
Abstract
Rhabdomyosarcoma (RMS), a malignant mesenchymal neoplasm derived from skeletal muscle, is relatively rare in both human and veterinary medicine. Here we report an unusual case of invasive spindle-cell RMS (SCRMS) with bone infiltration and pathologic fracture in a 3.5-y-old intact female Bulldog. Radiographically, a large, predominantly osteolytic mass in the tibia and fibula of the left hindlimb had features typical of a malignant primary bone tumor. Clinically, osteosarcoma was suspected, and the leg was amputated. Histologically, the mass was composed of loosely interwoven spindle-cell fascicles; tumor cells were fusiform with cigar-shaped nuclei and abundant eosinophilic cytoplasm. The neoplastic cells were strongly immunopositive for vimentin, muscle-specific actin, desmin, myogenin, and myoD1. Invasive SCRMS with osteolysis was diagnosed based on the histologic examination and immunohistochemical (IHC) stains. The dog was alive without any evidence of local recurrence or distant metastasis 18 mo post-surgery. RMS should be included in the differential diagnosis when osteolysis occurs; IHC staining confirmation is of great value for definitive diagnosis and treatment planning.
Rhabdomyosarcomas (RMSs), which are malignant mesenchymal neoplasms that exhibit features of skeletal muscle differentiation, have a wide range of location, age of onset, gross morphologies, and histologic variants. 3 RMSs can occur in any part of the body, including the head and neck region, the genitourinary tract, the trunk and extremities, and even in sites that normally lack skeletal muscle.1,5 Based on the classification system derived from human pathology, 4 common histologic subtypes of RMS exist in veterinary medicine: embryonal, alveolar, botryoid, and pleomorphic RMS.3,14 The various histologic subtypes have distinct biologic behavior and clinical prognosis. 14 Spindle-cell RMS (SCRMS) is a rare variant of embryonal RMS, and is thought to be less aggressive. 2 We describe here the radiographic, histologic, and immunohistochemical (IHC) characteristics of a case of invasive SCRMS with osteolysis in a dog. To our knowledge, there has been only one similar report in a dog. 5
A 3.5-y-old intact female Bulldog had a large mass (20 × 15 × 15 cm) in the left hind leg; the mass was first noticed 2 mo ago and had grown faster recently. There were no other significant signs reported by the owner. Physical examination revealed a soft tissue swelling of the left hind leg, without ulceration, that was painful on palpation. The left hindlimb radiographs showed severe osteolysis and pathologic fracture of the tibia and fibula (Fig. 1A). No evidence of metastasis was found by thoracic radiography and abdominal ultrasound examination. No significant abnormality was found in CBC and serum biochemistry. Clinically, osteosarcoma was suspected, and the left hindlimb was amputated without subsequent chemotherapy. Recurrence or metastasis have not been observed in 18 mo post-surgery.
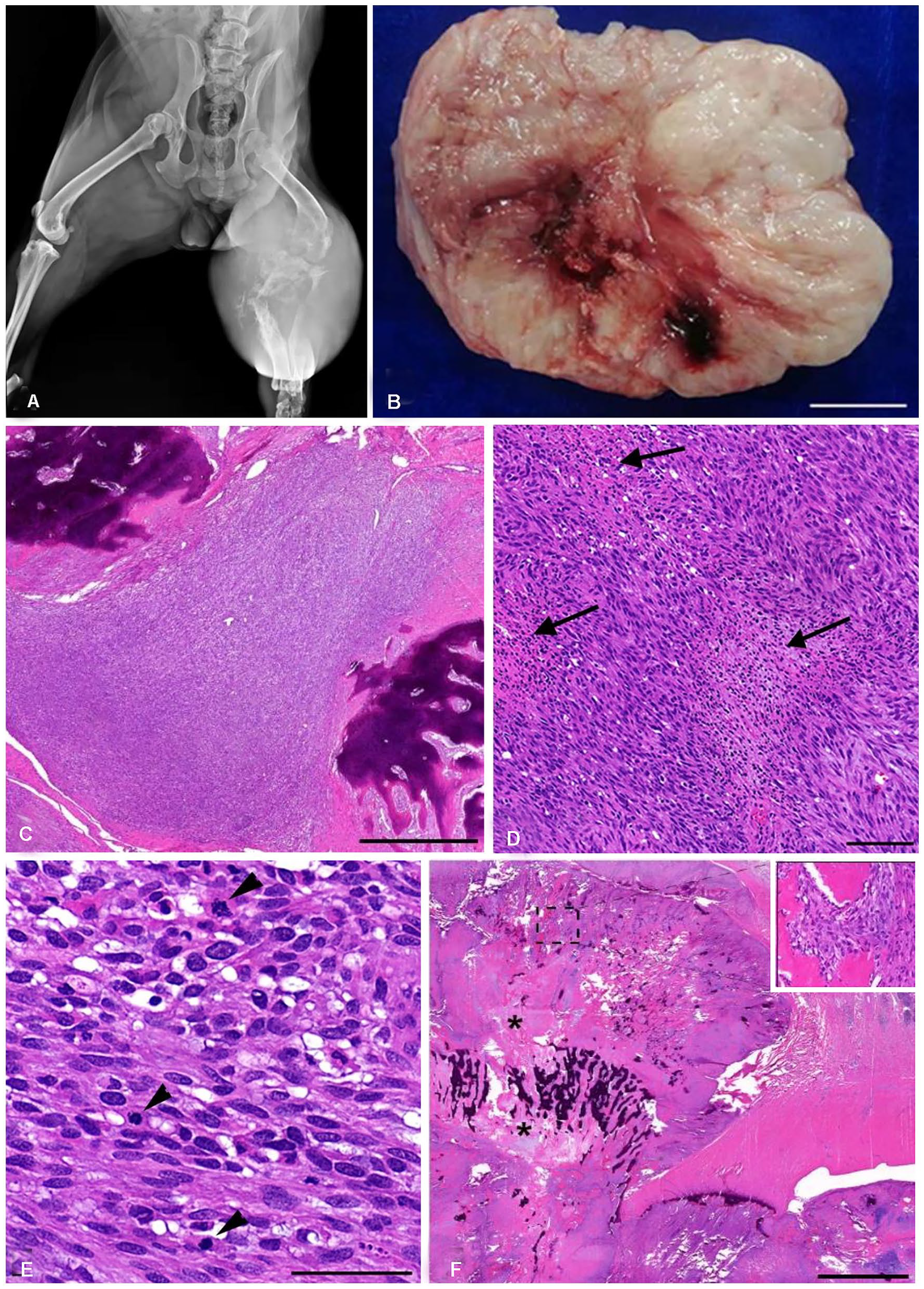
Gross and histologic features of an invasive spindle-cell rhabdomyosarcoma with bone infiltration and pathologic fracture in the left hindlimb of a dog.
Macroscopically, hemorrhagic foci were present subcutaneously on the mass, and the cut surface of the mass was pale-pink and contained bone fragments (Fig. 1B). Samples were collected from 9 sites in the lesion, fixed with 10% neutral-buffered formalin, processed routinely, and stained with H&E.
Microscopically, the mass consisted of spindle-cell tumor areas and osteolytic areas. The tumor area was located subcutaneously, densely cellular, poorly circumscribed, nonencapsulated, with invasion of bone (Fig. 1C). The tumor was made up of loosely interwoven spindle cells arranged in fascicles with random foci of necrosis (Fig. 1D). Tumor cells were round-to-spindle-to-polygonal, with oval-to-elongated, cigar-like nuclei and abundant eosinophilic cytoplasm. Anisokaryosis and anisocytosis were moderate, and the mitotic count was 5 in 2.37 mm2 (Fig. 1E).6,10,11 In the area of osteolysis, some bone trabeculae were present between which were spindle-shaped, loosely arranged mesenchymal cells. There were also cartilaginous matrix and new bone formation in the lesion (Fig. 1F).
Differential diagnoses for our case included osteosarcoma, chondrosarcoma, leiomyosarcoma, rhabdomyosarcoma, spindle-cell carcinoma, spindle-cell malignant melanoma, malignant peripheral nerve sheath tumor (PNST), fibrosarcoma, and undifferentiated pleomorphic sarcoma (UPS). To identify the origin of the tumor cells, we performed a series of IHC stains (Table 1). Sections were counterstained with Mayer hematoxylin. 15 Blood vessels in the tumor sections served as the internal positive control for α–smooth muscle actin (α-SMA). Homologous non-immune sera replaced corresponding primary antibodies as negative controls. 15
Immunohistochemical staining results for an invasive spindle-cell rhabdomyosarcoma with osteolysis in a dog.
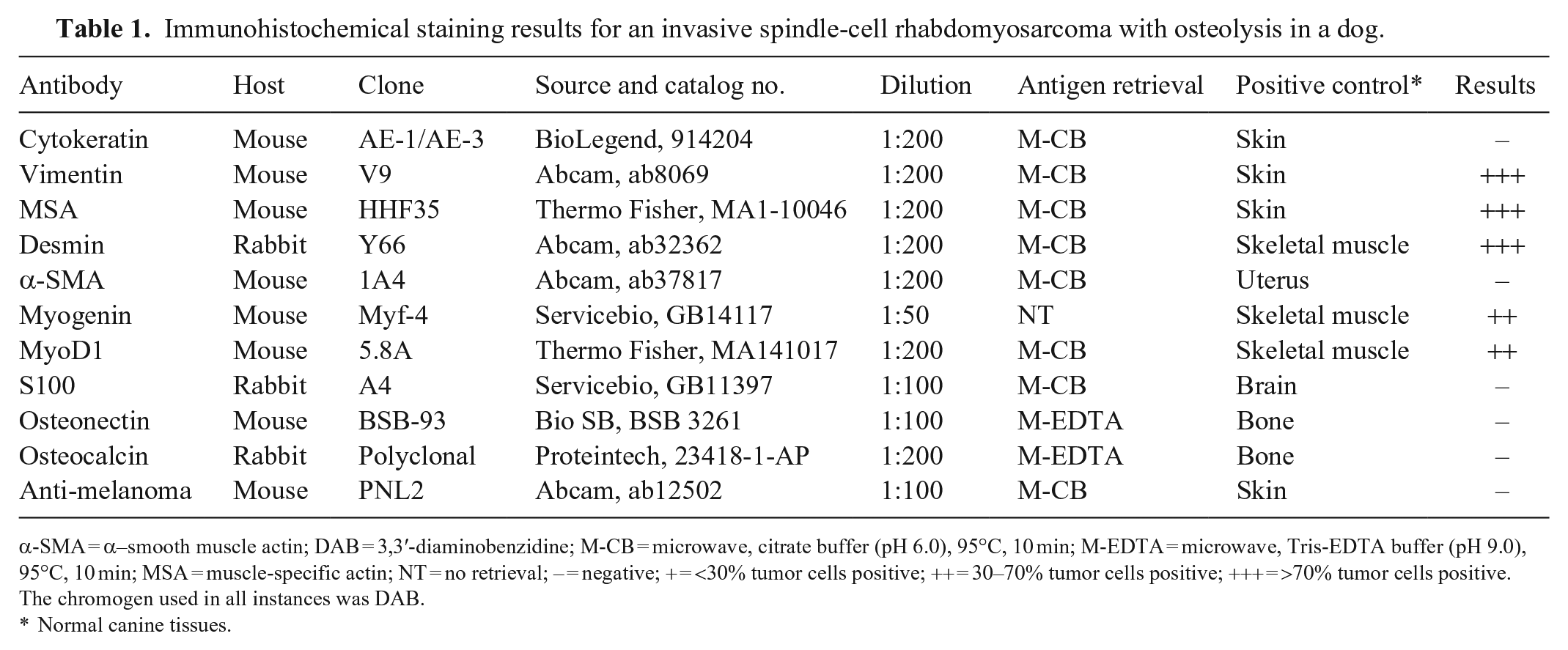
α-SMA = α–smooth muscle actin; DAB = 3,3′-diaminobenzidine; M-CB = microwave, citrate buffer (pH 6.0), 95°C, 10 min; M-EDTA = microwave, Tris-EDTA buffer (pH 9.0), 95°C, 10 min; MSA = muscle-specific actin; NT = no retrieval; – = negative; + = <30% tumor cells positive; ++ = 30–70% tumor cells positive; +++ = >70% tumor cells positive. The chromogen used in all instances was DAB.
Normal canine tissues.
Immunohistochemically, tumor cells were negative for cytokeratin (Table 1) and had strong cytoplasmic staining for vimentin in 90–95% of the tumor area (Fig. 2A), suggesting that the tumor cells originated from mesenchyme, thus excluding spindle-cell carcinoma. Most (~95%) of the tumor cells had diffuse cytoplasmic staining for muscle-specific actin (MSA; Fig. 2B), indicating that the tumor cells were of muscle cell origin; thus, fibrosarcoma was ruled out. Most (~90%) of the tumor cells had diffuse cytoplasmic staining for desmin (Fig. 2C); 60–70% of the tumor cells had moderate-to-strong nuclear staining for myogenin (Fig. 2D) and myoD1 (Fig. 2E); and all tumor cells were negative for α-SMA (Fig. 2F), indicating that the tumor cells were of skeletal muscle cell origin; leiomyosarcoma and UPS were excluded. Osteosarcoma and chondrosarcoma were excluded given that the tumor cells were immunonegative for osteonectin and osteocalcin (Table 1), and no chondroid or cartilage production was detected in the spindle-cell tumor areas. 19 All tumor cells were negative for S100 and anti-melanoma antibody (Table 1), which ruled out PNST and spindle-cell malignant melanoma.
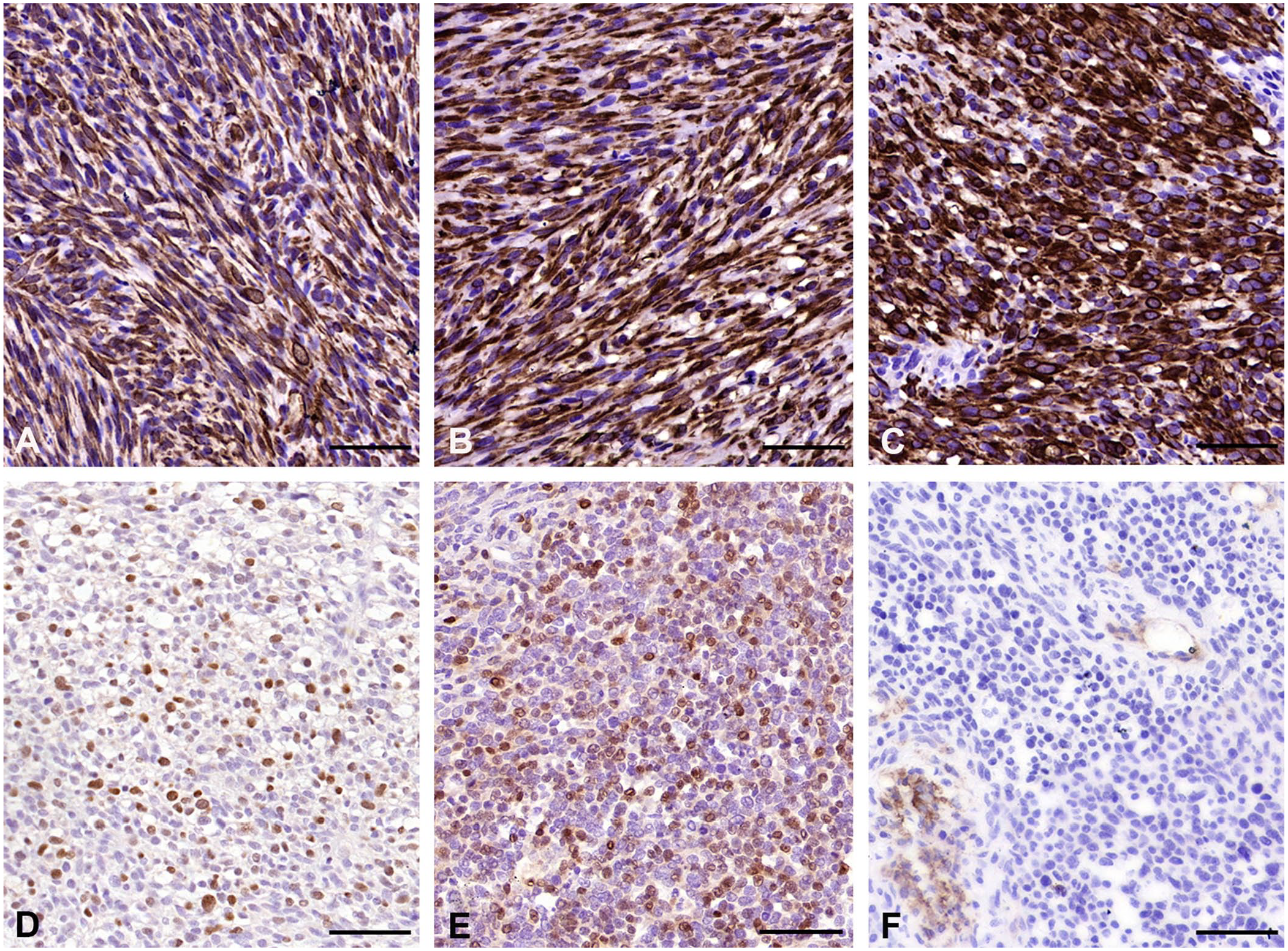
Immunohistochemical characteristics of invasive spindle-cell rhabdomyosarcoma with osteolysis in a dog. Chromogen: 3,3′-diaminobenzidine. Mayer hematoxylin counterstain. Bars = 50 µm.
According to the above radiographic features, gross appearance, and histologic and IHC results, we diagnosed this case as an invasive SCRMS with severe osteolysis. However, the origin of the tumor cells was not clear; we speculated that the cells may have originated from skeletal muscle in the deep dermis and subcutis or from a primary osseous RMS. 8 Only a few cases of primary RMS of bone have been reported in humans and none in dogs. 8 Intraosseous RMS in humans appears to be associated with specific gene fusions, and it is unclear whether bone RMS is a primary tumor or represents osteosarcoma with RMS differentiation. Therefore, despite the low prevalence of RMS in dogs, we suggest that RMS be considered in the differential diagnosis of cutaneous and subcutaneous masses with osteolysis. 5
In veterinary medicine, botryoid RMS is the most frequent type of canine RMS (43%), followed by embryonal RMS (23%), alveolar RMS (11%), and pleomorphic RMS (3%). 3 Depending on the histologic subtype of RMS, RMS is locally invasive, with potential to metastasize to the lungs, lymph nodes, and other sites.12,16 The histogenesis of RMS in different histologic subtypes may be different, and there are several hypotheses that have been proposed, including development from pluripotent stem cells or mesenchymal progenitor cells. 7
SCRMS, also known as leiomyomatous RMS, is a rare variant of embryonal RMS in both humans and animals. SCRMS, which was first reported in 1992 in a group of 21 children, had good biologic behavior and clinical prognosis compared to other subtypes of RMS. 4 In humans, this tumor is most common in the paratesticular area, and this might account for the good prognosis in these patients. 9 However, some reports indicate that a more aggressive clinical course with early disease death may be anticipated in SCRMS in adults. 13 In addition, tumor location is a prognostic factor; tumors occurring in the CNS may be linked to a poor prognosis. 5 In dogs, only a few cases of SCRMS have been reported, and the prognostic factors are poorly studied. 3 The most frequently affected areas of RMS in dogs are the urogenital tract (49%), followed by the head, neck, and face (37%), and limbs (8%).3,12
IHC stains are extremely useful in differentiating SCRMS from other spindle-cell sarcomas. 3 Given their similar morphologic characteristics and immunologic profiles, differential diagnosis of leiomyosarcoma and SCRMS remains challenging. RMS is diagnosed in both humans and dogs based on immunopositivity of muscle-specific markers, as well as by additional immunomarkers, such as myogenin and myoD1, which are sensitive and specific for skeletal muscle differentiation.3,18 In our case, the positive staining for MSA, desmin, myogenin, and myoD1, and negative staining for α-SMA led us to the diagnosis of SCRMS. In addition, transmission electron microscopy is considered the gold standard for the diagnosis of RMS, but it is not widely available for use in routine diagnosis in veterinary medicine.3,17,18 In our case, the bone trabeculae, cartilaginous matrix, and new bone formation in the areas of osteolysis mimicked primary bone tumors. Although osteosarcoma was considered as a diagnosis, given the negative osteocalcin and osteonectin in the spindle cell areas of the tumor and the presence of a fracture radiographically, the bone and cartilage formation were most likely secondary to fracture healing.
We diagnosed SCRMS based on IHC (myogenin and myoD1 positive) and histologic findings (highly cellular proliferation of spindle cells arranged in intersecting fascicles). Tumor cells, which infiltrated the deep muscle layer and invaded bone tissue, had a highly invasive growth pattern, but this dog was alive without any evidence of local recurrence or distant metastasis 18 mo post-surgery. Prognostic factors for different subtypes of canine RMS remain to be investigated.
Footnotes
Acknowledgements
We thank Dr. Chen-Hsuan Liu, School of Veterinary Medicine, National Taiwan University for his technical guidance and advice on diagnosis.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.