
Abstract
A mature male grizzly bear (Ursus arctos) that died of blunt-force trauma had numerous hard 1–3-mm nodules protruding from tracheal rings into the lumen of the distal trachea. Histologically, these were round aggregates of mature cartilage within the submucosa. Such lesions are consistent with tracheobronchopathia osteochondroplastica, a rare tracheal disease in humans and animals.
In October 2017, a mature male grizzly bear (Ursus arctos) was found dead adjacent to a highway in Glacier National Park, British Columbia, Canada. It was stored frozen until April 2018 when park officials submitted it to the Alberta Region of the Canadian Wildlife Health Cooperative, University of Calgary, for an autopsy. The bear was in excellent nutritional condition with abundant subcutaneous and visceral fat stores. The cause of death was severe blunt-force trauma (likely vehicular) with the presence of multiple acute fractures of the ribs, limbs, and skull.
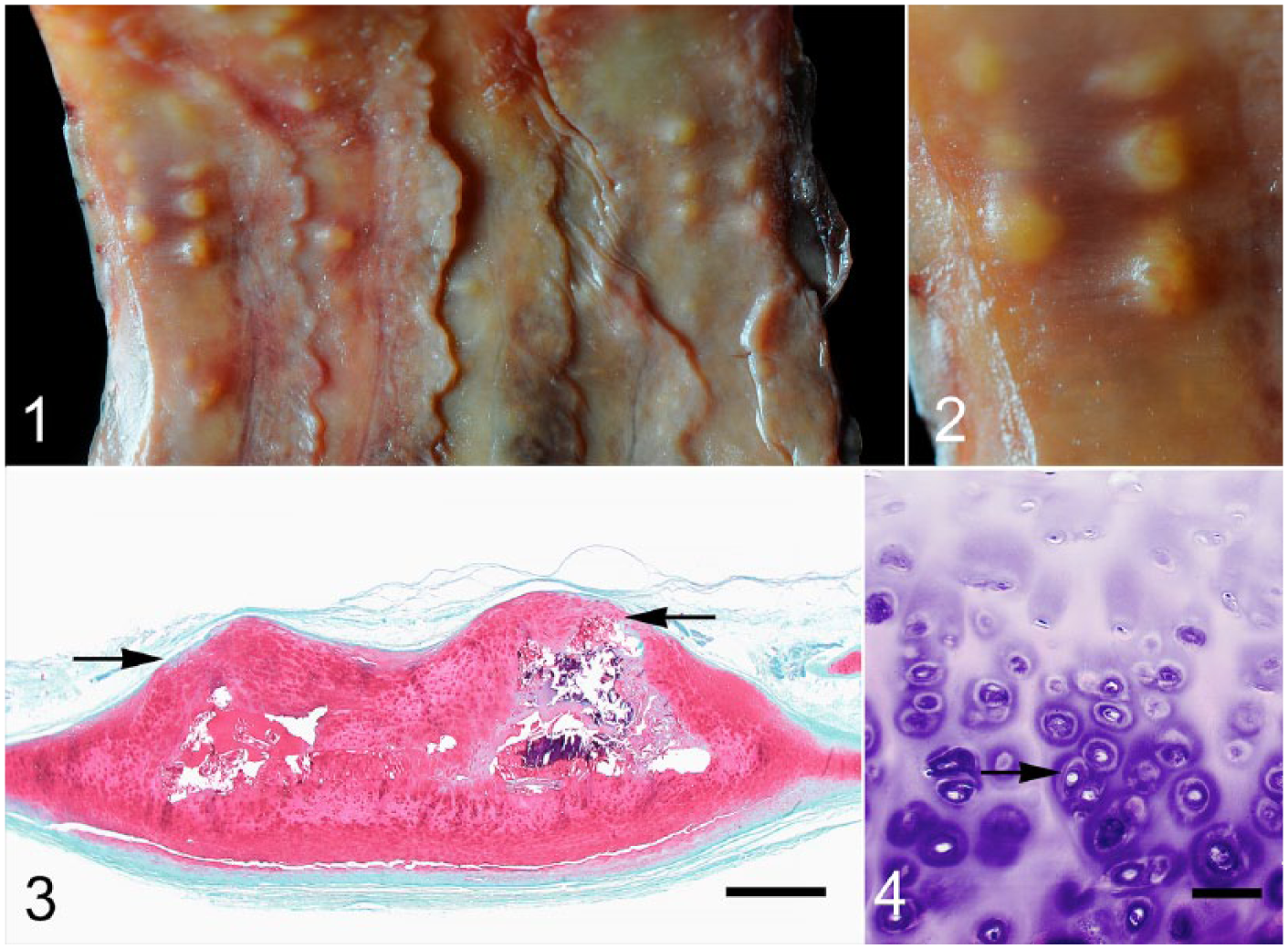
Within the lateral and ventral portions of the distal trachea and tracheal bifurcation, there were ~30–40, 1–3-mm hard tan nodules that protruded into the tracheal lumen (Fig. 1). These nodules were often associated with and arising from tracheal rings. Intact mucosa covered the nodules (Fig. 2). Samples of tracheal lesions and lung were fixed in 10% neutral-buffered formalin for 48 h prior to being processed routinely. Sections were stained with hematoxylin and eosin and Safranin O stains. Histologically, the nodules corresponded to focal, round, well-demarcated thickening of the tracheal cartilage that elevated the mucosa (Fig. 3). Nodules consisted of chondrocytes with moderate anisocytosis that were arranged haphazardly, either individually or in clusters of 2–4 cells within lacunae surrounded by moderate amounts of basophilic matrix (Fig. 4). Central portions of the nodules and tracheal cartilage adjacent to nodules, as well as in unaffected areas, were mineralized. There was no evidence of osseous metaplasia, bone marrow, or mitotic figures in any of the nodules examined. Although moderately autolyzed, there were no histologic abnormalities in the lungs.
Tracheobronchopathia osteochondroplastica in the trachea of a male grizzly bear (Ursus arctos).
Based on macroscopic appearance and histopathology, the tracheal nodules are consistent with tracheobronchopathia osteochondroplastica (TO). First described in people in 1857, these tracheal lesions are rare and progressive, characterized by firm cartilaginous nodules often arising from the tracheal rings. 8 In humans affected by this condition, the classical lesion includes nodules of submucosal cartilage that may mineralize and/or ossify. In some cases, there is squamous metaplasia of the overlying epithelium and the presence of bone marrow in the ossified foci. 1 Osseous metaplasia, hematopoietic bone marrow, and squamous metaplasia were not present in this bear. Lesions in humans occur in the ventral and lateral areas along the entire length of the trachea from the larynx to the primary bronchi 4 ; the lesions in this bear similarly affected the ventrolateral areas but were restricted to the distal portion of the trachea.
Other potential differential diagnoses for tracheal nodules include neoplasia, parasites (e.g., Oslerus osleri in canids), and granulomas. These are ruled out with histopathology. The pathogenesis of TO is unknown; however, connective tissue metaplasia and benign cartilage hyperplasia (ecchondrosis) are proposed causes. 1
The effect of these lesions on the bear’s overall health is unknown, given that this condition is exceedingly rare in animals. However, these lesions are most likely an incidental finding. TO was described previously in a pony that suffered from a ruptured trachea, although it is not clear if the TO lesions caused the rupture or if the lesions were an incidental finding. 7 A case of TO in a dog was associated with exercise intolerance, tracheitis, and tracheal collapse. 6 In humans, TO is often diagnosed incidentally during autopsy examination. Lesions may also be discovered during bronchoscopic examinations and/or computed tomography (CT) scans undertaken as part of a workup for chronic respiratory diseases such as persistent cough or for unrelated conditions. 1 Indeed, in one case series, 85% of human patients diagnosed with TO had a history of respiratory clinical signs. 4 Clinical signs associated with TO range from none to variable nonspecific signs that include cough, dyspnea, hemoptysis, chest pain, and exercise intolerance. 1 As space-occupying lesions, TO can result in narrowing of the tracheal lumen and reduced airflow in affected humans.1,4
Human-associated causes of mortality are considered the most important cause of death in grizzly bears2,5; however, there is little information on the role underlying disease may have in these fatal interactions. Given the excellent body condition of the bear, the large diameter of the bear’s trachea, and the diminutive size of these nodules, their effect on respiratory function was likely minimal, and given that lesions are progressive in people, 4 it is possible that growth in size and number may have been expected in this bear, which could have impaired respiration had it lived longer.
TO is likely an underdiagnosed condition in veterinary species, including wildlife. This case affirms the importance of thorough autopsy examinations in wildlife to uncover background and ongoing disease processes given that understanding underlying disease may provide insight into trauma-related mortality in bears and other wild animals. 3
Footnotes
Acknowledgements
Thanks to Blair Fyten and Tawnya Hewitt of Parks Canada for submitting this case, Susan Calder-Lodge and Jim Carlsen for technical support, and Melencio Nicolas and Paul Gajda for assistance with gross lesion photography. This work was supported by the University of Calgary Diagnostic Services Unit and the Canadian Wildlife Health Cooperative.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.