
Abstract
A 7-y-old male Labrador Retriever dog was presented because of acute onset of dark-colored urine after a hunting session the day prior. Moderate hemoglobinemia was observed, associated with transient hemoglobinuria and hematuria with no concurrent evidence of underlying urinary tract disease. The patient’s clinical signs resolved within 36 h post-exercise without specific treatment. The concurrent occurrence of exertional hemolysis and hematuria in a dog is uncommon; these conditions are commonly reported separately in human athletes.
Hemolysis following physical activity has been studied extensively in human medicine. It is described as mild, self-limiting RBC destruction following exercise of variable intensity. 16 A combination of mechanical21,27 and metabolic4,29 insults to erythrocytes during exercise is suspected to exacerbate their fragility, leading to hemolysis. Limited data exist in the veterinary literature regarding exertional hemolysis. This phenomenon has been reported in Standardbred horses during racing events, 19 and in phosphofructokinase (PFK)-deficient English Springer Spaniel dogs. 24
Transient macroscopic hematuria can also be seen after strenuous exercise in people 12 and exercising horses. 23 In this condition, direct mechanical injury to the bladder wall as well as renal injury secondary to internal movement, vascular spasm, and ischemia during exercise are suspected to promote the passage of RBCs into the urine.3,10 We describe here both transient hemolysis and macroscopic hematuria occurring simultaneously in a dog following a hunting session.
A 7-y-old, intact male Labrador Retriever weighing 31.6 kg was presented to the University of California–Davis, Veterinary Medical Teaching Hospital because of “urinating blood” in the absence of stranguria, pollakiuria, dysuria, or other obvious lower urinary tract signs. The day prior, the dog had been hunting and was reportedly running all day. Physical examination revealed adequate hydration by skin turgor and mucous membrane evaluation, normal vital signs, and a mildly stiff gait on all 4 limbs. Examination was otherwise normal.
CBC (Advia 2120; Siemens) showed mild mature neutrophilia (17.2 × 109/L; RI: 3.0–10.5 × 109/L) and mild lymphopenia (0.9 × 109/L; RI: 1.0–4.0 × 109 cell/L). The hematocrit and platelet count were within RIs. Evaluation of the blood smear showed RBC morphology changes such as polychromasia, rare blister cells, eccentrocytes, and a few echinocytes and acanthocytes. A serum biochemistry panel (Cobas c501; Roche) revealed mild hyperproteinemia (71 g/L; RI: 54–69 g/L) as a result of mild hyperalbuminemia (44 g/L; RI: 34–43 g/L), increased activity of creatine kinase (CK; 1,693 U/L, RI: 55–257 U/L) and aspartate aminotransferase (AST; 224 U/L, RI: 20–49 U/L), and mild hyperbilirubinemia (17.1 μmol/L; RI: ≤3.4 μmol/L). The laboratory reported “moderate plasma hemolysis” for the plasma appearance. Analysis of a free-catch urine sample showed coffee grounds–colored urine with USG of 1.037 and marked hematuria with too-numerous-to-count RBCs/hpf on microscopic sediment evaluation (Fig. 1A). Colorimetric chemistry testing using urine test strips (Chemstrips 10UA, Cobas c411 urine analyzer; Roche) for evaluation of glucose, protein, ketones, bilirubin, pH, and heme positivity in urine could not be performed given the marked sample pigmentation, even when attempting to use the supernatant. The cellular fraction of the urine was green (Fig. 1B); the supernatant was the color of coffee grounds. There was no associated pyuria, and the urine was negative for myoglobin upon an ammonium sulfate precipitation test (Cobas c501). The patient was discharged for monitoring at home, and a re-check appointment was scheduled through our hospital for the following day.
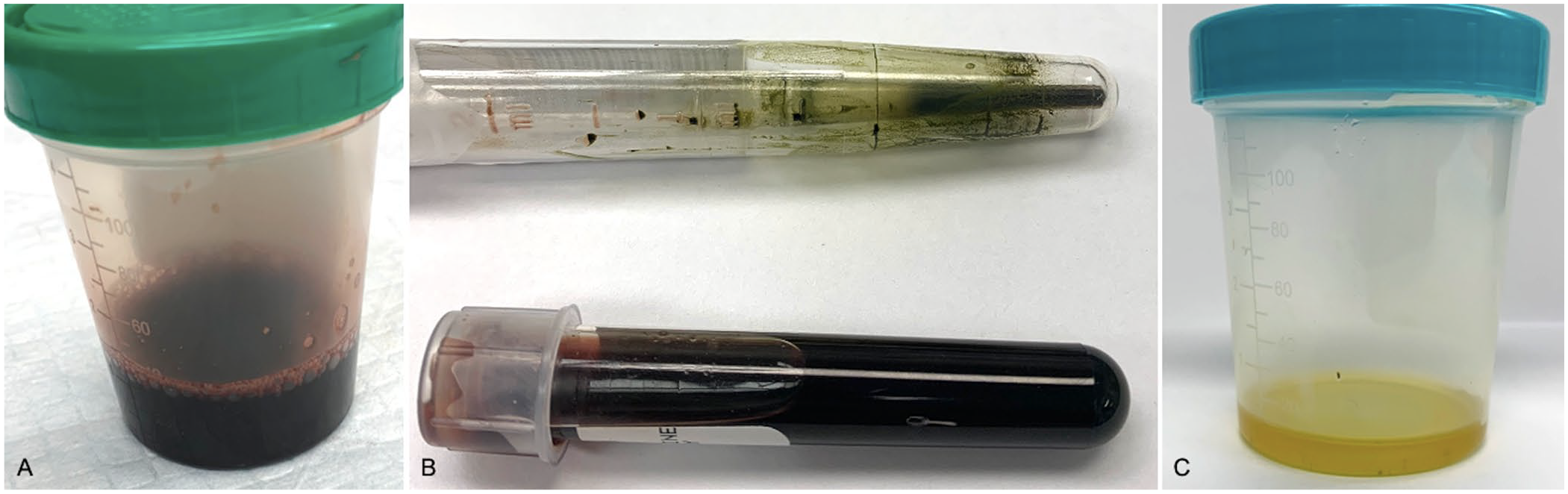
Exertional hemolysis and hematuria in a 7-y-old Labrador Retriever dog.
On the day 2 re-check examination at our hospital, the owner reported resolution of the pigmenturia (Fig. 1C). A repeat serum biochemistry panel showed improved AST activity of 98 U/L and a total bilirubin concentration within the RI. A new free-catch urine sample was yellow and somewhat cloudy, with USG of 1.034, pH of 6, 3+ proteinuria, 1+ bilirubinuria, and 3+ heme positivity. Microscopic evaluation of the sample sediment revealed rare bilirubin crystals, rare clumps of RBCs, and no other relevant findings. The patient was sent home for continued monitoring and re-checked again on day 3 at our hospital. The owner reported no abnormality in the dog’s urination. The physical examination was unremarkable. The patient was sedated with 150 μg of intravenous dexmedetomidine (Dexdomitor; Zoetis) and 7 mg of butorphanol tartrate (Torbugesic; Zoetis) for abdominal ultrasonography (Aplio i700; Canon). An incompletely filled urinary bladder with diffuse thickening of the urinary bladder wall was noted. The remainder of the ultrasonographic examination was within normal limits. The patient was homozygous normal for PFK and pyruvate kinase (PennGen Laboratories). The owner was instructed to restrict the dog from strenuous activity.
Over the following 9 mo, the dog was appropriately exercise-restricted, and no further episodes were witnessed. Upon routine re-check examination through our hospital, the physical examination was unremarkable except for marked excitement. No abnormalities were found on serum biochemistry panel or CBC. A free-catch urine sample had no gross abnormalities, hypersthenuria of USG 1.041, trace ketonuria in the absence of glucosuria, trace heme positivity, and 2+ proteinuria. The microscopic sediment examination revealed minimal-to-irrelevant hematuria (3–5 RBCs/hpf) and a few struvite crystals. There was no myoglobinuria. Abdominal ultrasonography showed changes consistent with prostatic hyperplasia with an unremarkable urinary tract. Minimum and maximum hemolysis occurred at 85% and 45% dilutions, respectively, in an RBC osmotic fragility test,5,9 which was consistent with increased osmotic fragility. 17
Exertional hemolysis is a frequent phenomenon in human athletes and was first reported in 1884. 13 Previously called foot-strike hemolysis, which implied direct mechanical trauma to the erythrocytes from repeated ground impact during running, 27 there is now evidence to suggest that exercise-induced hemolysis is multifactorial and may involve other mechanical factors, such as RBC compression at other anatomical sites as well as metabolic factors. During strenuous exercise, redistribution of blood flow to exercising muscles causes profound vasoconstriction in internal organs 11 resulting in direct RBC compression in small arteries. RBC compression within the muscular capillary beds during powerful contractions may also contribute to hemolysis. 16 Metabolic stressors associated with exercise, including dehydration, 22 lactic acidosis, 14 hyperthermia, 20 increased catecholamine concentrations, 28 regional hypoxia, 18 and oxidative damage 26 among others, are suspected to promote osmotic fragility and alter the RBC membrane structure and deformability, increasing the likelihood of hemolysis.
Exertional hemolysis could be worsened in a patient with preexisting RBC membrane mutations, 15 and has been reported following strenuous exercise in 2 English Springer Spaniel dogs with PFK deficiency. 24 In those 2 dogs, the authors hypothesized that transient hyperthermia and alkalosis, along with the increased temperature-dependent alkaline fragility of PFK-deficient RBCs, may have led to hemolysis. Exertional hemolysis in veterinary medicine was also suspected in a study of 15 Standardbred horses, as witnessed by a transient increase in free plasma hemoglobin 5 min after a 1.6 km (1 mi) race, which returned to baseline the following day. 19
To our knowledge, exertional hemolysis has not been reported previously in a dog without PFK or pyruvate kinase deficiency. The cause of increased osmotic fragility noted in our patient remains unclear and could be related to an undiagnosed spectrin deficiency 25 or hereditary stomatocytosis, 6 either of which could have exacerbated hemolysis secondary to exercise. Similar to reports in people, in whom hemolysis resolves within 24–48 h, 15 our patient’s hemolysis was mild and improved without specific intervention within 36 h following exercise.
Another unique aspect of our case is the concurrent development of exertional hematuria. Exertional hematuria was first reported in people in 1910 and was later defined as microscopic and macroscopic hematuria developing after a session of strenuous exercise in subjects without evidence of kidney or other urinary tract disease that resolves with rest, typically within 2–72 h following exercise.2,12,16 The exact mechanism of hematuria following exercise is not understood completely. A component of internal trauma to the urinary tract is suspected, as witnessed by the presence of hemorrhage at the bladder neck and posterior urethra in human male runners secondary to repeated impact, particularly if strenuous exercise is undertaken with an empty urinary bladder. 10 Other proposed mechanisms involve kidney trauma secondary to up-and-down movements, vascular spasms, and ischemia, and are suspected to result in altered glomerular permeability and subsequent passage of RBCs into the urine. 3
In veterinary medicine, transient exertional hematuria has been described in 8 mares performing treadmill exercise of various intensities. 23 At high-intensity exercise, macroscopic hematuria was detected in all 8 horses and resolved within 10 min of the recovery period, whereas microscopic hematuria was noted in most of them at lower intensity exercise and was still present at the final urine evaluation 2 h following exercise. Our dog did not appear to have underlying urinary tract disease, nor was there any known external trauma. The gross color of its urine was attributed to the RBCs observed on cytology in combination with suspected bilirubinuria (given the presence of green pigment in the cellular fraction, suspected to be biliverdin) and hemoglobinuria, given the presence of intravascular hemolysis and the coffee grounds color of the supernatant in the absence of evidence of myoglobinuria. Even though coffee grounds urine discoloration is often seen with cases of myoglobinuria, the degree of elevation in serum CK activity (interpreted as relatively mild) and lack of other consistent clinical evidence made extensive myocyte injury a less likely explanation for the overt pigmenturia. Nevertheless, the ammonium sulfate test is not considered to be completely reliable. Denatured myoglobin can precipitate in an 80% ammonium sulfate solution, and similar misclassifications might occur when pH is not adjusted.1,7 Hence, immunochemical methods are usually necessary to rule out myoglobinuria fully, 8 which is a limitation of our report. The diffuse thickening of the bladder wall noted ultrasonographically 72 h following exercise could have been secondary to the small size of the bladder, given the absence of pyuria. As reported in people and horses, our dog’s macroscopic hematuria was transient (<36 h) and not associated with clinical changes in renal function.
Considering the excellent outcome reported in human medicine and in our case, clinicians should include exercise-induced changes as a differential for transient hematuria and hemolysis in applicable cases.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.