
Abstract
A 5-y-old female Golden Retriever was presented with a 2-wk history of hyporexia, vomiting, diarrhea, lethargy, weight loss, polyuria, and polydipsia. Clinical examination and ultrasonography revealed multiple organ enlargement with gallbladder and kidney nodules suggestive of disseminated neoplasia. Hematologic and biochemical analyses revealed pancytopenia, hypercalcemia, and monoclonal IgA gammopathy suspicious for a plasma cell neoplasm. Bone marrow and blood smear examination revealed neoplastic atypical cells highly suggestive of lymphoid origin. Autopsy confirmed the presence of homogeneous white masses and multifocal pale infiltrates in the spleen, kidney, small intestine, gallbladder, and urinary tract. Histologic features were consistent with a multicentric atypical plasma cell tumor. Tumor cells were negative for CD204, IBA-1, E-cadherin, CD3, CD5, CD79a, CD20, and PAX5, and positive for MUM1, consistent with plasma cell origin. The presence of > 20% of circulating blastic plasma cells was consistent with primary plasma cell leukemia with plasmablastic morphology, a disease rarely described in veterinary medicine.
A 5-y-old spayed female Golden Retriever was presented to the Oniris Veterinary Teaching Hospital (Nantes, France) with a 2-wk history of hyporexia, vomiting, diarrhea, lethargy, weight loss, polyuria, and polydipsia. On physical examination, the dog was 5% dehydrated, had moderate tachycardia at 160 beats/min, and hyperthermia with 39.2°C rectal temperature. A cranial abdominal mass was detected on palpation, and abdominal ultrasound confirmed the presence of a 2-cm mass on a diffusely enlarged spleen. Ultrasound examination also revealed bilateral effacement of the renal corticomedullary junction with depressed and hyperechogenic foci in the cortex, and severe irregular thickening of the gallbladder wall. These findings were suggestive of multifocal-to-diffuse neoplasia. Survey skeletal radiographs did not reveal any abnormalities.
Biochemical analyses on serum (RX-Daytona; Randox Laboratories, Crumlin, County Antrim, UK) revealed marked hyperproteinemia (115 g/L; reference interval [RI]: 60–80 g/L) with severe hyperglobulinemia (90 g/L; RI: 25–45 g/L) and slight hypoalbuminemia (25 g/L; RI: 28–45 g/L), marked hypercalcemia (total calcium >4 mmol/L, RI: 2.2–2.7 mmol/L; ionized calcium = 1.95 mmol/L, RI: 1.13–1.38 mmol/L) as well as moderately elevated creatinine (221 µmol/L; RI: 35–105 µmol/L) with normal urea (9.3 mmol/L; RI: 3.6–10.0 mmol/L). Urine collected by cystocentesis had low specific gravity (1.012) without any other significant abnormality, and normal urine protein-to-creatinine ratio of 0.2 (RI: 0–0.5). The biochemistry results suggested an inflammatory process, polyclonal or monoclonal gammopathy, malignant hypercalcemia, primary or secondary hyperparathyroidism, and renal disease.
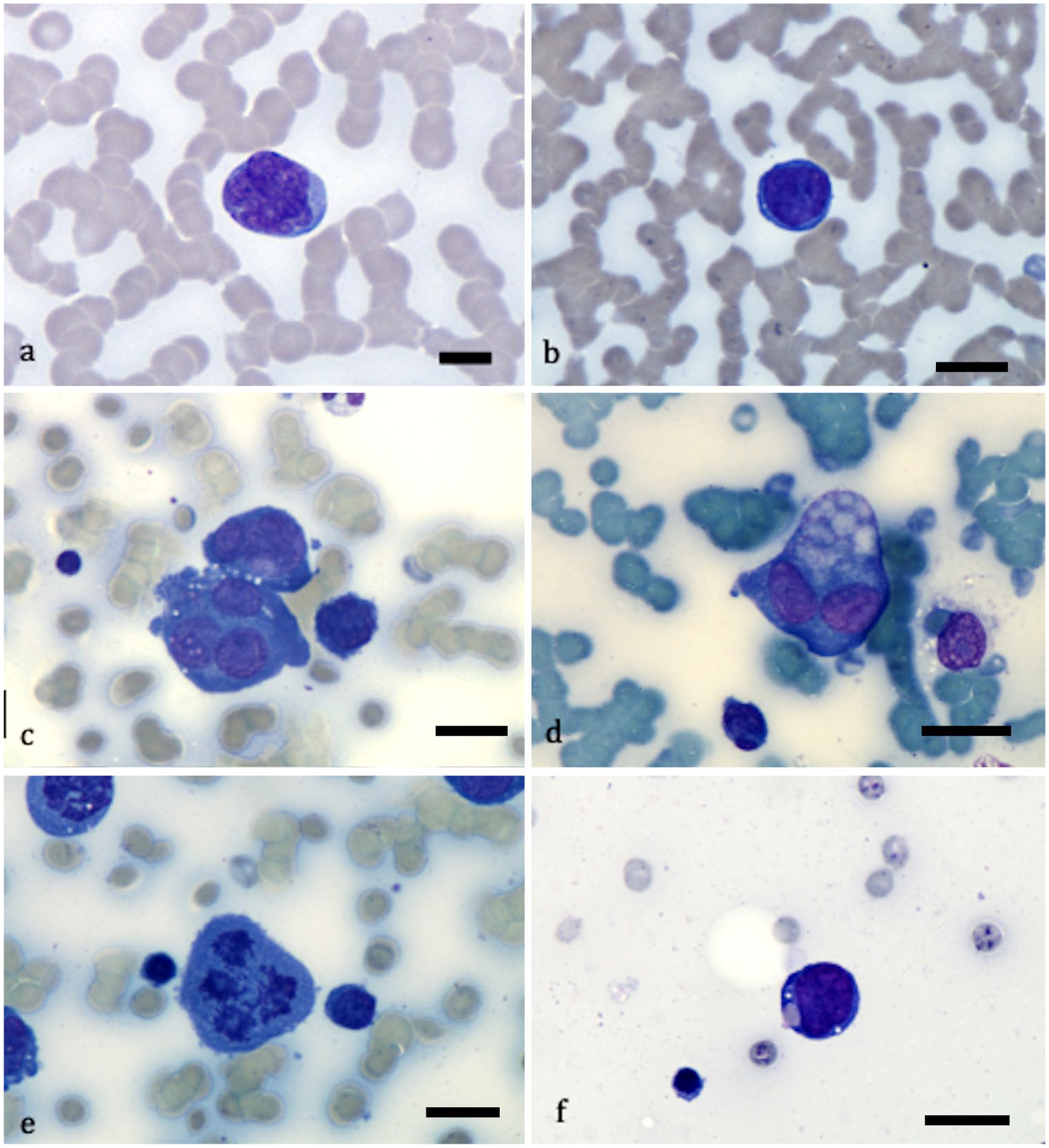
A complete blood cell count (Procyte Dx; IDEXX Laboratories, Westbrook, ME) indicated pancytopenia with moderate normocytic, normochromic nonregenerative anemia (hemoglobin = 84 g/L, RI: 120–180 g/L; hematocrit = 0.25 L/L, RI: 37–55 L/L; mean corpuscular volume = 63.3 fL, RI: 60.0–77.0 fL; mean corpuscular hemoglobin concentration = 21.1 pg, RI: 19.5–24.5 pg; reticulocytes = 33.0 × 109/L, RI: 0.0–80.0 × 109/L), marked thrombocytopenia (platelets = 25 × 103/µL; RI: 200–500 × 103/µL), and leukopenia (white blood cells = 2.8 × 109/L; RI: 6–17 × 109/L). There was marked neutropenia (mature neutrophil count = 1.0 × 109/L; RI: 3.0–11.5 × 109/L) without toxic change. The blood smear had marked rouleaux formation that dispersed upon saline dilution. Atypical immature cells were observed and represented 23% of the total nucleated cells on a differential count of 200 nucleated cells. These atypical cells consisted of large (20–30 µm) round cells with a high nuclear-to-cytoplasmic ratio, round-to-convoluted nuclei with a finely stippled chromatin pattern, infrequent nucleoli, distinct borders, and basophilic cytoplasm. Anisokaryosis and anisocytosis were moderate. Morphologic characteristics were highly suggestive of atypical lymphoid cells compatible with plasmablasts 12 (Fig. 1).
Blood (
Slides from an iliac bone marrow aspirate taken with an 18-g (3.8-cm) Illinois needle (CareFusion, Coveto, France) were prepared and stained with May-Grünwald/Giemsa. Smears were hypocellular with multi-lineage hypoplasia but a progressive and complete maturation process in all cell lines. The myeloid-to-erythroid ratio was low (0.9), as were iron stores. Almost 11% of the cells on a multi-field 400 total nucleated cell count were similar to those observed in the peripheral blood, and had marked atypia including marked anisocytosis and anisokaryosis, frequent multinucleation, and abnormal mitotic and phagocytic activity with engulfed red blood cells and platelets (Fig. 1).
Serum protein electrophoresis (Hydrasys 2, Hydragel; Sebia, Evry, France) was performed on the previously collected serum and suggested a monoclonal gammopathy in the β region (Fig. 2). This was confirmed by serum immunoelectrophoresis (Hydragel IEP; Sebia; specific canine antisera provided by Bethyl Laboratories, Montgomery, TX) that demonstrated a monoclonal IgA hypergammaglobulinemia with a monoclonal increase in light chains and a marked decrease in IgG and IgM (Fig. 3).
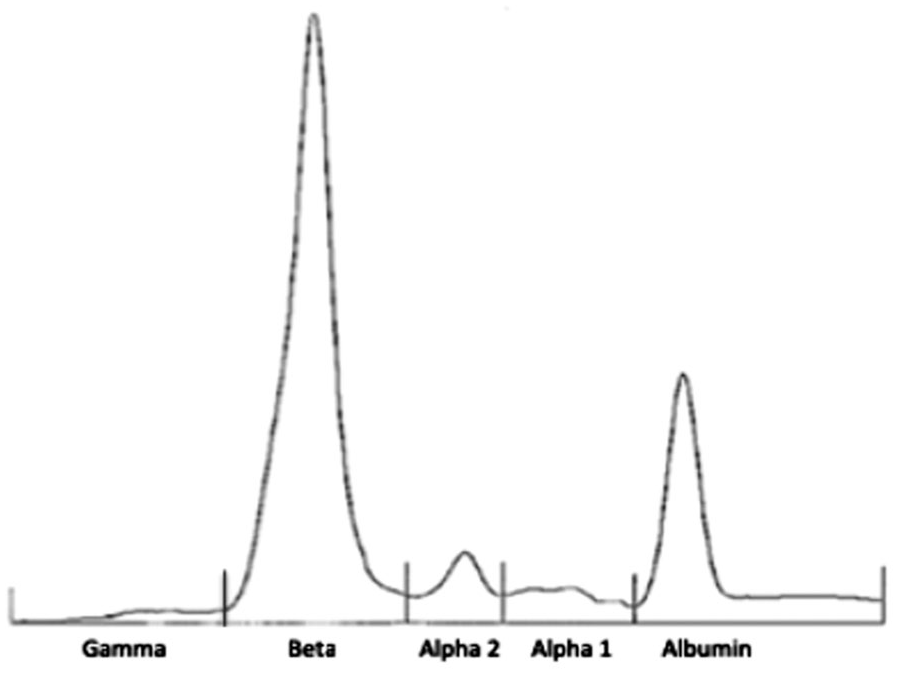
Serum protein electrophoresis in a 5-y-old Golden Retriever. A narrow peak in the beta region indicates monoclonal gammopathy.
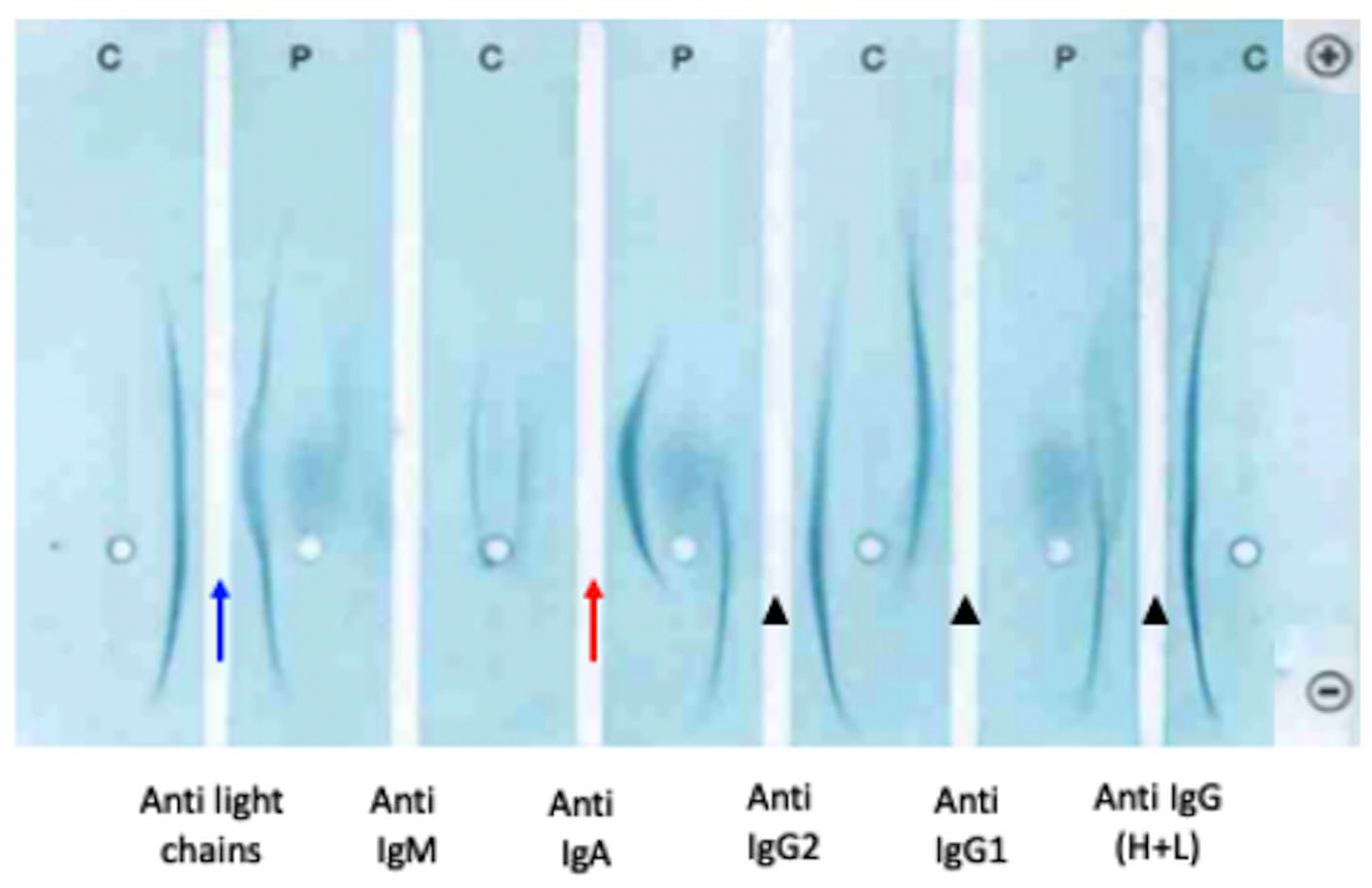
Serum protein immunoelectrophoresis in a 5-y-old Golden Retriever. Specific antisera were loaded in corresponding channels. In the anti-IgA column (red arrow), the presence of a thick arch for the patient versus the absence for the control indicates monoclonal IgA gammopathy. The patient arch in the anti–light chains column (blue arrow) is thickest and closer to the central strip than the control, suggesting increased production of light monoclonal chain, as well. However, all arches in the anti-IgG columns (arrowheads) are absent or lighter for the patient, which is consistent with decreased production of these immunoglobulins. C = control serum; P = patient serum.
Given the results described above, we considered monoclonal IgA gammopathy of neoplastic origin with blood, bone marrow, and visceral involvement to be likely. Differential diagnoses included stage V lymphoma, multiple myeloma with secondary plasma cell leukemia, or primary plasma cell leukemia. Other neoplasms such as acute lymphoid and myeloid leukemia or histiocytic sarcoma with concurrent monoclonal gammopathy were considered less likely. In addition to symptomatic and supportive care, patient therapy included broad-spectrum antibiotics, bisphosphonates, and a chemotherapeutic combination of melphalan and prednisolone. The dog was discharged a few days later; however, 2 wk later, the owners elected euthanasia given the progressive decline in the dog’s clinical picture.
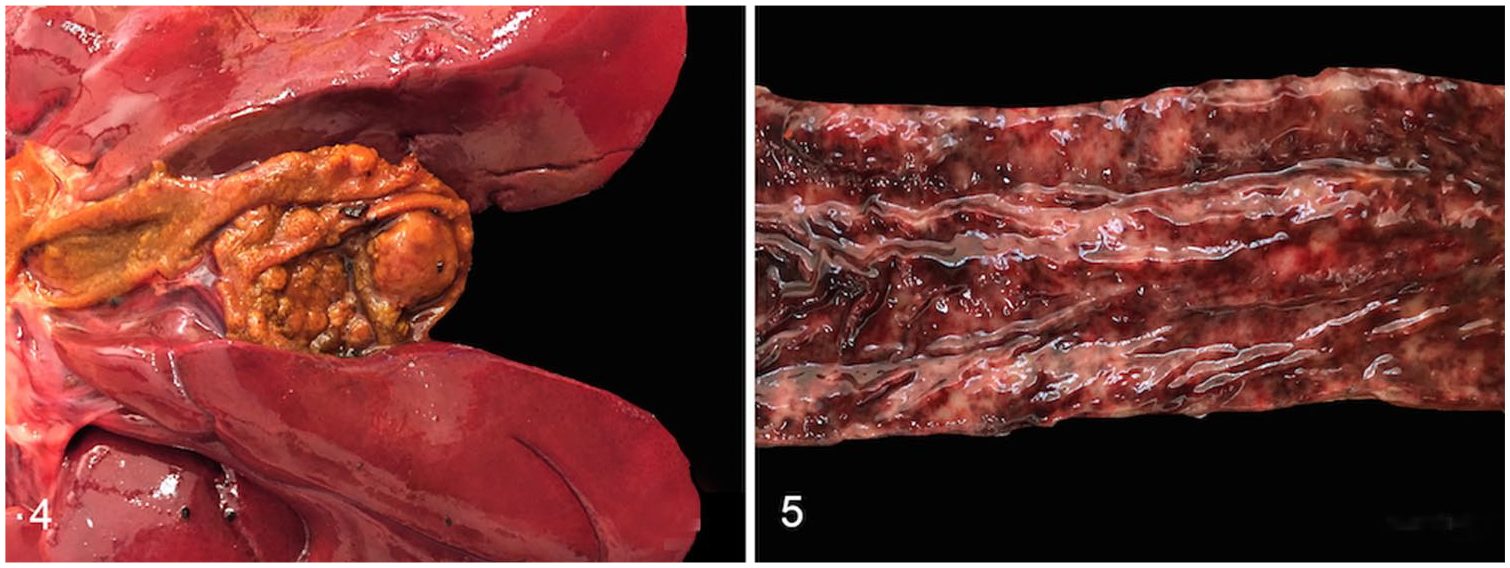
An autopsy was performed 2 h after euthanasia. Firm white 0.1–4-cm masses were observed in the spleen, gallbladder wall (Fig. 4), intestinal serosa, and kidneys. Many of these masses had hemorrhagic foci. The spleen, mesenteric and pancreatic lymph nodes, mucosae of the stomach, urinary bladder, and intestines were abnormally pale, and markedly and diffusely thickened (Fig. 5). Other significant gross lesions included severe, acute, multifocal-to-diffuse colonic and urinary bladder mucosal hemorrhage (Fig. 5), chronic bilateral renal infarcts, and mild diffuse hepatomegaly.
Samples of spleen, liver, gallbladder, stomach, intestines, kidney, lymph nodes, pancreas, and bone marrow were fixed in 10% neutral-buffered formalin, processed routinely, and sections stained with hematoxylin–eosin–saffron. Histologic examination revealed a densely cellular, nodular-to-diffuse, poorly demarcated neoplastic cell population invading and replacing the red and white pulp in the spleen, the intestinal mucosa and serosa, the gallbladder wall, the urinary bladder and gastric mucosa, the cortex of the kidney, the cortex and medulla of the mesenteric and pancreatic lymph nodes, the periportal areas of the liver, and multifocally throughout the bone marrow. Tumor cells were arranged in sheets of round, large cells, 20–40 µm diameter, with a high nuclear-to-cytoplasmic ratio, a thin rim of eosinophilic cytoplasm, and a round-to-folded eccentric nucleus with finely stippled chromatin and usually one, medium-sized, basophilic nucleolus (blastic appearance). Anisocytosis, anisokaryosis, and nuclear pleomorphism were marked, with numerous multinucleate cells, and tumor cells displaying erythrophagocytic activity. Mitotic index was > 30 mitoses per 3.07 mm2. Tumor cell morphology differed between organs, for example, the blastic appearance of neoplastic cells was more evident in the kidneys (Fig. 6); erythrophagocytic activity and multinucleate giant cells were particularly prominent in the small intestine, urinary bladder mucosa, and mesenteric lymph node (Fig. 7). Postmortem bone marrow examination revealed multifocal-to-diffuse infiltration of neoplastic cells with mild trabecular osteolysis. Based on the described histologic changes, postmortem findings corroborated the hypothesis of a monoclonal IgA gammopathy of neoplastic origin with blood, bone marrow, and visceral involvement.
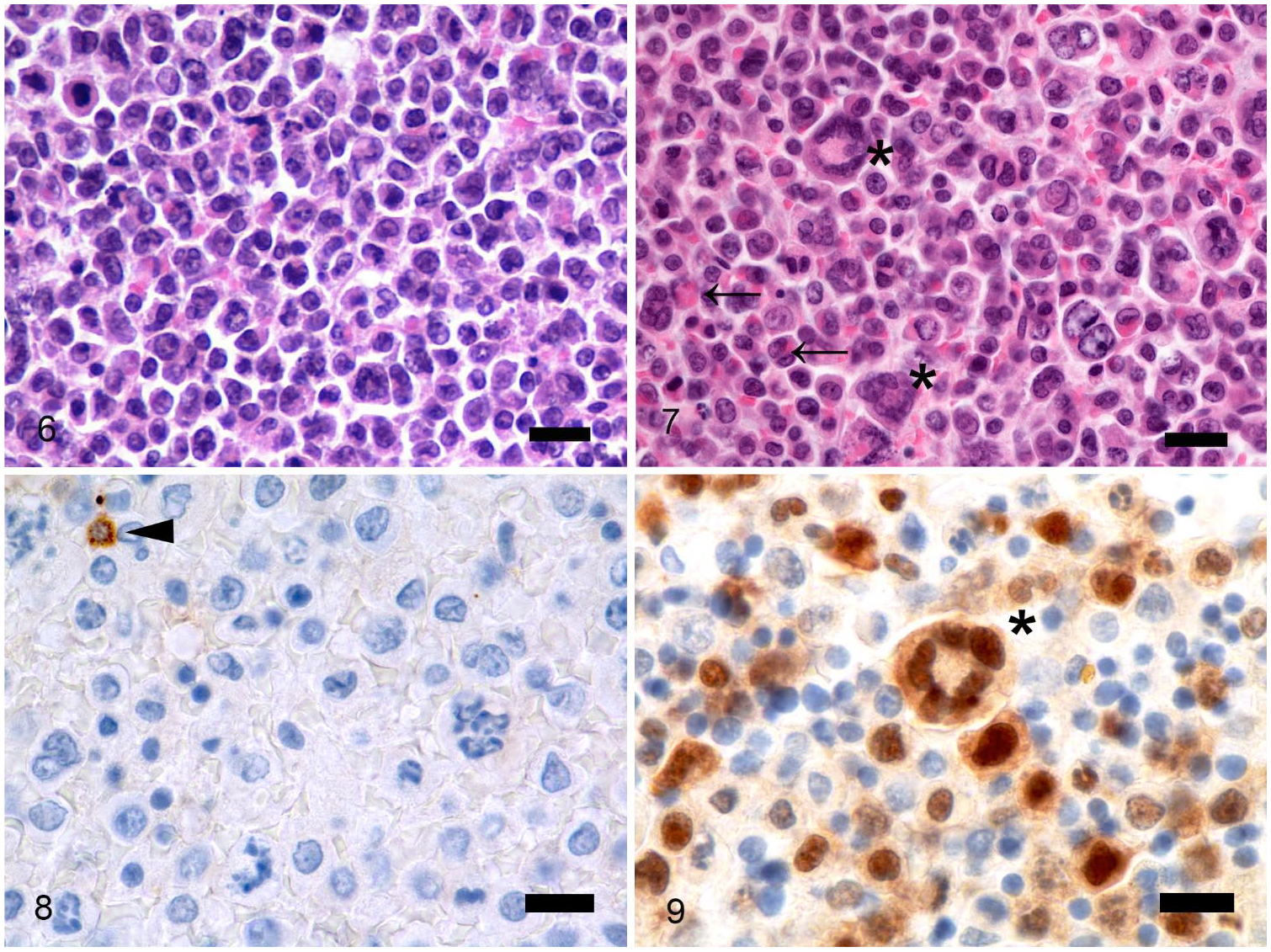
Light microscopic images of multi-organ tumor infiltration in a 5-y-old Golden Retriever.
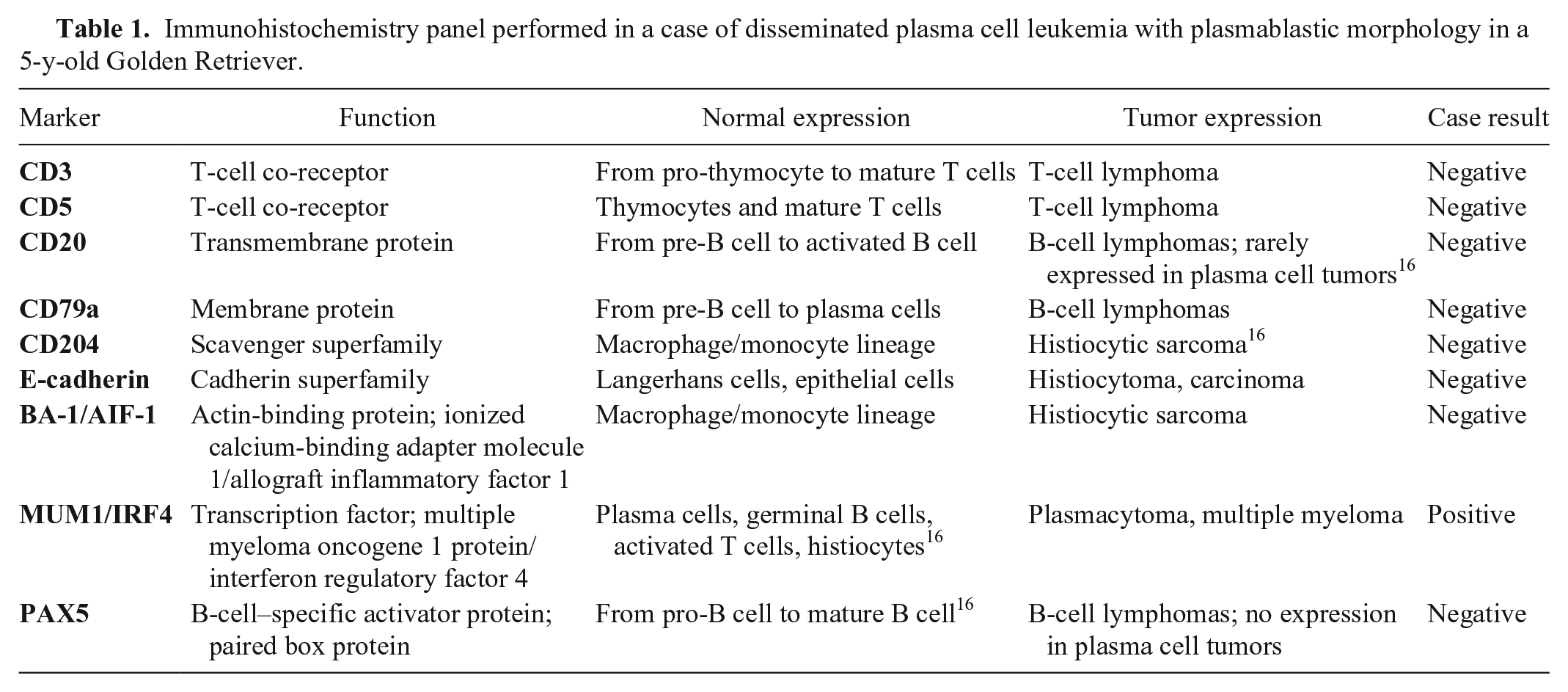
A complete immunohistochemistry (IHC) panel (Table 1, Supplementary Table 1) was performed on deparaffinized sections (Benchmark Discovery XT, DAB detection system; Ventana Medical Systems, Roche Diagnostics, Tucson, AZ). Primary antibodies used were anti-CD204 (clone SRA-E5; Abnova, Taipei, Taiwan), anti–E-cadherin (clone 4A2; Cell Signaling, Danvers, MA), anti–IBA-1 (clone EPR16588; Abcam, Cambridge, UK), anti-PAX5 (clone SP34, Spring Biosciences, Pleasanton, CA), anti-CD79a (clone HM57; Dako, Waltham, MA), anti-CD20 (polyclonal PA5-16401; Thermo Fisher, Rockford, IL), anti–MUM1 (clone MRQ-43; Ventana), anti-CD3 (clone 2GV6; Abnova), and anti-CD5 (clone SP19; Spring Biosciences). Histiocytic and Langerhans cell origin of the tumor was ruled out given negativity for CD204, E-cadherin, and IBA–1.13,15 The tumor was also negative for common B-cell markers (CD79a, CD20, and PAX5), which are rarely expressed in plasma cells 16 (Fig. 8). Labeling for CD3 and CD5 was not observed, excluding a T-cell origin. Plasmacytic origin of the tumor cells was confirmed by the nuclear expression of MUM1 in the spleen (90% positivity) as well as in the bone marrow (39% positivity; Fig. 9). PARR (PCR for antigen receptor rearrangements) was performed with protocols and primers previously published and validated in formalin-fixed, paraffin-embedded tissues.1,4,21,27 PARR confirmed that the tumor was negative for both B and T clonality as previously reported in canine plasma cell tumors.20,25
Immunohistochemistry panel performed in a case of disseminated plasma cell leukemia with plasmablastic morphology in a 5-y-old Golden Retriever.
Combining morphologic and immunophenotypic observations, our final diagnosis was disseminated plasma cell neoplasm at the leukemic stage. Taking into consideration the plasmablastic morphology of the cells, plasma cell leukemia (primary or secondary to multiple myeloma) and plasmablastic lymphoma at leukemic stage were the 2 differentials.
In human medicine, a lymphocyte-derived neoplasm named plasmablastic lymphoma can have an overlapping morphology and immunophenotype with plasma cell leukemia when exhibiting plasmablastic morphology. These neoplasms can both reach a leukemic stage and are nearly impossible to distinguish using morphologic criteria alone.2,3,5,7,18 This overlap is further complicated by virtually identical immunophenotypic profiles, even when an exhaustive panel of immunomarkers is used. 20 In agreement with previous studies, plasmablastic lymphomas have a post-germinal center B-cell/plasma cell phenotype, expressing MUM1/IRF4 and CD138/syndecan-1, but not CD20,3,24,26 unlike other large B-cell lymphomas that usually express the pan-B cell antigens, CD20, CD79a, and PAX–5.8,22 In these studies, several markers that may be aberrantly expressed in plasma cell neoplasms (i.e., CD56, CD10, and CD4) were also expressed in most cases of plasmablastic lymphoma. In veterinary medicine, plasmablastic lymphoma, a rare variant of aggressive B-cell lymphoma, was reported to be CD20-positive and less often CD79-positive. 23 For all of these reasons, an IgA-producing plasmablastic lymphoma was considered unlikely in this dog.
Plasma cell leukemia is very rarely described in the veterinary literature, with only 2 cases reported, to our knowledge: 1 with a similar presentation that had IgG production, and the other suspected to have a cutaneous plasmacytoma origin.6,17 In human medicine, plasma cell leukemia is the most aggressive presentation of the plasma cell neoplasms and is characterized by circulating plasma cells > 2 × 109/L or 20% of the leukocyte differential count. 19 Primary plasma cell leukemia is a malignant proliferation of plasma cells first diagnosed in the leukemic phase; secondary plasma cell leukemia corresponds to the leukemic transformation of primary underlying multiple myeloma.9,19 In our case, using human and canine criteria for the differential diagnosis, many features were more consistent with primary plasma cell leukemia than leukemic multiple myeloma. The high tumor burden and >20% circulating neoplastic cells at the time of the dog’s initial presentation is more consistent with primary plasma cell leukemia than with leukemic multiple myeloma. This is important, given that a 2017 article concluded that the prognosis between plasma cell leukemia and multiple myeloma was similar when circulating plasma cells were > 5%, 11 raising the question of the blood threshold for the diagnosis of plasma cell leukemia.
Interestingly, the degree of bone marrow involvement, defined as the percentage of neoplastic cells among all nucleated cells, is not considered a criterion for the diagnosis of plasma cell neoplasm, even with leukemic disease. Indeed, the 2017 World Health Organization classification of Tumors of Hematopoietic and Lymphoid Tissues defined that plasma cell myeloma, even when symptomatic, may have < 10% neoplastic plasma cells in bone marrow aspirate smear differentials. 19 In our patient, the discrepancy between the percentage of neoplastic cells in the bone marrow when based on morphologic observation (11%) and when based on IHC (39%) illustrated a potential lack of sensitivity of cytologic examination alone for the identification of bone marrow neoplastic disease involvement. This discrepancy could be explained by the focal distribution of the neoplastic cells and/or by the time delay between bone marrow aspiration and autopsy.
The median patient age at diagnosis for plasma cell leukemia is reported to be younger than for myelomas: multiple myeloma usually affects dogs 8–12 y old, 14 whereas our patient was 5 y old. In plasma cell leukemia, the bone marrow is usually extensively and diffusely infiltrated, and neoplastic plasma cells are frequently found in extramedullary sites with massive organomegaly (e.g., liver, spleen, or lymph nodes), as we observed in our case. Our case had only mild microscopic osteolytic lesions; lytic bone lesions are less commonly reported in plasma cell leukemias compared to multiple myeloma. Better response to therapy with longer survival is reported in multiple myeloma (930 d under therapy) 10 compared to plasma cell leukemic patients.9,19 The dog in our case had a short clinical course pre-diagnosis, and survived only 15 d after diagnosis, despite prompt initiation of therapy.
Supplemental Material
Supplemental_material – Supplemental material for Plasma cell leukemia with plasmablastic morphology in a dog
Supplemental material, Supplemental_material for Plasma cell leukemia with plasmablastic morphology in a dog by Elie Dagher, Nicolas Soetart, Florian Chocteau, Bérengère Dequéant, Esther Piccirillo, Catherine Ibisch, Jérôme Abadie and Laëtitia Jaillardon in Journal of Veterinary Diagnostic Investigation
Footnotes
Acknowledgements
We thank the following technicians for their contribution: Bernard Fernandez, Florence Lezin, Anabelle Ravet, and Hélène Gautier. We also acknowledge Michelle Moughaizel, Gabrielle Callanan, and Cyril Parachini-Winter for revising the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.