
Abstract
Hepatic lobe torsion is a rare condition in domestic animals. Clinical signs are variable, with some cases remaining subclinical and others resulting in death. Most cases are diagnosed either by laparotomy or during postmortem examination. During postmortem inspection of 670 slaughtered dromedary camels, hepatic lobe torsion of the quadrate lobe was detected in 3 adult female camels. Clinical signs had not been noted on antemortem veterinary inspection, and hepatic lobe torsion was likely an incidental finding. Histologically, the affected liver lobe exhibited severe hepatocellular loss with replacement by fibrous connective tissue. When investigating abdominal pain in camels, veterinarians should include hepatic lobe torsion in the list of differential diagnoses.
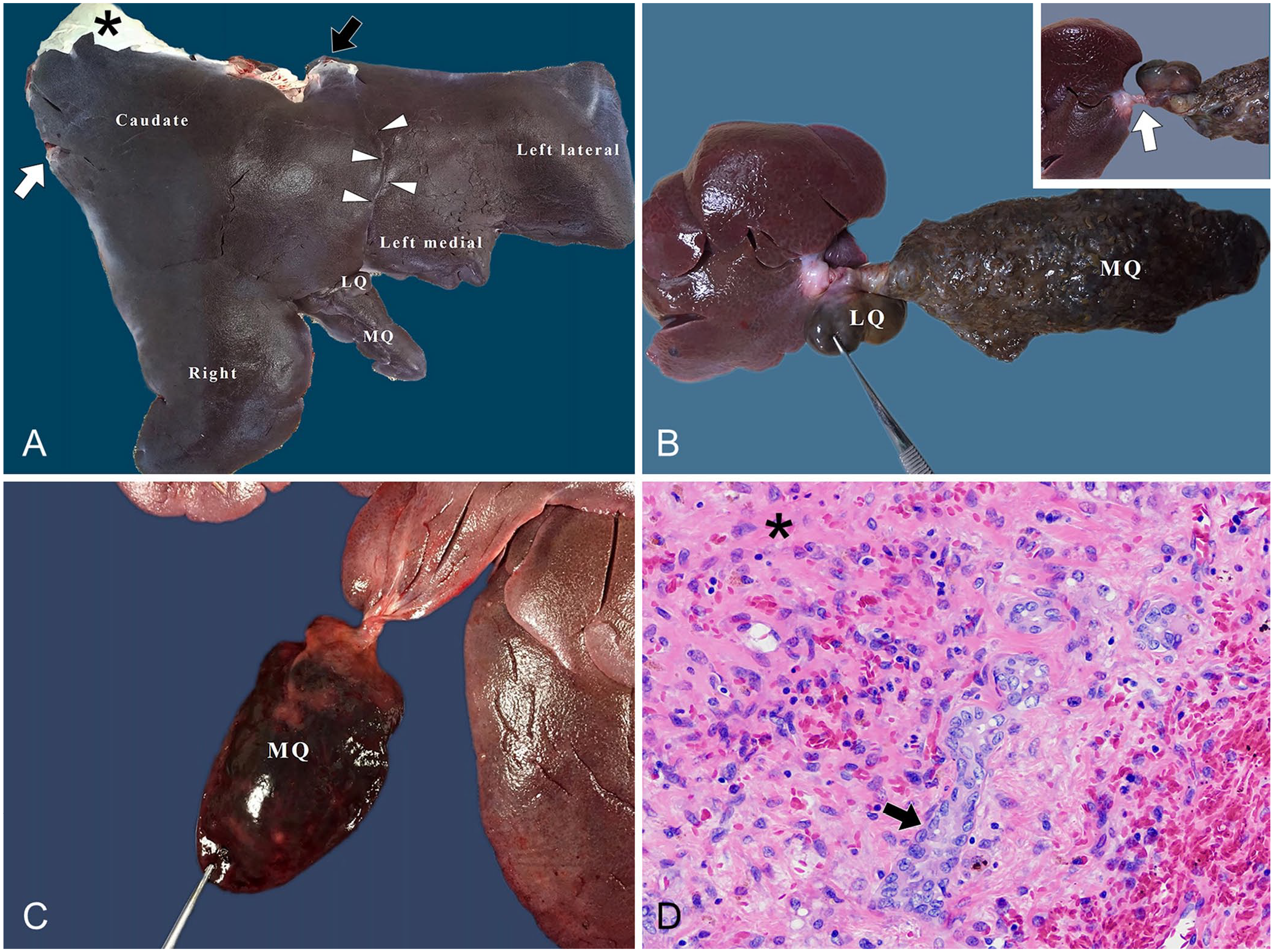
The anatomy of the camel’s liver is unique.4,10 It is divided into 4 main lobes: left, right, caudate, and quadrate (Fig. 1A). The left lobe is subdivided into lateral and medial lobes; the caudate lobe is separated into papillary and caudate processes. The quadrate lobe is split by a shallow fissure into lateral and medial parts. The medial part of the quadrate lobe is variable in color and size and may be tongue-shaped or heart-shaped. The camel liver has marked interlobular septa, is devoid of a gall bladder, and its visceral surface has small fissures. Hepatic lobe torsion has been documented in rabbits, dogs, horses, cats, rats, mice, otters, pigs, and humans.1,3,5–7,12,15 Affected animals may exhibit anorexia, abdominal pain, lethargy, tachycardia, tachypnea, fever, and icterus. 9 Some animals die suddenly because of acute venous infarction, which has led to hemoperitoneum and shock.1,8 Diagnosis is challenging given the nonspecific clinical findings. Most cases are diagnosed either by laparotomy or during postmortem examination. 6 We describe here the gross and histopathologic findings associated with hepatic lobe torsion in 3 dromedary camels (Camelus dromedarius) in Saudi Arabia.
Hepatic lobe torsion in dromedary camels.
During a study to determine the prevalence of hydatid cysts in dromedary camels in the eastern region of Saudi Arabia between January 2017 and September 2018, the livers of 670 camels were examined by A. Ibrahim, a trained pathologist. The collection was done at Al-Omran Central Slaughterhouse in Al-Ahsa, Saudi Arabia. Slaughtered camels were mostly older animals of local breeds (Majaheem, Magateer, and Wadha). During the study, hepatic lobe torsion was observed in 3 adult females of the Majaheem breed. Case 1 was 10 y old and in good body condition, case 2 was >10 y old and in fair condition, and case 3 was ~6 y old and in good body condition. Clinical signs were not observed in these 3 animals on antemortem veterinary inspection.
In case 1, the entire quadrate lobe was rotated 360° clockwise around its base, and the lobe base appeared as a white cord. The medial part was markedly enlarged, firm, and dark brown with small raised nodules on its surface; the lateral part was swollen, rounded, and dark gray (Fig. 1B). Microscopically, both the medial and lateral parts of the quadrate lobe lacked identifiable hepatic architecture. Hepatocytes were largely replaced by fibrous connective tissue with only rare individualized necrotic hepatocytes. Blood vessels were congested. Macrophages containing accumulations of hemosiderin were common. The hepatic capsule was markedly thickened by fibrous connective tissue. The tissue was often mineralized. The hepatic tissue adjacent to the affected lobe had mild cytoplasmic lipid vacuolation of zone 1 hepatocytes and diffuse accumulation of pigment within hepatocytes. Given that the hepatocellular pigment was negative with Prussian blue, Hall, and copper stains, it was presumed to be lipofuscin. Within centrilobular-to-midzonal areas, the spaces of Disse often contained homogeneous, amphophilic to lightly basophilic material that did not stain with Congo red, reticulin, or Masson trichrome stains.
In case 2, the medial part of the quadrate lobe was rotated 180° counterclockwise. The affected part of the lobe was enlarged with rounded borders, dark red, friable, and mottled with small pale areas (Fig. 1C). Histopathologic alterations in the affected lobe included marked loss of hepatocellular architecture, replacement by loose fibrous connective tissue, multifocal areas of severe hemorrhage, and small blood vessels with plump endothelium. Rarely, faint remnants of hepatocyte cords were seen. Hemosiderin-laden macrophages were numerous, and low numbers of lymphocytes and plasma cells surrounded occasional blood vessels. The blood vessels at the border of the hemorrhagic area were markedly congested. The grossly normal adjacent hepatic parenchyma had mildly increased connective tissue between portal areas, sinusoidal fibrosis, accumulation of presumed lipofuscin within hepatocytes, multifocal necrosis of biliary epithelium, and small accumulations of the same homogeneous, amphophilic to lightly basophilic material within spaces of Disse that was observed in case 1.
Similar to case 2, case 3 involved a 180° counterclockwise torsion of the medial part of the quadrate lobe. The affected liver was pale and firm with rounded edges. Microscopically, this area of liver had almost complete loss of hepatocytes with replacement by abundant fibrous connective tissue (Fig. 1D). Biliary hyperplasia was prominent, and there were multiple large areas of hemorrhage. Small multifocal aggregates of hemosiderin-laden macrophages, lymphocytes, and plasma cells were present. The adjacent unaffected hepatic parenchyma had moderate hepatocellular lipidosis affecting all parts of the lobule but was otherwise unremarkable. Serum biochemical analysis revealed no abnormalities associated with hepatic disease.
Hepatic lobe torsion is a rare entity in all of the species in which it has been reported, and it also appears to be uncommon in the dromedary camel. Of 670 camels examined in our study, only 3 cases were observed. To our knowledge, hepatic lobe torsion has not been reported previously in camelids.
Torsion has been recorded in all hepatic lobes of dogs; the left lateral lobe appears to be most commonly affected.9,11 Large-breed dogs, particularly the Akita and Golden Retriever, have been shown to be more commonly affected than small- and medium-sized breeds. 9 In rabbits, the caudate lobe is most prone to torsion because of its narrow attachment to the dorsal hilar region of the liver; 14 the left lobe appears to be predisposed in the horse.1,13 Of the 7 cases of hepatic lobe torsion reported in pigs, 4 involved the left lateral lobe and 3 involved the right lateral lobe. 7 Possible contributing factors in domestic animals include congenital lack of hepatic ligaments, trauma to the hepatic ligaments, hepatic abscesses, gastric dilation and volvulus, and bile duct neoplasia. 13
These 3 cases of hepatic lobe torsion in camels all affected the quadrate lobe, which may be predisposed given its relatively long length and narrow width, separation from other lobes, and increased mobility. The camel liver is fixed in position by surrounding organs and by its ligaments, including the right and left triangular, falciform, coronary, round, and hepatorenal ligaments, thus hepatic torsion is unlikely to occur in other lobes.4,10
Hepatic lobe torsion in camels may be comparable to torsion of the Riedel lobe in humans.2,5 The Riedel lobe is an anatomic variation, described as a tongue-like elongation of hepatic segments V and VI extending from the right lobe to the level of the umbilicus. Various studies estimate the prevalence of this variation in the human population at 3.3–14.5%. The presence of the Reidel lobe is usually not problematic, but the narrow pedicle and absence of fixating ligamentous attachments make the lobe susceptible to torsion.
Based on gross and microscopic findings, these 3 cases of hepatic torsion were considered chronic and incidental. In all 3 cases, hepatocytes were largely replaced by fibrous connective tissue, and there was no evidence of active secondary infection. Considering the presence of hemorrhage, congestion, and less extensive fibrosis, cases 2 and 3 were likely less chronic than case 1. Animals with hepatic lobe torsion often have nonspecific clinical signs, including inappetence, weight loss, elevated heart and respiratory rates, and abdominal pain. In these camels, no clinical signs were reported during antemortem examination. Blood examination was performed only in case 3, and the lack of elevation of liver enzyme activity in that case likely reflects the chronicity of the lesion.
The nature of the material in the space of Disse in the non-affected liver of cases 2 and 3 was not determined. Although this material was negative with Congo red staining, and hepatic amyloidosis has apparently not been reported in a camelid, its location and appearance are most suggestive of amyloid. Further characterization to rule out amyloid, including thioflavin T staining, electron microscopy, and immunohistochemistry for immunoglobulin light chains, was not pursued.
Footnotes
Acknowledgements
We thank the deanship of scientific research at the King Faisal University for support. We thank Tawfik Aboellail, John Cullen, and Eunju Choi for consultations.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was financially supported by the deanship of scientific research at the King Faisal University under Nashir Track (grant 186103).