
Abstract
Our goal was to validate a human hyaluronic acid (HA) ELISA (Hyaluronic acid plus ELISA; TECOmedical Group) for use in feline plasma. Plasma from 5 healthy cats and 5 critically ill cats was used for validation of the assay. Validation methods performed included intra- and inter-assay variability, spike-and-recovery, and dilutional linearity. All measurements were performed in duplicate. The precision study revealed good intra-assay CV of 7.4–8.9%; inter-assay CV was 3.4–4.2%. Extraction efficiency via spiking tests yielded mean recovery of 89.6%. The assay met criteria for acceptable linearity using 3 serial dilutions. Our results demonstrate that this commercial HA ELISA had acceptable analytical performance using feline plasma and could be a useful tool in the veterinary clinical research setting.
Hyaluronic acid (HA) is a large glycosaminoglycan with wide distribution throughout the body. It is found in most biological fluids and tissues and is conserved in all vertebrates.8,10 Hence, HA is utilized as a biomarker for multiple conditions in human medicine including renal insufficiency, 1 hepatic fibrosis, 30 diabetes, 22 and atherosclerosis. 28 Reports of HA quantification are limited in veterinary medicine. Increases in serum HA concentration have been reported in dogs with histologic evidence of cirrhosis compared to non-cirrhotic hepatic disease, 18 increasing extent of hepatic fibrosis, 12 dermatologic conditions, 35 and with congenital portosystemic shunts compared to healthy controls. 29 More recently, HA has emerged as a biomarker of endothelial glycocalyx (EG) integrity, with numerous human studies reviewed in the literature. 32
The EG is a complex, dynamic structure that lines the luminal surface of vascular endothelium. The structure consists of a cell-bound anchoring component comprised of proteoglycans (syndecans, glypicans) and glycoproteins (selectins, immunoglobulins, integrins), which support and contribute to an intricate mesh-like layer. In addition to the anchoring component, multiple non–membrane-bound glycosaminoglycans are woven into this mesh-like structure. HA is one such glycosaminoglycan, found most abundantly at the luminal surface of the EG. 11 Dynamic changes in EG integrity have been identified in various conditions in human patients, including sepsis, 2 ischemia reperfusion injury post-cardiac arrest, 15 trauma, 26 hemorrhagic shock, 16 and hypervolemia secondary to intravenous fluid administration. 7 When the EG is damaged, its degradation is accompanied by shedding into the bloodstream of multiple EG constituents, such as HA, which can be quantified. Commercial HA assays have been successfully validated by manufacturers for use in dogs.24,31 To date, there are no EG biomarkers validated for use in cats. We validated a human HA ELISA (Hyaluronic acid plus ELISA; TECOmedical Group) for use with feline plasma.
The assay utilized is a sensitive sandwich ELISA used for the quantification of HA in plasma, serum, and other biological fluids in humans. The assay is based on a HA-specific binding protein that is not species specific; it has been validated by the manufacturer for use in multiple species including dogs, horses, mice, rats, sheep, pigs, monkeys, and goats. The assay consists of a microtiter plate coated with HA-binding protein (HABP), with horseradish peroxidase (HRP)-conjugated HABP used for detection. The HRP-conjugated HABP binds to HA in the sample, followed by a substrate reaction. Color development is catalyzed quantitatively dependent on the HA concentration in the sample. The reportable assay range is 15–1,000 ng/mL.
Blood samples from 5 healthy blood donor cats and 5 critically ill cats with evidence of systemic inflammation or abnormal perfusion were used to provide an anticipated range of HA concentrations. Our study was approved by the Institutional Animal Care and Use Committee of the University of Guelph. Blood donor cats were deemed healthy based on unremarkable physical examination, biochemical profile, complete blood count, and urinalysis. Prior to scheduled blood donation, cats received oral gabapentin. Premedication with intramuscular butorphanol was administered to facilitate placement of a cephalic intravenous catheter. Intravenous ketamine and midazolam were then used to achieve adequate sedation. Jugular venipuncture was performed to collect 0.5 mL of blood for the study prior to the volume collected for blood donation.
Cats in the critically ill group were included based on abnormalities in 3 or more of the following objective parameters suggesting the presence of systemic inflammation or abnormal perfusion: rectal temperature <37.8 or >39.7°C, heart rate <140 or >225 beats per minute, respiratory rate >40 breaths per minute, capillary refill time >2 s, systolic arterial pressure <90 mm Hg, or blood lactate concentration >2.5 mmol/L.5,6,27 All critically ill cats except for one had received various levels of treatment elsewhere prior to referral, but remained in critical condition on hospital arrival. For critically ill cats, residual blood sample was utilized from the time of admission to hospital upon intravenous catheter placement.
For all collections, the blood sample was transferred immediately to a blood collection tube containing EDTA as an anticoagulant (EDTA tube Vacutainer plus; Becton Dickinson). Within 30 min of collection, the sample was centrifuged at 1,000 × g for 15 min. Plasma samples were then aliquoted and stored at –80°C for up to 6 mo prior to batch analysis. The manufacturer reports stability of HA concentration for up to 3 y at –80°C. The samples were assayed immediately after thawing at room temperature. Given that the samples were frozen in aliquots, an aliquot was thawed for each analysis to prevent potential variation as a result of freeze–thaw cycles. The assay was performed according to the manufacturer’s instructions, which included dilution of all samples (1:50) using the supplied standard solution to reduce matrix interference. All measurements were performed in duplicate. A standard curve was prepared using serial dilutions of the standard diluent buffer provided in the test kit and according to the manufacturer’s instructions. Absorbance was detected at 450 nm with an ELISA plate reader (Epoch microplate spectrophotometer; BioTek Instruments).
Imprecision was evaluated by determining intra- and inter-assay variability. CVs were based on repeated measurements within the same analytical run as well as across analytical runs. Intra-assay variability was performed using 10 duplicate measurements across 2 experiment days. Inter-assay variability was assessed over 2 experiment days using 5 duplicate measurements on 5 different plates. For each analytical run, SD was calculated as the square root of the estimated variance components. The CV was then calculated as (SD/global mean) × 100 to evaluate imprecision of the assay. Imprecision was deemed acceptable for CVs ≤10%. 19 Intra- and inter-assay CVs were 7.4–8.9% and 3.4–4.2%, respectively (Table 1).
Imprecision of the human ELISA (Hyaluronic acid plus ELISA; TECOmedical Group) for measuring plasma hyaluronic acid concentration in cats over 2 experiment days.
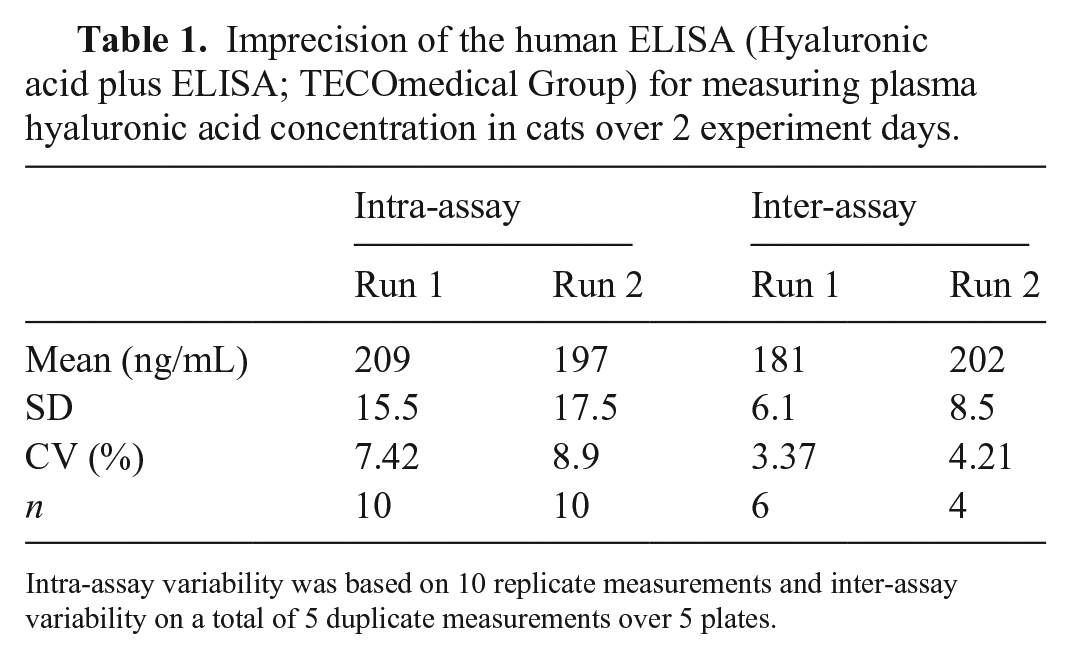
Intra-assay variability was based on 10 replicate measurements and inter-assay variability on a total of 5 duplicate measurements over 5 plates.
Accuracy was assessed by evaluating the ability of the assay to recover a known concentration of analyte. A recovery method based on addition of provided standard solution (HA 1,000 ng/mL) to baseline plasma samples was used. Recovery was performed using 5 healthy feline plasma samples at various concentrations (20–100 ng/mL) and adding the provided standard (HA 1,000 ng/mL) to create a 10% spiked solution. All samples were run in duplicate. Acceptable recovery-after-spiking was set at 80–120%. 3 The mean accuracy assessed by the recovery study was 89.6% (Table 2).
Recovery method of the human ELISA (Hyaluronic acid plus ELISA; TECOmedical Group) for measuring plasma hyaluronic acid (HA) concentration in cats.
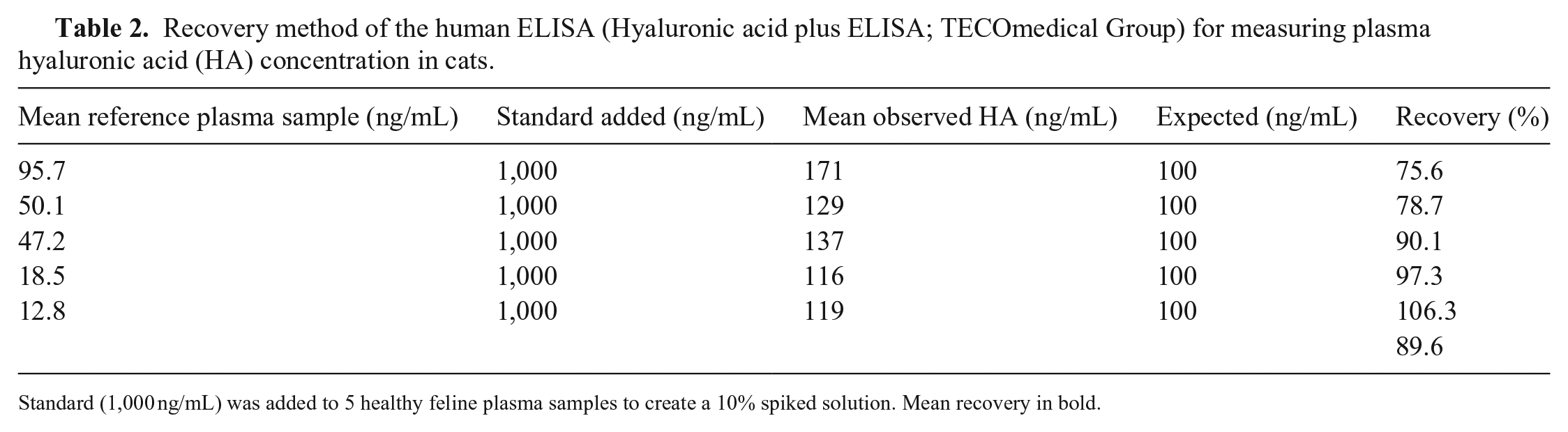
Standard (1,000 ng/mL) was added to 5 healthy feline plasma samples to create a 10% spiked solution. Mean recovery in bold.
Linearity was evaluated by serial dilutions of baseline samples. This was assessed using 3 plasma samples from critically ill cats (HA concentration of 287–435 ng/mL) performed in a single run. Duplicate HA measurements were performed on each sample. The samples were serially diluted by adding diluent (HA 0 ng/mL) to obtain 50%, 25%, 12.5%, and 6.25% dilutions. The dilutional linearity was plotted (Fig. 1) as the measured values versus expected values calculated on the basis of the baseline samples and subsequent serial dilutions (Prism v.9; GraphPad). The comparable measured and expected values of HA concentration was demonstrated by the slope of the linear regression curve, which was 0.95–1.00 in each analytical run. The coefficient of correlation of the linear regression curve was also meaningful, with an R2 of 0.98–0.99.
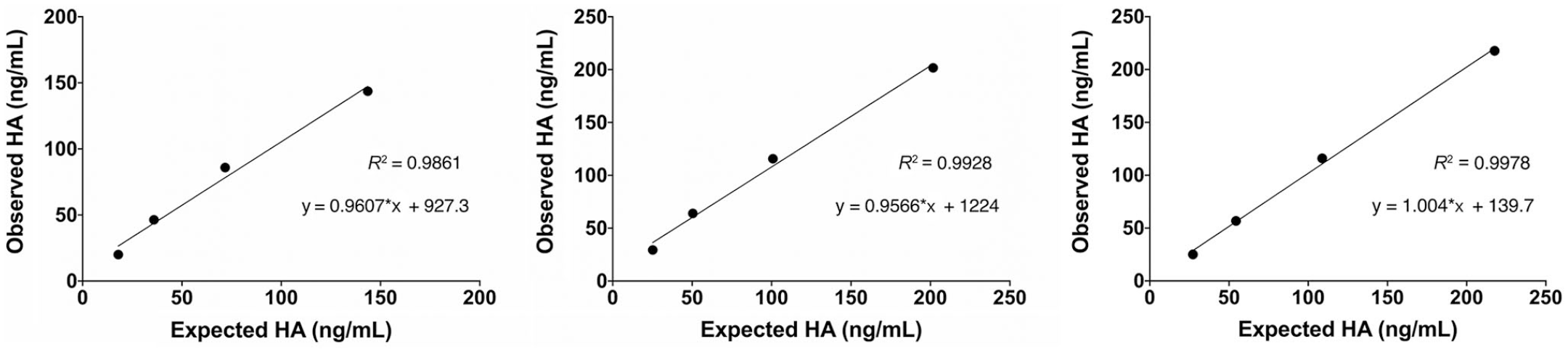
Linear regression analysis of expected versus observed hyaluronic acid (HA) concentrations of 3 serially diluted feline plasma samples. Data points are the means of 2 determinations.
Our results support analytical validation of this human HA assay for measurement of plasma HA in cats. In the small cohort of cats used in our study, the median plasma HA concentration was 47.2 ng/mL (12.8–95.7) for healthy cats and 202 ng/mL (287–435) for critically ill cats. The assay demonstrated adequate intra- and inter-assay variability. The spike-and-recovery method revealed acceptable mean accuracy of 89.6%. Interestingly, as baseline plasma HA concentration increased, the percent recovery decreased. When this effect occurs at extremely high concentrations, it can be consistent with a prozone effect. However, because this effect occurred well within the reportable range of the kit, it is likely that another form of matrix effect was occurring. Given that all samples were collected, handled, and stored uniformly, analyte-independent interference is considered unlikely. The overall recovery rate remains acceptable; however, it is possible that the kit’s performance could differ at higher baseline HA concentrations. The linearity under dilution was performed at both high and intermediate concentrations with 3 different samples, and results were considered acceptable.
The main limitation of our study pertained to the volume of sample available from each cat, which prevented a higher number of repetitions, and the lack of availability of baseline samples at a wider HA concentration range. Performing dilutional linearity with 5 different samples is recommended by American Society for Veterinary Clinical Pathology (ASVCP) guidelines 4 ; however, the samples meant to represent low concentrations were close to the lower limit of detection prior to dilution and therefore were excluded from further analysis. Linearity above the upper limit of quantification was also not performed, and therefore prozone effects at extremely high concentrations again cannot be ruled out. Overall, our results for linearity were excellent when performed at clinically relevant values. Furthermore, the principle of fit-for-purpose validation states that validation efforts should be tailored to meet the intended purpose of the biomarker study, and with a level of fastidiousness proportionate to the intended use of the data. 20 The accuracy and linearity achieved in our study are therefore considered acceptable for ongoing investigation; however, future investigators should consider their intended use of this biomarker to ensure that supplemental validation at various concentrations is not required. Finally, although the manufacturer considers serum, EDTA plasma, cell culture supernatant, and synovial fluid to all be appropriate sample types for use in this assay, our study was performed specifically on EDTA plasma samples and therefore validation studies would need to be performed prior to its use with other sample types.
As mentioned, damage to the EG occurs in several conditions and can also be iatrogenic, such as secondary to intravenous fluid therapy.7,17,25,31 Measurement of circulating EG constituents, such as HA, serve as biomarkers of EG health, and allow quantification of the extent of EG damage. 9 Recent human literature has shown increased interest in the utility of EG biomarkers, and has stressed the importance of EG integrity in critically ill patients. HA is not a specific EG biomarker, and therefore its utility is strengthened when used in conjunction with additional EG biomarkers (e.g., syndecan-1, heparan sulfate, chondroitin sulfate). Human studies thus far indicate that there is high variability in reported concentrations of EG biomarkers dependent on the commercial assay that is used for detection. 33 Therefore, particular attention to the assays used when considering comparison between studies is essential.
To date, the value of EG biomarker measurement in cats is unknown. Our investigation was prompted by an interest in the effects of fluid therapy on the EG in cats. Cats have an increased susceptibility to the negative effects of fluid therapy given their small blood volume,13,14 high incidence of occult cardiomyopathy,21,23 and slow rate of fluid elimination. 34 Successful validation of this HA ELISA will now allow its use for EG biomarker quantification in prospective feline studies.
Footnotes
Acknowledgements
We thank Michelle Beaudoin-Kimble for technical assistance.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Our study was funded by the Ontario Veterinary College Pet Trust Fund. The funding agency had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.