
Abstract
The enormous scale of suffering, breadth of societal impact, and ongoing uncertainty wrought by the COVID-19 pandemic introduced dynamics seldom examined in the crisis entrepreneurship literature. Previous research indicates that when a crisis causes a failure of public goods, spontaneous citizen ventures often emerge to leverage unique local knowledge to rapidly customize abundant external resources to meet immediate needs. However, as outsiders, emergent citizen groups responding to the dire shortage of personal protective equipment at the onset of COVID-19 lacked local knowledge and legitimacy. In this study, we examine how entrepreneurial citizens mobilized collective resources in attempts to gain acceptance and meet local needs amid the urgency of the pandemic. Through longitudinal case studies of citizen groups connected to makerspaces in four U.S. cities, we study how they adapted to address the resource and legitimacy limitations they encountered. We identify three mechanisms—augmenting, circumventing, and attenuating—that helped transient citizen groups calibrate their resource mobilization based on what they learned over time. We highlight how extreme temporality imposes limits on resourcefulness and legitimation, making it critical for collective entrepreneurs to learn when to work within their limitations rather than try to overcome them.
Keywords
Introduction
“We were the last resort. We were the people that would meet you on your doorstep or in a parking lot and get you something because you weren’t officially being provided what you needed.” (Citizen interview during COVID-19)
Crisis response research shows that in the early stages of a crisis, emergent citizen groups are often more effective than governments and emergency response organizations because they learn to rapidly adapt to changing circumstances as they respond to local needs (Aldrich, 2012a, 2012b; Shepherd & Williams, 2019; Williams & Shepherd, 2016b). Ad hoc citizen groups self-organize to alleviate suffering by mobilizing latent resources and temporarily filling gaps in official response structures (Dinger et al., 2020; Drabek, 1986; Mittermaier et al., 2022), which often fail to address urgent local needs in a timely manner (James et al., 2011; Milburn et al., 1983; Shepherd & Williams, 2014; van der Vegt et al., 2015). As they mobilize heterogeneous resources, citizen groups act in and between organizations and systems through spontaneous collective actions that are not yet institutionalized (Drabek, 1986; Stallings & Quarantelli, 1985; Williams & Shepherd, 2018). To be effective, emergent citizen groups must adapt using nonroutine resources and fluid organizational designs (Kendra & Wachtendorf, 2007; Kreps, 1984; Majchrzak et al., 2007; Rodríguez et al., 2006), with failures to learn weakening resilience and causing the ineffective use of resources (Sutcliffe & Vogus, 2003; Williams et al., 2017).
However, when citizen groups responded to the COVID-19 pandemic in 2020, two issues pertaining to resources and legitimacy challenged our understanding of emergent crisis response groups. First, resource mobilization to alleviate local suffering during a global pandemic required more than redirecting external resources to local pain points of resource scarcity (Korsgaard et al., 2020). Crisis research based on natural disasters tends to assume a large scale and broad scope of resources will be provided from sources outside the disaster area, leaving emergent citizen groups to focus on rapidly customizing received solutions based on their local knowledge of immediate needs (Quarantelli, 1988; Shepherd & Williams, 2014, 2019; Tierney, 2007). But citizen groups responding spontaneously to an unfolding pandemic faced the formidable challenge of learning how to be effective in four areas simultaneously—achieving scale in the solutions they provided, offering a varied scope of solutions, delivering solutions with speed, and customizing useful solutions to meet local needs (Dutton et al., 2006). Furthermore, when the public health crisis disrupted supply chains and emergency stockpiles proved inadequate, citizens engaged in creating new solutions rather than receiving, bundling, and delivering existing solutions (Petri, 2020; Ranney et al., 2020; Thompson, 2020). Citizens coordinated personal and organizational resources, such as 3D printers and sewing machines, and experimented with the local production of items such as ventilators, ultraviolet decontamination machines, and personal protective equipment (PPE) (Clark, 2020; Lunny, 2020; McCue, 2020).
Second, emergent citizen actions to help local institutions—such as hospitals overwhelmed with COVID-19 patients—highlighted the critical role of legitimacy as local actors sought acceptance by the institutional system (Laufer, 2007). Crisis research indicates that citizen groups garner legitimacy by virtue of being locals affected by the crisis and through actions perceived as trustworthy by outside resource donors and local officials (Shepherd & Williams, 2019; Voorhees, 2008; Williams & Shepherd, 2016a). Research suggests that the localness of citizen groups confers advantages on them because of their local know-what, know-how, and know-who (Shepherd & Williams, 2014, 2019). But localness also presents legitimacy disadvantages because, as newcomers largely unknown to dominant actors in the institutional field, citizen groups’ nonroutine forms and activities highlight their legitimacy deficit relative to established organizations (Aldrich & Fiol, 1994; Drabek, 1986). Geographic localness fails to overcome institutional “disdain for accepting assistance from actors outside of the system and an aversion to using activities which are not already part of the system” (Takeda & Helms, 2006, p. 404). Thus, during the pandemic, citizen groups that engaged with the bureaucratic domains of large health systems and governments (Corsini et al., 2020b) faced illegitimacy as outsiders to the system, compounded by their lack of specialized knowledge and limited ability to communicate directly with essential workers at risk.
Therefore, in this study, we explore the mechanisms by which self-organized citizen groups adapted to the resource and legitimacy challenges they encountered in the temporal context of a crisis during COVID-19 (Madden et al., 2012; Mittermaier et al., 2022). We ask: How do emergent citizen groups learn to mobilize resources to gain acceptance and meet local needs amid the urgency of crisis? To answer this question, we conducted longitudinal case studies of citizen groups that organized PPE creation and distribution efforts involving makerspaces in four cities in the United States. We trace temporal patterns of crisis response effectiveness and adaptive behaviors of ordinary citizens acting entrepreneurially (Shepherd, 2020) across three periods of pandemic response—activation, advancement, and abatement. We identify how emergent citizen groups learned to make three adaptations—augmenting, circumventing, and attenuating—in attempts to overcome, work around, or work within their resource and legitimacy limitations. From these results, we build a process model of citizen resource mobilization to meet local needs in response to crisis. Our findings contribute to the entrepreneurship literature by advancing understanding of how the extreme temporality of crisis changes resource mobilization processes involving resourcefulness and legitimation.
Theoretical Background
Scholars have employed the concept of resource mobilization to account for resource search, resourcefulness, and legitimacy in the entrepreneurship and crisis literatures (Clough et al., 2019; Dutton et al., 2006; Williams & Shepherd, 2018). To build a framework for our inquiry, we integrate salient concepts pertaining to resources and legitimacy from each literature. We highlight temporality as a central concern that confounds citizen efforts to mobilize resources.
Resources in Crisis Entrepreneurship
Entrepreneurship research on resourcefulness emphasizes two factors germane to a crisis context: (1) the extent to which diverse types of resources are constrained and (2) the behaviors entrepreneurs enact to generate value from resources. First, entrepreneurial actors often operate in resource scarce environments, including crises (Corbett & Katz, 2013; Williams & Shepherd, 2018). Despite being able to draw on heightened solidarity to help other locals in a crisis, emergent citizen groups are immediately confronted with damaged infrastructure and other resource conditions outside their control and beyond their existing knowledge stocks (Bishop, 2019; Dinger et al., 2020; Shepherd & Williams, 2014; Stevenson & Jarillo, 1990). Thus, entrepreneurial actors must cope with varying levels of constraint across a combination of resource types, including financial, human, physical, and social resources (Clough et al., 2019; Grichnik et al., 2014; Welter et al., 2018).
Second, in the face of a constrained resource environment, entrepreneurs engage in a range of behaviors to mobilize resources, including search to obtain new resources and (re)combining resources to create useful new solutions (Michaelis et al., 2020; Sonenshein, 2014). The entrepreneurship literature has largely focused on behaviors that help entrepreneurs acquire more resources (Hertel et al., 2021), creatively work around constraints as bricoleurs (Baker & Nelson, 2005; Davidsson et al., 2017; Garud & Karnøe, 2003; Korsgaard et al., 2021), and adapt goals according to resources currently available (Fisher, 2012; Perry et al., 2012; Sarasvathy, 2001). Accordingly, Williams et al. (2021, p. 2) define resourcefulness as “a boundary-breaking behavior of creatively bringing resources to bear and deploying them to generate and capture new or unexpected sources of value in the process of entrepreneurship.” A behavioral perspective thus helps us examine the mechanisms by which entrepreneurial citizens attempt to exercise personal and collective agency to overcome resource and institutional limitations (Desa, 2012; Michaelis et al., 2022; Welter et al., 2018).
However, the extreme temporality under which emergent citizen groups operate can impose limits on their resourcefulness (Williams et al., 2021). Emergent groups form spontaneously without time to build up resources in advance before deploying them (Shepherd & Williams, 2019). As primarily volunteer organizations, the energy required to act resourcefully with scale, scope, and speed cannot be sustained indefinitely (Barker & Gump, 1964; Oliver, 1984). As temporary ventures (Bakker et al., 2016), truncated efforts to rapidly develop new solutions may compress and damage the timelines and transitions of creative processes (Sonenshein, 2014). Indeed, generating greater scale, scope, or speed of solutions without customizing them to local needs can prove wasteful and counterproductive (Dutton et al., 2006; Williams & Shepherd, 2018). Moreover, some limits on resourcefulness may be appropriate because deviant behaviors temporarily tolerated in the interest of alleviating suffering may harm a community if not discontinued (Steffens et al., 2022; Williams & Shepherd, 2016b).
Legitimacy in Crisis Entrepreneurship
Suchman (1995, p. 574) defined legitimacy as a “generalized perception or assumption that the actions of an entity are desirable, proper or appropriate within some socially constructed system of norms, values, beliefs and definitions.” Entrepreneurship research indicates that legitimacy should precede resource mobilization to ameliorate an emergent organization’s liability of newness (Delmar & Shane, 2004; Fisher et al., 2016; Stinchcombe, 1965). In a crisis, illegitimacy can thwart citizen groups’ entrepreneurial efforts to create collective goods (Drabek, 1986; Mittermaier et al., 2022). The legitimacy deficit citizen groups experience relative to more visible, recognized, and powerful institutions has also been referred to as an illegitimacy discount (Zhao et al., 2013; Zuckerman, 1999). Groups with low legitimacy face considerable pressure to overcome this deficit and may engage in activities that detract from their original objectives, thereby inhibiting their effectiveness (Drabek, 1986).
Although prior studies have noted the importance of legitimacy for emergent groups responding to local crises (Shepherd & Williams, 2019), COVID-19 wreaked havoc on the “system of legitimacy itself” and the impact of this systemic confusion on citizen groups warrants closer analysis (Laufer, 2007, p. 65). For our framework, we draw on the work of Aldrich et al. (2020), which distinguished between cognitive legitimacy—acceptance of a new venture as taken for granted—and learning—the need for entrepreneurs to overcome a lack of organizational knowledge for their intended audience and to develop effective routines under conditions of ignorance and uncertainty. Aldrich et al. (2020) also defined two types of sociopolitical legitimacy: regulatory legitimacy—acceptance by political and certifying authorities—and moral legitimacy—when the value of an activity is accepted within cultural norms, especially if it creates a public good, uses accepted procedures, and is structured according to familiar forms (Suchman, 1995).
Legitimation is a complex, multifaceted process that unfolds over time as low legitimacy actors attempt to overcome local institutions’ skepticism and achieve greater acceptance (Johnson et al., 2006; Suddaby et al., 2017; Vaara & Tienar, 2008). For emergent citizen groups, this process requires them to seek acceptance for themselves as actors, their organizations, their artifacts (i.e., PPE), and their actions (i.e., design, production, delivery) from a range of stakeholders such as hospital administrators, individual clinicians, government officials, potential donors, and the public. However, the urgency of a crisis curtails this process and places emergent groups in a difficult position of needing to confront multiple legitimacy complications simultaneously (Delmar & Shane, 2004; Fisher, 2020). Such extreme time pressure weakens the effectiveness of legitimation mechanisms such as (1) framing narratives to make unknown activities believable (Lounsbury & Glynn, 2019), (2) forming new social ties where existing relationships and inter-organizational contacts are lacking (Drabek, 1986), (3) collaborating with other groups to speak with one voice and develop joint problem-solving arrangements (Uzzi, 1997), and (4) pursuing regulatory approval to gain third-party certification from cautious agencies (Baron & Markman, 2003; Kramer & Cook, 2004). Thus, emergent citizen groups present a valuable research context for expanding our understanding of legitimation mechanisms under conditions where temporary objectives have supplanted the traditional goal of establishing and maintaining long-term organizational legitimacy (Fisher et al., 2017).
Method
To understand how emergent citizen groups learn to mobilize resources to gain acceptance and meet local needs amid the urgency of crises, we followed a grounded theory approach and built multiple case studies of four metropolitan areas in the United States during the COVID-19 pandemic in 2020 (Eisenhardt, 1989; Glaser & Strauss, 1967). This approach provides a systematic way to collect open-ended data, guided by the literature, without imposing an overly restrictive a priori explanatory framework (Strauss & Corbin, 1998). Qualitative data are well-suited for capturing mechanisms involving complex processes with temporal dynamics embedded in social interactions (Graebner et al., 2012; Langley, 1999).
Research Setting
The heterogeneous group of citizens that responded to the need for PPE during the pandemic consisted of do-it-yourself hobbyists, engineers, artisans, hackers, students, and small business owners with varying degrees of expertise in design, textiles, prototyping, and digital and traditional fabrication. Over the last two decades, this diverse group of actors has collaborated to varying extents on projects in shared digital and physical spaces, including thousands of innovation workshops and local fabrication facilities referred to as makerspaces (Browder et al., 2019; Halbinger, 2018; Mortara & Parisot, 2016). Makerspaces are known as places attracting people who wish to break away from encumbering institutions, but who are also adept at collaborating across differing degrees of disciplinary expertise and organizational affiliations (Furnari, 2014). As the global pandemic spread, these citizen makers rapidly and organically produced entrepreneurial responses to help with the dire shortage of solutions such as PPE (Abbassi et al., 2021; Corsini et al., 2020a, 2020b; Vesci et al., 2021).
The growth of Open Source Medical Supplies (OSMS) illustrates the spontaneous diffusion of the citizen response. OSMS began as a Facebook group the day prior to COVID-19 being declared a pandemic and grew to include over 73,000 Facebook members supporting a roster of 547 local citizen groups in more than 50 networks connecting groups to resources and partners such as suppliers, governments, and hospitals (OSMS, 2020). In September 2020, OSMS and Nation of Makers organized a survey to document their impact. They reported receiving 1,878 survey responses, representing 42,000 volunteers and staff in 86 countries, but with responses heavily weighted toward the United States (Cavalcanti et al., 2021). In the United States, people reported producing 34 million units of medical supplies consisting of PPE such as face shields, disposable gowns, cloth masks, surgical caps, and powered air purifying respirators, as well as novel solutions developed during the pandemic, such as ear savers, non-invasive ventilation helmets, ventilator splitters, and door openers. Overall, emergent crisis response groups such as those documented by OSMS represented entrepreneurial citizens’ efforts to meet significant local needs until supply chains and official crisis management channels recovered.
Sample and Research Design
We drew from the population of OSMS local citizen groups to evaluate eight cities where a crisis response emerged. We selected a final sample of four cities located in the United States (to control for the regulatory and political environment) where citizen groups were connected to established makerspaces, groups engaged established institutions such as hospitals, resources were channeled toward meeting local PPE needs, varied approaches to the production and provision of PPE were attempted, and data were available throughout the study period. To maintain anonymity, we renamed the four cities Midburg, Edgeville, Triport, and Stilton.
In contrast to cross-sectional crisis studies, we adopted a racing design that allowed us to compare the historical evolution of the four cases during the same era (Eisenhardt et al., 2016). We began when the World Health Organization (WHO) declared COVID-19 a pandemic on March 11, 2020, and traced each case throughout 2020. As each citizen group responded, our research design allowed us to identify and analyze their patterns of adaptive behaviors.
Data
We collected data from multiple sources to ensure coverage throughout the study period and to enable triangulation across different types of data (Gibbert et al., 2008). Data sources include field participation and observation, OSMS documents and survey reports, secondary documentation, and interviews. Following the lead of other crisis research scholars, we engaged in preliminary field work to understand the phenomenon of interest (Dinger et al., 2020; Williams & Shepherd, 2021). In March 2020, we began observing and discussing how citizens responded to the pandemic. Over the subsequent months, members of our team participated in virtual conferences, makerspace workgroups, and OSMS projects that informed our overall understanding (Cavalcanti et al., 2021). Figure 1 shows a timeline of data collection and analysis.
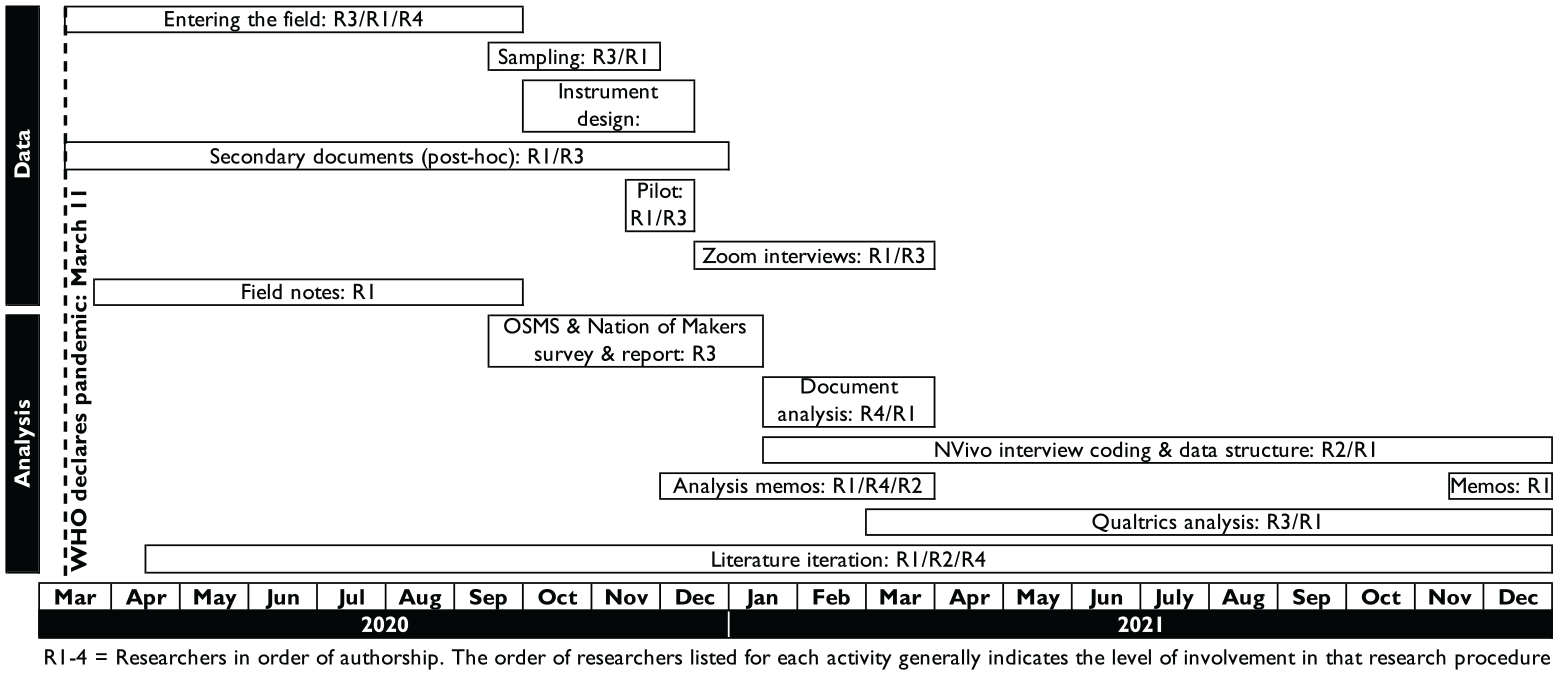
Timeline of data collection and analysis procedures.
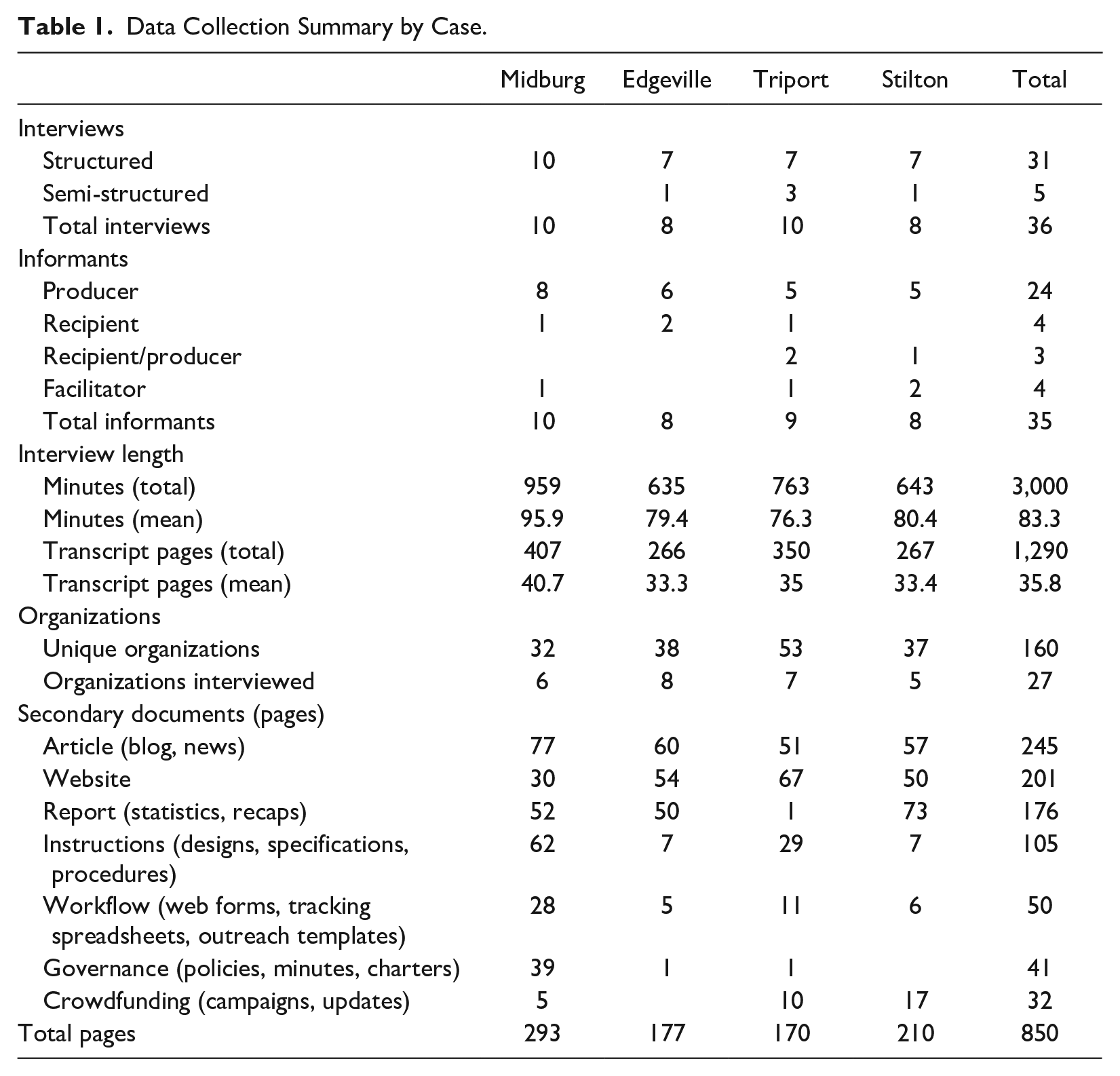
We also collected archival data to inform our understanding of how self-organizing activities evolved throughout 2020. Types of documents collected include news and blog articles containing interviews and timelines, websites, summary reports containing stories and statistics, instructions about PPE designs and volunteer procedures, workflow process documents and tools such as web forms and spreadsheets, governance documents such as policies and meeting minutes, and crowdfunding campaigns with chronological updates. These documents—combined with the OSMS roster of citizen groups, web and media searches, and input and vetting from initial contacts who were key organizers in each city—allowed us to compile an initial list of 160 unique organizations that emerged to respond to the need for PPE. Table 1 summarizes the data collection according to source and case study.
Data Collection Summary by Case.
We developed an extensive protocol to conduct structured interviews remotely using Zoom to screen-share our instrument in Qualtrics. We designed our questions to elicit responses about the timing of key events, social ties across organizations, PPE production and delivery activities, and key decisions regarding citizen organizing. We piloted the interview instrument with four subject matter experts in North American cities outside our sample to refine the protocol. Pilot interviews lasted 109 minutes on average.
We recruited informants across different organizations. We began with four primary contacts who functioned as key organizers in each city, then identified potential new informants using a combination of snowballing and purposive sampling by emailing other organizational contacts. Informants represented PPE producers, PPE recipients such as clinicians, as well as people who acted in multiple roles or brokered contacts between people in dissimilar roles. Overall, we conducted 36 interviews with 35 informants representing 27 unique makerspaces, local businesses, and healthcare organizations across the four cases. Interviews occurred between December 10, 2020 and March 13, 2021, and lasted an average of 83 minutes. We conducted 31 structured interviews using the Qualtrics instrument and five shorter semi-structured interviews. We recorded and transcribed interviews using Otter.ai for a total of 1,290 pages of transcriptions. See the Supplemental Material for additional details about our interviews.
Analysis
We assigned different roles to researchers on our team to analyze case evidence in multiple iterations from different perspectives, helping us maintain varying degrees of closeness to informants and increasing the objectivity of our analysis (Eisenhardt, 1989). To record our observations and link them with relevant theories, we made extensive use of field notes and analysis memos (Lempert, 2007). Beginning in March 2020, we wrote 17 single-spaced pages of field notes to record our early observations of the phenomenon in progress (Van Maanen, 2011). Later, we wrote 31 single-spaced pages of memos while analyzing secondary documents to gain a longitudinal perspective throughout the study period and to mitigate potential informant hindsight bias from interviews. To contribute to our theory building, we wrote 88 single-spaced pages of additional memos after individual interviews or coding sessions to reflect on topics such as interview insights, potential themes and variables emerging from coding, within and cross-case temporal patterns, and relevant literature to consult (Strauss & Corbin, 1998).
Structured analysis of our interview data proceeded in two ways. First, we analyzed the quantitative and textual data provided through Qualtrics. We generated a database of responses encompassing Likert scales (e.g., How well did the types of PPE produced match what recipients needed? Where 1 = very poor match and 5 = very good match), dates (e.g., first involvement in PPE production), raw numbers (e.g., amount of PPE produced), and percentages (e.g., percentage of PPE provided to different types of recipients). While extensive statistical analysis of this data was not appropriate due to the sample size, this approach allowed us to capture comparable data in clear categories while also enabling us to create case history timelines in combination with dates found in secondary documents. Using timeline information about monthly volunteer activity levels and PPE production volume, we used temporal bracketing to identify three periods that each case moved through (Langley, 1999). We labeled these periods: activation (March 2020), advancement (April to mid-June 2020), and abatement (mid-June to December 2020).
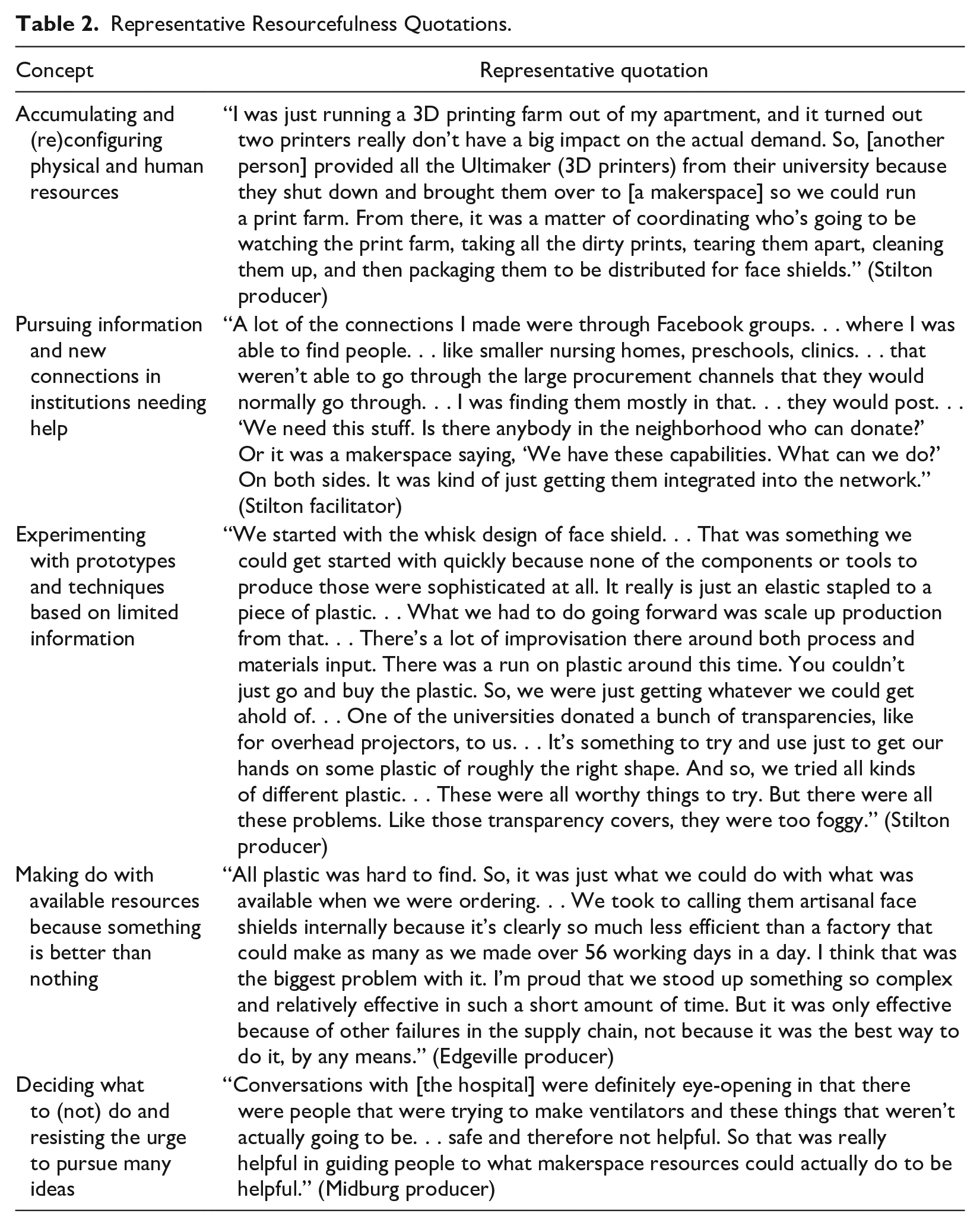
Second, we imported and categorized interview transcripts in NVivo for coding and constant comparative analysis (Eisenhardt, 1989). We engaged in open coding (Strauss & Corbin, 1998), reading the data line by line to generate 147 codes. While we did not presuppose the directionality of relationships in the data, a guiding coding framework emerged to focus our attention on three general concepts: (1) the barriers and challenges that arose, (2) the adaptations made in response, and (3) the effectiveness of the crisis response. We discussed interim findings within the author team, helping us identify 76 additional codes primarily related to two main themes that emerged from the data: resourcefulness and legitimation. We then categorized codes into second-order concepts and theoretical themes, as depicted in Figure 2. Tables 2 and 3 provide representative quotations about resourcefulness and legitimation concepts, respectively. From this process, we derived aggregate theoretical dimensions about the adaptation mechanisms that citizen groups learned to apply to their resourcefulness and legitimation behaviors during crisis response: augmenting, circumventing, and attenuating. Finally, we combined insights from the two analysis steps to examine crisis response effectiveness, resource constraints, legitimacy deficits, and adaptation behaviors according to the three periods in the timeline.
Representative Resourcefulness Quotations.
Representative Legitimation Quotations.
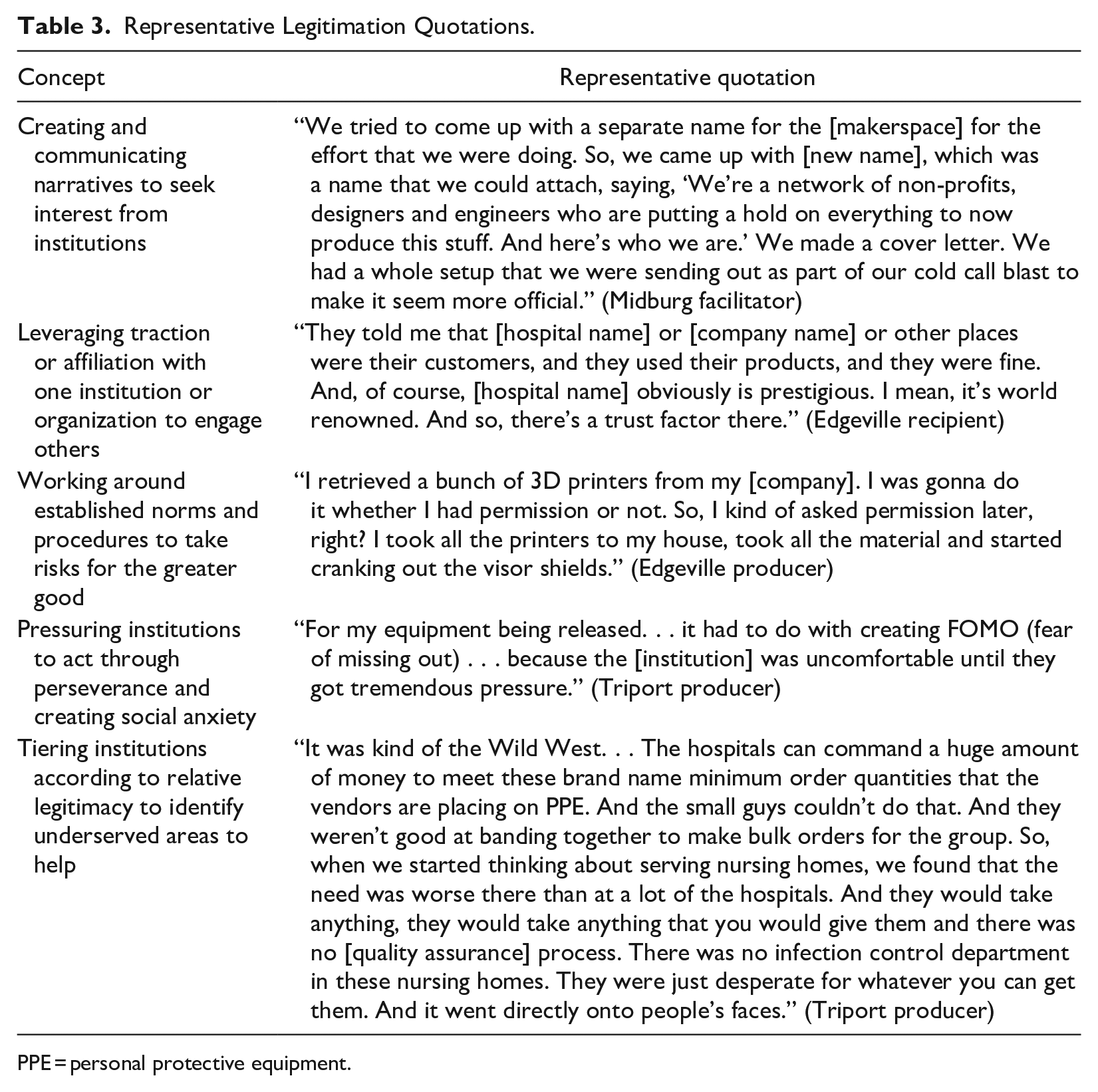
PPE = personal protective equipment.
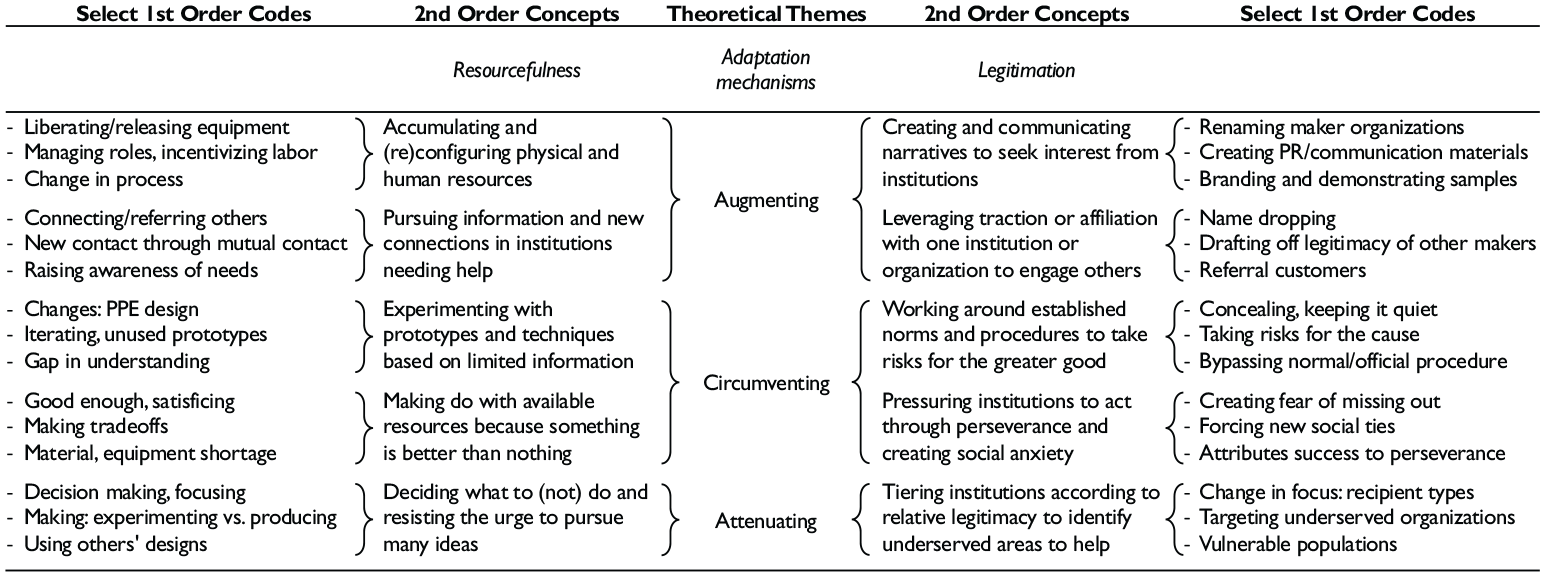
Theoretical themes and concepts from interview analysis.
We engaged in a series of five procedures to assess the reliability and validity of our analysis. First, we triangulated our findings by crosschecking across data types (Gibbert et al., 2008). For example, we compared key dates and events discussed in interviews with the timelines we created from secondary documents. Second, two authors (one who interacted directly with informants and one who had not met informants) engaged in multiple rounds of coding. By trading off coding rounds, we were able to iterate toward agreement on emergent themes and leverage diverse vantage points to construct an increasingly robust account of data patterns (Eisenhardt, 1989). Our author team also regularly discussed emerging themes, their definitions, distinctions between similar concepts, and the appropriate ordering of constructs in the model. Third, we engaged in member-checking with five key informants representing all cases to receive input on the extent to which our interpretations of the data reflected their lived experiences and if they felt anything important was missing from the narrative or model (Creswell & Miller, 2000). Fourth, we spoke with five subject matter experts at OSMS and Nation of Makers to ensure we accurately interpreted the details of citizen PPE production activities. Finally, throughout the analysis, we continually revisited the literature to identify prior constructs and potential explanations of relationships related to our emergent findings.
Findings
Our findings tell a story that highlights the conditions under which some citizen adaptations were effective, as well as revealing the limitations of emergent citizen groups. The citizen maker response to COVID-19 proved to be a context where issues of resource constraints and legitimacy deficits were acute. Citizen groups struggled with the early barriers they encountered, but they learned to make successful adjustments over time. Thus, learning played a critical role in the resourcefulness and legitimation behaviors of ordinary people acting entrepreneurially in a public health crisis. Citizens learned about local needs from the media, Internet, clinicians, institutional administrators (e.g., procurement contacts), and city officials, as well as other citizens. The needs they learned about were not just local in a geographic sense. Citizens also learned about matters requiring specific domain expertise (e.g., clinical practices, institutional policies and processes, regulations, medical supply design, and manufacturing) at a time when knowledge about the disease itself was lacking.
The three periods that emerged from our temporal research design show the evolution of the citizen response from activation to advancement to abatement. Many citizens came to see their efforts as temporary “stop-gap” measures, in which they worked intensely until more traditional supply chains could take over. A PPE producer in Midburg emphasized how extreme temporality was top of mind, “You literally had a six-to-eight-week window where you can make a real impact.” A clinician in Stilton concurred, “By June or July, that’s when the surge died off and supply chains were a little bit better.” As shown in Figure 3, the weekly volunteer hours informants in each case devoted to PPE production and distribution activities confirm their rapid initial activation in the month of March 2020. Average volunteer activity peaked at 40 hours per week in April and continued at almost 30 hours per week by June. Lower volunteer participation levels followed from July to December. Figure 4 illustrates a similar pattern of activity according to the total quantities of PPE produced by three citizen groups that included monthly tracking data in their secondary documents. The figure shows low initial production in March, followed by peak production for each case in April or May. The citizen group examples in Midburg and Edgeville represent singular organizations that halted production by June, although other citizen groups in those cases remained somewhat active. The citizen group in Stilton represents four makerspace organizations that collaborated, and thus provides a comprehensive view of declining production levels for this case.
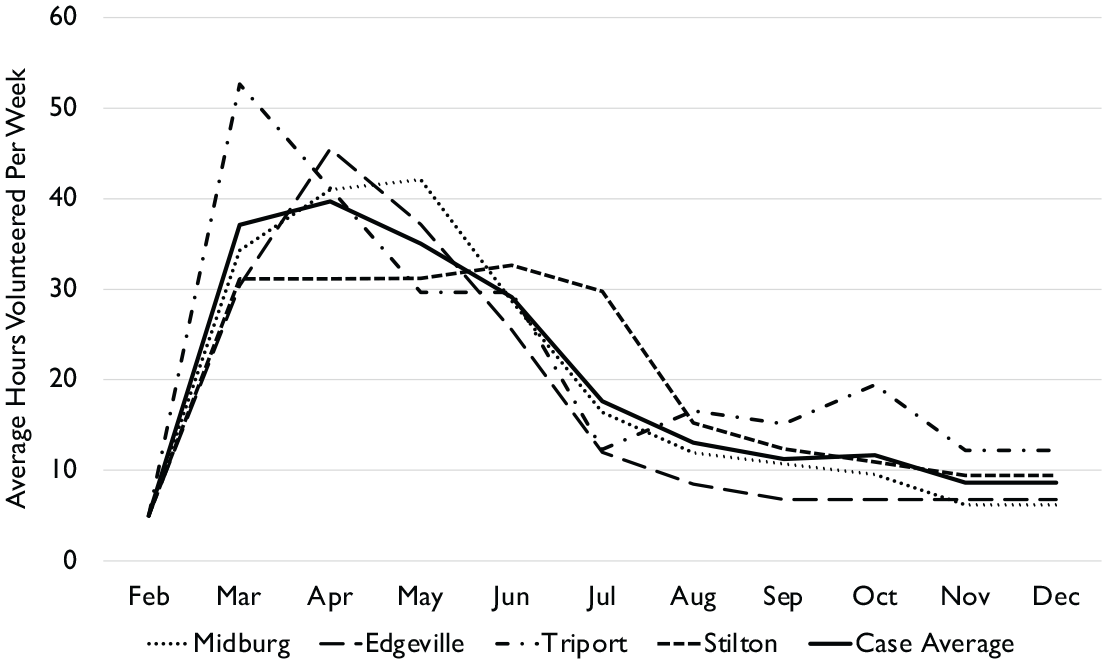
Average weekly volunteer hours by case in 2020.*
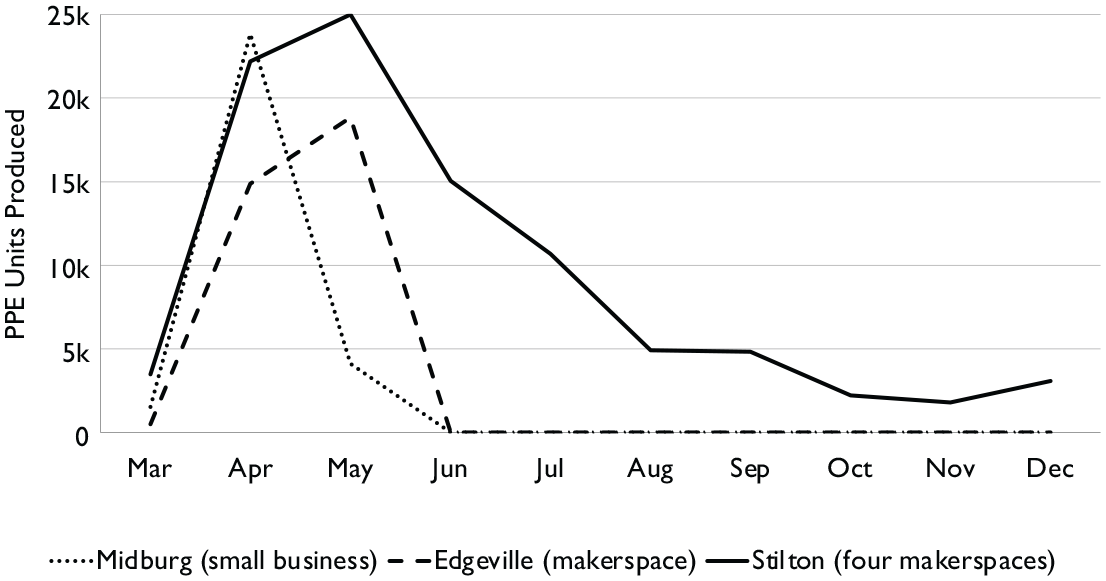
Examples of monthly PPE production volume in three citizen groups in 2020.
Over this timeframe, the citizen groups in our cases produced more than 410,000 units of the most urgently needed PPE varieties in rapid response to urgent community needs. Our data on scale and scope of PPE indicates cumulative production in Midburg was greatest across the widest variety of PPE types, whereas Edgeville produced the least PPE of all cases, with less variety. Table 4 summarizes the quantities and types of PPE as well as the top categories of PPE recipients, listed by case. Our findings also show the speed with which citizen groups in each city launched production in mid-March of cloth masks, face shields, and gowns. These efforts began weeks ahead of federal announcements from the U.S. Centers for Disease Control and Prevention recommending the use of cloth masks (April 3) and Emergency Use Authorizations (EUAs) for non-certified face shields (April 9) or gowns (May 22). Figure 5 summarizes the production timelines in each case according to PPE types.
Summary of PPE Distribution and Recipients by Case.
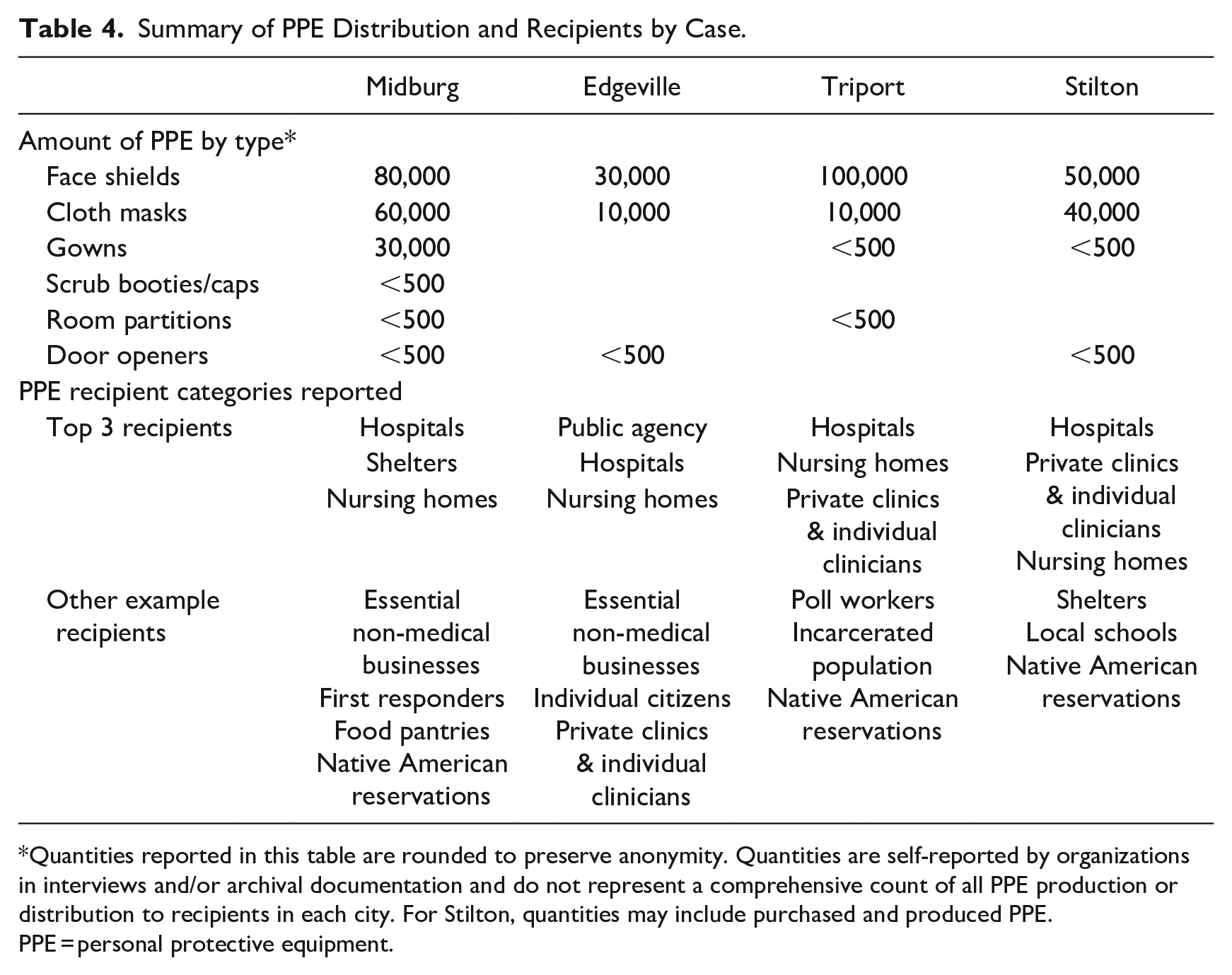
Quantities reported in this table are rounded to preserve anonymity. Quantities are self-reported by organizations in interviews and/or archival documentation and do not represent a comprehensive count of all PPE production or distribution to recipients in each city. For Stilton, quantities may include purchased and produced PPE.
PPE = personal protective equipment.
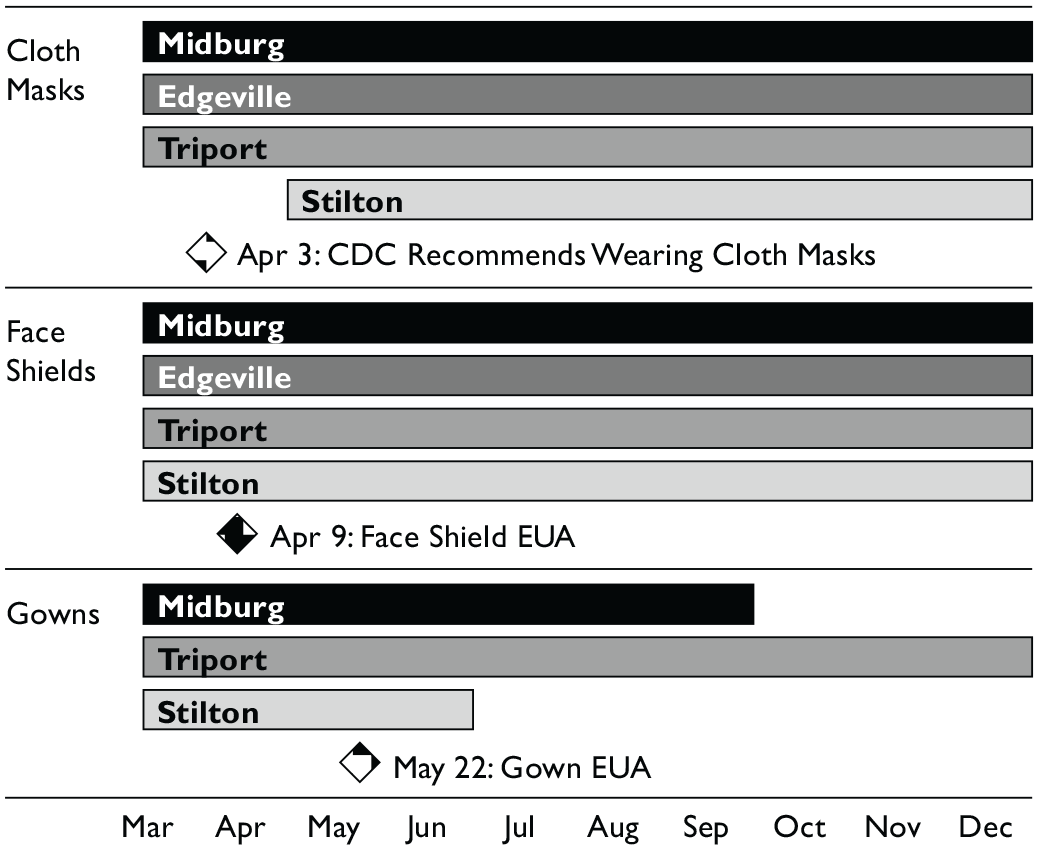
Timeline of case production and federal announcements according to PPE type in 2020.
Whereas these results provide helpful measures of the general scale, scope, and speed dimensions of citizen group response effectiveness, our process analysis revealed that attempts to customize production to meet local needs prompted three specific types of adaptations. Citizens sought to augment their resources and legitimacy while also attempting to circumvent the barriers they encountered. Over time, citizens also learned to adapt their behaviors to meet local needs by attenuating their resourcefulness, legitimation, and PPE production activities. Next, we report our analysis of crisis response effectiveness, resource constraints, legitimacy deficits, and adaptation behaviors according to the three time periods, as summarized in Table 5.
Periods of Citizen PPE Production in Response to COVID-19.
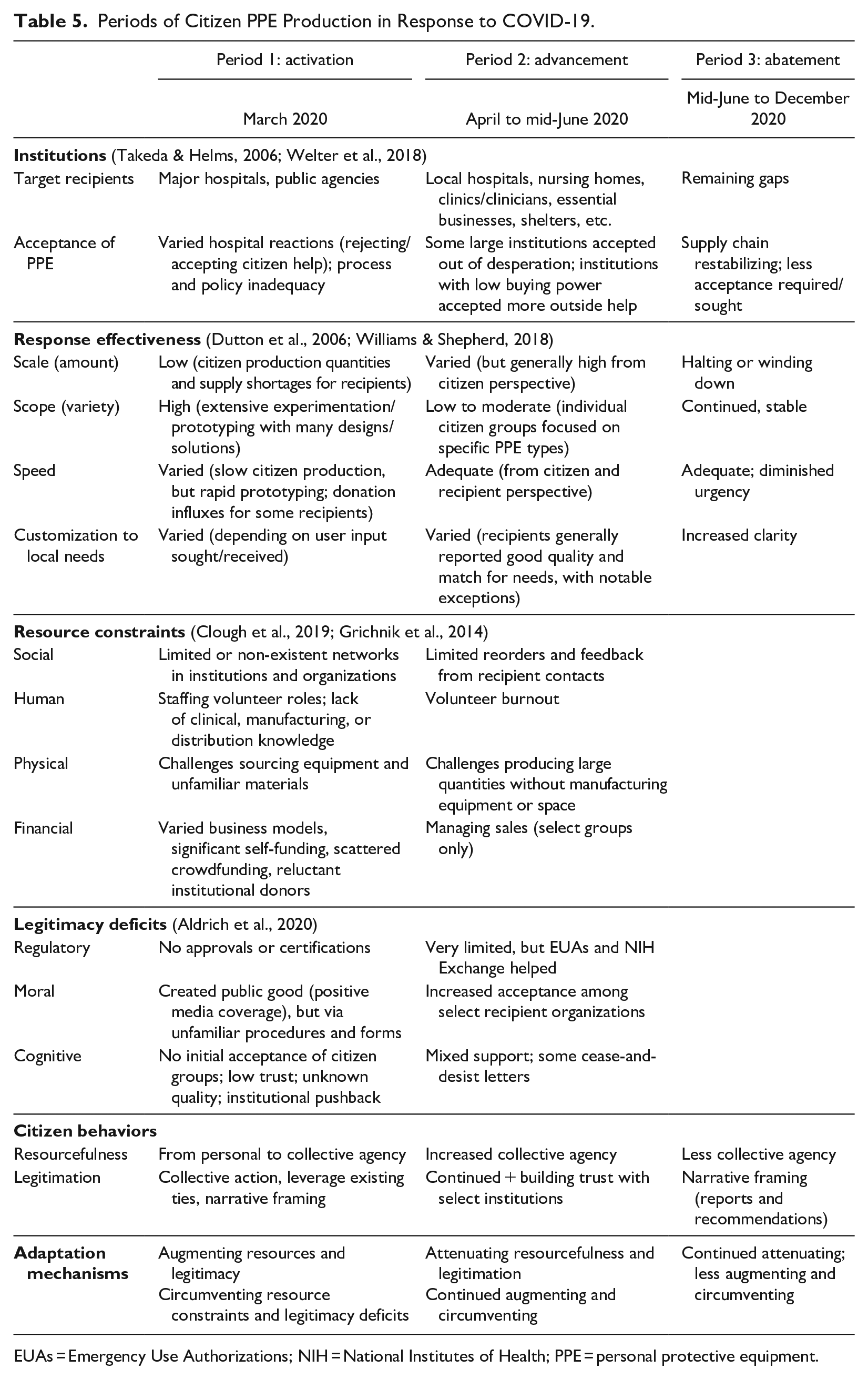
EUAs = Emergency Use Authorizations; NIH = National Institutes of Health; PPE = personal protective equipment.
Period 1: Activation
When the WHO declared COVID-19 a global pandemic, citizen groups in our four cases spontaneously began to self-organize to meet local needs for PPE (see Figure 3). We report how effective their initial response was in the activation period in March 2020 and how they used two adaptive behaviors—augmenting and circumventing—to address the resource constraints and legitimacy deficits they immediately encountered.
As the pandemic spread in each city, exponentially growing case counts revealed a dire need for PPE. A clinician in Stilton described a moment of realization regarding a public goods failure in mid-March, “[The N-95 masks] weren’t coming in from the top, from the federal government. . . That’s when I realized that it’s gonna take a grassroots effort to be able to at least brace for the incoming surge.” The ensuing lag between the initial recognition of local needs for PPE and the federal EUAs (see Figure 5) exemplified the dilemma hospitals and other institutions faced—whether to wait for authorized supplies or address the immediate shortage with non-authorized supplies of potentially unknown quality and origin. Institutional acceptance of outside help varied, as many hospitals officially prohibited non-certified PPE, while others did not take an official stance. Many individual frontline PPE users and decision-makers ignored their own institutions’ pre-existing policies, contending that “anything is better than nothing.”
In mid-March, however, a major hospital in Midburg acknowledged its desperate need for supplies, specifically calling on people and organizations with access to 3D printers. Large Zoom meetings quickly attracted individuals as well as people representing prestigious universities and leaders of small businesses, makerspaces, and community organizations across the city. In these instances, a mix of curious and well-intentioned citizens sought to identify potential connections, learn what was needed, learn what others intended to do, and inform their own decisions about how to get involved. Citizen groups began to emerge in all four cities.
Response Effectiveness
Grasping the urgent need, most citizen groups prioritized expediency and targeted initial PPE supplies for hospitals. Citizen makers rapidly prototyped a wide variety of PPE, inventing their own designs or modifying designs they learned about on the Internet. Because citizens had to design novel solutions rather than bundle existing resources, production was slow in the activation period. A volunteer in Midburg explained how citizens soon encountered a scaling problem they were ill-equipped to address, “You have these institutional levels of [large hospitals] who can use on the order of 10,000 gowns in a single day. And for us, we were producing things on the order of dozens a day, 100 a day.”
By targeting large institutions, citizens immediately faced knowledge gaps about what to produce and how to gain access. A PPE production organizer in Triport described how an initial phone call with a major hospital helped them learn about a local need:
They said, ‘The most important thing is that we need it fast.’ We were talking about 3D printing a lot of stuff. . . ‘Maybe making the mask is a harder thing, but maybe face shields.’ And within an hour or two, a couple of our team members who are engineers came up with a good design. . . [The hospital contact] said, ‘Oh, that’s interesting, but could you put something so it’s not hitting their face?’ And then they sent over a clinician who came over that night and looked at the prototype. They made some modifications, and within a day or so we started printing them.
When well-connected citizens received user input like this, they quickly customized initial solutions to begin meeting local needs. However, other citizens lacked information, social ties, and the resources necessary to customize solutions.
Resource Constraints
Exercising personal agency, many individuals used personal funds, equipment, and materials to voluntarily begin making PPE, even if they did not know where or how it might be used. An individual in Triport who purchased a 3D printer to make PPE from home struggled due to a lack of social ties, “[Hospitals] were not returning calls. Here I am producing things with nobody to get them to. . . I couldn’t get through to find somebody to take these things. I was stuck with red tape.” By joining emergent groups, individual citizens like this were better able to coordinate PPE assembly and distribution through collective agency.
Nevertheless, most citizen groups lacked collective knowledge about servicing clinical settings that needed PPE, and they lacked expertise in establishing manufacturing and supply chain operations from scratch. One group leader in Edgeville described getting involved in creating demand generation and fulfillment functions out of necessity, not because they had experience with such functions, “Folks were struggling and figuring out what the heck was in a supply chain and buying blindly.” In addition to knowledge gaps, human resource constraints were evident in extensive volunteer staffing challenges across all four cases.
Physical resource constraints in the activation period included equipment challenges as citizens attempted to produce large quantities with tools intended for prototyping or small-scale fabrication. Many citizens produced PPE from home due to business shutdowns and stay-at-home restrictions. Those who were able to access workshops or makerspaces still struggled with inadequate facilities for medical grade purposes, such as sterilization of products. Materials shortages also posed a significant obstacle as citizens competed with producers worldwide for large quantities of materials such as elastic or plastic just as major global supply chain disruptions became apparent. Shortages of the most desirable materials required makers to improvise, designing PPE that used more readily available materials, often locally sourced.
Financial resource constraints posed major challenges, but the citizen groups in our study addressed these very early. In Stilton, for example, one group that formed around four makerspaces relied on the one organization already set up as an independent non-profit to lead a crowdfunding campaign. Crowdfunding donations was a common way to pool resources and provide financial runway as the crisis response continued. While most citizen groups in our data chose to donate their PPE, the groups that decided to sell PPE as part of a self-sustaining initiative required additional efforts to educate volunteers about the rationale for the decision.
Legitimacy Deficits
Citizen groups quickly encountered legitimacy barriers that impeded their ability to help frontline workers in need of PPE. A clinician in Triport described the impact of the lack of regulatory legitimacy for citizen-made PPE:
We had all these homemade masks and [the hospital] just said, ‘No. We can’t [accept them]. These are not certified.’ Instead, then we had to just wear the same certified mask for two weeks and it was disgusting.
A clinician in Stilton who acted as recipient and producer of PPE perceived a lack of acceptance by political and regulatory authorities:
None of these [PPE designs] were ever being evaluated in terms of a design that would be supported by these agencies. They were mum about the situation. At a state and federal level. . . they appreciate these efforts, but they weren’t supporting them outright.
Across all four cases, informants reported they experienced the greatest hindrances from public agencies whose nominal missions were the provision of public goods. Thus, citizens faced sociopolitical legitimacy deficits as they attempted to work with complex bureaucratic institutions.
Citizen groups persisted despite obstacles because they perceived the moral legitimacy of their cause to be high. Informants uniformly cited “doing the right thing” among their driving motivations, a perception that was encouraged by their social ties and media reports in each city. In Triport, one religiously affiliated university’s administration quickly approved citizen use of institutional equipment. However, this institutional response was atypical because citizen groups represented unfamiliar organizational forms using unfamiliar procedures. Most citizen groups in Triport faced “pushback” from the institutions to which they were connected. Indeed, altruistic help to create a public good was insufficient justification for cautious institutional leaders who feared that even well-intentioned citizen actions would cause more harm than the pandemic itself. A leader in Triport described one effort to overcome liability concerns:
[Another makerspace leader] and I talked to the lawyers at [one institution]. Even after we had the state’s department of public health tell us they would provide blanket indemnity to anybody who made things, their lawyer still didn’t want to get involved.
Unlike the large traditional suppliers that institutions had established contracts with, citizen groups had low cognitive legitimacy. A volunteer who brokered between hospitals and a makerspace in Midburg described the lack of trust this engendered:
There was a perception that we were this ragtag bunch. . . vigilantes trying to solve this problem. We weren’t really established. . . Supply chain managers are like, ‘Are you just a bunch of people. . . knitting in a garage together making face masks? . . .We don’t know who the f— you are. . . .I don’t know if we can trust you.’
To build legitimacy, citizen groups focused their collective action on existing local ties. A leader in Triport emphasized “localism” so that citizens would concentrate on taking care of needs in their immediate neighborhoods (Shepherd & Williams, 2014). We found Edgeville’s citizen groups experienced greater initial cognitive legitimacy than the other cases because of existing social ties. Prior to the pandemic, Edgeville’s key makerspace established relationships with the city, the small business development association, the state manufacturing association, local universities, and charities. As a result, it was able to diffuse cognitive legitimacy to the many citizen volunteers sending PPE components from home to the makerspace for assembly.
Augmenting Resources and Legitimacy
During the activation period, citizen groups adapted to their conditions by engaging in four behaviors intended to increase their resources and legitimacy. First, they accumulated and (re)configured physical and human resources to overcome the logistical challenges of conducting distributed operations out of personal homes and vehicles. To gain access to equipment, many people took items such as 3D printers from universities and corporations—with or without permission—when they encountered prohibitive institutional policies and/or administrator anxiety over liability concerns. People often referred to the “liberating” of equipment from institutions so that it could be put into service for the public good, typically asserted with a hint of pride at defeating institutional constraints.
Second, citizens augmented knowledge and social resources by pursuing information and new connections in institutions needing help. A makerspace leader in a Triport group described beginning with existing social ties to learn and develop new ties:
I had relationships within the health systems that may not have been the right contact for what they were looking for, but they knew [our organization] and what we were capable of doing. They were making calls to places like us, or we were making calls into them.
An informant from Midburg served as the sole clinical consultant for a large makerspace as well as for other groups in the city. Even though this individual was not in an official position of influence in a hospital, the existence of hospital ties gave them the social capital required for gathering and sharing knowledge within citizen groups. Thus, family members, friends, or neighbors who worked in any capacity at hospitals were considered to be potential connections to utilize for learning how to gain access to unfamiliar institutions (Clement et al., 2018).
Third, citizen groups sought to augment their legitimacy by creating and communicating narratives to attract institutions. Citizens sought legitimacy for their artifacts by demonstrating prototypes to hospital executives, clinicians, and other potential recipients. While this form of legitimation seemed intuitive and familiar to citizen makers, the challenge was finding the right types of users to seek feedback from. Citizen groups also engaged in narrative framing by branding their efforts in websites, outreach letters, and press packets. In all four cases, even established organizations renamed their groups to clearly signal PPE activities to potential institutions, rather than to approach recipients under idiosyncratic makerspace or small business names. In Midburg, members of one makerspace disagreed strongly about whether to rename themselves for this reason, or whether it was important to “get credit” and recognition for their efforts even if their name seemed less likely to be perceived as legitimate.
Fourth, citizen groups augmented their legitimacy by leveraging traction or affiliation with one institution or organization to engage others. A small business owner in Midburg recited a sales pitch to show how “name-dropping” the names of area hospitals sometimes helped him leverage the reputation of those institutions:
We’ve already got six different major hospitals in your area that have approved these and say they are the best things they’ve ever seen. I really think you need to see one of these at a minimum. . . I will get in the car right now. I’m already making another drop to [another hospital] right down the street from you. . . How many do you need?
Similarly, a sewing group organizer in Midburg explained how ties with the PPE production efforts within a reputable institution opened doors for the citizen sewing community:
We had the COVID response team from [a university hospital], which was really helpful in legitimizing. So, we can say, ‘[This hospital] is working with us.’ Then [another hospital] asked. . . which felt like I could launch the whole thing.
Examples such as these illustrate how citizens perceived vicarious increases in legitimacy based on the legitimacy of other organizations with which they interacted.
Circumventing Resource Constraints and Legitimacy Deficits
As citizens began engaging in augmenting behaviors to increase resources and legitimacy, they encountered barriers they tried to circumvent. First, limited access to specialized equipment and materials meant that most citizens were left to act as bricoleurs, making do with resources available locally because they believed something was better than nothing (Baker & Nelson, 2005; Korsgaard et al., 2021). The need for a rapid response meant that citizens frequently satisficed, or made do with solutions deemed adequate but far from optimal (Simon, 1987). This reflected an intentional trade-off between providing fast stop-gap solutions and crafting high-quality, but time-consuming “custom, bespoke, artisanal PPE,” as one informant in Stilton joked about. Given their dire need, some recipients of citizen-produced PPE expressed an initial tolerance for these trade-offs. A public agency administrator in Edgeville stated:
We knew it wasn’t the perfect solution. But we knew we had to give [our employees] something to protect them as soon as possible because we knew that this was a gravely dangerous virus. And so, something was better than nothing.
Second, citizen groups worked around knowledge gaps by experimenting with prototypes and techniques with the limited information available. Although many actors were familiar with prototyping and iterating designs, the nature of the pandemic demanded experimentation with unfamiliar materials, use case scenarios, and production techniques necessitating design for manufacturing rather than prototyping. One informant in Edgeville described how user input informed their experimentation, “I remember giving [a clinician] a few different styles and sizes of ear savers, and her nurse buddies figuring out which ones they liked more. [I was] pivoting the design files that I was using based on that real world feedback.” In lieu of subject matter expertise or official government guidance, the best citizen groups could hope for was to receive user feedback directly or obtain it indirectly through their social ties or the Internet.
Third, citizen groups adapted to overcome legitimacy deficits by bypassing established norms and procedures to take risks for the greater good. In Stilton, one informant summarized the citizen group’s relationship to the government, “Regulatory agencies. . . we ignored them, and they ignored us.” Multiple informants used subversive language to describe how they dealt with this lack of regulatory legitimacy. A group leader in Stilton said:
We’re a guerilla organization. . . .If you try to go through the front door, there’s just lawyers’ arms akimbo. You just can’t make any headway that way. So, what we’re doing is reaching out to our friends saying, ‘Hey, do you know any people in the health care field who need PPE?’ We made those relationships to get our stuff in the back door.
Perceiving that hospital bureaucracy impeded effective crisis response, citizens often justified circumventing norms rather than relying on augmenting their legitimacy.
Many frontline workers in need of PPE gave credence to the citizen perception that moral legitimacy trumped a lack of regulatory or cognitive legitimacy in a crisis. An informant in Triport conveyed a common theme:
Individual nurses or doctors who worked within the hospital said, ‘You know what? We’re going to ignore the supply chain and I’m going to reach out for help directly because the hospital isn’t helping me get what I need. I’m gonna go to these people who can get me what I need directly.’ I know that happened a lot.
Some clinicians urged secrecy about deviant activities, while others were vocal, posting supportive social media messages. Stories like these motivated citizens by casting their efforts in heroic terms. Thus, by circumventing their regulatory and cognitive legitimacy deficits vis-à-vis institutions, citizen groups acted based on their perceived moral legitimacy.
Fourth, citizens also sought to circumvent legitimacy deficits by pressuring institutions to act through perseverance and creating social anxiety. Some citizens applied social pressure in attempts to help their groups overcome resistant administrators and prohibitive institutional policies. In Midburg, a small business owner whose group made face shields characterized his behavior in contacting hospital purchasing managers, “I am very obstinate. I would call and call and not take no for an answer and tell them I’ll be there in 30 minutes.” A medical student with ties to multiple citizen groups in Triport described using “brute force” to contact hospital supply chain managers. Also, an institutional makerspace manager in Triport bypassed institutional channels to pressure an influential donor to help release equipment for PPE production:
I did some social engineering on a really heavy level. . . Then getting the release of the equipment cascaded into [a university] released their equipment. . . Because of the social pressure, they couldn’t say ‘no’ at that point. . . That’s a known technique—social engineering in the hacker community. . . We did social hacks in order to force equipment because we believed it was very important to get this PPE out.
The use of social pressure to “liberate” equipment illustrates how citizen resource mobilization involved both legitimation and resourcefulness behaviors to circumvent obstacles.
Period 2: Advancement
After weeks of activating their crisis response efforts, citizen groups began to produce and distribute large quantities of PPE during the period from April to mid-June (see Figure 4). In Table 5, we report how their response effectiveness and adaptive behaviors evolved as they continued to customize their solutions to meet local needs. While augmenting and circumventing behaviors continued, citizen groups also learned to attenuate their resourcefulness and legitimation behaviors to target beneficiaries who would accept and use their solutions.
During this period, institutions began to recognize the difference between a local crisis and a global, systemic crisis (Laufer, 2007). One key indication of this was when desperation in hospitals outweighed liability concerns. An informant in Triport explained how institutional resistance to outside help at some hospitals yielded to urgent needs:
If you had the face shield design that made its way onto the NIH (National Institutes of Health) 3D Print Exchange and it had the ‘verified by clinician’ checkmark next to it, it would give you a huge leg up in getting that item into a hospital and past the purchasing folks. . . .The purchasing folks gave us a really hard time over respiratory protection. Face shields were really not a huge concern for the infection control departments. . . They were splash protection. It wasn’t going to hurt their providers in such a way that they’d be liable for anything. But the respiratory protection was really the major concern. . . that they were very reluctant to work with us on if we didn’t have the right brand of N-95 [mask] in our inventory. . . Until a couple weeks later, when they were like, ‘Give us whatever you have.’ That’s the way it worked for a lot of these hospitals. Very quickly [their purchasing policies] didn’t matter anymore.
Thus, citizens learned how to customize types of PPE based on changing institutional certification requirements, even as the regulatory legitimacy landscape fissured.
However, even as citizen-made PPE became more readily accepted, citizen groups continued to encounter institutional resistance as well as obstacles that proved insurmountable, despite citizen augmenting and circumventing behaviors. Among clinicians, stories circulated of people being fired for violating hospital policies that prohibited employees from openly asking for outside PPE. A clinician in Stilton described similar access restrictions in nursing homes at a point in the pandemic when nursing homes were already COVID-19 hot spots. Facing these challenges in major institutions and urban centers, citizen groups adapted by searching for and responding to more receptive organizations, such as smaller hospitals in surrounding communities. As shown in Table 4, private clinics and nursing homes were also high on the list of recipients by volume of PPE received in our cases. Groups also began to distribute PPE to non-hospital first responders, non-medical essential businesses, food pantries, local schools, Native American reservations, and the incarcerated population.
Response Effectiveness
Regarding scale, our data on volunteer involvement and PPE production volume both indicate that citizen groups reached peak activity in this period (see Figures 3 and 4). Regarding customization to local needs, our data on recipient opinions of PPE quality and usefulness ranged from viewing it as superior to traditional supplies to viewing it as inadequate or counterproductive. The negative or lukewarm response from some PPE recipients highlights how cognitive legitimacy involves both acceptance and use of a solution, and how extensive efforts to customize and legitimize solutions did not guarantee their use.
Importantly, inverse relationships surfaced between the four response effectiveness dimensions as the urgency of customizing novel solutions to meet local needs prompted citizens to temper the scale, scope, or speed of their efforts at times. Several citizen groups reduced scope (by producing fewer types of PPE) so they could meet local needs with increased speed and scale. A Midburg makerspace organizer explained how local customization required learning:
If we had known from the beginning that we should just focus on face shields, that would have saved us a lot of time and we would have been able to produce a lot more of them. That floundering at the beginning was just a lot of stress and time wasted.
In other instances, reducing speed and scale enabled better customization to local needs. An informant from another makerspace in Midburg described how institutional reluctance helped his group learn to prioritize meeting local needs, “I respect a lot the way [a major hospital] slowed things down and was resistant to reacting quickly.” Thus, learning was critical to overcome lack of know-what and know-how for customizing solutions institutions would utilize, even at the expense of scale, scope, or speed.
Resource Constraints
New resource challenges arose during the advancement period. Inadequate citizen social ties to institutions led to a lack of feedback from recipient contacts and therefore a gap in learning. Although some larger institutions found that imperfectly matched PPE from citizens caused problems, nonetheless the only feedback many citizen groups received came in the form of not receiving reorders. Without further explanation, groups did not know how to interpret this information. A makerspace member in Stilton expressed concern:
We very rarely got repeat requests. That’s a bad metric. . . You want repeat customers. . . It’s speculative as to why. Maybe they got what they needed and made it last. Maybe they found another source. . . I have no idea.
A sewing group in Midburg celebrated a 20% reorder rate as a success.
Human resource constraints surfaced as mostly uncompensated volunteers risked burnout from working long hours and taking on excessive responsibilities (Oliver, 1984). Although motivated by altruism and a sense of civic duty, the volunteer amateur labor pool was generally insufficient for the demand and poorly matched to the specialized circumstances (Barker & Gump, 1964). Moreover, despite extensive citizen learning, some expertise gaps proved too much to overcome. A paid staff member at a Midburg makerspace expressed frustration that incompetence for industrial scale manufacturing inhibited personal agency:
There’s a big difference between how you make things at a small scale, like prototyping and flexible manufacturing, and how. . . things that we use are genuinely made. . . I’m interested in it, and I still find it hard to understand.
Even if such expertise were available, most citizen physical resources such as space and equipment simply could not support large-scale manufacturing. An individual in Triport who contributed 3D parts to a large, distributed citizen group said, “I learned about how to produce mass quantities of things on a machine built for prototyping.” However, the aggregate “mass quantities” achievable from such efforts still constituted a small portion of the overall demand.
Regarding financial constraints in this period, citizen groups that initially decided to sell PPE at cost experienced complications related to cash flow and organizing a sales operation function. The ramifications of this decision led one informant at a Midburg makerspace to regret not attempting crowdfunding at the outset. Although it was difficult to observe unsuccessful attempts, web searches and secondary documents indicated many crowdfunding campaigns to fund citizen efforts gained only minimal traction.
Legitimacy Deficits
The relative cognitive and sociopolitical illegitimacy of citizen groups continued to be a challenge. As groups gained access to select institutions, they faced regulatory legitimacy questions from sophisticated purchasing managers accustomed to rigid product specifications and quality standards. An informant from Midburg commented:
Some hospitals. . . were like, ‘What have you done to show that these are up to a certain quality?’ And we didn’t have anything, really, to show or to prove. . . Nothing about longevity or efficacy testing. I don’t think that we were able to do those things.
The federal response to the proliferation of unofficial PPE included a COVID-19 section for PPE designs on the NIH 3D Print Exchange website as well as the EUA announcements made during this period (see Figure 5). A citizen leader in Triport described the temporal implications:
[Hospitals] said, ‘If you can get us the NIH model, we can get more official approval for it.’ So, we started putting the NIH model on for those situations, but we kept printing [a different] model as well because it’s faster. It takes like three times less to make.
Thus, citizen groups sometimes perceived a trade-off between building trust via pursuit of regulatory legitimacy and improving the speed and scale of production.
Citizen groups eventually learned more about their cognitive legitimacy, based on how their actions were received by local organizations and institutions. A corporate makerspace manager in Edgeville told us that people with ready access to corporate resources were nevertheless often stymied because the company did not “fully support” their efforts to utilize company equipment and space. In other instances, citizen groups experienced increased trust based on early efforts in the activation period. An informant reported how the collective actions of Triport medical students to distribute PPE eventually overcame institutional reluctance, “Our university paid us no attention until we got up and running. They welcomed us with open arms once they saw what we were doing.”
However, even when institutions tolerated entrepreneurial efforts out of necessity, citizen groups were far from a taken-for-granted part of the environment. A clinician in Edgeville explained why major hospitals represented difficult targets for unofficial PPE:
[My hospital] seems reluctant to formally rely on any of these kinds of supplies. We were receiving donations and they were made available to us. But otherwise, [the hospital] went to great efforts to kind of put together its own PPE supply chains for the face shields and managed at least one way or another to supply everything else pretty well.
Some institutions issued cease-and-desist letters to citizen groups engaged in circumventing behaviors. Other hospitals, such as those in Stilton, simply ignored the efforts of its various departments to procure unofficial PPE by any means necessary.
In this period, many citizen groups shifted their focus and began supplying organizations that accepted them based on urgent need and moral legitimacy. Thus, citizen groups sought recipient institutions that perceived them as helping create a public good through procedures and organizational forms that, despite their unorthodoxy, were acceptable in a crisis.
Attenuating Resourcefulness and Legitimation
We found that the lessons citizen groups learned from augmenting and circumventing helped them make additional adaptations in the advancement period. We label these adaptive behaviors “attenuating” because of how citizens shifted away from trying to do more to overcome constraints and deficits, to instead finding a better fit based on their limited resources and legitimacy. Attenuating was important because crisis response could prove ineffective if citizen groups became overwhelmed with too many PPE design ideas or with trying to customize solutions to innumerable local needs. We found attenuating to be among the most common adaptations for both resourcefulness and legitimation across all four cases. By attenuating resourcefulness and legitimation, citizen groups learned to accept their limitations and become more selective about how to meet local needs in the process.
First, attenuating resourcefulness involved deciding not only what to do but also what not to do, as citizen groups resisted the personal and collective urge to pursue a wide range of divergent ideas. A group leader in Stilton talked about resisting the creative allure of inventing novel designs, “We’re extremely creative people and, left to our own devices, we could just create things all day. . . But we didn’t want whatever we made to end up in a trash bin because nobody asked for it.” Pressure to respond quickly created tension between the need to produce useful solutions at scale versus experimenting with plentiful ideas. A leader in Triport stated, “[The way] maker people do things, everybody wants to make their own version of something. Eventually, we just put the kibosh on that.” Strong leadership decision-making within emergent groups proved to be a critical component in helping citizens focus their customization efforts.
Attenuating resourcefulness helped citizen groups decide which feedback regarding local needs to act on so they could move forward with greater scale and speed. We found that more focused groups produced quicker responses to local needs. An independent makerspace leader in Midburg explained how feedback from a hospital helped them learn where to focus:
The biggest [obstacle] was. . . trying to figure out a safe way to contribute. . . It seemed like there was such a rush of people wanting to help, having some resources, and not knowing what the best direction to direct your efforts was. It wasn’t until that call with [a hospital] where we realized the only feasible way for us to engage was with face shields.
Focusing production by limiting scope of PPE varieties helped citizen groups better match their resources to local needs. This also required citizens to be willing to stop any given project if it failed to meet local needs.
Second, attenuating legitimation involved tiering institutions according to relative legitimacy to identify underserved areas to help. In time, citizen groups adapted their target recipients (see Table 4) based on each organization’s legitimacy in its own field, as reflected in purchasing power and access to supply chains and government assistance. A makerspace volunteer in charge of outreach in Midburg described their group’s evolution to match their efforts with a middle tier of underserved organizations:
There’s this small business middle ground where you have retirement facilities, you have dentist offices, you have salons who are struggling... Then you have this institutional level of your [large hospitals] . . . It was not as effective for us to just make [PPE] to order for the public and we would be a drop in the ocean for the bigger tier. . . There really is this middle tier where we can give PPE to people serving the public and trying to stay in business. They don’t have access to the same places that the hospitals do.
Several informants described changing strategies to “right-size” their target recipients based on less prominent institutions. A group of medical students in Triport categorized five tiers of clinical facilities. Citizen groups learned to decrease their legitimacy deficit by targeting organizations with lower legitimacy levels of their own.
Through collective action, each citizen group learned about its legitimacy relative to other citizen groups. A makerspace member in Midburg explained how other groups with direct university and hospital ties focused their efforts on producing disposable PPE in large quantities to help serve the needs of large hospital systems, “The disposable ones were being handled by other organizations that had a bigger mission to solve. And ours was kind of smaller in some ways, but just as important for the right people.” Part of determining which institutions to help included learning what other citizen groups with greater legitimacy were doing so as not to duplicate efforts or waste time attempting to augment legitimacy there. When citizen groups matched their relative legitimacy to that of their intended recipients, they experienced improved fit between their mission and their environment (Naman & Slevin, 1993).
The Temporal Tensions of Urgency
A cautionary tale that occurred in the Edgeville case during this period illustrates the potential negative consequence of achieving scale and speed based on successful augmentation behaviors, but without sufficient adaptations to customize to local needs through attenuation. A public agency ordered large quantities of PPE from a citizen group anchored by a makerspace in Edgeville. An agency procurement manager learned about the citizen group at a time when PPE could not be sourced from other suppliers and “speed was very important in a situation where lives were at stake.” Despite the unknown citizen group, the manager chose to trust the group to equip employees nationwide based on the group’s legitimacy augmenting behaviors, such as “name dropping” a reputable hospital they were in contact with.
However, after several rounds of prototyping feedback and multiple orders amounting to several thousand units of PPE, the procurement manager determined that the PPE “just didn’t really meet our people’s needs.” The manager shared the institutional perspective:
Hindsight is always 20/20. . . Even with the time pressures, I would have done. . . more field testing. . . Resist the temptation to provide an immediate solution. . . It’s like pay now or pay later. If you get stuff to [employees] immediately, it appeases the leadership to a certain extent. . . But as soon as the complaints come in from the field about fit, or ‘this doesn’t work. . .’ When the administrator hears complaints from an [employee]. . . it really comes back to haunt us in a big way. In hindsight, even at a time when we’re under great duress, sometimes it’s better to make the right decision rather than the fastest decision.
This example is a reminder that regulatory requirements concerning quality and liability serve a purpose in institutions charged with the provision of public goods. In this instance, citizen efforts to help a public agency in need resulted in temporarily suppressed institutional norms being reinforced in the crisis aftermath (Bitektine & Haack, 2015). This example also shows how attempting to create a public good amid urgency bypassed satisfactory customization to local needs. By failing to recognize this and attenuate legitimation and resourcefulness accordingly, a citizen group produced a negative outcome while trying to help.
Period 3: Abatement
Beginning around mid-June 2020, citizen groups began to wind down their PPE activities at varying rates, as illustrated by volunteer activity and production levels in Figures 3 and 4, respectively. Our analysis did not identify any new adaptation behaviors intended to improve response effectiveness in this period, although PPE production and distribution continued to evolve for a few groups. In Stilton, one group utilized excess financial resources from successful crowdfunding to transition to outsourced manufacturing in China for some PPE components. They also purchased ready-made PPE to deliver through their existing distribution channels.
In each case, at least some citizen PPE activity continued until the end of the year, albeit at reduced scale. The groups that remained active focused on identifying and serving need gaps in their communities, such as PPE for poll workers during the 2020 U.S. election in November. Due to their attenuation adjustments, citizen groups operated with increased clarity about their roles in addressing local needs for underserved beneficiaries. Overall, groups recognized that the temporary effort ran its course as volunteer burnout increased and supply chains recovered. Thus, augmenting and circumventing behaviors diminished.
Resourcefulness behavior gradually involved less collective agency in this period. Even though citizen group narratives on websites continued to highlight collective action, only a few committed volunteers continued the effort driven by personal agency. Legitimation behavior also abated as the emergent citizen ventures wound down and no longer sought complete acceptance by the public or institutions. Still, what citizen groups learned about their response effectiveness influenced their legitimacy narratives regarding planning to potentially reactivate in future crises. Several groups compiled reports to celebrate their accomplishments and volunteers, and some wrote policy recommendations based on the lessons learned.
Summary: Adaptive Citizen Resource Mobilization
Our study traces the spontaneous start, temporary burst, and subsequent decline of emergent citizen groups producing and distributing PPE in four U.S. cities during the COVID-19 public health crisis. To overcome resource and legitimacy barriers to effective crisis response, the citizen groups in all of our cases learned to adapt their resource mobilization through collective action (Mithani, 2020). At the onset of the crisis, citizen groups immediately encountered constraints across social, human, physical, and financial resources. Citizen resources paled in comparison to the problems they faced, as citizen makers were small scale, often unknown players, compared to the large institutions they dealt with. Over time, citizen groups encountered relative deficits compared to the level of regulatory, moral, and cognitive legitimacy that local institutions required to trust citizen groups, accept their help, and use their PPE.
Early on, citizen groups adapted to overcome these barriers by attempting to augment their resource stocks as well as their moral and cognitive legitimacy. Due to the urgency of the crisis, citizen groups quickly determined they could neither wait for nor rely on augmenting behaviors alone. Thus, they also developed behaviors intended to circumvent resource constraints and institutional norms. Despite the complexities of navigating regulatory and cognitive legitimacy deficits, citizen groups that performed well over time learned to find alternative targets for their PPE based on (1) identifying underserved institutions through the process of matching local needs and (2) finding organizations where the moral legitimacy deficit was lower. These adaptations required citizen groups to attenuate their resourcefulness and legitimation behaviors, as well as to recognize that creating custom solutions acceptable to local institutions sometimes required reductions in scale, scope, or speed (Dutton et al., 2006).
As a result, many citizen groups in our cases eventually learned to accept their limitations and to operate within them. A clinician in Stilton who functioned as both PPE recipient and producer expressed a sense of resignation about the reality of these limits:
I think back to nursing homes. I don’t even know what I could have even done because, even if I sound the alarm or told the media, no one’s gonna believe me. . . At the end of the day, we tried our best to really help these places.
Although emergent citizen groups contributed in impressive ways during a critical early stage in the crisis, resource and legitimacy limitations nevertheless limited the success of their efforts during a crisis of overwhelming magnitude.
The extreme temporality of emergent citizen groups responding to crisis also revealed the complexity and tensions of resource mobilization in transient ventures. Ultimately, some citizens viewed their efforts not only as temporary organizations that had served a short-term purpose, but also as a mode of collective action that could be reactivated (Bakker et al., 2016). Others viewed the volunteer PPE effort more narrowly as an achievement unto itself that allowed citizens to feel like they made a difference early on, before the shared sense of civic responsibility waned (Dinger et al., 2020).
Discussion
Our temporal analysis of emergent groups responding to a public health crisis revealed the process through which citizens mobilized resources despite being outsiders relative to local institutions such as hospital systems (Takeda & Helms, 2006). Emergent citizen groups attempted to overcome, work around, or work within their resource constraints and legitimacy deficits as they operated in the interstices between established institutions (Madden et al., 2012; Stallings & Quarantelli, 1985). We found that citizen groups made three adaptations—augmenting, circumventing, and attenuating—to how they mobilized resources based on continual learning throughout a time-compressed process that was unfamiliar to them and to the institutions they sought to help. Whereas the entrepreneurial resource mobilization literature emphasizes resource search, access, and transfer (Clough et al., 2019), we explain how adaptive resource mobilization involves constant iteration between entrepreneurs and their environment. Thus, entrepreneurs must continually learn about their progress and decide how to adapt—whether to augment resources through search, circumvent resource constraints through bricolage, or attenuate their pursuit of more resources and work within their limitations. When entrepreneurs work under time pressures, such as during crises, adaptive resource mobilization requires simultaneous rather than sequential pursuit of legitimacy alongside resource search and bundling (Delmar & Shane, 2004).
Based on our findings, we built theory to explain how collective entrepreneurial action can lead to effective crisis response via the limited resources and fragile legitimacy of emergent citizen groups (Mithani, 2020). In Figure 6, we depict the emergent theory as a model of citizen resource mobilization to meet local needs amid crises. The model depicts how varying endowments of resources and legitimacy mediate the relationship between entrepreneurial citizen action and crisis response effectiveness. The model shows the moderating roles of the three adaptation behaviors that can function as mechanisms to help emergent groups respond more effectively.
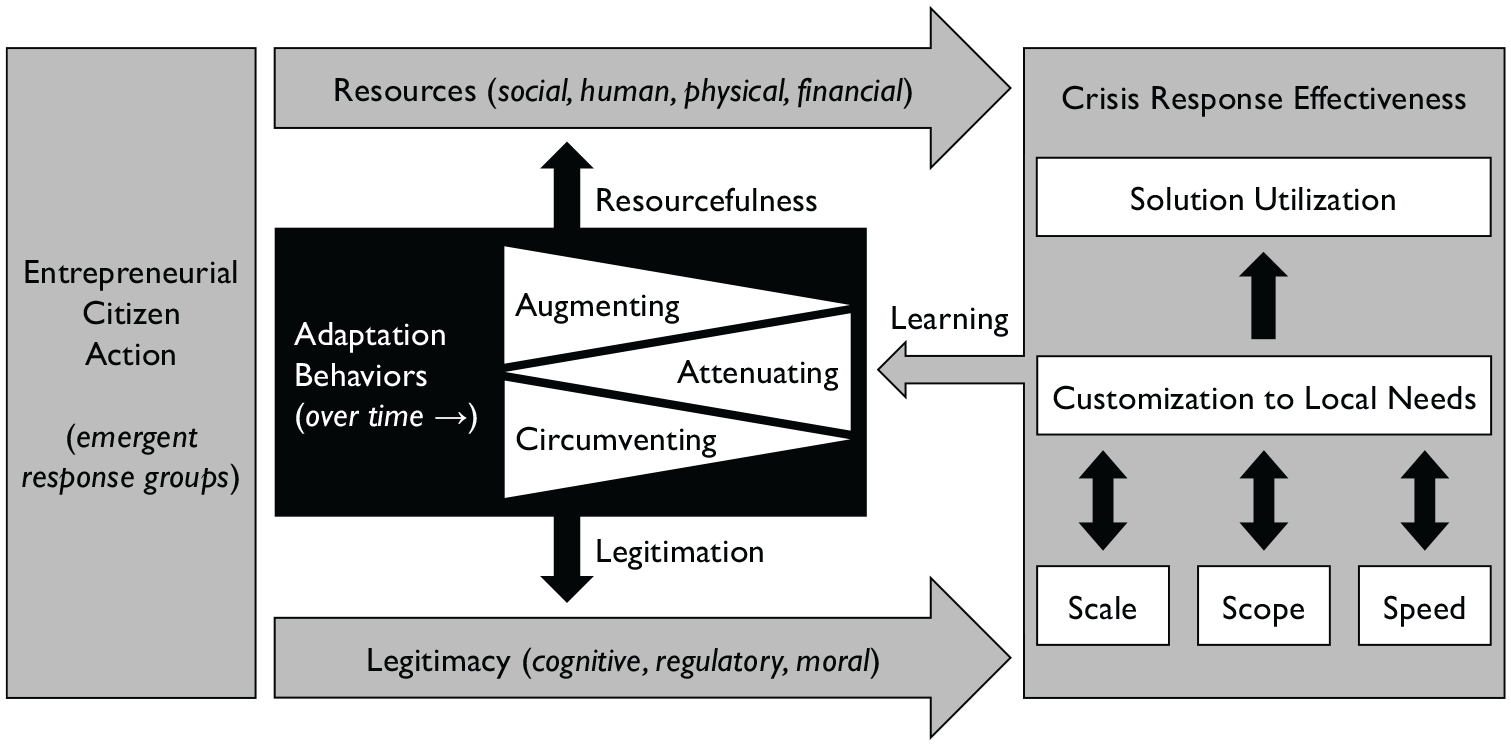
Model of citizen resource mobilization to meet local needs amid crises.
In the “crisis response effectiveness” section of Figure 6, we distinguish between the action of customizing solutions to local needs versus the utilization of solutions by those in need, based on our finding that customization by citizens did not necessarily result in utilization within local institutions. We also position customization to local needs as the key dimension of response effectiveness, which mediates the relationship between solution utilization and response scale, scope, and speed (Dutton et al., 2006). To improve customization, citizens may adjust the scale, scope, or speed of their response, as indicated by the bidirectional arrows pointing to those features. Although an ideal crisis response effort might be capable of maximizing all four dimensions, the reality for emergent citizen groups operating amid extreme temporality reveals a potential for inverted relationships that, left unmanaged, can be wasteful or counterproductive (Williams & Shepherd, 2018). We argue that citizens must learn the contingencies regarding when to reduce scale, scope, or speed to improve customization to local needs, particularly when crisis response involves the local creation of new solutions rather than the bundling of abundant outside resources (Shepherd & Williams, 2019).
The “adaptation behaviors” in Figure 6 indicate the relationship between entrepreneurial citizen action and response effectiveness is strengthened when adaptative behaviors are high and timely. The three behaviors function as mechanisms to help citizen groups calibrate resource mobilization based on learning over time (Majchrzak et al., 2007; Sutcliffe & Vogus, 2003). The “resourcefulness” arrow depicts how citizen actors can address social, human, physical, and financial resource constraints by increasing resources (augmenting), working around constraints (circumventing), or focusing resources to work within limitations (attenuating). The “legitimation” arrow depicts how citizen actors can address cognitive, regulatory, and moral legitimacy deficits by increasing legitimacy (augmenting), working around legitimacy deficits and institutional norms (circumventing), or matching their efforts with lower legitimacy institutions where the relative deficit is smaller (attenuating). We highlight attenuating as the mechanism by which citizen groups adapt to work within their limitations to mobilize resources under extreme time pressure. The shapes of the “augmenting,” “circumventing,” and “attenuating” features depict the relative timing and extent each type of behavior may occur over the life cycle of a transient crisis response effort. The triangular shapes show augmenting and circumventing behaviors decline over time, whereas attenuating behaviors increase. Thus, variance in citizen resource mobilization stems from (1) high or low levels of the three adaptation mechanisms as well as (2) the timing of when citizens adapt given temporal pressures. The “learning” arrow indicates how effective citizen groups utilize available feedback from their crisis response efforts to inform continued adaptations through resourcefulness and legitimation.
Implications for Theory
Our study in the context of the COVID-19 pandemic contributes to the literatures on crisis entrepreneurship, resourcefulness, legitimacy, and makerspaces. First, we extend the crisis entrepreneurship literature by examining how adaptability and temporality influence citizen response effectiveness amid the limitations of a systemic, ongoing crisis (Hallen et al., 2020; Laufer, 2007; Sullivan & Ford, 2014; Williams et al., 2017). We trace the timing of when three adaptive mechanisms were learned to help citizens address disadvantages of localness (e.g., low pre-existing knowledge as system outsiders) during critical early weeks when they scrambled to respond (Bishop, 2019; Chamlee-Wright, 2010). We extend research on citizen adaptation at the community level (Shepherd & Williams, 2019) by specifying three adaptation mechanisms and relating them to resources and legitimacy. We explain how attenuating can help citizen groups focus and work within constraints to meet targeted local needs while expending less time and energy augmenting and circumventing. Unlike other entrepreneurial ventures in which organizational survival and growth are paramount, emergent citizen groups learn to prioritize attenuation over augmentation of resources because of their temporary objectives.
Our process study elevates temporality to show how the urgency of crises constrict the time entrepreneurs would otherwise need to build trust to establish cognitive legitimacy or achieve certification to establish regulatory legitimacy (Aldrich et al., 2020). By taking a longitudinal rather than a cross-sectional approach, we distinguish between citizen action to customize to local needs versus subsequent solution utilization by locals in need. Whereas other studies emphasize the ability of citizens groups to customize a rapid local response (Shepherd & Williams, 2019), we explicitly prioritize customization to local needs for citizen response effectiveness, particularly when citizens must attempt to achieve scale, scope, speed, and customization simultaneously under extreme temporality (Dutton et al., 2006; Williams & Shepherd, 2018). Failure to detect and adapt to these contingencies can lead to negative outcomes in which altruistic intentions cause harm (Sutcliffe & Vogus, 2003).
Second, we contribute to the literature on resourcefulness as a boundary breaking behavior by showing how resourcefulness can drive resource search (i.e., procuring equipment and volunteers) when time-constrained actors must creatively obtain new resources, including alternative resources due to supply shortages (Williams et al., 2021). In addition, we show how legitimacy limitations can inhibit resourcefulness for citizen groups amid extreme temporality by examining cognitive and sociopolitical legitimacy deficits (Aldrich & Fiol, 1994; Delmar & Shane, 2004). Whereas bricolage research examines how entrepreneurs refuse to enact or be constrained by resource limitations (Baker & Nelson, 2005; Di Domenico et al., 2010), the COVID-19 crisis revealed that entrepreneurs cannot always circumvent limitations and that refusal to adapt to limitations may lead to negative outcomes. Thus, a legitimacy lens provides greater explanatory power than subsuming legitimacy among other social resource stocks (Clough et al., 2019; Fisher et al., 2021; Hertel et al., 2021). Furthermore, we show how community resourcefulness (Hertel et al., 2021) in a disrupted environment requires attentive leadership to direct collective action for creating novel, useful solutions (Sonenshein, 2014).
Third, we extend the legitimacy literature by analyzing an empirical context that often eludes research on populations with truncated histories (Aldrich et al., 2020). Our racing design enabled us to observe the transient nature of legitimacy in temporary organizations (Bakker et al., 2016). Temporary legitimacy is fragile and may not last beyond the duration of a crisis if not institutionalized by measures such as formal recognition by established players (Voorhees, 2008). Crises not only truncate the time for acceptance of entrepreneurial actors, but also alter the objective of legitimation (Fisher et al., 2017). Rather than attempting to achieve population acceptance, some groups serve temporary but important purposes such as the creation of public goods (Suchman, 1995). Moreover, following Aldrich et al. (2020), we demonstrate the theoretical leverage gained by distinguishing learning from cognitive legitimacy to theorize how learning occurs at the interplay between legitimation and resourcefulness behaviors over time. In addition, we recharacterize the notion of illegitimacy discount in relative terms as a legitimacy deficit between organizations (Zhao et al., 2013; Zuckerman, 1999).
Finally, we contribute to the literature on makerspaces by highlighting the importance of studying their institutional and spatial contexts (Corsini et al., 2020a, 2020b; Korsgaard et al., 2020). We found that the relative obscurity of makers before the pandemic made them largely invisible to the powerful institutions they sought to engage (Furnari, 2014). We show how under certain conditions, makerspaces can be sites for social value creation in addition to serving as sites for learning, social interaction among hobbyists, or support of early-stage ventures (Halbinger, 2018). Thus, we show how studying makerspaces can extend our understanding of the role of creativity in resource mobilization outside organizational boundaries (Sonenshein, 2014). In addition, as hubs of social, knowledge, and technological resources (Browder et al., 2019), makerspaces can be further studied as nimble, potentially novel organizational forms with unique capabilities for managing technology intensive shared resources (Mortara & Parisot, 2016).
Limitations
We acknowledge three limitations of our study. First, we studied only four cities in the United States and thus could not include all types of self-organized responses to the pandemic in other political, institutional, or regulatory environments. Second, our observations of response effectiveness are not comprehensive. We were aware of many response efforts that gained little traction, but we could not observe all unsuccessful attempts. Third, our structured interview format was flexible for producers and recipients but presented constraints we had to work around for some informants. Despite offering anonymity, some potential informants, especially clinicians and hospital administrators, were reluctant to disclose things or declined participation due to the sensitivity of their experiences and employment.
Conclusion
In this study, we traced the temporal evolution of emergent citizen groups engaged in collective entrepreneurial action in response to the COVID-19 pandemic. We identified the adaptive behaviors citizens learned as they attempted to overcome, work around, or work within their resource and legitimacy limitations. Based on these findings, we built a theory explaining how augmenting, circumventing, and attenuating adaptations can strengthen the relationship between entrepreneurial citizen action and crisis response effectiveness. Thus, we add to research about the significant role of spontaneous venturing in crises.
Supplemental Material
sj-pdf-1-etp-10.1177_10422587221120206 – Supplemental material for Pandemic Makers: How Citizen Groups Mobilized Resources to Meet Local Needs in a Global Health Crisis
Supplemental material, sj-pdf-1-etp-10.1177_10422587221120206 for Pandemic Makers: How Citizen Groups Mobilized Resources to Meet Local Needs in a Global Health Crisis by Russell E. Browder, Stella Seyb, Angela Forgues and Howard E. Aldrich in Entrepreneurship Theory and Practice
Footnotes
Acknowledgements
The authors wish to thank: Sarah Jack for expert editorial guidance; two anonymous reviewers for constructive feedback; Gui Cavalcanti and the Open Source Medical Supplies team, and Dorothy Jones-Davis at Nation of Makers for encouraging this research; Ryan Bailey, Jacob Brennan Conley, and Brady Moore for research assistance; and Daniel P. Aldrich, participants at the Academy of Management Annual Meeting, and participants at the Babson College Entrepreneurship Research Conference for feedback on early versions of this research. We appreciate the citizen makers, clinicians, and other front-line workers who responded with speed and perseverance during the onset of the COVID-19 pandemic. Your example inspires us, and we thank you for sharing your stories with us.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support was provided from the Office of the Vice President for Research and Partnerships and the Office of the Provost, University of Oklahoma.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.