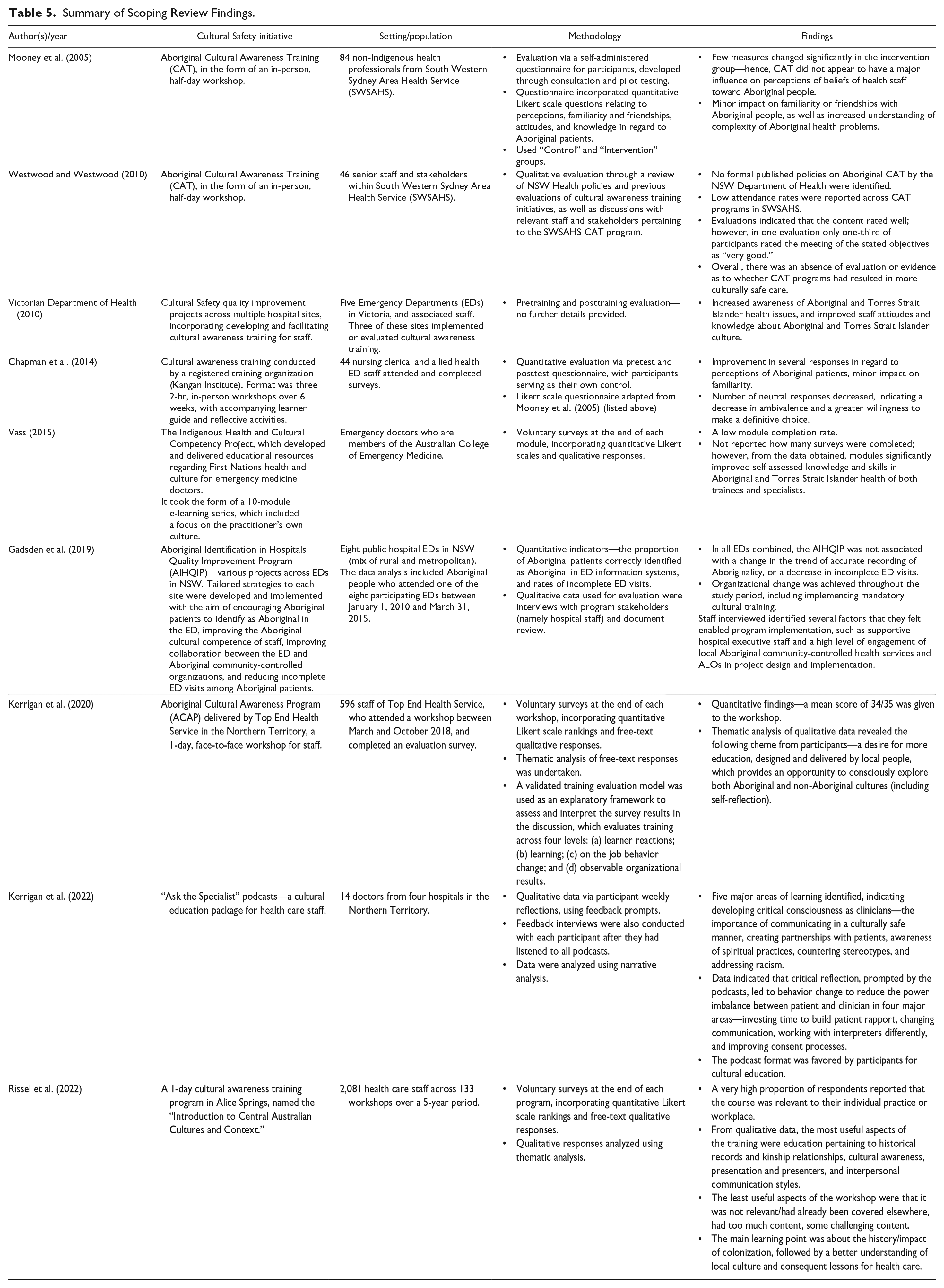
The search strategy resulted in 857 studies following the deduplication process, which were then screened according to the process in Figure 1, yielding 9 eligible studies. Excluded studies did not meet the eligibility criteria for this review. A summary of these studies is documented in Table 5. Full text of eligible studies were analyzed thematically drawing on Braun et al.’s (2019) six-step method. This analysis resulted in five themes: the process of implementation, the process of evaluation, change in health professional’s behavior, change in patient experience, and future recommendations.
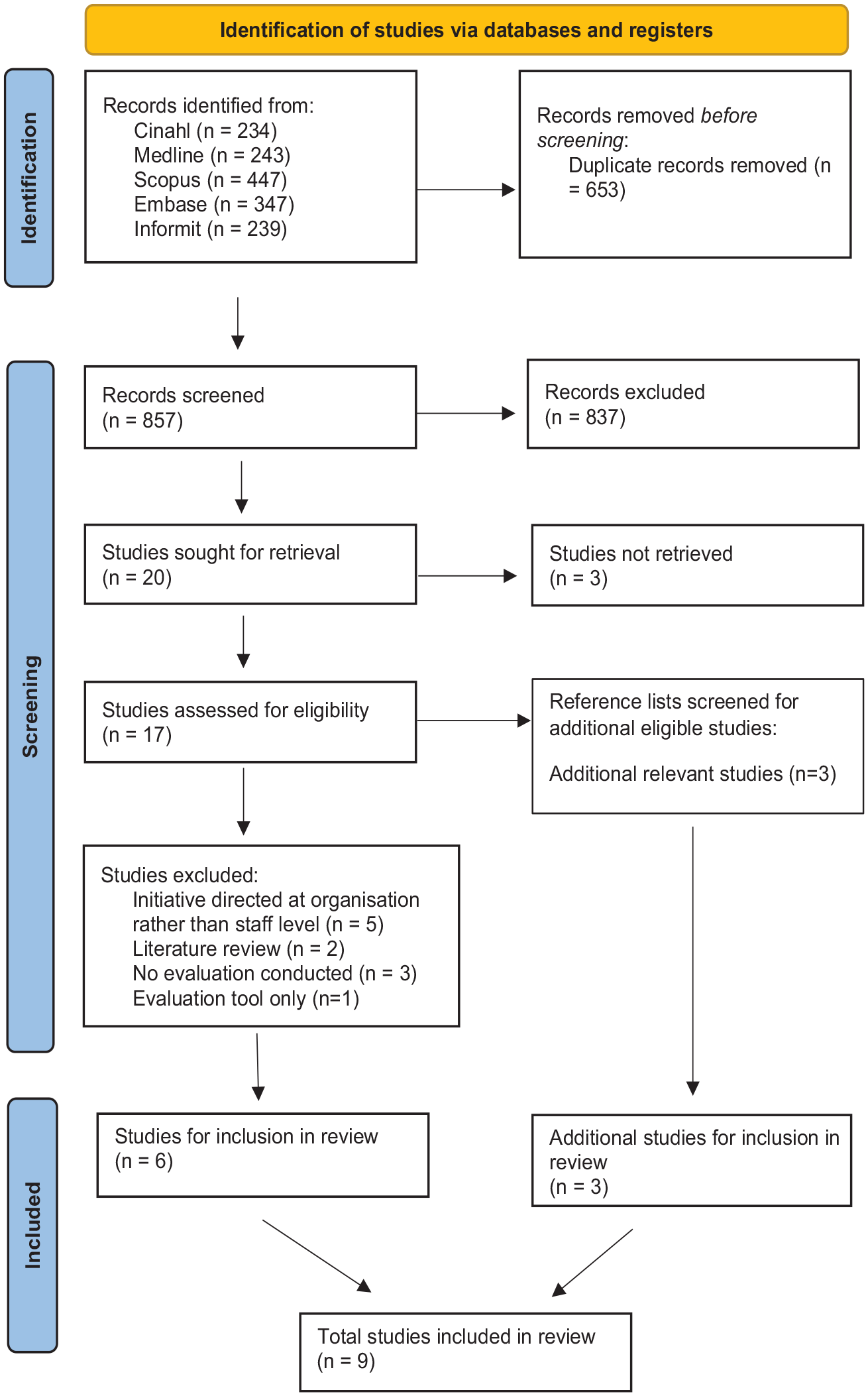
PRISMA Flowchart Depicting Search Results.
Summary of Scoping Review Findings.
Process of Implementation of Cultural Safety Initiative
Five studies implemented new Cultural Safety initiatives in hospital settings (Chapman et al., 2014; Gadsden et al., 2019; Kerrigan et al., 2022; Vass, 2015; Victorian Department of Health, 2010). Four studies conducted evaluations of preexisting initiatives (Kerrigan et al., 2020; Mooney et al., 2005; Rissel et al., 2022; Westwood & Westwood, 2010), which consequently offered minimal insight into the implementation process.
In examining the nature of the new initiatives, most were implemented across multiple hospital sites (Gadsden et al., 2019; Kerrigan et al., 2022; Vass, 2015; Victorian Department of Health, 2010), with only one study focused on a specific hospital setting (Chapman et al., 2014). A variety of staff were included in the initiatives, including nursing, medical, allied health, management, and clerical staff. It was unclear across all of the studies whether participation in the Cultural Safety training was on a voluntary or a mandatory basis. Most Cultural Safety training was in the form of in-person workshops, presented by Aboriginal or Torres Strait Islander facilitators. Only Chapman et al. (2014) identified that supportive learning materials were also provided and critical reflection was incorporated into the content. Two other initiatives were in the form of e-learning modules or podcasts that could be completed independently, targeted solely at medical officers (Kerrigan et al., 2022; Vass, 2015).
Overall, minimal detail was provided about the process of implementation itself, with the exception of the large-scale Cultural Safety quality improvement project in Emergency Departments (EDs) reported on by Gadsden et al. (2019). Gadsden et al. (2019) outlined in detail a thorough implementation protocol, including a 1.5-day preparation session for working group members workshopping the implementation process, regular site visits from project officers, and regular communication between working groups to share resources and advice.
Working groups were established to oversee implementation in three of the studies, each including at least one Aboriginal or Torres Strait Islander staff member or stakeholder (Gadsden et al., 2019; Kerrigan et al., 2022; Victorian Department of Health, 2010). Only Gadsden et al. (2019) and Kerrigan et al. (2022) identified the underlying theoretical frameworks used to guide their implementation. Vass (2015) alone helpfully identified barriers to implementation of Cultural Safety training, namely the varying levels of baseline cultural knowledge, particularly with international doctors, as well as the challenge of scheduling the training within a busy teaching program for doctors.
Process of Evaluation of Cultural Safety Initiative
All studies evaluated either a new or preexisting Cultural Safety initiative, although two studies evaluated the same preexisting Cultural Safety initiative in a slightly different way (Mooney et al., 2005; Westwood & Westwood, 2010). Evaluation was predominately undertaken among health professionals, assessing self-reported change in perceptions, attitudes, and behavior regarding First Nations patients, primarily using questionnaires. Use of an overarching evaluation framework was identified only by Kerrigan et al. (2020) and Kerrigan et al. (2022), in which Kirkpatrick’s training evaluation framework was utilized.
Three studies used solely qualitative evaluation (Kerrigan et al., 2022; Victorian Department of Health, 2010; Westwood & Westwood, 2010). Kerrigan et al. (2022) utilized participants’ written reflections and free-text comments, submitted after listening to the Cultural Safety training podcasts. These were then analyzed by both Aboriginal and non-Aboriginal researchers using inductive narrative analysis. The remaining two studies provided minimal detail as to their evaluation techniques; however, the results indicate they were based on informal discussions, email feedback, and pretraining and posttraining surveys from participants.
Two studies utilized quantitative methods only by use of the same questionnaire, developed by Mooney et al. (2005). This questionnaire was developed and pilot-tested in the early 2000s through consultations with key stakeholders and Aboriginal health workers in South Western Sydney Area Health Service (now Local Health District), where the Cultural Safety training was being conducted. The questionnaire contained six statements to measure perceptions, and five statements to measure attitudes toward Aboriginal and Torres Strait Islander people, with a 5-point Likert-type scale to indicate agreement. There were also three “yes/no” questions regarding familiarity or friendship with Aboriginal and Torres Strait Islander people, and two multiple choice questions about Aboriginal and Torres Strait Islander health status. This questionnaire was conducted before and after completing the Cultural Safety training with results comparison. Chapman et al. (2014) utilized this questionnaire in their evaluation of Cultural Safety training, however concluded that the questionnaire may not be sensitive enough in assessing the effectiveness of the initiative.
The remaining studies undertook evaluation using mixed methods (Gadsden et al., 2019; Kerrigan et al., 2020; Rissel et al., 2022; Vass, 2015). Qualitative methods used in these studies included semistructured interviews with participants and free-form survey questions, while quantitative methods were primarily Likert-type scale survey questions.
Other than the tool developed by Mooney et al. (2005), no other studies utilized a validated evaluation tool, but rather used self-developed survey tools tailored to the specific initiative (Gadsden et al., 2019; Kerrigan et al., 2020; Rissel et al., 2022; Vass, 2015). Furthermore, only one study evaluated changes in patient experience following the Cultural Safety initiative. Gadsden et al. (2019) undertook this quantitatively by assessing identification of Aboriginal and Torres Strait Islander patients in the health care sites and rates of incomplete ED visits by Aboriginal and Torres Strait Islander patients. It was however identified by the authors that these indicators were likely not sensitive enough as a measure of Cultural Safety.
Change in Health Professionals’ Practice
The resulting changes in health professional’s practice were undoubtedly dictated by the effectiveness of both the implementation and evaluation strategies. Three studies indicated very minimal or no change in health professional’s practice following participation in the Cultural Safety initiative (Gadsden et al., 2019; Mooney et al., 2005; Westwood & Westwood, 2010). The remaining studies found overall improved attitudes, awareness, skills, confidence, and self-assessed knowledge in relation to Aboriginal and Torres Strait Islander health and patient care, to varying degrees. Two of the studies also reported feedback indicating that the Cultural Safety training was perceived to be highly relevant and valued by participants (Kerrigan et al., 2020; Rissel et al., 2022).
Change in Patient Experience
Evaluation of the Cultural Safety initiative in terms of patient experience was not assessed in eight of the nine studies. Gadsden et al. (2019) analyzed changes in the proportion of incomplete ED visits made by Aboriginal and Torres Strait Islander patients at their site and reported very minimal change. The Victorian Department of Health (2010) large-scale Cultural Safety project also identified that positive feedback was received from local Aboriginal and Torres Strait Islander communities regarding some of the changes initiated but no further detail was provided regarding how this feedback was obtained or measured.
Future Directions
All studies provided a number of recommendations for future implementation and evaluation of Cultural Safety initiatives. Regarding implementation, recommendations were focused on strategies to improve engagement of hospital staff with the initiatives, such as providing staff Cultural Safety training on a shorter, regular (rather than one-off) basis during work hours, or alternatively in an online self-directed format (Kerrigan et al., 2020, 2022; Westwood & Westwood, 2010). Suggestions in relation to future evaluations of Cultural Safety initiatives focused on the ongoing need for rigor in evaluation, ideally utilizing both qualitative and quantitative methods with both hospital staff and patients (Rissel et al., 2022). More specifically, it was recommended that further research be conducted into appropriate wording and sensitivity of survey questions to ensure accurate evaluation.
Discussion
This scoping review contributes valuable context to current implementation and evaluation strategies of Cultural Safety initiatives in Australian hospitals. First, it is evident from the findings that evaluation remains primarily focused on staff perspectives rather than patient experience of Cultural Safety. Jongen et al. (2018) also identified this theme in a similar review with an international scope. They concluded that the impact of Cultural Safety initiatives for patients remains unclear, as evaluation is focused on changes in health practitioner knowledge and attitudes. This approach to evaluation neglects the important premise underlying Cultural Safety—that it can only be defined by the recipient of care (Australian Human Rights Commission, 2018). This finding highlights the need to prioritize patient perspectives when evaluating the effectiveness of Cultural Safety initiatives.
However, this must be carefully balanced with the reframing of the concept and practice of Cultural Safety in recent years to focus attention on the need for critical reflection of the health practitioner, while still acknowledging that Cultural Safety can only be defined by the recipient of care (Curtis et al., 2019). Critical consciousness and reflection from the health practitioner are essential to ensure awareness of their own cultural biases and assumptions that may impact on care (Curtis et al., 2019). Therefore, evaluation of Cultural Safety initiatives must encapsulate both changes in both the health practitioner, in regard to incorporating critical self-reflection into their care, and Aboriginal and Torres Strait Islander peoples’ perceptions and experiences of the care received. Although most studies to date did not adopt both of these forms of evaluation, this two-pronged approach is outlined in a recent protocol by Ralph et al. (2023) for the implementation of Cultural Safety initiatives in a Northern Territory hospital setting, in which qualitative and quantitative evaluation from both health professionals and patients will be undertaken in accordance with Cultural Safety principles. This presents a promising model for evaluation for other future Cultural Safety initiatives.
This scoping review also highlights the need for utilization of validated tools in evaluation of Cultural Safety initiatives in hospital settings, as the findings revealed their use was lacking in favor of self-developed tools. This theme was also identified in the international scoping review conducted by MacLean et al. (2023) across health, education, and social work disciplines, which revealed a lack of consistency in the objectives and methods used to evaluate Cultural Safety initiatives. To this end, several new validated evaluation tools have emerged in the wider literature for potential use in this context. For example, Brumpton et al. (2023) have published a recent protocol outlining the planned evaluation of a Cultural Safety initiative among both staff and patients in a general practice setting. Attitudinal change among staff will be assessed with validated survey tools from Ryder et al. (2019) and West et al. (2017), while patient evaluation will occur via semistructured interviews. These tools were also endorsed by Ganeshananthan et al. (2022) in their limited rapid review of self-assessment tools for assessing Cultural Safety. However, for instances where patient interviews are not practicable or possible, Elvidge et al. (2020) have also developed a survey tool to assess patient experience of Cultural Safety in hospitals.
The rigor in validation of these tools and alignment with more developed conceptualizations of Cultural Safety makes them a recommended option for future implementation and evaluation of Cultural Safety initiatives. However, consideration should still be given to self-developed evaluation methods specific to the Cultural Safety intervention, as utilized by the majority of studies, as well as the possibility of adapting the aforementioned validated tools to the specific learning outcomes of the initiative. This approach allows for tailoring of the evaluation tools to the specific setting, population, and initiative.
These evaluation tools should sit under a validated theoretical framework to guide implementation and evaluation, as this was also found to be lacking in the scoping review findings. The implementation process of Cultural Safety initiatives occurred in a mostly ad hoc manner without guidance of an evidence-based framework or theoretical principles. An example of one such framework is the Ngaa-bi-nya Aboriginal and Torres Strait Islander program evaluation framework developed by Williams (2018), which is underpinned by Aboriginal and Torres Strait Islander knowledge and research ethics. It aims to provide a practical guide for evaluating Aboriginal and Torres Strait Islander health and social programs. The framework provides prompts to consider throughout the implementation and evaluation process, and again recommends a mix of quantitative and qualitative methods for evaluation (Williams, 2018). Utilization of frameworks such as Ngaa-bi-nya would help ensure an evidence-based and rigorous implementation and evaluation, guided by Aboriginal cultural knowledge.
Finally, attention needs to be given to the implementation of Cultural Safety initiatives in fast-paced contexts where health care practitioners have considerable preexisting demands on their time and energy—a barrier identified in several studies (Kerrigan et al., 2020; Vass, 2015). Implementing these initiatives in an online self-directed format such as the podcasts evaluated by Kerrigan et al. (2022) can go some way in addressing this barrier. It also allows for Aboriginal and Torres Strait Islander voices and stories to be heard by a wider audience. This makes it a valuable option to be considered in future research.
Strengths and Limitations
This scoping review contributes valuable evidence to this research area, as no other reviews have focused on implementation and evaluation of Cultural Safety initiatives in the Australian hospital context—a setting where Aboriginal and Torres Strait Islander people continue to experience culturally unsafe care (Durey et al., 2012). Nevertheless, it must be acknowledged that the review was limited by the quality of the relatively small number of studies. Utilizing validated quality appraisal checklists, less than half of the 12 studies were evaluated to be of good quality, which should be considered when examining the findings. In addition, only one of the authors (T.P.) is a First Nations person, descendant of the Wiradjuri people. Other authors, including the first author (B.C.) and other authors (J.F. and T.F.) are non-Indigenous, Caucasian Australian citizens. We acknowledge the impact this may have had on the study.
Recommendations and Conclusion
The current body of evidence, as analyzed by this review, indicates that significant improvement is needed in adopting evidence-based and carefully considered approaches to implementing and evaluating Cultural Safety initiatives in hospital settings. Specifically, implementation should be underpinned by a validated theoretical framework and consider and address potential practical barriers in engaging health practitioners. It is recommended that evaluation also utilizes validated evaluation tools and incorporates quantitative and qualitative methods to assess changes in both staff and patient perspectives and experiences. This will encapsulate the important notion that Cultural Safety is determined by recipients of care. These valuable insights will guide the implementation and evaluation of future Cultural Safety initiatives in Australian hospitals, to augment efforts to promote Cultural Safety for Aboriginal and Torres Strait Islander families accessing health care services in Australia.
Footnotes
Acknowledgements
The authors acknowledge the Aboriginal and Torres Strait Islander Peoples of Australia whose knowledge underpins this review and on whose unceded land this paper was written.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.