
Abstract
Fecal canine alpha1-proteinase inhibitor (cα1-PI) concentration has been reported to be increased in dogs with protein-losing enteropathy due to the loss of cα1-PI into the gastrointestinal tract. A chronic loss of cα1-PI may theoretically deplete serum cα1-PI, potentially altering the proteinase-to-proteinase inhibitor balance. Protein-losing enteropathy has been reported to occur frequently in certain dog breeds such as Yorkshire Terriers and to be associated with hypocobalaminemia. The objective was to compare serum cα1-PI concentrations in Yorkshire Terriers with and without cobalamin (COB) deficiency. Serum samples from 52 COB-deficient and 69 normocobalaminemic Yorkshire Terriers, which had been submitted to the Gastrointestinal Laboratory (2008–2011; College Station, TX), were included retrospectively. Serum cα1-PI concentrations were measured using an in-house radioimmunoassay and compared between Yorkshire Terriers with and without COB deficiency using a Mann–Whitney U test. A Fisher exact test was used to evaluate whether a decreased serum cα1-PI concentration is associated with COB deficiency in Yorkshire Terriers. Serum cα1-PI concentrations were significantly lower in COB-deficient Yorkshire Terriers (median: 1,016 mg/l, range: 315–3,945 mg/l) than in normocobalaminemic Yorkshire Terriers (median: 1,665 mg/l, range: 900–2,970 mg/l; P < 0.0001). One-fourth (n = 13) of the COB-deficient Yorkshire Terriers had a serum cα1-PI concentration below the lower limit of the reference interval (<732 mg/l), and COB deficiency was associated with decreased serum cα1-PI concentrations (P < 0.0001). In the current study, serum cα1-PI concentrations are significantly lower in COB-deficient Yorkshire Terriers when compared to normocobalaminemic Yorkshire Terriers. Further studies are needed to determine the functional and potential prognostic implications of serum cα1-PI concentrations in dogs with gastrointestinal disease.
Keywords
Protein-losing enteropathy (PLE) is a chronic gastrointestinal disease associated with excessive loss of plasma proteins into the gastrointestinal (GI) tract as well as malabsorption of proteins and other nutrients.5,20 Important causes of PLE are altered lymphatic drainage (e.g., intestinal lymphangiectasia) or increased mucosal permeability (e.g., inflammatory bowel disease [IBD] or lymphoma).5,20
A primary (idiopathic) form of intestinal lymphangiectasia has been reported in Yorkshire Terriers, Chinese Shar-Peis (Shar-Peis), and Rottweilers.14,15,20 Secondary intestinal lymphangiectasia has been described with mucosal infiltration in IBD, intestinal neoplasia, and/or infectious diseases in dogs12,16 and certain dog breeds such as Basenjis,18,20 German Shepherd Dogs (GSDs), 1 Shar-Peis,2,20 and Soft Coated Wheaten Terriers have been reported to be predisposed.17,20 However, it is often challenging to differentiate primary and secondary intestinal lymphangiectasia because intestinal inflammation may develop secondary to lymphangiectasia and obscure or even exacerbate the primary GI disease process.
PLE has been reported to occur frequently in certain dog breeds such as the Yorkshire Terrier.13,15,20 Clinical signs observed in Yorkshire Terriers with PLE include diarrhea, vomiting, weight loss, and ascites, and resemble signs present in dogs with PLE belonging to other dog breeds.5,20 However, some clinical features, such as bicavitary effusion14,24 (Craven M, Duhamel GE, Sutter NB, et al.: 2009, Absence of bacterial association in Yorkshire terriers with protein-losing enteropathy and cystic intestinal crypts. J Vet Intern Med 23:757. Abstract) or chylothorax 6 and intestinal crypts lesions15,20,25 are observed more often in Yorkshire Terriers with PLE than in dogs with PLE of other breeds. The exact pathogenesis of PLE in the Yorkshire Terrier is unknown.
The histologic features in biopsies from dogs with IBD and/or intestinal lymphangiectasia can vary between duodenal and ileal samples.3,5 In some dogs, intestinal lymphangiectasia can only be seen in the ileum. 5 Cobalamin (COB) absorption occurs exclusively in the ileum of dogs. Hypocobalaminemia and hypoalbuminemia can occur concurrently, and both have been shown to be associated with chronic GI diseases (e.g., PLE and IBD) in dogs. 1 However, to the authors’ knowledge, serum albumin and fecal and/or serum canine alpha1-proteinase inhibitor (cα1-PI)9,10 have not yet been reported in COB-deficient dogs of breeds frequently diagnosed with PLE (e.g., Yorkshire Terriers).
Measurement of serum albumin and fecal cα1-PI concentrations have been recommended for the diagnosis of dogs with suspected PLE,5,20 as PLE is associated with increased loss of cα1-PI into the GI tract and fecal cα1-PI concentrations have been shown to be increased in dogs with PLE. 19 Theoretically, chronic loss of cα1-PI may deplete serum cα1-PI, potentially altering the proteinase-to-proteinase inhibitor balance.10,23 Furthermore, serum cα1-PI concentrations are regulated within a narrow concentration range in healthy dogs 10 and have been reported to be decreased in a subset of dogs with IBD and/or PLE (Equilino M, Théodoloz V, Doherr M, et al.: 2011, Biochemical markers and survival in dogs with protein-losing enteropathy. J Vet Intern Med 25: 691–692. Abstract). Serum cα1-PI concentrations may allow further characterization of GI diseases such as PLE and IBD. Therefore, the aim of the current study was to compare serum cα1-PI concentrations in COB-deficient Yorkshire Terriers and normocobalaminemic Yorkshire Terriers. It was hypothesized that serum cα1-PI concentrations are decreased in COB-deficient Yorkshire Terriers and that a decreased serum cα1-PI concentration reflects more severe clinical disease.
Materials and methods
Sample population
Database information on canine serum samples from Yorkshire Terriers, submitted to the Gastrointestinal Laboratory (GI Lab) at Texas A&M University (College Station, TX) between December 1, 2008, and December 1, 2011, was retrospectively reviewed. Canine serum samples were generally submitted by primary care veterinarians to the GI Lab for evaluation of GI function.
Yorkshire Terriers
Serum samples from 121 Yorkshire Terriers were included. Serum COB concentrations (reference interval [RI]: 251–908 ng/l)a had been measured using an automated chemiluminescence assay.b Serum cα1-PI concentrations (RI: 732–1,802 mg/l) were measured using an in-house radioimmunoassay. 10 Concentrations of serum albumin (RI: 2.4–4.5 g/dl) and serum creatinine (RI: 0.5–1.4 mg/dl) were measured using a chemistry analyzer.c
Because the canine serum samples had been submitted to the GI Lab for evaluation of GI function, results of routinely conducted serum tests to assess GI health, such as folate measured by an automated chemiluminescence assay (RI: 7.7–24.4 μg/l),d canine trypsin-like immunoreactivity (cTLI) using a commercially available radioimmunoassay (RI: 5.7–45.2 μg/l),d and canine pancreatic lipase immunoreactivity (cPLI) using the specific pancreatic lipase immunoassay (RI: 0–200 μg/l),d were also available.
For additional information about the clinical signs of the dogs at the time of sample submission, a standard questionnaire was sent to the primary care veterinarians. However, because the serum samples from some Yorkshire Terriers had been submitted via a reference laboratory, it was not possible to obtain additional information for all Yorkshire Terriers. Questionnaires for 15 (28.8%) COB-deficient and 24 (34.8%) normocobalaminemic Yorkshire Terriers were completed and returned by primary care veterinarians.
Cobalamin-deficient dogs of 6 other breeds
In addition, serum samples from 253 dogs (GSD, Labrador Retriever [Labrador], Shar-Pei, Boxer, Cocker Spaniel, and Beagle; Table 1) with undetectable serum COB concentrations from a previous study evaluating COB deficiency in Shar-Peis and dogs of 6 other breeds 8 were used to compare serum cα1-PI concentrations in COB-deficient Yorkshire Terriers and COB-deficient dogs of 6 other breeds. Also, serum albumin concentrations were measured using a chemistry analyzerc (as described above) to compare and correlate serum cα1-PI concentrations in COB-deficient Yorkshire Terriers and COB-deficient dogs of 6 other breeds. Serum samples from only those dogs were included where a sufficient amount of serum was available to measure serum concentrations of cα1-PI and albumin.
Patient demographics of all dogs that were enrolled in the current study.*
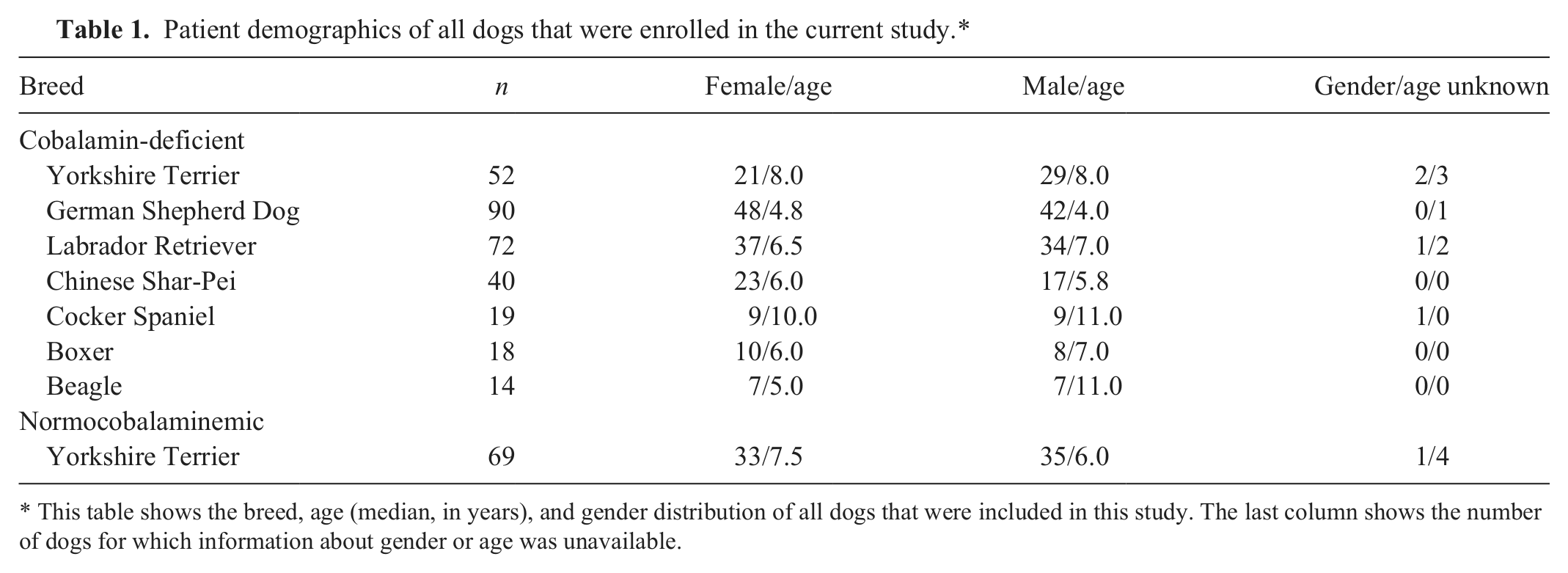
This table shows the breed, age (median, in years), and gender distribution of all dogs that were included in this study. The last column shows the number of dogs for which information about gender or age was unavailable.
Statistical analyses
A commercially available software packagee was used to perform all statistical analyses. A Mann–Whitney U test was used to compare age, serum cα1-PI concentrations, serum albumin and creatinine concentrations, GI function tests (i.e., serum folate, cTLI, and cPLI concentrations), and body condition score between COB-deficient Yorkshire Terriers and normocobalaminemic Yorkshire Terriers. A Fisher exact test was used to evaluate whether COB deficiency in Yorkshire Terriers is associated with decreased serum cα1-PI concentrations and decreased serum albumin concentrations. A Kruskal–Wallis test with a Dunn posttest was used to compare serum cα1-PI and serum albumin concentrations in COB-deficient Yorkshire Terriers and COB-deficient dogs of 6 other breeds. A Spearman rank sum correlation coefficient (ρ) was used to test the relationship between serum cα1-PI and serum albumin concentrations in COB-deficient Yorkshire Terriers and COB-deficient dogs of 6 other breeds. For all tests significance was set at P < 0.05.
A Fisher exact test was performed to determine whether the clinical signs are associated with COB deficiency in Yorkshire Terriers. Also, the odds ratio (OR) and the 95% confidence interval (CI) were calculated for these parameters. The cutoff for statistical significance was adjusted according to the number of clinical signs evaluated (n = 8) from P < 0.05 to P < 0.006, using a Bonferroni correction for multiple statistical comparisons.f
Results
Yorkshire Terriers
Fifty-two Yorkshire Terriers with an undetectable serum COB concentration (<150 ng/l) and 69 normocobalaminemic Yorkshire Terriers (median serum COB concentration: 615 ng/l, range: 394–906 ng/l) were identified; gender and age of the dogs from which the samples had been collected were recorded (Table 1). COB-deficient Yorkshire Terriers were significantly older (median: 8.0 years, range: 2.0–14.0 years) than normocobalaminemic Yorkshire Terriers (median: 7.0 years, range: 1.0–15.0 years; P = 0.0329; Table 1). Gender-specific differences were not identified between the 2 groups of Yorkshire Terriers (P > 0.05; Table 1).
Serum cα1-PI concentrations were significantly lower in COB-deficient Yorkshire Terriers than in normocobalaminemic Yorkshire Terriers (P < 0.0001; Fig. 1). One-fourth (n = 13) of the COB-deficient Yorkshire Terriers had serum cα1-PI concentrations below the lower limit of the RI (i.e., <732 mg/l), and COB deficiency was associated with a decreased serum cα1-PI concentration (OR: 47.5, 95% CI: 2.7–821.5; P < 0.0001; Fig. 2).
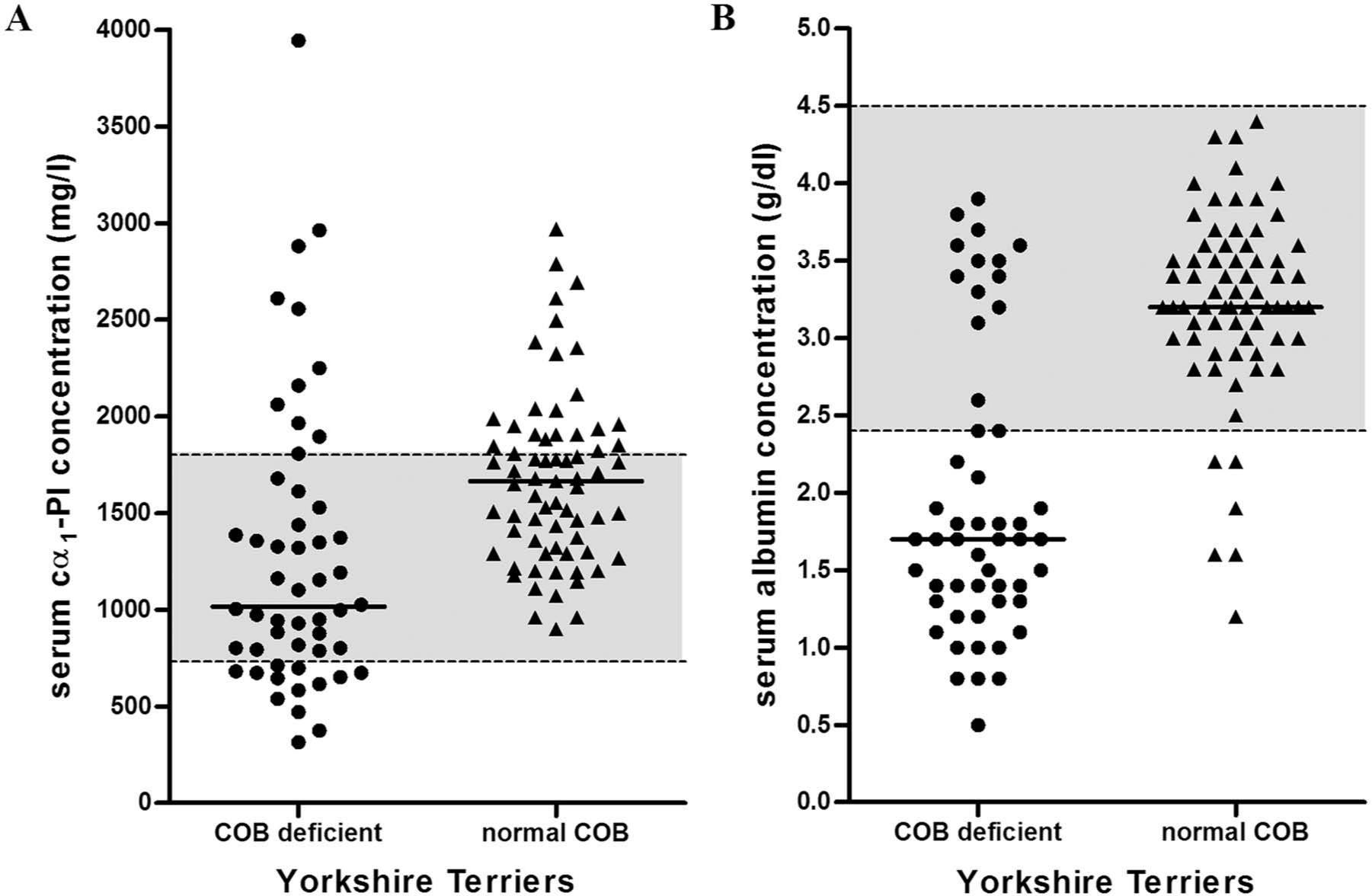
Serum canine alpha1-proteinase inhibitor (cα1-PI) and serum albumin concentrations in 52 cobalamin (COB)-deficient and 69 normocobalaminemic Yorkshire Terrier dogs.
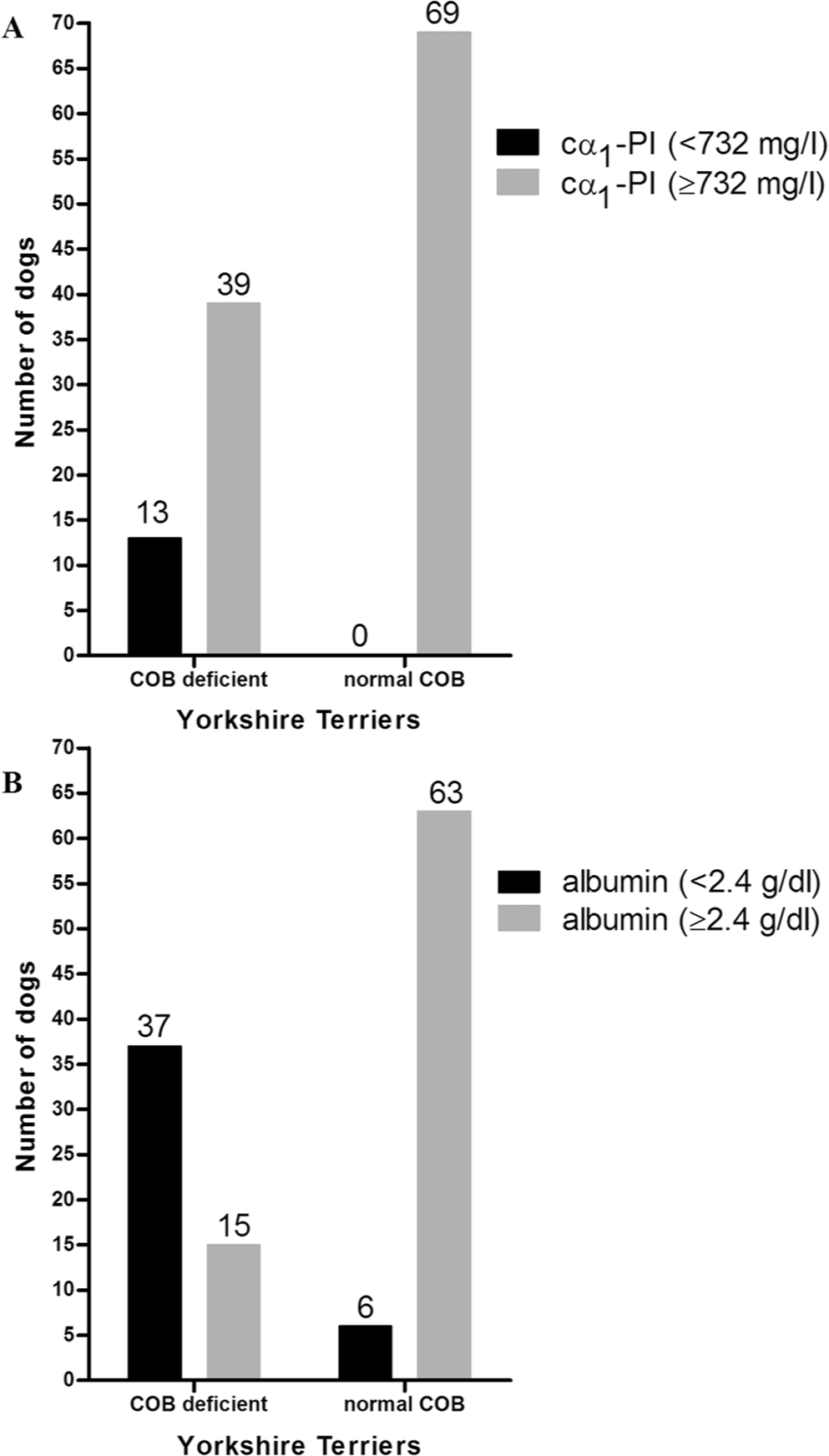
Bar graph showing the proportions of cobalamin (COB)-deficient and normocobalaminemic Yorkshire Terrier dogs with subnormal serum canine alpha1-proteinase inhibitor (cα1-PI) and serum albumin concentrations.
Serum concentrations of albumin were also significantly lower in COB-deficient Yorkshire Terriers than in normocobalaminemic Yorkshire Terriers (P < 0.0001; Fig. 1). Approximately 71% (n = 37) of the COB-deficient Yorkshire Terriers had serum albumin concentrations below the lower limit of the RI (<2.4 g/dl), and COB deficiency was associated with a decreased serum albumin concentration (OR: 25.9, 95% CI: 9.2–72.6; P < 0.0001; Fig. 2). All COB-deficient Yorkshire Terriers with a serum cα1-PI concentration <732 mg/l were also hypoalbuminemic.
Concentrations of serum creatinine were statistically significantly lower in COB-deficient Yorkshire Terriers (median: 0.6 mg/dl, range: 0.3–2.8 mg/dl) compared to normocobalaminemic Yorkshire Terriers (median: 0.8 mg/dl, range: 0.1–2.3 mg/dl; P = 0.0078). However, this difference was not considered clinically relevant because the median serum creatinine concentrations were within the RI for both groups of Yorkshire Terriers.
Serum folate concentrations were lower in COB-deficient Yorkshire Terriers (n = 52, median: 7.1 μg/l, range: 1.4–34.3 µg/l) than in normocobalaminemic Yorkshire Terriers (n = 69, median: 11.8 μg/l, range: 6.2–22.2 µg/l; P < 0.0001). No significant difference was found in serum cTLI concentrations between the 2 groups of Yorkshire Terriers (COB-deficient group: n = 47, median: 14.0 μg/l, range: 0.7–39.0 µg/l; and normocobalaminemic group: n = 67, median: 11.5 μg/l, range: 5.7–34.3 µg/l; P = 0.0534). Serum concentrations of cPLI were higher in COB-deficient Yorkshire Terriers (n = 43, median: 121 μg/l, range: 29–640 µg/l) than in normocobalaminemic Yorkshire Terriers (n = 68, median: 45 μg/l, range: 29–797 µg/l; P < 0.0001).
Information from the retrospective questionnaires revealed no differences in most clinical signs such as diarrhea, vomiting, weight loss, anorexia, respiratory signs, and abdominal distension between the 2 groups of Yorkshire Terriers (all P > 0.05; Table 2). COB-deficient Yorkshire Terriers were more commonly lethargic (n = 4, 27%) than normocobalaminemic Yorkshire Terriers (none, 0.0%; P = 0.0166; Table 3), but this difference was no longer significant after the Bonferroni correction. The body condition score (scale 1–5) was lower in COB-deficient Yorkshire Terriers (median: 2, range: 1–4, n = 15) than in normocobalaminemic Yorkshire Terriers (median: 3, range: 1–5, n = 20; P = 0.1310), but this difference did not reach statistical significance.
Clinical signs of cobalamin-deficient and normocobalaminemic Yorkshire Terrier dogs.*
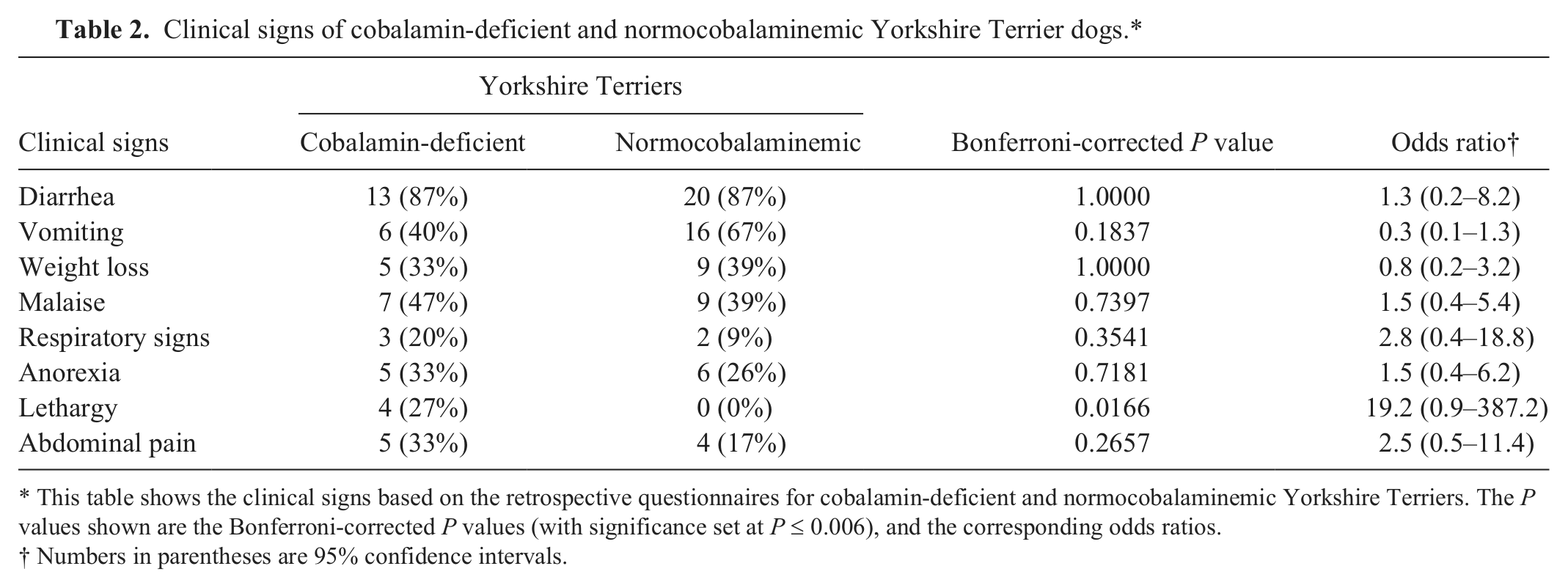
This table shows the clinical signs based on the retrospective questionnaires for cobalamin-deficient and normocobalaminemic Yorkshire Terriers. The P values shown are the Bonferroni-corrected P values (with significance set at P ≤ 0.006), and the corresponding odds ratios.
Numbers in parentheses are 95% confidence intervals.
Spearman rank sum coefficients (ρ) for the correlation between serum canine alpha1-proteinase inhibitor (cα1-PI) and serum albumin concentrations in cobalamin-deficient dogs of 7 breeds and in normocobalaminemic Yorkshire Terriers.*
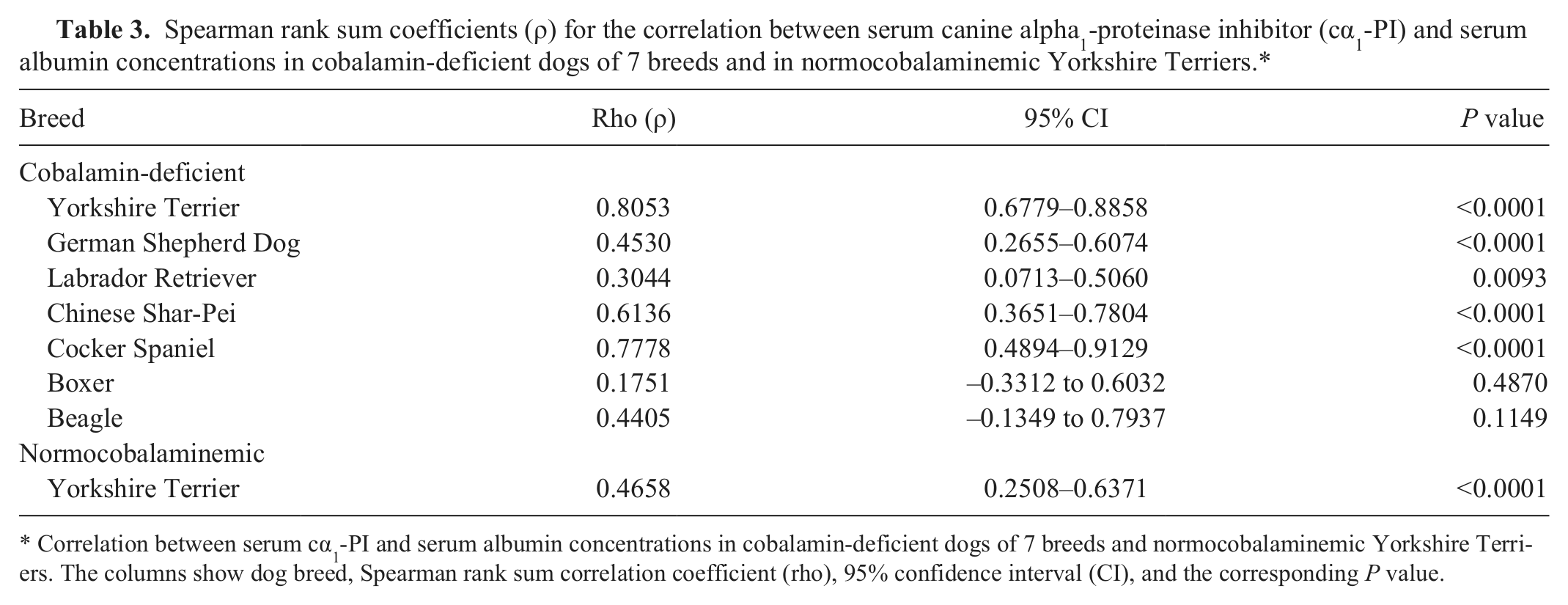
Correlation between serum cα1-PI and serum albumin concentrations in cobalamin-deficient dogs of 7 breeds and normocobalaminemic Yorkshire Terriers. The columns show dog breed, Spearman rank sum correlation coefficient (rho), 95% confidence interval (CI), and the corresponding P value.
Cobalamin-deficient dogs of 6 other breeds
Serum cα1-PI concentrations differed among the 7 breeds of COB-deficient dogs (P < 0.0001; Fig. 3). The posttest revealed that COB-deficient Yorkshire Terriers had lower serum cα1-PI concentrations than COB-deficient GSDs, Labradors, and Shar-Peis (for all: P < 0.01), and COB-deficient Cocker Spaniels had lower serum cα1-PI concentrations than COB-deficient Labradors (P < 0.01).
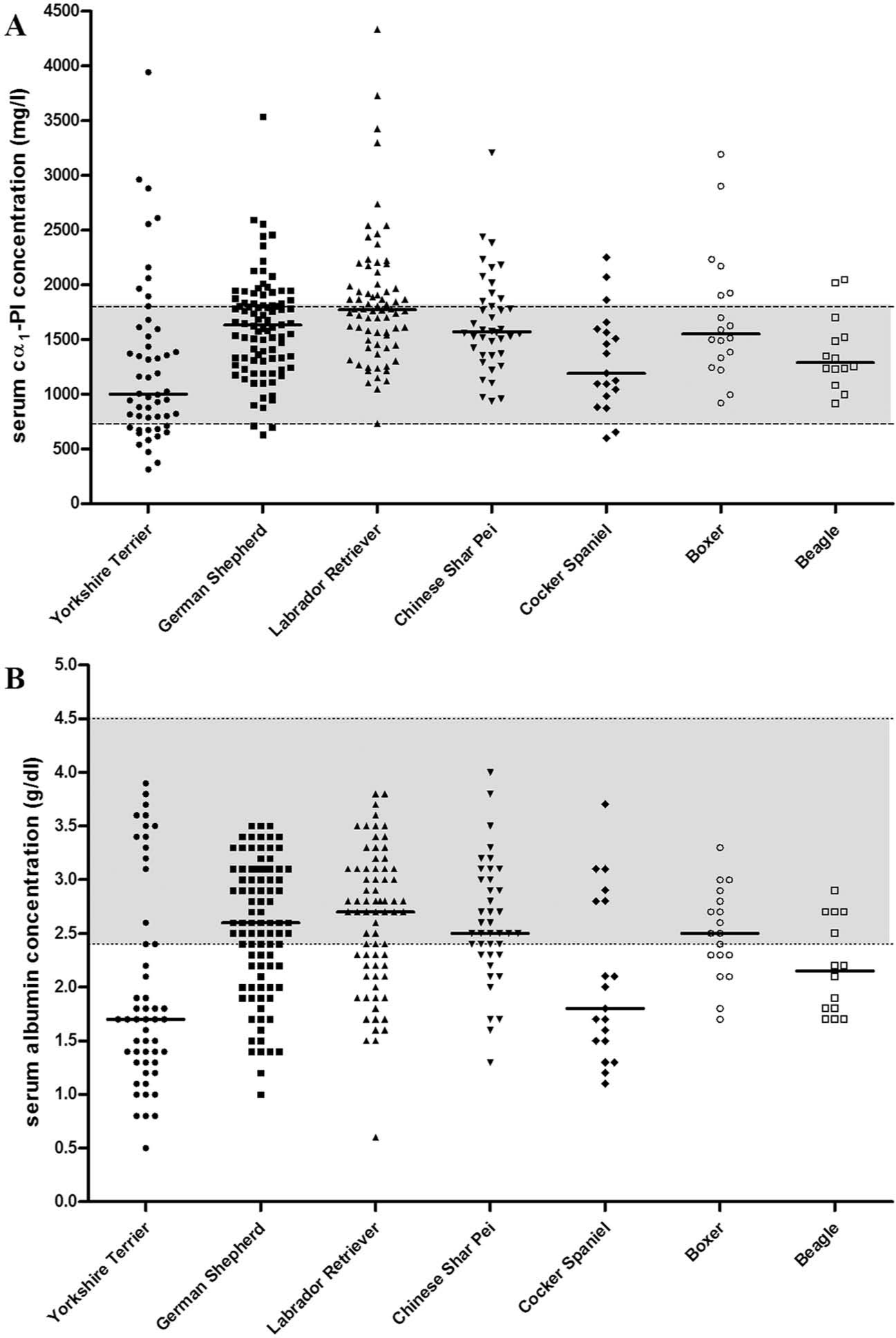
Serum canine alpha1-proteinase inhibitor (cα1-PI) and albumin concentrations in cobalamin (COB)-deficient Yorkshire Terrier dogs and COB-deficient dogs of 6 other breeds.
Similarly, serum concentrations of albumin differed among the 7 breeds of COB-deficient dogs (P < 0.0001; Fig. 3). The posttest showed that COB-deficient Yorkshire Terriers had lower serum albumin concentrations than GSDs, Labradors, and Shar-Peis (for all: P < 0.01) with an undetectable serum COB concentration, and COB-deficient Cocker Spaniels had serum albumin concentrations lower than COB-deficient Labradors (P < 0.05).
A strong correlation was observed between serum cα1-PI concentrations and serum albumin concentrations in COB-deficient Yorkshire Terriers and COB-deficient Cocker Spaniels (for both: Spearman correlation coefficient ρ ≥ 0.78; P < 0.0001; Table 2; Fig. 4). Along these lines, a moderate to weak correlation between these 2 serum proteins was observed for normocobalaminemic Yorkshire Terriers, COB-deficient GSDs, COB-deficient Labradors, and COB-deficient Shar-Peis (0.30 ≤ ρ ≤ 0.61; P < 0.01; Table 3; Fig. 4). In contrast, no correlation between serum cα1-PI and albumin was found in COB-deficient Boxers and COB-deficient Beagles (for both: P > 0.05; Table 3; Fig. 4).
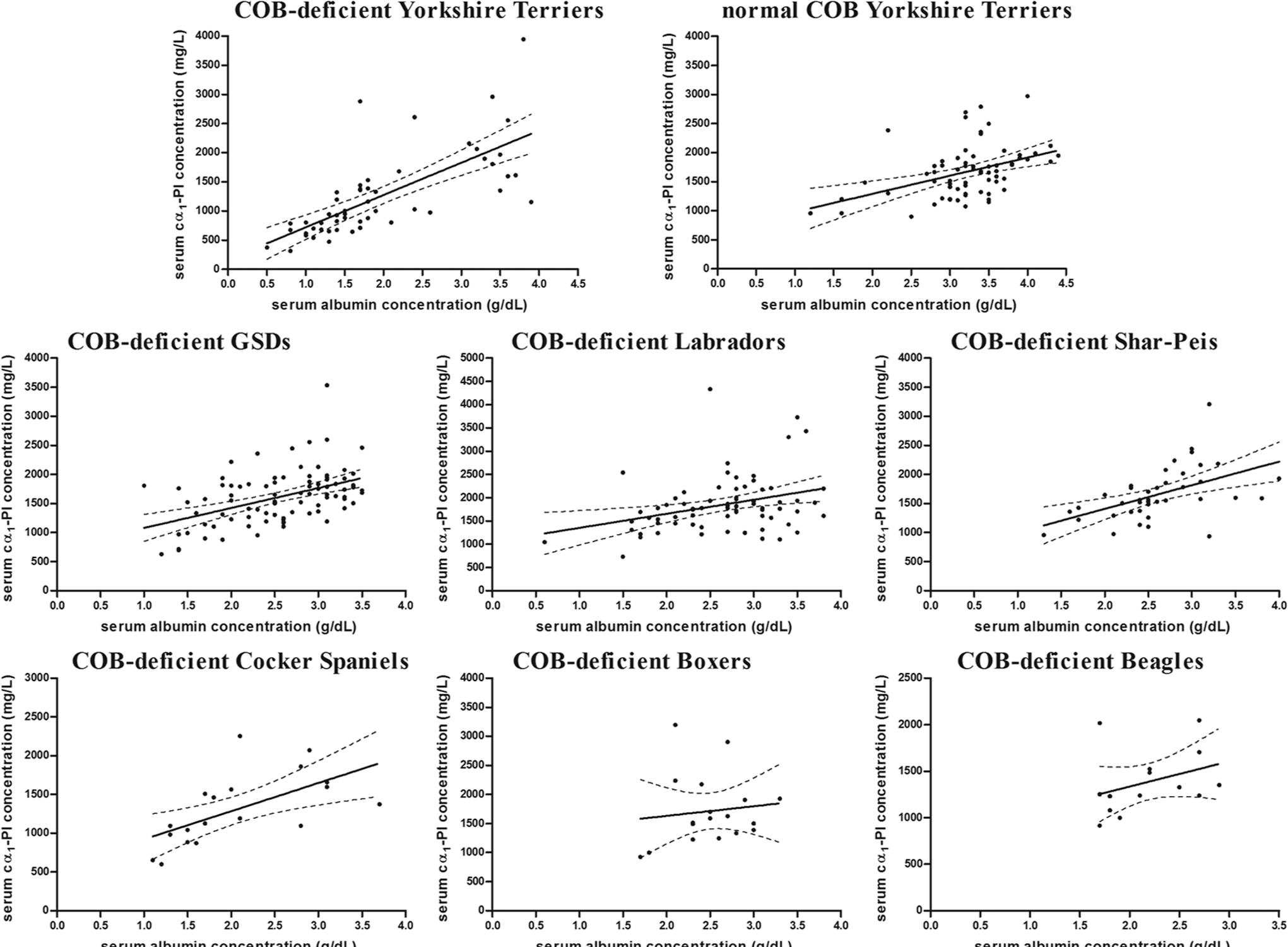
Correlation between serum canine alpha1-proteinase inhibitor (cα1-PI) and serum albumin concentrations in cobalamin (COB)-deficient dogs of 7 breeds and in normocobalaminemic (normal COB) Yorkshire Terriers. Correlation [strong, moderate, weak, none] between serum cα1-PI and serum albumin concentrations in COB-deficient Yorkshire Terriers [strong], normocobalaminemic (normal COB) Yorkshire Terriers [moderate], COB-deficient German Shepherd Dogs (GSDs) [moderate], COB-deficient Labrador Retrievers (Labradors) [weak], COB-deficient Chinese Shar-Peis (Shar Peis) [moderate], COB-deficient Cocker Spaniels [strong], COB-deficient Boxers [none], and COB-deficient Beagles [none]. The regression line (solid line) and its 95% confidence interval (dashed lines) are shown (the corresponding P values are listed in Table 3).
Discussion
In the current retrospective study, serum concentrations of cα1-PI were compared between COB-deficient and normocobalaminemic Yorkshire Terriers to evaluate the functional and potential prognostic implications of serum cα1-PI concentrations. It was found that COB-deficient Yorkshire Terriers were older than normocobalaminemic Yorkshire Terriers, while gender-specific differences were not observed. This may suggest that the disease process associated with COB deficiency in Yorkshire Terriers occurs in middle-aged to older dogs.
In the present study, it was observed that COB-deficient Yorkshire Terriers had lower serum cα1-PI and albumin concentrations than normocobalaminemic Yorkshire Terriers. Also, serum cα1-PI and serum albumin concentrations measured below the respective lower limit of the RI in approximately 25% and 71% of COB-deficient Yorkshire Terriers as opposed to 0% and approximately 9% of normocobalaminemic Yorkshire Terriers, respectively. The data revealed that COB deficiency in Yorkshire Terriers was associated with decreased serum cα1-PI and decreased serum albumin concentrations.
It has been stated that healthy dogs have a relatively narrow range of serum cα1-PI concentrations, and moderate changes (± 510.9 mg/l) in serum cα1-PI would be needed to be clinically significant. 10 In the current study, the difference in the median serum cα1-PI concentrations between COB-deficient and normocobalaminemic Yorkshire Terriers was greater than this value of 510.9 mg/l, 10 suggesting that the decrease in serum cα1-PI concentrations in Yorkshire Terriers with COB deficiency is clinically relevant.
COB (vitamin B12) deficiency in Yorkshire Terriers was associated with decreased serum cα1-PI concentrations in the present study. Diseases, such as chronic liver 22 or exocrine pancreatic diseases,21,26 could affect serum cα1-PI concentrations. For instance, the liver is the main site for synthesis of cα1-PI and is also the main storage site for COB, which could explain a massive depletion of COB from the liver together with a decreased synthesis of cα1-PI in patients with chronic hepatic disease. It would have been ideal to measure additional serum parameters (e.g., hepatic enzyme activities and the concentration of pre- and postprandial bile acids) to evaluate hepatic function, especially because COB-deficient Yorkshire Terriers were older than normocobalaminemic Yorkshire Terriers in the study and changes in hepatic structure and function may occur in older dogs. 11 Also, the increased cPLI, and numerically higher cTLI concentrations in COB-deficient Yorkshire Terriers could indicate that pancreatic disorders are associated with decreased serum cα1-PI concentrations, as shown in human patients with chronic pancreatic disease.21,26 Along these lines, pancreatic dysfunction has also been described in dogs with PLE, 13 but serum cα1-PI concentrations were significantly higher in a small number of patients (n = 24) diagnosed with pancreatitis when compared to healthy controls (unpublished data, R. M. Heilmann, 2012). Thus, further studies are needed to evaluate serum cα1-PI concentrations in dogs with exocrine pancreatic or hepatic disease.
The association between hypoalbuminemia and hypocobalaminemia is consistent with the results of studies in dogs with chronic enteropathies (e.g., IBD and PLE). 1 Fecal cα1-PI concentrations have been reported to be increased in dogs with PLE 19 ; however, serum cα1-PI concentrations in dogs with PLE and other GI diseases have not been evaluated extensively. The current breed-specific evaluation of serum cα1-PI concentrations showed that all COB-deficient Yorkshire Terriers with a serum cα1-PI concentration below the lower limit of the RI were also hypoalbuminemic. However, ruling out renal protein loss as a cause of hypoalbuminemia 4 was a limitation due to the retrospective nature of the study. Measurement of the urine protein-to-creatinine ratio would be necessary to definitively rule out protein loss due to renal disease, such as chronic kidney disease. All COB-deficient Yorkshire Terriers in the present study had serum creatinine concentrations within the RI. However, with serum being the only sample type available due to the retrospective nature of the study, only serum creatinine was able to be used to rule out advanced chronic kidney disease, which does not rule out renal protein loss. Further research is warranted to evaluate serum cα1-PI concentrations in dogs with a normal urine protein-to-creatinine ratio.
In some cases of intestinal lymphangiectasia, endoscopic and/or histologic changes can be found in the ileum but not the duodenum.3,5 The results of the current study showed that approximately half of the hypocobalaminemic Yorkshire Terriers with decreased serum cα1-PI concentrations also had a decreased serum folate concentration, which would be consistent with the assumption that intestinal lymphangiectasia can affect the small intestine diffusely or be localized to the ileum alone. Further investigations to evaluate whether endoscopic and/or histologic GI lesions in Yorkshire Terriers with COB deficiency are associated with a decreased serum cα1-PI concentration are warranted.
Because left-over serum samples were used for the current study, the clinical history and disease status remains unknown for many Yorkshire Terriers included in the study. However, a short questionnaire provided information about the disease status of a few Yorkshire Terriers with and without COB deficiency. Information obtained from the questionnaires revealed no differences between the 2 groups of Yorkshire Terriers regarding the presence of diarrhea, vomiting, weight loss, anorexia, respiratory signs, and abdominal distension. The body condition scores were lower in COB-deficient Yorkshire Terriers than in normocobalaminemic Yorkshire Terriers, although the difference did not reach statistical significance. However, using a 1–9 point scale instead of a 1–5 scale for the body condition score may have yielded a different result. Also, lethargy was the only clinical sign seen more frequently in COB-deficient Yorkshire Terriers but, after Bonferroni correction, this difference no longer reached statistical significance.
COB deficiency has been shown to be prevalent in some dog breeds predisposed to the development of specific GI diseases (e.g., Shar-Peis, Labradors, GSDs) but not in Beagles, Boxers, Cocker Spaniels, and Yorkshire Terriers. 7 Interestingly, COB-deficient Yorkshire Terriers had lower serum cα1-PI and albumin concentrations than COB-deficient GSDs, Labradors, and Shar-Peis. In contrast, serum cα1-PI and albumin concentrations did not differ between COB-deficient Yorkshire Terriers and COB-deficient Cocker Spaniels, Boxers, and Beagles (breeds that have not been previously reported as being predisposed to GI disease such as PLE). This separation based on clinicopathologic parameters may suggest that different disease mechanisms are involved in the pathogenesis of COB deficiency and/or GI disease in these breeds and may aid in further characterizing these conditions.
Breed-specific differences were observed for the relationship between serum cα1-PI and albumin. A strong correlation (as found in COB-deficient Yorkshire Terriers and Cocker Spaniels) would suggest that both cα1-PI and albumin are expressed and lost at the same rate. A weaker correlation between both protein concentrations in serum (seen in COB-deficient GSDs, Labradors, and Shar-Peis as well as in normocobalaminemic Yorkshire Terriers) or a lack of correlation (found in COB-deficient Boxers and Beagles) could be explained by differences in either their biosynthesis (e.g., inflammatory cells in the GI tract as a source of cα1-PI) or their different function (e.g., increased turnover of cα1-PI acting as a proteinase inhibitor in disease states or conditions with an increased release of proteinases). Again, these differences support the theory that breed-specific conditions can lead to COB deficiency and/or GI disease.
In conclusion, the current study found that COB-deficient Yorkshire Terriers had lower serum cα1-PI and albumin concentrations than normocobalaminemic Yorkshire Terriers, and decreased serum cα1-PI and serum albumin concentrations were associated with COB deficiency in Yorkshire Terriers. The findings of this study provide an important additional parameter for the characterization of GI disease in Yorkshire Terriers. Further studies are needed to determine whether the COB status in these dogs is always associated with PLE and to determine the functional and potential prognostic implications of serum cα1-PI concentrations in dogs with GI disease (e.g., PLE and IBD).
Footnotes
Acknowledgements
The authors are grateful to Manjusha Sala and Dr. Barbara Gastel for their critical review of this manuscript. The data in the current study was presented in part at the 2012 Annual Forum of the American College of Veterinary Internal Medicine (ACVIM), New Orleans, LA.
Notes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.