
Abstract
Sudden death (SD) is the second most important syndrome associated with death in racehorses. The cause of SD in a large number of horses remains undetermined, and, in many of these cases, causes are not found by gross or microscopic postmortem examinations. Among the known causes of SD are traumatic injuries, including fractures of skull, neck, and pelvis; intoxications (e.g., anticoagulant rodenticides); and others. For many cases of SD in which no significant lesions are found, heart failure, probably associated with arrhythmias, is suspected. Precise phenotypic characterization of SD in horses is critical for diagnosis and prevention. Standardized gross and microscopic postmortem protocols are needed to discern normal background changes that may be present in healthy horses from significant changes that directly contribute to SD. Here, we review the current knowledge on the pathology of SD in racehorses.
Keywords
The practices and protocols that support the highest standards of racehorse viability, safety, and welfare are essential to maintain the health of the industry that is under public scrutiny. The development of evidence-based strategies that reduce fatalities can improve longevity and quality of life for the animals and for their drivers and riders. After catastrophic musculoskeletal injuries that often necessitate euthanasia, the second most common condition responsible for the demise of racehorses is sudden death (
Compared with SD in human athletes, the incidence of SD in racehorses is significantly higher.35,41 In most racing jurisdictions around the world, SD accounts for 10–25% of deaths, with an incidence of 1–3 per 10,000 starts.2–4,19,22,31,50 In human athletes, the incidence of sudden death is 1 in 40,000–80,000 person-years. 21
Precise phenotypic characterization of SD in horses is critical for diagnosis and prevention. Normal background changes that may be present in healthy horses must be differentiated from significant changes that directly contribute to SD. Information about lesions observed in cases of SD in racehorses is limited. Here, we review the literature on the pathology of SD in racehorses.
Definitions
A standardized definition of SD and its variables is necessary to compare data from different studies. However, these definitions vary between authors and jurisdictions. We use the following definitions in this paper:
SD is the death of a closely observed, apparently healthy animal, in which no premortem clinical signs have been observed.31,34,36
Exercise-associated sudden death (
Exercise-associated sudden cardiac death (
Sudden cardiac death (
The definitions of SCD and EASCD used here and in other studies are made despite the lack of definitive functional or morphologic evidence of heart disease on the assumption that fatal cardiac dysfunction directly resulted in the animal’s sudden demise. These assumptions are usually based on the lack of non-cardiac abnormalities that could directly lead to SD or EASD. As more information and tools become available for the diagnosis of cardiac dysfunction, in both veterinary and human medicine, the diagnosis of SD in horses should become more precise.
Postmortem findings in racehorses with sudden death
A. Cases with significant postmortem lesions
Skull and neck fracture
Fractures involving the axial skeleton typically encompass <10% of all reported musculoskeletal injuries of racehorses.12,19,51 Skull fractures may involve several bones,1,2 but the most common are basisphenoid fractures that compress and damage the brainstem (

Traumatic causes of sudden death of Thoroughbred racehorses.
EASD associated with skull and/or vertebral fractures often occurs as a result of displaced fractures with hemorrhage and bone fragments that compress the brain or sever the spinal cord (Figs. 1, 2). It can be difficult to determine if axial fractures were the primary cause of fall of a horse or were the result of a fall produced by underlying lesions elsewhere (e.g., catastrophic limb fracture, or EASCD).12,44
Pelvic fractures
Catastrophic pelvic fractures are often comminuted, involve multiple bones of the pelvis, and have evidence of pre-existing stress fractures associated with the catastrophic fracture (
Pulmonary hemorrhage
Pulmonary hemorrhage is frequently found in horses with SD. Exercise-associated fatal pulmonary hemorrhage (
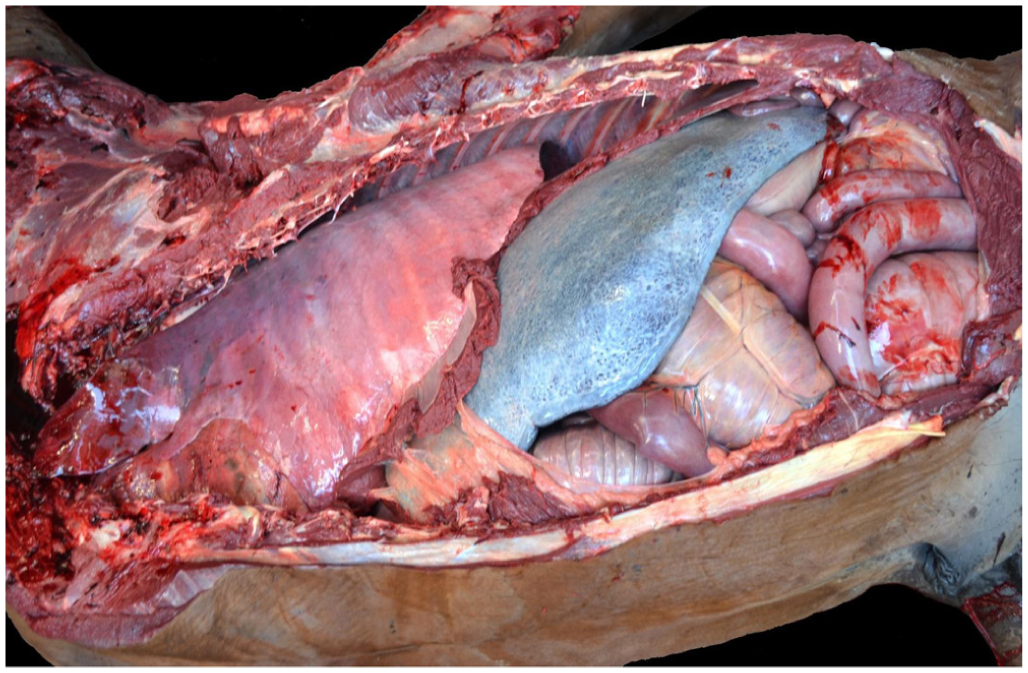
In cases of EAFPH, grossly, the lungs fail to collapse, and there is widespread dark-red to gray discoloration, which is more prominent in the dorsal area of the caudal lobes (

Pulmonary hemorrhage and edema in Thoroughbred horses.

Pulmonary hemorrhage and edema in Thoroughbred horses. H&E.
Other than gross and microscopic examination, no other tests can confirm a case of EAFPH. Pulmonary hemorrhage has been considered to be the cause of death if a large portion of the lung parenchyma is affected and no other identifiable cause of death is present.34,39 However, this conclusion has not been confirmed. Massive pulmonary hemorrhage may also occur as a consequence of previous heart failure with blood pooling in the lungs, leading to hypoxia, endothelial cell damage, and vascular failure within the lungs.
Strenuous exercise has been speculated to be the cause of EAFPH. A sudden diffuse spasm of postcapillary venules with hypercontraction of postcapillary sphincters, similar to those present in rodents, might cause a massive rise in capillary pressure with subsequent vascular rupture.9,43 However, the presence of such sphincters has not been confirmed in horses, and this hypothesis remains unproven. Therefore, given that the etiopathogenesis of EAFPH remains unknown and the severity of lesions can be subjective, the criteria used to attribute death to pulmonary hemorrhage usually vary among institutions and individual pathologists. It is possible that the physical effect of the horse’s collapse in mid-exercise affects the development of pulmonary hemorrhage, given that the intrathoracic force exerted by the collapse of a 450–500-kg animal moving at speed must be significant.
The cause of EAFPH remains unknown, in part because the pathophysiology of this process is poorly understood. Therefore, the criteria used to attribute death to pulmonary hemorrhage usually vary among institutions and individual pathologists. 43 A standardized protocol for gross and microscopic examination of the respiratory system, including rating the severity and extension of hemorrhage, determining chronicity of the lesions, and recording the areas of the lungs affected, among other features, should be established and used by pathologists throughout the world.
Anticoagulant rodenticide poisoning
A cluster of SD of racehorses associated with massive hemorrhage occurred in California, USA.
8
Traces of several anticoagulant rodenticides (
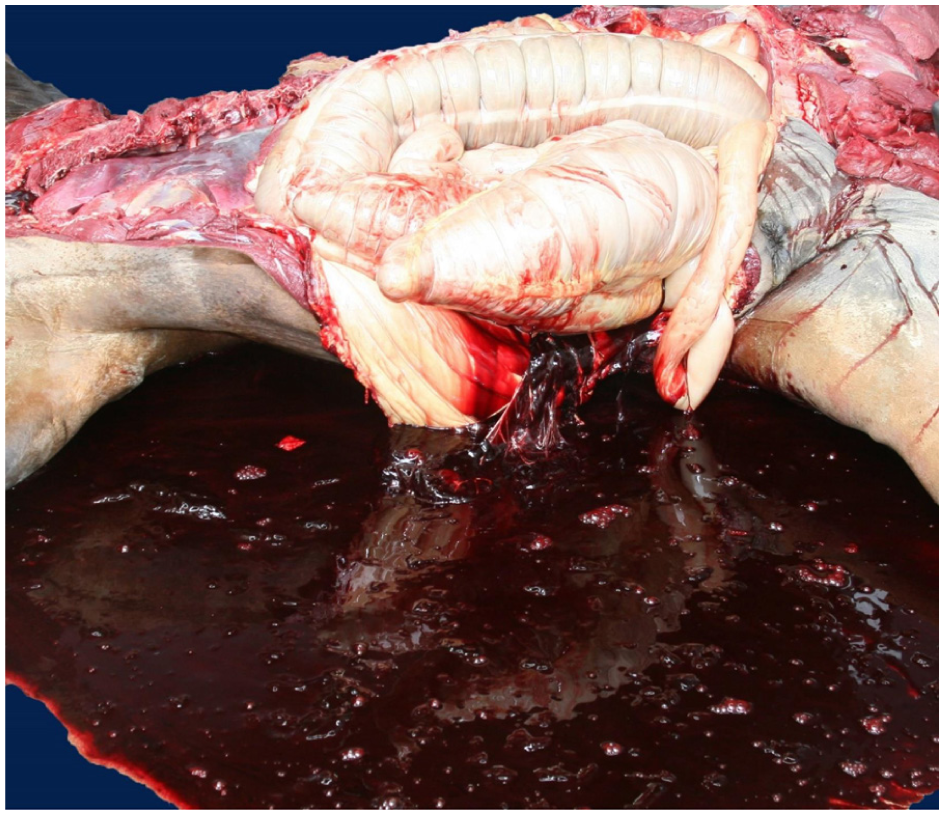
Hemoabdomen in a Quarter Horse with rodenticide anticoagulant intoxication. Reproduced from Carvallo et al. 8
The diagnosis of AR intoxication should be based on detection of these substances in animal tissues by liquid chromatography–tandem mass spectrometry and high-performance liquid chromatography coupled, if possible, with coagulation tests in the living animals. Other differential diagnoses for massive hemorrhages in horses include trauma, neoplasia, vessel rupture, and mesenteric injury.
Vascular rupture
Hemorrhagic shock secondary to vascular rupture occurs in equids. In an international study of racehorse SD,
31
39 of 143 (27%) cases of hemorrhagic shock were diagnosed. Of these, 62% were attributed to idiopathic extra-pulmonary blood vessel rupture, 23% to hemorrhage associated with pelvic fracture, 13% to disseminated hemorrhage, and 3% to pulmonary vessel rupture. Hemoabdomen was reported more frequently than hemothorax or hemopericardium, but the site of rupture was found in less than half of cases.
31
Vessels most commonly implicated in cases of hemoabdomen include cranial mesenteric vessels, caudal vena cava, and the external iliac artery (

Vascular rupture in Thoroughbred horses.
Hemopericardium (
Cardiac lesions
Several primary cardiac lesions can occur in horses, they can be congenital or acquired (
Summary of cardiac lesions reported in several studies of racehorse sudden death (SD).
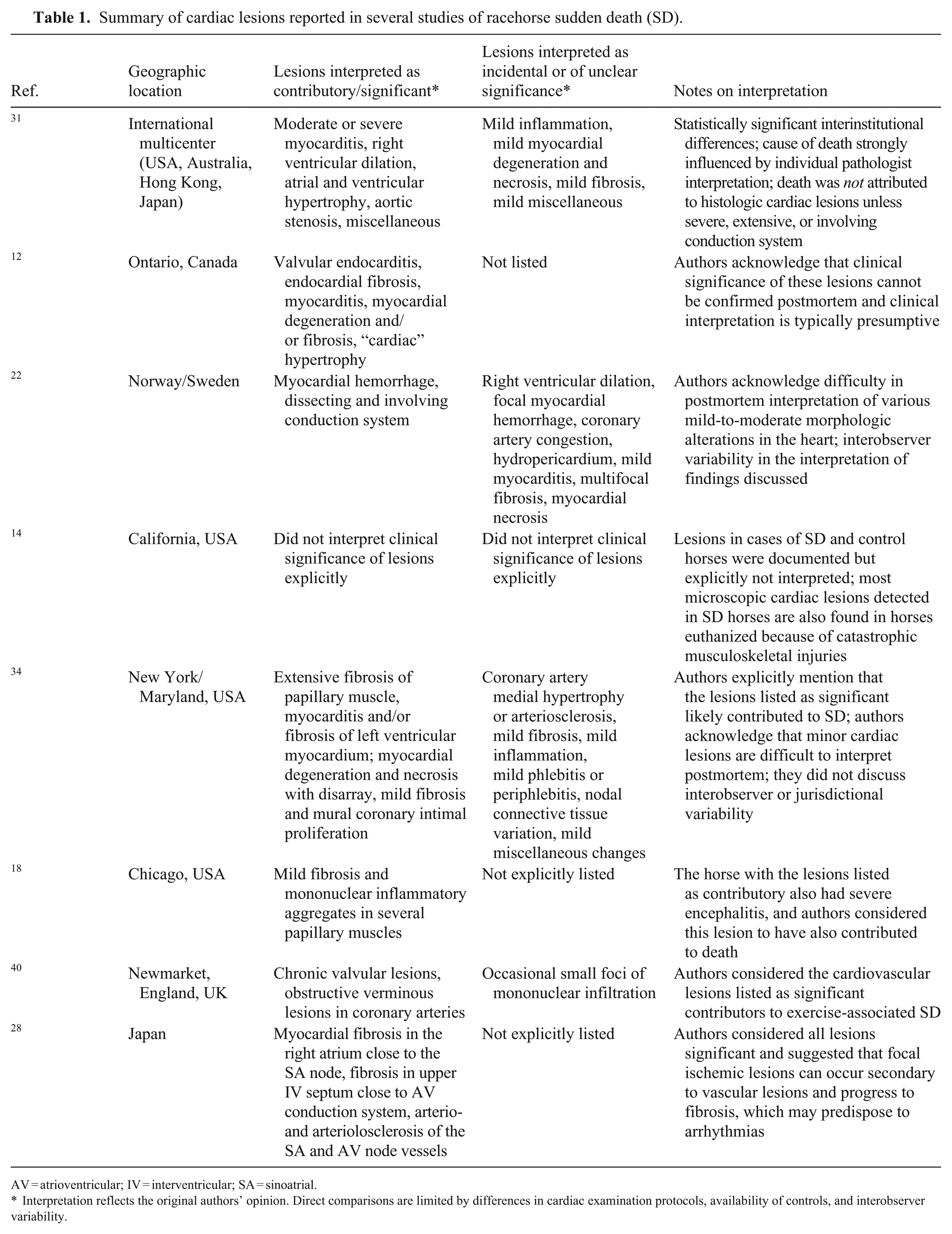
AV = atrioventricular; IV = interventricular; SA = sinoatrial.
Interpretation reflects the original authors’ opinion. Direct comparisons are limited by differences in cardiac examination protocols, availability of controls, and interobserver variability.
The main cardiac lesions mentioned as potential contributors to SD in horses include myocarditis, endocarditis, fibrosis, cardiomyocyte degeneration and necrosis, ventricular or atrial wall hypertrophy, and dilation of cardiac chambers. The great majority of the lesions are microscopic with no gross correlate.12,32,34
Gross lesions in the heart of EASD cases are rarely reported. In a 2011 multicenter study, 31 just 14 of 268 (5%) cases had significant gross changes in the heart, including chamber dilation (3 cases), valvular changes (3), right atrial hypertrophy and right ventricular dilation (1), left ventricular hypertrophy and aortic stenosis (1), subendocardial fibroelastosis and trabecular hypertrophy (1), and other miscellaneous cardiac changes (4).
A retrospective study from Ontario, Canada identified significant cardiac lesions in 6 of 157 (4%) cases, including 2 cases of valvular endocarditis and 1 case each of endocardial fibrosis, mild myocarditis, focal myocardial degeneration and fibrosis, and significant cardiac hypertrophy. 12 In a 2022 study from Melbourne, Australia, 6 of 57 (11%) cases of SCD had significant cardiac lesions, including cardiomyopathy, myocarditis, and left ventricular concentric hypertrophy. 35 In a study from Norway and Sweden, only 3 of 30 (10%) cases with suspect cardiac or pulmonary failure had cardiac lesions suspected to have caused death, and in all cases the main lesion was a dilated right ventricle. 22 Similarly, cardiac lesions interpreted as probable cause or contributory to death were identified in 3 of 40 (8%) cases of EASD of another study from New York and Maryland in the United States 34 ; lesions included regionally extensive cardiomyocyte loss and fibrosis in a papillary muscle, and extensive areas of lymphohistiocytic myocarditis and fibrosis in the left ventricle. In the same study, 34 2 additional cases had lesions interpreted as possible cause or contributor to death, including regional subepicardial areas of cardiomyocyte degeneration and disarray with mild fibrosis in the left ventricle, and mural coronary vessel intimal proliferation.
In a study involving 3 Chicago, United States, racetracks, only 1 of 25 horses with EASD had cardiac papillary muscle fibrosis, which was interpreted as contributory to death, but that horse also had encephalitis; hence, the role of the myocardial fibrosis in the death of the animal was not fully determined.
18
In a different study, a horse from Newmarket, UK at autopsy had small jet lesions in the subaortic endocardium consistent with reflux, and the trainer mentioned abnormalities in gait during fast work.
40
In a 2025 case in California, SD associated with myodegeneration, fibrosis, and myocarditis involved a large proportion of the ventricular myocardium (
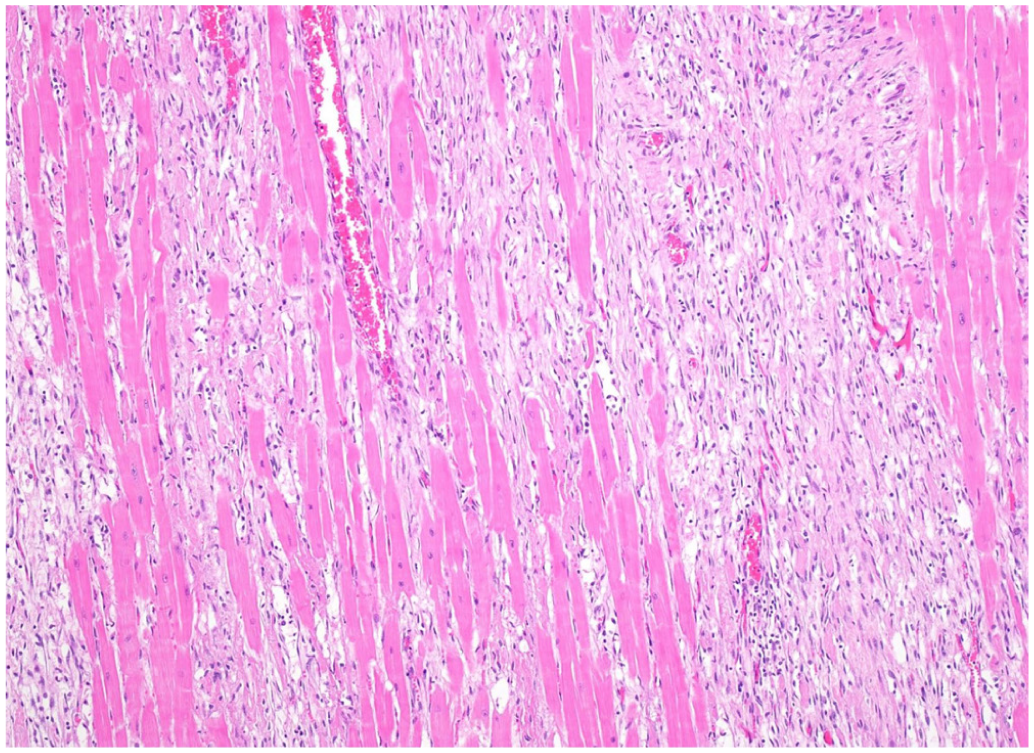
Lymphoplasmacytic myocarditis and extensive myocardial fibrosis in a Thoroughbred horse with presumed embolic myocarditis further to sepsis. H&E.
Ancillary tests depend on the type of gross and/or microscopic cardiac lesions encountered. Special stains such as Masson trichrome or picrosirius red can be used to highlight areas of fibrosis. Masson trichrome staining can also be used to visualize areas of cardiomyocyte degeneration and necrosis; damaged cardiomyocytes are stained purple-blue over a background of red-stained, unaffected, viable cardiomyocytes. 38 Gram and other stains can be used to visualize bacteria in heart tissue, and bacterial cultures can be used to determine the specific microorganism involved. Although viral agents might be involved in some cases of EASD in racehorses, virology studies are rarely performed in horses with EASD, and the role of viruses remains undetermined.
Other
Occasionally, gastrointestinal displacements and ruptures are associated with SD in equids, but these conditions are not commonly reported in retrospective analyses of EASD of racehorses. 31 Most gastrointestinal lesions associated with SD are described in non-exercise–associated SD cases. 12 SD is an unusual outcome of intestinal displacements because affected horses often have clinical signs of colic before death and therefore do not qualify as cases of SD.
Typically, <5% of cases of SD have been attributed to anaphylaxis or an adverse drug reaction, and in some studies, these cases were labeled as injection-associated deaths.12,26 In cases of anaphylaxis, affected animals can have significant laryngeal, pharyngeal, and/or pulmonary edema. A history of drug administration is often critical for the diagnosis. Examination of the neck and vasculature for evidence of injection sites may be warranted when anaphylaxis is suspected. It has also been proposed that nasopharyngeal obstruction by the bit can result in obstruction of more distant portions of the airways, resulting in cardiac failure, a condition that is known as bit-induced pulmonary hemorrhage and asphyxia. 11
B. Cases without significant postmortem lesions, or with lesions of unclear clinical significance
No significant gross lesions that can be used to confirm a definitive cause of death are found in 20–60% of cases of SD or EASD.4,12,26,31,34 Although these cases are often referred to as “autopsy-negative,” some lesions are frequently found, although they are not specific or definitive for a cause of death. Hence, death is presumed to be associated with acute cardiac failure based mostly on the lack of another possible explanation. The most common gross lesions in these cases are severe pulmonary edema, congestion, and hemorrhages of variable severity, and congestion in multiple other organs, particularly the spleen (
Splenomegaly in a Thoroughbred horse with exercise-associated sudden cardiac death.
Although various microscopic lesions in the heart and lungs of the so-called autopsy-negative cases have been reported,4,12,14,22,28,32,34 consensus is lacking regarding their clinical significance and their direct association (or lack thereof) with the cause of death. This lack of consensus is multifactorial, mostly driven by different sampling protocols, lack of controls, limited data, variable expertise, and differences in experience and interpretations among veterinary pathologists and institutions. Here, we summarize the postmortem findings described in horses with SD that had an autopsy report without a clearly established cause of death.
In a study of racetracks in New York and Maryland, United States, 34 findings in SD and control horses were compared. Autopsy was performed in 37 of 40 SD horses. In 22 of the cases, the postmortem examination was performed following the equine SD postmortem examination protocol reported previously by our laboratory. 13 In the other 15 horses, randomly collected cardiac samples were examined. In addition, histology was performed on the heart of 35 control horses, which had been euthanized mostly because of fatal musculoskeletal injuries. Seventeen of the 40 horses with SD were classified as autopsy-negative and had no significant microscopic lesions in the heart. Significant microscopic cardiac lesions were reported in 5 horses from the SD group; no significant microscopic cardiac lesions were reported in any of the horses from the control group. These authors did not consider the presence of mild myocardial fibrosis, mild myocardial inflammation, coronary arteriosclerosis, and variations in cardiac nodal connective tissue as significant and/or the cause of SD because these findings were also observed in the control group. 34 Although it is possible that mild myocardial fibrosis and inflammation may not interfere with cardiac function, severe lesions might lead to severe cardiac arrythmias and SD. 48
In a 2025 study from California,
14
the microscopic lesions of horses with SCD, EASCD, and control horses euthanized because of fatal musculoskeletal injuries were compared. Autopsy-negative racehorses from the EASCD group and control horses were both examined using a standardized SD postmortem examination protocol
13
and had a variety of microscopic cardiac lesions that were classified into 4 major categories: acute cardiomyocyte injury (

Microscopic myocardial lesions of undetermined significance. H&E.
In a 2011 international multicenter study, 31 the cause of death remained undetermined in 22% of cases, and 25% had a presumptive diagnosis of cardiac or cardiopulmonary failure, as suggested by the lack of significant lesions and as interpreted by the individual pathologist. Microscopic cardiac lesions were reported in 25% of all cases. These lesions included inflammation, cellular degeneration, necrosis, fibrosis, mixed, and miscellaneous changes. However, death was not interpreted as associated with microscopic cardiac lesions unless the lesions were severe, extensive, or affected the conduction system. Based on these results, it was concluded that statistically significant interinstitutional differences were evident, both in interpreting the cause of death and in the reporting of cardiopulmonary lesions. Therefore, determination of the cause of death was significantly affected by the interpretation of the individual pathologist. As an example, compared with California, pathologists in Australia were more likely to record acute and chronic pulmonary lesions, pathologists in Pennsylvania were more likely to record pulmonary hemorrhage, pathologists in Hong Kong were less likely to report acute pulmonary congestion, and pathologists in Japan were less likely to record acute pulmonary hemorrhage. Higher proportions of gross and microscopic cardiac lesions were described in California and Victoria, Australia, probably reflecting the more extensive cardiac dissection and sampling protocol used in these centers. 31 The variation in postmortem technique and description of lesions emphasized in that study was a springboard for the development and subsequent publication of a SD postmortem examination protocol, 13 which is now used in several institutions. Toxicology was not reported in most of these cases; hence, a toxic cause of death could not be completely ruled out.13,31
In a different study performed in Victoria, Australia, 4 autopsies were performed using a standardized protocol in 25 racehorses that died or were euthanized while exercising. Seventeen of those 25 horses (68%) were reported to have died of acute pulmonary edema, congestion, and hemorrhage, lesions that are often interpreted by others as nonspecific findings.4,32 The severity of the pulmonary lesions reported in these 17 horses varied but was moderate to severe in most cases. These combinations of pulmonary lesions were considered significant, and it was suggested that they possibly caused SD. In the mentioned study, 4 the authors hypothesized that an increase in hydrostatic pressure in the pulmonary microvasculature during intense exercise may lead to variable degrees of pulmonary edema and hemorrhage. They also suggested that left-sided heart failure caused by myocardial lesions or disorders in the conduction system can contribute to increased hydrostatic pressure in pulmonary capillaries, especially in cases in which pulmonary edema is more severe than hemorrhage. The authors did not discuss, however, why this may only occur in a small subset of horses, given that the vast majority of horses do not develop significant pulmonary edema or severe hemorrhage under intense training or racing. Additional studies are necessary to better understand the pathogenesis of acute pulmonary edema and hemorrhage during intense exercise and whether it may be the primary cause of SD, a consequence of cardiac failure, a terminal/agonal finding, or a combination of these and/or other physiologic factors at play during intense exercise. In the same study, 4 3 horses had mild microscopic myocardial lesions.
Another study described the postmortem findings in 963 racehorses in Ontario, Canada 12 in which 32 of 157 (20%) SD cases had no significant lesions, speculating that cardiac arrhythmia may have been the possible cause. In a study on causes of so-called sudden athletic death (which, according to the description of the authors, is equivalent to EASD) in 38 Standardbreds and 10 Norwegian-Swedish Coldblooded Trotter harness racehorses, 22 30 of these deaths were possibly related to acute circulatory collapse secondary to cardiac or pulmonary failure, or both. However, no convincing gross or microscopic evidence was found to support a definitive diagnosis in 27 of these cases. The other 3 horses had a dilated right ventricle, which was suspected to be the cause of heart failure.
A 1971 study 15 described the gross and microscopic changes in the atrial myocardium of horses with atrial fibrillation. Although it is unclear whether the horses examined succumbed to SD or were euthanized, the authors described atrial fibrosis, mainly in the left atrium, but also in the right atrium. In a 1987 study, 28 the authors also described myocardial fibrosis, possibly the result of ischemia, in the atrial myocardium of 10 horses that died suddenly. These lesions were found close to the sinoatrial (SA) node and in the atrioventricular (AV) junction, often associated with arteriosclerosis. Grossly, the hearts of 8 of the 10 horses examined had significant lesions in the right atrium, which consisted of irregular patchy, gray-white areas on the epicardial surface and also within the atrial wall. Microscopically, all 10 horses had focal myocardial fibrosis in the atria, close to the SA node. These authors suggested that ischemic changes may lead to myocardial injury that is possibly related to atrial fibrillation, SA block, or paroxysmal ventricular tachycardia, depending on the localization of the fibrotic changes. 28 However, other reports studying cardiac lesions in sudden death horses do not mention significant atrial fibrosis as a consistent lesion in horses with SD12,14,32,34 (authors’ unpublished observations). In another study, 29 the same group examined the hearts of 5 horses that died of SCD during or shortly after intense exercise. In one of these horses, an electrocardiogram (ECG) had been performed before death. The ECG had the R-on-T phenomenon following a pair of ventricular premature contractions. This phenomenon rapidly degenerated into ventricular fibrillation and led to cardiac arrest. All 5 horses had foci of myocardial fibrosis in the right atrium near the SA node, fibroblastic or fibrotic changes in the upper portion of the interventricular (IV) septum, and arteriosclerosis of blood vessels near the SA and AV nodes, suggesting that ischemia of the conduction system contributed to SCD.
A study investigating the cause of SD in 200 horses 6 divided these cases in 2 groups: group 1 had 49 horses, mostly Thoroughbreds, in which the SD was witnessed and with a definition of SD similar to that used in our review; group 2 was composed of 151 horses and ponies that were considered clinically normal 24 h prior and died unexpectedly, but they were not closely monitored. In group 1, 15 of 49 cases (31%) had no gross or histologic lesions. 6 In a similar study in Newmarket, England, 40 the authors reviewed 69 cases of SD, which were divided into 3 groups, one of which included 24 horses with clinical histories consistent with the definition of SD used in our review. In 9 of the 24 cases (38%) no significant gross lesions were found. In 8 of these 9 cases, microscopic examination of random areas of the heart was performed. Only 3 horses had rare small foci of lymphoplasmacytic inflammation, but these were considered of unlikely clinical significance. In another study of 25 horses succumbing to SD during training or racing in Chicago, 18 a clear cause of death was found in only 8 of 25 horses (32%). In 17 cases (68%), the cause of death was undetermined, but the authors postulated that these horses may have undergone acute cardiovascular failure. Nearly all horses had pulmonary edema, congestion, and/or hemorrhage. However, the authors did not associate the pulmonary changes with the cause of death.
Discussion and conclusions
Some lesions, such as major internal hemorrhages caused by blood vessel rupture, severe trauma to the skull or cervical vertebrae, or certain intoxications, are usually accepted as definitive causes of SD.8,12,22,31 However, other causes, such as cardiac and/or respiratory failure, and pulmonary hemorrhages, are less definitive, reflect a degree of uncertainty, and have significant interinstitutional and interpersonal variability in the interpretation of gross and microscopic findings.4,12,22,24,32,34,36 For instance, in many cases of EASCD, severe acute pulmonary hemorrhage was observed, but pathologists disagreed as to whether this hemorrhage was a primary event that led to death, as in cases of EAFPH, 43 or if it was the result of heart failure that led to pulmonary congestion, hemorrhage, and anoxia. Another example is a study from California in which microscopic cardiomyocyte injury was found with higher prevalence in horses with EASD than in control horses. 14
We believe that, regardless of their nature, small microscopic lesions in the heart can be clinically significant if they serve as arrhythmogenic substrate or otherwise interfere with normal cardiac function. The data from California 14 also suggests that the opposite may be true: small, and even larger cardiac microscopic lesions may not be associated with the cause of death if they do not serve as arrhythmogenic substrate or significantly interfere with cardiac function. The fact that many apparently healthy, control horses had myocardial inflammation, fibrosis, and miscellaneous lesions suggests that many such alterations may not necessarily be arrhythmogenic.
Horses often have cardiac arrhythmias, which can be frequent in equine athletes during and immediately after exercise.36,48 Whereas some arrhythmias are physiologic, usually related to vagal tone, others are pathologic and pose a risk to horses. The latter can be triggered by underlying cardiac disease, such as acquired valvular disease, congenital malformations, myocardial injury, pericarditis, myocarditis, and endocarditis. Non-cardiac conditions, such as electrolyte and acid-base disturbances, hypoxemia, endotoxemia, and toxic causes can also trigger pathologic arrhythmias. 48 The clinical significance of an arrythmia depends on its hemodynamic impact (blood pressure, cardiac output) and the risk of deterioration to a more dangerous rhythm. 48 Although it is beyond the scope of our review to explore the pathophysiology of equine arrhythmias in detail, they are relevant to any discussion of equine SD, given that an association between arrhythmias during intense exercise and poor performance or SD is strongly suspected, but still poorly understood. 36 This is especially the case in autopsy-negative horses with none or mild cardiac microscopic lesions.
Evidence exists that sudden cardiac death is weakly heritable. 27 Certain stallions appear to be more likely to have progeny that experience SCD, which suggests possible genetic markers associated with this condition. If that is the case, the use of those genetic markers as predictors for EASD would be useful. Although no genetic markers have been identified for EASD at this time, studies to investigate the genetic risk of EASD in horses are ongoing, including whole-genome sequencing, with preliminary results expected soon (C Finno, S Durward-Akhurst, pers. comm., 2026 Feb 23).
In summary, most published data from the last 50 y, together with our unpublished findings and our combined professional experience of performing autopsies in cases of SD in racehorses, indicate that a proportion of cases occur without significant gross lesions4,22,30,32,34,36,48 (authors’ unpublished data). A subset of these cases have either no microscopic cardiac lesions or only mild-to-moderate lesions, the significance of which is variably interpreted by individual pathologists.4,12,22,32,34 Microscopic cardiac alterations can predispose horses to arrhythmias, but they may also occur as background lesions in horses that die or are euthanized for non-cardiac conditions, such as musculoskeletal injuries.14,34,37 A definitive postmortem diagnosis of arrhythmia is not possible, and attributing fatal arrhythmias or SD to mild-or-moderate microscopic cardiac lesions remains largely speculative. These limitations underscore the need for standardized pathology criteria and the integration of advanced, multidisciplinary diagnostic approaches that include antemortem cardiac monitoring with detailed postmortem cardiac examinations. In particular, we recommend standardized histologic examination of the heart
13
(

Recommended 11 sections for heart histology in cases of sudden death.
Further work is needed to determine the cause of SD of racehorses. A critical step in this regard is that all racing jurisdictions perform clinical examinations, postmortem examinations, and reporting following standardized protocols. Standardization of terminology and definition of SD and its variants (CSD, EASD, EACSD) in the literature would also be helpful. Autopsy of a number of horses with SD from which ECG during the hours before death is available would be critical for this purpose.
Footnotes
Acknowledgements
We thank the California Horse Racing Board for the support provided to the CAHFS racehorse post-mortem program for nearly 35 y. We thank Drs. Carrie Finno and Sian Durward-Akhurst for their insightful comments about genetic markers for EASD.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.