
Abstract
A 10-y-old giraffe (Giraffa camelopardalis reticulata) bull developed colic after a 3-mo history of reduced feed consumption. Physical examination and management were performed with 2 standing sedations. The giraffe developed metabolic alkalosis and progressive pre-renal azotemia followed by compensatory respiratory acidosis and paradoxical aciduria. A metallic “ping” sound was auscultated on the left side near ribs 10–12. The giraffe was euthanized given the grave prognosis, and postmortem examination confirmed left displacement of the abomasum (LDA) with fluid sequestration (150–190 L [40–50 gal]) within the rumen. Dental disease was evident at postmortem examination and perimortem skull computed tomography. To ensure cases of LDA are not overlooked, the position of the abomasum must be noted during postmortem examination prior to removal of the gastrointestinal tract. The risk factors for the development of LDA in giraffes are not known, and associations such as those of dairy cattle (hypocalcemia, high-concentrate low-fiber diet, and indoor housing) remain to be elucidated.
Giraffe (Giraffa camelopardalis) are an iconic species; however, reports on their diseases are infrequent and have focused primarily on common hoof and musculoskeletal lesions.1,11 Sporadic reports of giraffe gastrointestinal disease have included ruminal acidosis, functional or obstructive ileus or impaction, and nutritional serous atrophy of fat or “peracute mortality syndrome.”1,6,11,18 Displacement of the abomasum (DA) has not been reported previously in giraffe, to our knowledge, and is also extremely rare other than in peri-parturient domestic dairy cows.2,8,19 We describe here the clinical presentation, laboratory testing, and attempted stabilization of a giraffe bull with left displacement of the abomasum (LDA), as well as a description of steps for accurate diagnosis during postmortem examination.
A 10-y-old reticulated giraffe (G. camelopardalis reticulata) bull at Binder Park Zoo (Battle Creek, MI, USA) had a 3-mo history of reduced feed consumption and primarily indoor housing given cold winter ambient temperatures. The bull was successfully trained for blood collection using operant conditioning, and repeated bloodwork (serum biochemistry and complete blood count [CBC]) was unremarkable except for mild hypophosphatemia (Table 1). Urinalysis, fecal occult blood, and serum trace mineral panel tests were unremarkable. During this period, the following changes were made resulting in improved feed consumption; trace mineral block moved to an appropriate height, novel puzzle feeders, and slow transition from grass hay to free-choice alfalfa, and from Mazuri wild herbivore diet hi-fiber to Mazuri wild herbivore plus diet (PMI Nutrition International).
Bloodwork and urinalysis results from a 10-y-old giraffe bull with left displacement of the abomasum. Included are results from −60 and −30 d prior to acute presentation (time 0) and the subsequent 86 h.
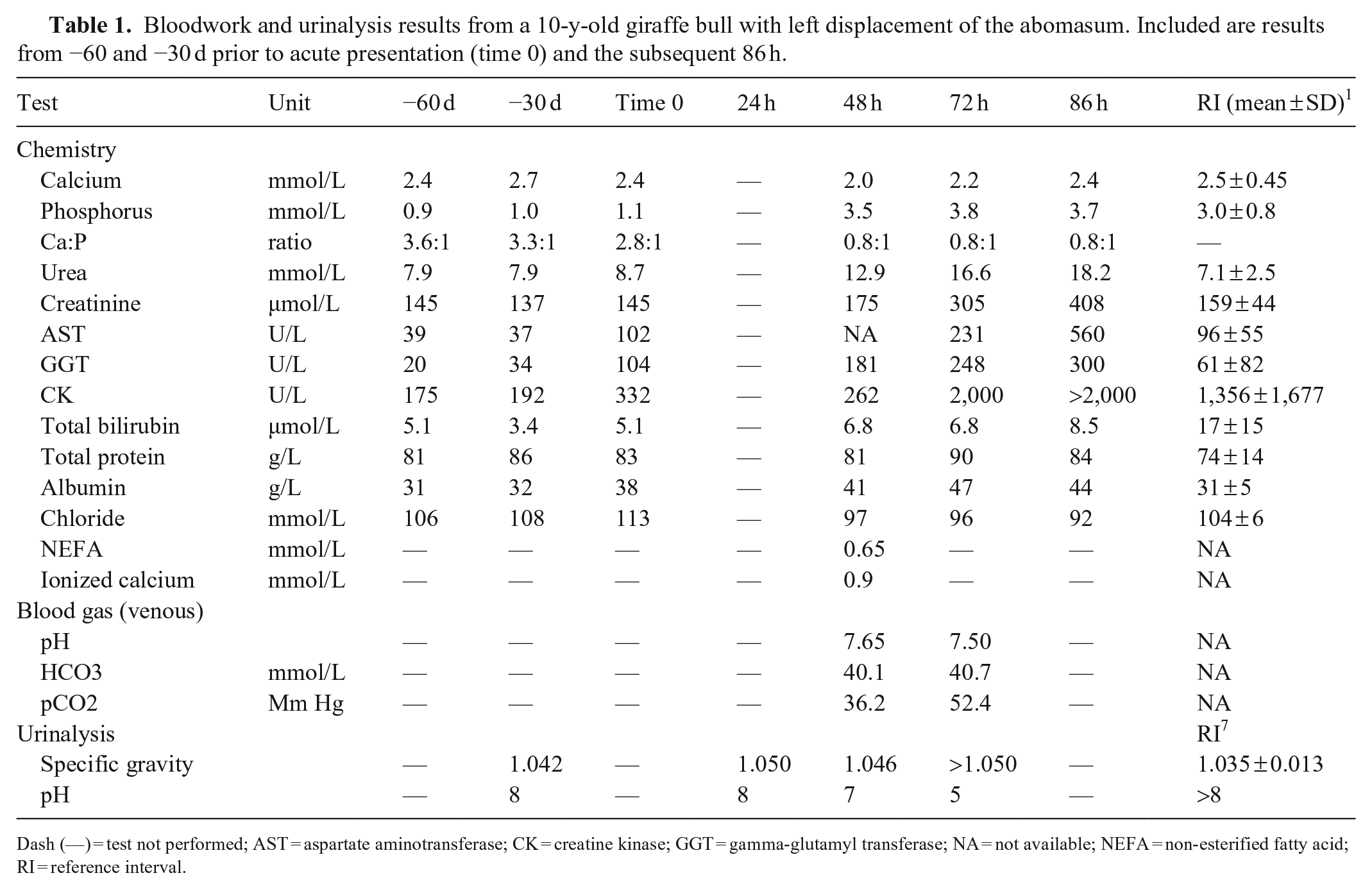
Dash (—) = test not performed; AST = aspartate aminotransferase; CK = creatine kinase; GGT = gamma-glutamyl transferase; NA = not available; NEFA = non-esterified fatty acid; RI = reference interval.
The giraffe then developed acute signs of colic: anorexia, dull attitude, vocalizing, muscle tremors, reluctance to stand, head pressing, crossing hindlimbs, swishing tail, and stretching. Urinalysis was unremarkable, other than being consistent with dehydration (SG = 1.050). Fecal occult blood was negative. Serum chemistry and CBC changes were unremarkable except for mild hypophosphatemia and a mild increase in gamma-glutamyl transferase (GGT) activity (Table 1). Serum non-esterified fatty acids (NEFA) were elevated and supportive of a negative energy balance based on cutoff values in dairy cattle. 14 Initially, there was improvement in clinical signs after treatment with phenylbutazone and butorphanol.
Over the subsequent 38 h, the giraffe remained dull and anorexic with worsening dehydration, increased eructation, and decreased defecation. Two standing sedations were performed. During the first sedation, the giraffe developed acute midcervical segmented torticollis that resolved with direct manual force and antagonist administration (flumazenil, atipamezole, and naltrexone). Bloodwork alterations included: metabolic alkalosis, inversion of the calcium: phosphorus ratio as a result of hypocalcemia and hyperphosphatemia, hypochloremia, increased GGT activity, and azotemia (Table 1). A metallic “ping” was auscultated with percussion on the left side at ribs 10–12, suggestive of LDA.
During the standing sedation the following day, percutaneous rumen trocarization for decompression was unsuccessful because the trocar was obstructed by ingesta. The bull’s dehydration of 7% was estimated to entail a deficiency of 50–60 L of fluid. Intravenous 0.9% NaCl, 23% calcium gluconate, vitamin B complex, and flunixin meglumine were administered via jugular catheter. Bloodwork, performed both before and after fluid administration, demonstrated worsening pre-renal azotemia, hypocalcemia, hypochloremia, and elevated GGT, creatine kinase, and aspartate aminotransferase activities (Table 1). In response to the metabolic alkalosis, the giraffe developed compensatory respiratory acidosis and hypochloremia with paradoxic aciduria (Table 1). Acute severe torticollis of midcervical vertebrae re-occurred during standing sedation and worsened over the following hours, despite reversal of sedation. The goal to stabilize the giraffe through vascular support was unsuccessful, the animal’s condition declined, and euthanasia was elected rather than pursue exploratory laparotomy for suspected LDA.
The giraffe was transported to the Michigan State University Veterinary Diagnostic Laboratory (Lansing, MI, USA) for postmortem examination. The giraffe weighed 820 kg with low-to-moderate amounts of adipose tissue but no serous atrophy of fat. The rumen was markedly distended with fluid and had normal papillae. The rumen, reticulum, and omasum contained 150–190 L (40–50 gal) of fluid with scant fibrous material. The abomasum was displaced to the left side of the abdomen (Figs. 1, 2). Postmortem examination confirmed the diagnosis of LDA, with fluid sequestration in the rumen, reticulum, and omasum. The mucosa of the abomasum had numerous, linear-to-irregular dark-red hemorrhages (Fig. 3). The ventral aspect of the left cranial lung lobe had a 14 × 8 × 6 cm subpleural bulla. All other organs appeared normal at postmortem examination. Premolars and molars had flattening of the occlusal surfaces and gingival recession with root exposure of the buccal surface of right maxillary molars 1 and 2 (Fig. 4). Perimortem skull computed tomography confirmed severe horizontal bone loss and evidence of bone lysis around the roots of right maxillary molars 1 and 2 (Fig. 5).
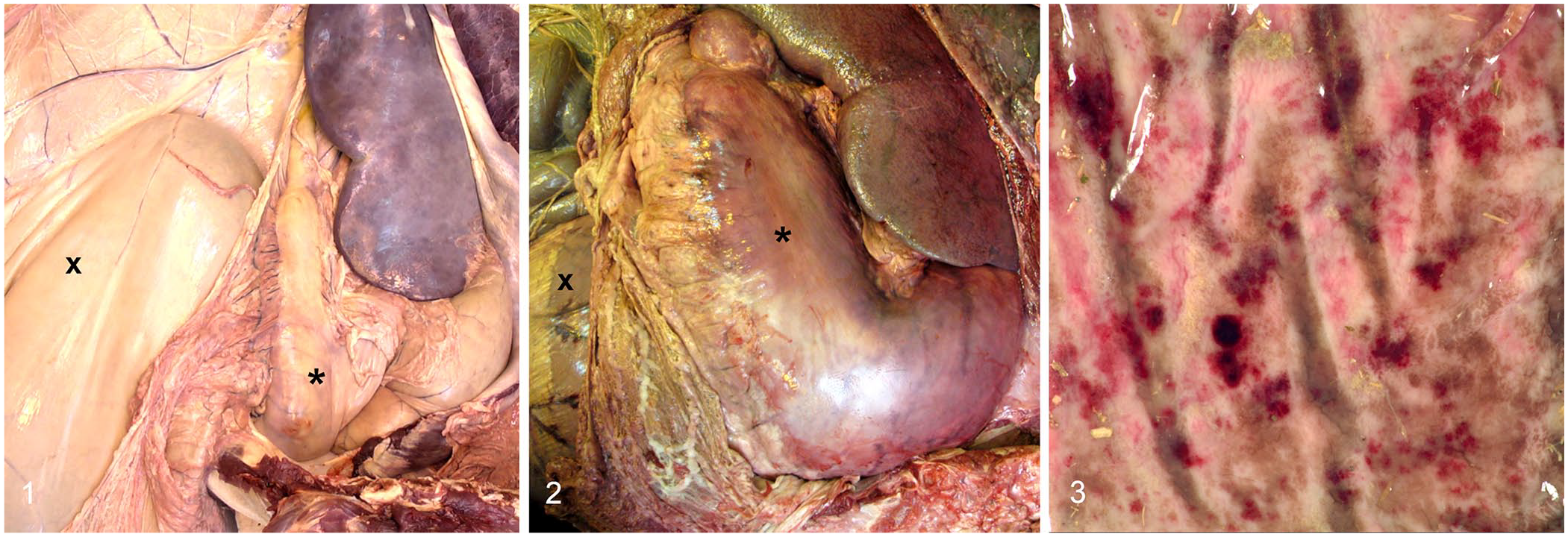
Postmortem findings from a 10-y-old giraffe bull with left displacement of the abomasum (LDA) and dental disease.
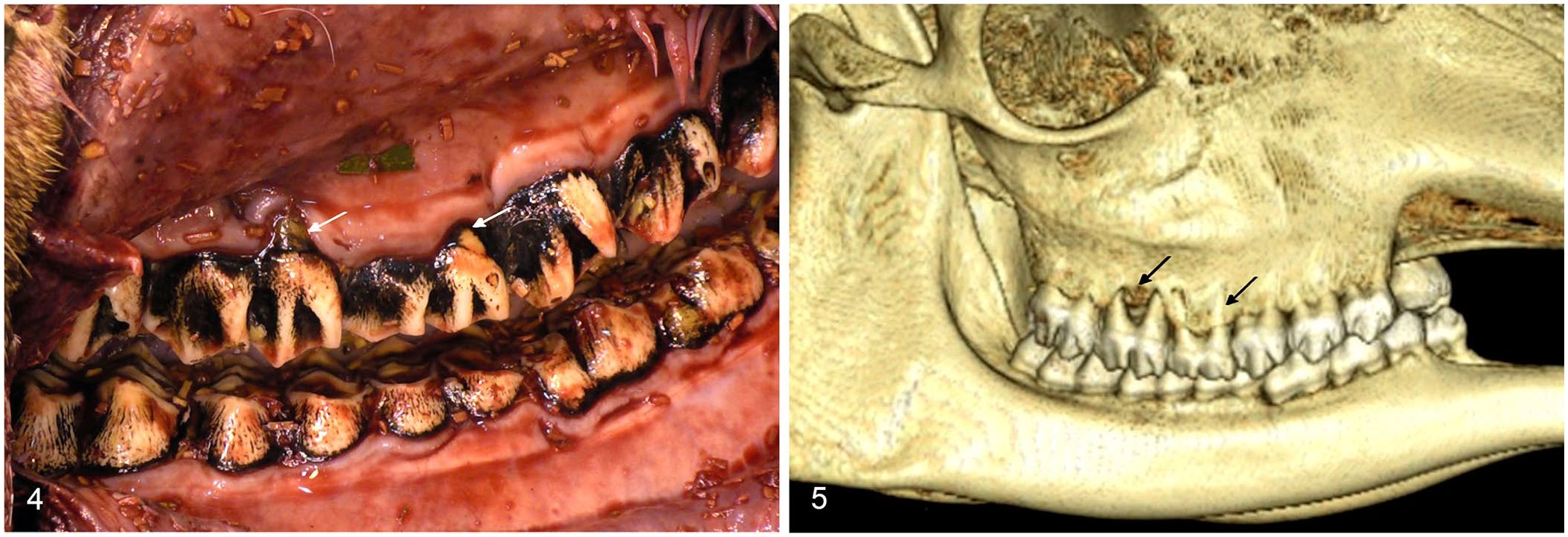
Dental disease in a 10-y-old giraffe bull with left displacement of the abomasum.
Representative sections of cerebrum, cerebellum, brainstem, eye, heart, lung, liver, kidney, spleen, forestomachs, small and large intestine, thyroid gland, gallbladder, haired skin, adrenal gland, tongue, skeletal muscle, testis, and trachea were placed in formalin and processed routinely for histologic examination. Histologically, the mucosa of the abomasum had areas of acute hemorrhage with mild superficial-to-shallow ulcers infiltrated by neutrophils. Additional incidental morphologic diagnoses included mild multifocal necrotizing hepatitis and mild multifocal myocardial fibrosis. The final diagnosis in this giraffe was left displacement of the abomasum with fluid sequestration in the forestomachs. It remains unknown if the rumen distention and forestomach fluid sequestration, consistent with vagal indigestion, occurred prior to or as a consequence of LDA.
Placement of a ruminant in left lateral recumbency for postmortem examination allows visualization of the abomasum in its normal proper anatomic location (Fig. 2). 15 The prosector must confirm that the position of the abomasum is correct or displaced either to the right or left prior to removal of the gastrointestinal tract to ensure that cases of DA are not overlooked given that the abomasum may be otherwise normal in appearance. Our case demonstrates that exotic ruminants can be subject to diseases observed commonly in domestic species.
The diagnosis of LDA is extremely rare, except in peri-parturient early-lactation dairy cows.2,8,19 Risk factors for the development of DA include causes of rumen and abomasal hypomotility, including the peri-parturient period, winter indoor housing, hypocalcemia, high-concentrate low-fiber diets, ruminal acidosis, and concurrent diseases.2,8,9,21 Many of the aforementioned risk factors are known to occur in managed giraffes, but their relationship to LDA development is unknown in this species.1,3,18,22 Giraffes are strict browsers and therefore may have difficulty adapting to a captive diet.4,10–12,16,17,20 Captive giraffes frequently consume a high proportion of concentrates with short fiber lengths. Small fiber lengths are a risk factor for DA because they do not adequately stimulate rumen contractions.2,21 Grass forages have higher silica levels than browse, which accelerate wear of browser teeth and may lead to dental disease and altered feed intake in giraffe and exotic ruminants.4,11,18 Alfalfa and browse, compared to grass hay, have higher calcium and lower silica, which may preserve dental health and prevent subclinical hypocalcemia in these species.4,12,13,16 Giraffes from northern zoos spend a large portion of the winter indoors with decreased activity and sunlight, which may alter gastrointestinal motility and calcium metabolism. Underlying dental disease may have predisposed to the decreased feed consumption, especially of fiber, observed in this giraffe bull. Other potential factors predisposing to development of LDA in this bull may have included hypocalcemia, indoor winter housing, and high concentrate consumption.
The diagnosis of LDA in cattle is supported by metabolic alkalosis with hypocalcemia, hypokalemia, hypochloremia, dehydration, a metallic ping between ribs 8 and 13, decreased feed intake, elevated NEFA, and weight loss8,9; these abnormalities were all observed in this giraffe bull (Table 1). Sequestration of hydrochloric acid within the displaced abomasum results in metabolic alkalosis, interstitial movement of fluid, and hypovolemia, as was evident in the severe fluid distension of the forestomachs of this giraffe. 8 Just prior to euthanasia, the giraffe developed paradoxic aciduria (Table 1), which can be observed in severe cases of abomasal displacement or volvulus. 8 Paradoxic aciduria develops as a result of stimulation by hypochloremia and hypovolemia of renal secretion of aldosterone and hence absorption of sodium. 8 In a healthy animal, sodium is exchanged for potassium; however, with depleted potassium, sodium is exchanged for hydrogen resulting in paradoxic aciduria. 8 Elevated NEFA values are associated with increased risk of abomasal displacement in dairy cows.2,14,21 Research is needed to investigate NEFA levels in giraffes with underlying diseases, such as LDA, and those in negative energy balance. Acute segmental torticollis of cervical vertebrae is a potential complication during standing sedation of giraffes, especially with large bulls or debilitated animals. 5
Displaced abomasum should be included as a differential diagnosis in giraffes with signs of colic and abdominal distension. Although our case of LDA was in a novel species, the biochemical changes mirrored those that are reported commonly in dairy cattle, namely metabolic alkalosis, elevated NEFA, and paradoxic aciduria.8,14 Our case emphasizes the importance of blood gas analysis as a diagnostic tool for ruminants with acute abdomen, and reinforces dental evaluation of giraffes with poor feed consumption. Current zoo-housed giraffe husbandry practices, including high-concentrate low-fiber diets and indoor housing, and health issues, such as hypocalcemia, are similar to risk factors for the development of DA in cattle.
Footnotes
Acknowledgements
We thank the animal care staff at Binder Park Zoo for their dedication and hard work with the giraffes under their care, and Dr. Thomas Mullaney for his assistance with the postmortem examination and histologic interpretation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.