
Abstract
We used magnetic resonance imaging (MRI) to evaluate the CNS, and confirmed CNS lesions histologically, in 3 psittacine birds with neurologic signs. One bird was recumbent as a result of non-ambulatory paraparesis, and 2 birds were ataxic with impaired proprioception. In all 3 cases, imaging was performed, and infectious diseases were excluded in cases 1 and 2. In case 1, a large mass arose from the left lung; in case 2, a multinodular coelomic mass encompassed the left caudal pulmonary area to the left cranial renal pole; and in case 3, a diffuse hyperintensity affected the lumbar spinal cord. In the first 2 cases, masses invaded the vertebral canal, causing spinal cord compression. All 3 birds were euthanized given the poor prognosis, and postmortem examinations were performed. The final diagnoses were pulmonary adenocarcinoma in cases 1 and 2, and granulomatous and lymphocytic leptomeningitis caused by Mycobacterium genavense in case 3. MRI enabled visualization of the lesions in the affected area of the CNS, and MRI findings were confirmed by histopathology.
Keywords
The neurologic examination of birds is challenging because many of the tests designed to evaluate mammalian species are difficult to perform or interpret in avian species. Depending on the localization of the lesion, clinical signs of neurologic disease can vary from nonspecific signs such as apathy and anorexia, to changes in the mental status, head tilt and nystagmus, muscle tremors, seizures, blindness, ataxia, lameness, and total recumbency.3,9
In psittacine birds, the most common neurologic dysfunctions occurring in the CNS are the result of infectious diseases of various etiologies.13,15 However, other causes should also be considered, such as ingestion of toxic substances, metabolic or nutritional conditions, trauma, and congenital disorders. 13 Furthermore, neoplasia is a common finding affecting primarily the central and peripheral nervous systems, or even arising from coelomic organs and invading or compressing the spinal cord or sciatic nerves.2,13 In cases in which neoplasia affects the spinal cord or sciatic nerves, birds display unilateral or bilateral leg weakness, and slight ataxia or paralysis. Sciatic nerve compression secondary to gonad, adrenal gland, or kidney enlargement as a result of neoplasia or other conditions should be considered in the differential diagnosis. 9
Magnetic resonance imaging (MRI) is a noninvasive process that provides excellent soft tissue contrast of the CNS and spatial orientation of anatomic structures. MRI has been used increasingly in avian medicine for anatomic description of the brain 14 and also for the diagnosis of neurologic diseases. 9 We compare here MRI findings and postmortem examination in 3 psittacine birds that manifested neurologic clinical signs.
Three psittacine birds with neurologic signs were evaluated. After physical and neurologic examination, a MRI was performed. All 3 birds were premedicated with butorphanol (1 mg/kg) and meloxicam (0.5 mg/kg). Anesthesia was induced with 5% isoflurane in oxygen, administered via a facemask, followed by tracheal intubation and maintenance with 2% isoflurane in oxygen. MRI provided evidence of spinal cord abnormalities in all cases. Given the poor prognosis, all birds were euthanized with pentobarbital sodium (100 mg/kg, IV) after completing the MRI. A postmortem examination of each bird was performed. Representative tissue samples were collected from each case, fixed in 10% neutral-buffered formalin, embedded in paraffin, sectioned routinely, and stained with H&E.
Case 1
A 24-y-old male green-winged macaw (syn. red-and-green macaw; Ara chloroptera) was presented with a 5-d history of recumbency. The owner found the bird lying on the ground, and, although the bird could not stand, it was able to eat. Physical examination revealed atrophy of the pectoral muscles and body condition score of 1 of 5, with a body weight of 890 g. Neurologic examination revealed non-ambulatory spastic symmetrical paraparesis and no apparent spinal hyperesthesia. The lesion was localized to the thoracic and cranial synsacrum spinal cord segment. Whole-body radiographs revealed a soft-tissue opacity involving the left lung, which was enlarged caudally and compressed the left caudal thoracic air sac. Results of the CBC were unremarkable. An MRI was performed to confirm spinal cord involvement. A large mass arising from the left lung was confirmed, infiltrating vertebrae T5 and T6, and T7 of the synsacrum, invading the vertebral canal, and causing spinal cord compression. The mass was heterogeneously hyperintense on T2-weighted images and slightly hyperintense on T1-weighted images. These findings were compatible with pulmonary neoplasia extending to the adjacent vertebrae and vertebral canal causing spinal cord compression.
The autopsy revealed that the bird was in fairly poor body condition. The left lung was markedly enlarged with prominent white-to-yellow, ≤1-mm nodules, distributed throughout the parenchyma. The nodules adhered firmly to the adjacent thoracic spine and ribs and infiltrated the vertebral bodies and the spinal canal. Histologically, ~90% of the lung parenchyma was effaced by a multinodular, non-encapsulated, poorly demarcated, moderately cellular, and highly infiltrative epithelial neoplasm that reached and replaced several vertebral bodies and transverse processes of thoracic vertebrae, and also invaded the spinal canal, compressing the spinal cord. The cuboidal-to-columnar neoplastic cells with distinct borders grew in cords, papillae, and large densely packed nests. Anisocytosis and anisokaryosis were moderate, and there were 45 mitoses in 2.37 mm2. Neoplastic cells occasionally had small cilia at their apical pole. There were extensive areas of necrosis that underwent mineralization multifocally. The spinal cord had extensive areas of vacuolation of the parenchyma, with axonal degeneration and spheroids as a result of compression. Neoplastic cells were also present within lymphatic vessels. Immunoperoxidase (IP) staining for cytokeratin (CK) AE1/AE3 was performed with cytoplasmic immunoreaction of the neoplastic cells (Fig. 1A–C; Suppl. Fig. 1). These findings were consistent with a pulmonary carcinoma infiltrating the vertebral bones, invading the spinal canal, and compressing the spinal cord.
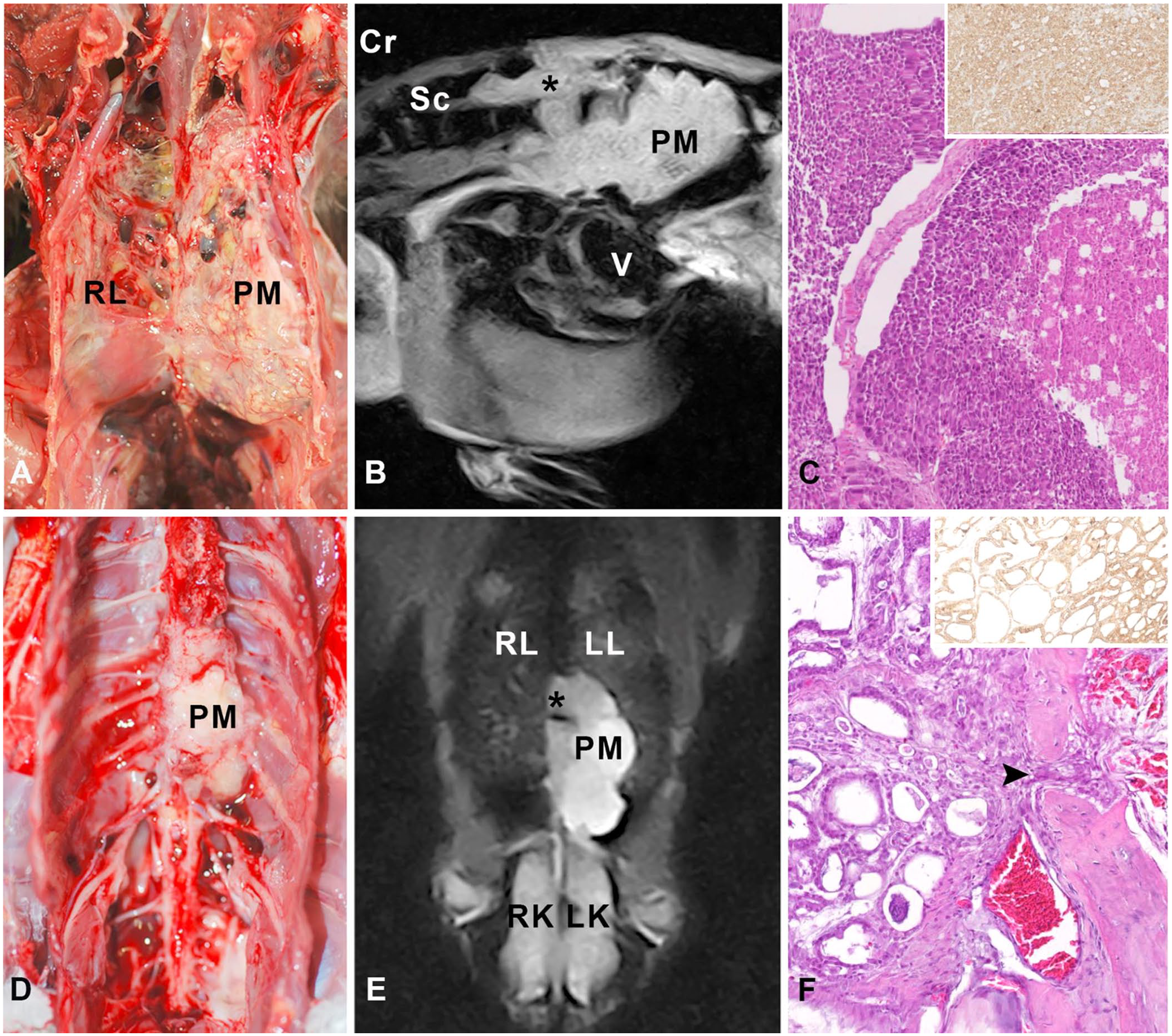
Green-winged macaw, case 1.
Case 2
A 16-y-old male African grey parrot (Psittacus erithacus) was presented with lameness of the right leg, unable to stand. Upon physical examination, the bird was bright, alert, and had good body condition (score 3 of 5; 410 g body weight). Neurologic examination revealed loss of proprioception in the left leg, reduced proprioception in the right leg, and non-ambulatory spastic paraparesis, more severe on the right side. The lesion was localized to the thoracic and cranial synsacrum segment of the spinal cord. Radiographs revealed a coelomic mass in the cranial pole area of both kidneys and a soft-tissue radiodense mass at the caudal left lung area. Results of a CBC were unremarkable. MRI was performed given the suspicion of spinal canal invasion. A large multilobulated mass was identified in the left lung also involving the cranial aspect of the left kidney, infiltrating adjacent vertebrae at the level of vertebrae T6 and T7, and T8 of the synsacrum, causing spinal cord compression. Solid and cystic areas were identified within the neoplasm. Also, round, small masses were identified, scattered throughout the parenchyma of both lungs, with heterogeneous hyperintensity in T2-weighted images and hypointensity in T1-weighted images. Contrast enhancement (gadolinium, 0.2 mL/kg) was slight and peripherally distributed in the cystic areas. These findings were compatible with pulmonary or left kidney neoplasia extending to the adjacent vertebrae and vertebral canal causing spinal cord compression.
The autopsy of case 2 confirmed that the bird was in good body condition. The most relevant finding was a white-to-yellow, highly infiltrative mass arising from the left lung, reaching adjacent thoracic vertebral bodies and rib 4, and invading, compressing, and displacing the thoracic and abdominal air sacs. Microscopically, the mass was a diffuse non-encapsulated, non-demarcated, and highly infiltrative epithelial neoplasm. In the lung, neoplastic cells grew in a densely cellular solid pattern with no evident areas of necrosis. In the surrounding invaded tissues and organs (air sacs, aorta, vertebral bodies, spinal canal, spinal cord), the neoplasm had a different growth pattern, consisting of monolayer tubules with a central lumen filled with eosinophilic amorphous material and foamy macrophages, over a thin loosely arranged fibrovascular stroma. Neoplastic cells were cuboidal, with distinct cell borders and cilia at their apical pole. There was moderate anisocytosis and anisokaryosis, and the mitotic count was 65 mitoses in 2.37 mm2. The same changes seen in case 1 in the vertebrae and spinal cord were seen in this bird. As in case 1, IP staining for CK AE1/AE3 was performed with cytoplasmic immunoreaction of neoplastic cells (Fig. 1D–F; Suppl. Fig. 2). These findings were consistent with a pulmonary carcinoma infiltrating the vertebral bones, invading the spinal canal, and compressing the spinal cord.
Case 3
A 17-y-old male orange-winged parrot (Amazona amazonica) was presented with a 1-mo history of generalized weakness. Upon physical examination, the bird was mildly depressed, with a body weight of 445 g and a body condition score of 3 of 5. General physical examination was unremarkable. Radiographs revealed hepatomegaly and increased opacity of the left and right caudal air sacs, compatible with airsacculitis. The bird had severe leukocytosis (76 × 109/L; RI: 6–11 × 109/L) and hyperbetaglobulinemia (14.2 g/L; RI: 3.8–7.6 g/L). 7 Liver and air sac biopsies taken by endoscopy revealed granulomatous hepatitis and airsacculitis. Ziehl–Neelsen (ZN) stain of the liver sample demonstrated intracellular acid-fast bacilli compatible with mycobacteria. Initial treatment consisted of enrofloxacin (15 mg/kg q12h), azithromycin (40 mg/kg q24h), and pentoxifylline (100 mg/kg q12h), for 1 mo. Two months later, the bird developed ataxia and proprioceptive deficits in both legs. Neurologic examination revealed paraparesis. T2-weighted MRI images showed diffuse hyperintensity of the lumbar spinal cord, with greater severity on the left side, suggesting a spinal cord inflammatory process or edema. No other abnormalities were observed in the rest of the coelomic cavity.
Postmortem examination showed that the bird was in poor body condition with marked muscle atrophy. The most relevant gross finding in the coelomic cavity was mild-to-moderate thickening of the duodenum wall. Microscopically, the changes detected in the spinal cord by imaging corresponded to mild perivascular aggregates of histiocytes with foamy cytoplasm, and fewer lymphocytes and plasma cells in the leptomeninges; in the brain and leptomeninges were perivascular cuffs of the same inflammatory cells up to 6 cells thick. Duodenal villi were markedly thickened and blunted as a result of massive infiltration by large histiocytes with foamy cytoplasm plus some multinucleate giant cells in the lamina propria. There were also histiocytic inflammatory infiltrates in the lung, adipose tissue of the coelomic cavity, pericardium, spleen, liver, and adrenal glands. ZN staining revealed intracytoplasmic acid-fast bacilli compatible with mycobacteria (Fig. 2). A direct PCR assay 4 of frozen liver samples revealed Mycobacterium spp., neither M. avium nor M. tuberculosis complex; bacterial culture in liquid medium for 3 wk confirmed the presence of Mycobacterium spp. The rRNA sequencing had a 100% match with the 16S gene of M. genavense, allowing the diagnosis of multisystemic infection caused by Mycobacterium genavense.
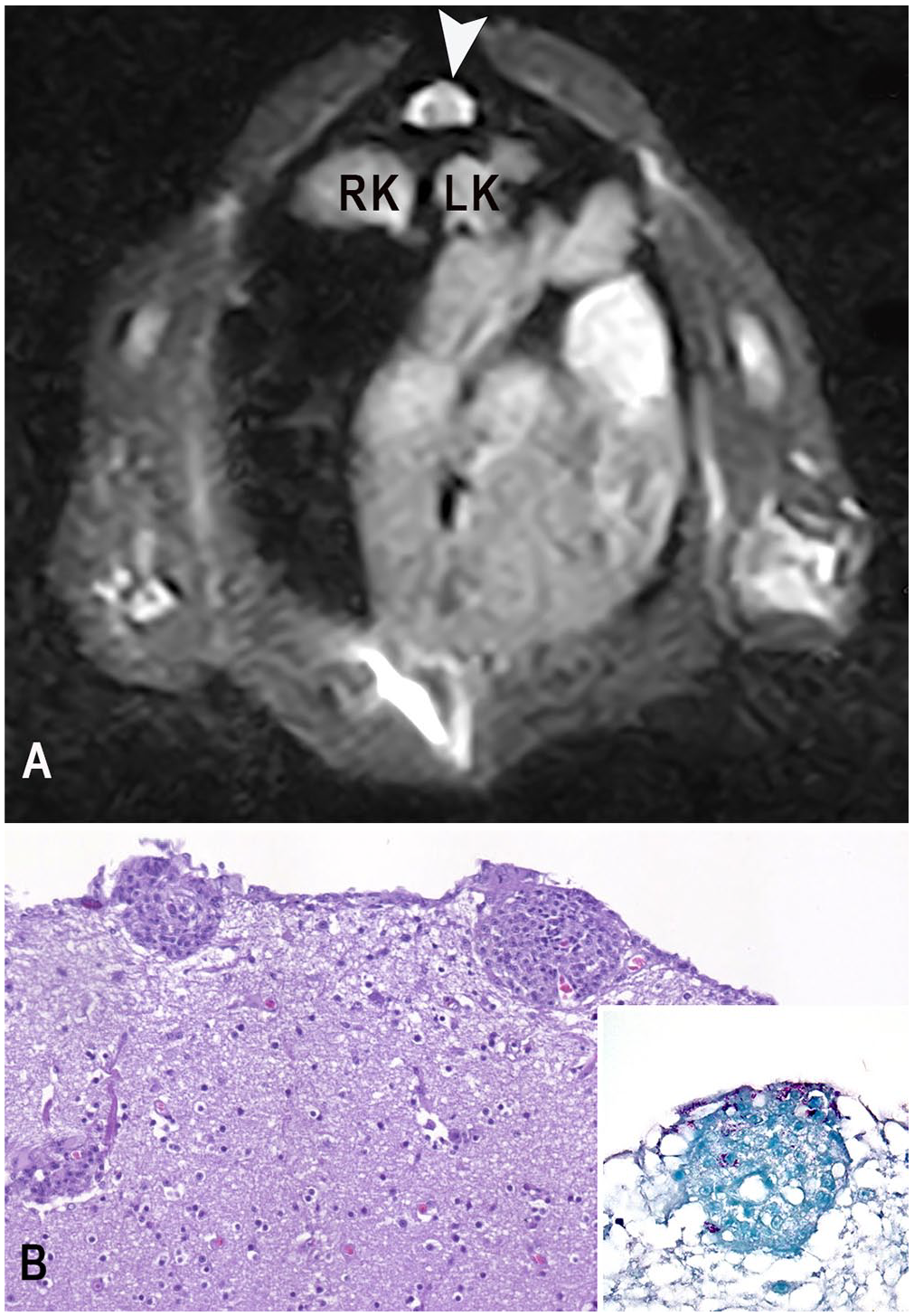
Orange-winged parrot, case 3.
We have described here 3 cases of neurologic alterations in the legs of psittacines. Ataxia and paraparesis or paraplegia is common in birds, especially in psittacines. 10 In all 3 cases, MRI allowed a more appropriate prognosis than radiography, as has been suggested in other cases. 15 Furthermore, MRI made it possible to confirm the poor prognosis resulting in the election of euthanasia.
The multilobular masses observed by MRI within the coelomic cavity of cases 1 and 2 and their infiltrative behavior were consistent with malignant neoplasia or an inflammatory process with a nodular pattern. The postmortem examination of both birds revealed similar findings highly compatible with carcinoma effacing the left lung and widely infiltrating adjacent tissues and the thoracic vertebral spine, reaching the spinal cord and inducing compressive degenerative changes, thereby causing the observed clinical signs such as paraparesis, in agreement with previous reports.2,5 The microscopic findings are in accord with reported carcinomas arising from the lung2,5,13 or the air sacs, 13 although the growth pattern and cellular features of both tumors were different. The growth pattern in case 1 was in multi-layered nests with areas of necrosis, whereas in case 2, the MRI detected cystic cavities correlated with the abundant monolayer tubules with a central lumen detected in the surrounding soft tissues, air sacs, and vertebral bone. In case 1, the neoplastic cells had only occasional cilia, whereas cilia were a common finding in case 2. The difference between these 2 neoplasms could be a consequence of different cellular origin: case 1 being potentially of pulmonary origin, and case 2 originating from the air sacs, as the appearance of case 2 was similar to reported air sac cystadenocarcinomas.1,11,12 The differentiation between pulmonary carcinoma and air sac cystadenocarcinoma is challenging. Although infiltration of the humerus has been reported as a constant finding in air sac carcinomas, it has also been described in some lung carcinomas.2,8 We did not find changes in the humerus by MRI nor in postmortem examination in any of the birds, and therefore we classified both tumors as pulmonary adenocarcinomas.
In case 3, the MRI revealed diffuse hyperintensity of the lumbar spinal cord, more severe on the left side. These changes corresponded histologically to mild histiocytic leptomeningitis of the spinal cord. The detection of mild changes in the MRI in case 3 supports its utility in the diagnosis of CNS diseases in this species. The gross and histologic findings in our case are in accord with the only report of M. genavense infection involving the CNS of a parrot. 6 Culture of a liver sample confirmed M. genavense. Infection of the CNS in psittacines is usually part of a systemic process, and the microscopic lesions in case 3 are similar in other affected organs. 13 Although the source and route of infection with M. genavense in our case could not be determined, an oral route was suggested given the severe gastrointestinal lesions. However, moderate lesions were found in the respiratory tract; hence, an aerogenic route could not be ruled out. Hematogenous dissemination is a feasible explanation for the extension of the lesions to the CNS, as has been suggested in other reports.6,15
Supplemental Material
sj-pdf-1-JVD-10.1177_10406387221097655 – Supplemental material for Clinical, imaging, and pathologic features in cases of neurologic disease in 3 psittacine birds
Supplemental material, sj-pdf-1-JVD-10.1177_10406387221097655 for Clinical, imaging, and pathologic features in cases of neurologic disease in 3 psittacine birds by Ester Pintado, Jaume Martorell, Ferran Solanes and Antonio J. Ramis in Journal of Veterinary Diagnostic Investigation
Footnotes
Acknowledgements
We thank Blanca Pérez and Aida Neira from the Servei de Diagnòstic de Patologia Veterinària, Universitat Autònoma de Barcelona (Spain) for their technical assistance, and Caroline Idowu for revising the manuscript.
Declaration of conflicting interests
The authors declared no conflict of interest with respect to the research, authorship, or publication of this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.