
Abstract
We compared results of a serum immunofluorescence assay (IFA) and lymph node quantitative PCR (qPCR) in dogs classified as exposed, infected, or sick because of leishmaniasis. We also determined how IFA or qPCR results changed in response to treatment and reflected different clinical and clinicopathologic improvement of dogs. We included 108 dogs in our retrospective study: 12 exposed, 25 infected, and 71 sick, as classified according to Canine Leishmaniasis Working Group standards. Between-group comparison showed higher IFA values (p < 0.01) for sick dogs; qPCR values were higher for sick than infected dogs (p < 0.01). A novel clinical and clinicopathologic score was created and applied to 50 sick dogs. Using this score, 41 were reclassified as partially recovered (PR) within 3 mo, and 37 as totally recovered (TR) 3–6 mo after presentation. Statistically significant differences in IFA values were found between the sick and TR dogs (p < 0.01), but not between sick and PR dogs (p = 0.98). During follow-up, qPCR revealed a progressive decrease in parasite load, with a statistically significant difference in sick versus PR (p < 0.01), sick versus TR (p < 0.01), and PR versus TR (p < 0.01) dogs. A decrease of 1 point in the clinical score corresponded to 1.3 Leishmania/μL qPCR decrease (p < 0.01) and decrease of 1:42 in IFA (p < 0.01). Our findings confirm that the clinical status of dogs affected by leishmaniasis is closely related to parasite load and antibody level, both before and after treatment.
Canine leishmaniasis (CanL) is a zoonotic disease caused by the protozoan parasite Leishmania infantum. Dogs are the main peridomestic reservoir for this organism in the Mediterranean basin. Host immune response is the most important factor for efficiently controlling parasite infection. Clinical features of infection vary widely because of the various pathogenic mechanisms involved in the disease process. Diagnosing CanL is extremely challenging as a result of nonspecific clinical presentations.3,11
Two guidelines for clinical classification of infected dogs, proposed by LeishVet 16 and by the Canine Leishmaniasis Working Group (CLWG), 9 can aid in establishing a diagnosis, and correlating infection classes with treatment and prognosis.13,15 The CLWG classification 9 divides dogs into 3 classes (exposed, infected, and sick) based on positive serology, parasitologic analysis, and the presence or absence of clinical signs, including laboratory abnormalities suggestive of leishmaniasis. The guidelines indicate therapeutic protocols and follow-up evaluations but are less clear about how to interpret laboratory test results for monitoring response to therapy and progression of associated chronic diseases such as proteinuric nephropathy and chronic renal failure.8,16 To date, an objective method does not exist to evaluate the clinical and laboratory improvements of dogs after therapy, and to identify early changes compatible with disease recurrence.
The techniques used most commonly in the diagnosis of Leishmania infection are the indirect immunofluorescence assay (IFA), which measures the humoral antibody response, and PCR for direct identification of protozoal DNA in tissues.9,10 Studies have shown correlation of humoral response, clinical status, and tissue parasite density,1,2,5,12,14,18 and have evaluated the ability of ELISA, IFA, or PCR to monitor therapeutic response.2,14,17 If treatment is successful, antibody titer and parasite loads decrease with time; however, contradictory results are reported for early or late declines in antibody titer and its usefulness to monitor treatment.14,17
We compared IFA and quantitative PCR (qPCR) values in dogs in the 3 classification groups: exposed, infected, or sick. We also determined how IFA or qPCR results changed in response to treatment and reflected different degrees of clinicopathologic improvement of dogs. We reviewed the medical records of all dogs examined at our Veterinary Hospital at Turin University (Grugliasco, Torino, Italy), between 2010 and 2015. Dogs included in our study were privately owned, brought to the hospital for suspected Leishmania infantum infection or routine checkup, and had both IFA and qPCR performed.
Our Institutional Ethical and Animal Welfare Committee did not require study approval given the observational nature of the study. The owners of all dogs examined at our hospital had consented to diagnostic procedures proposed by the attending veterinarians.
The clinicopathologic data collected included: physical examination findings, complete blood count (ADVIA 120 hematology, Siemens Healthcare Diagnostics, Tarrytown, NY), biochemical profile and urine protein-to-creatinine ratio (ILAB 300 plus, Clinical Chemistry System, Instrumentation Laboratories, Milan, Italy), serum protein electrophoresis, urinalysis (Multistix 10 SG reagent strips, Siemens Healthcare Diagnostics), and urine sediment analysis.
Testing for L. infantum, including serologic IFA and qPCR assay, was carried out by an external laboratory (Istituto Zooprofilattico Sperimentale of Piemonte, Liguria and Valle d’Aosta, Torino, Italy). Samples for qPCR and cytologic evaluation were obtained by fine-needle lymph node aspiration upon presentation. We included dogs testing positive by IFA or qPCR at the first visit in our study. Based on these test results, the dogs were classified as exposed if they had negative qPCR findings, positive antibody titer, and were clinically normal or did not have clinical signs associated with leishmaniasis. Dogs were classified as infected if they had positive qPCR findings, a positive antibody titer, and were healthy or did not have clinical signs associated with leishmaniasis. Sick dogs had positive qPCR findings, a positive antibody titer, and displayed one or more clinical signs common to leishmaniasis. 9
IFA was performed as described in the World Organization for Animal Health Manual of Diagnostic Tests and Vaccines for Terrestrial Animals. 20 Anti-leishmania antibodies were detected with the use of anti-dog IgG conjugated to fluorescein isothiocyanate (MilliporeSigma, St. Louis, MO).
For the qPCR assay, 1 mL of each lymph node aspirate was centrifuged at 16,000 × g for 5 min. The pellet was resuspended in 100 μL of lysis kit buffer and then processed for total genomic DNA extraction (Illustra tissue and cells genomic prep mini spin kit, GE Healthcare Bio-Sciences, Pittsburgh, PA) according to the manufacturer’s instructions. Three replicates of 6 DNA concentrations (103/μL–109/μL) in 10-fold serial dilutions obtained from a culture of L. infantum (MON-1 IPT1; provided by the National Reference Centre for Leishmaniasis, Istituto Zooprofilattico Sperimentale della Sicilia, Palermo, Italy) were used to evaluate the qPCR assay sensitivity and efficiency. The purified DNA concentration was determined by ultraviolet spectrophotometer (GeneQuant Pro, Amersham Biosciences, Buckinghamshire, UK) and normalized to 40 ng/μL. TaqMan probe, PCR primers, master mix concentrations, and thermal profile were used as described previously. 19 DNA samples were amplified in a thermocycler (CFX96 Touch real-time PCR detection system, Bio-Rad, Hercules, CA). All samples were tested in triplicate. A negative control (DNA-free water) and the 6 DNA concentrations were included in each run. The results were expressed as parasites per μL.
All laboratory analyses performed at the initial diagnosis (CBC, biochemical profile, urine protein-to-creatinine ratio and urinalysis, serum protein electrophoresis, IFA, and qPCR) were repeated at subsequent follow-up visits. A novel clinicopathologic score (Table 1) was created and used to score each patient before initiation of therapy and at each visit. 9 This score was based on previously reported scores, and was created to provide a more comprehensive clinical–pathologic assessment.4-7,12 The most common clinical signs reported in the literature as well as laboratory alterations useful for monitoring and prognosis were included, and were assigned a value that increased depending on the severity of change. The score was created to be an objective value at each follow-up, creating a continuous variable based on clinical evaluation. Response to therapy consistent with current guidelines was evaluated for the sick dogs that began treatment. 8 Prophylaxis for sandflies, with synthetic pyrethroids (spot-on or collar) applied every month, was prescribed for all dogs. Treated dogs with partial improvement in clinical signs and laboratory abnormalities, defined as a decrease of 1 score point on ≥50% of the parameters in the novel scoring system, were classified as partially recovered (PR). Dogs with complete regression of clinical signs and laboratory abnormalities defined as when all score parameters in the novel scoring system returned to zero, were classified as totally recovered (TR). Dogs with chronic diseases (e.g., proteinuric nephropathy, chronic renal failure, arthropathy, or permanent ocular disease) were classified as TR although the clinicopathologic score was >0. In these latter cases, the residual clinical signs and laboratory abnormalities composing the clinicopathologic score were related to irreversible injury resulting from chronic illness.
Novel clinicopathologic scoring system for dogs with suspected Leishmania infantum infection.
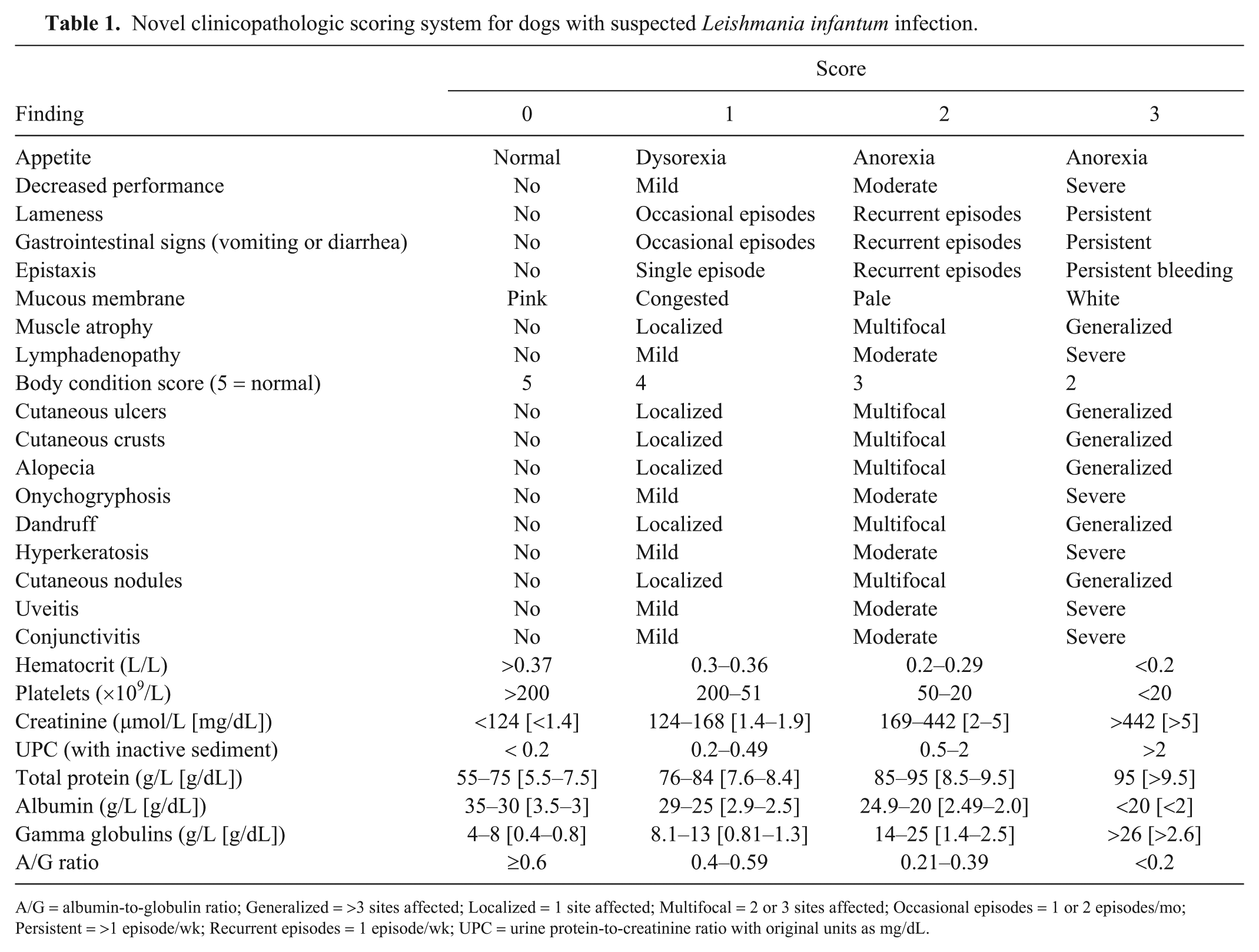
A/G = albumin-to-globulin ratio; Generalized = >3 sites affected; Localized = 1 site affected; Multifocal = 2 or 3 sites affected; Occasional episodes = 1 or 2 episodes/mo; Persistent = >1 episode/wk; Recurrent episodes = 1 episode/wk; UPC = urine protein-to-creatinine ratio with original units as mg/dL.
Statistical analysis was performed (Stata v.14, StataCorp, College Station, TX). An ANOVA was used to compare the results of initial IFA (exposed vs. infected vs. sick) and qPCR values (infected vs. sick), or a Mann–Whitney test when underlying assumptions for an ANOVA were absent. Bonferroni correction was applied to correct for multiple comparisons. To evaluate the effect of treatment and because of repeated measures on the same patient, a quantile multivariate regression model was used to identify a correlation between IFA values and clinical status (i.e., sick, PR, TR), and a random-effects model for panel data was used to identify a correlation between qPCR values and clinical status. A random-effects model for panel data, if the underlying assumptions were met, or a quantile multivariate regression model if not, was used to identify differences in scores between the sick, PR, and TR dogs. A linear regression model was applied to identify correlations between IFA and qPCR in comparison to the clinicopathologic score, without considering the clinical status or patient age (covariates). To compare the IFA and qPCR values before and after treatment in sick dogs, an ANOVA with Bonferroni multiple-comparison correction was used if underlying assumptions were met; if assumptions were not met, then the Mann–Whitney test was applied. Statistical significance was set at 5% (p ≤ 0.05).
There were 108 dogs with positive IFA and/or qPCR that qualified for inclusion in our study. There were 60 males (36 intact, 24 neutered) and 48 females (33 intact, 15 spayed), 1–15 y old (median: 7 y). Breed distribution was 45% mixed-breed, 6% Segugio Italiano, 5% Labrador Retriever, and 44% other breeds. Based on IFA, qPCR, clinical score, and laboratory evaluation at first visit, 12 dogs were classified as exposed, 25 as infected, and 71 as sick (Table 2). There was no significant difference in IFA values between exposed and infected dogs (p = 0.09), whereas IFA values were significantly higher for sick dogs (p < 0.01; Table 2, Fig. 1). Quantitative PCR values were significantly higher in sick dogs compared to infected dogs (p < 0.01; Table 2, Fig. 1).
Indirect immunofluorescence assay (IFA) and quantitative PCR (qPCR) values at presentation of 108 dogs exposed to Leishmania infantum. Dogs were classified as exposed, infected, or sick based on IFA and qPCR results, and on our leishmaniasis clinicopathologic score.
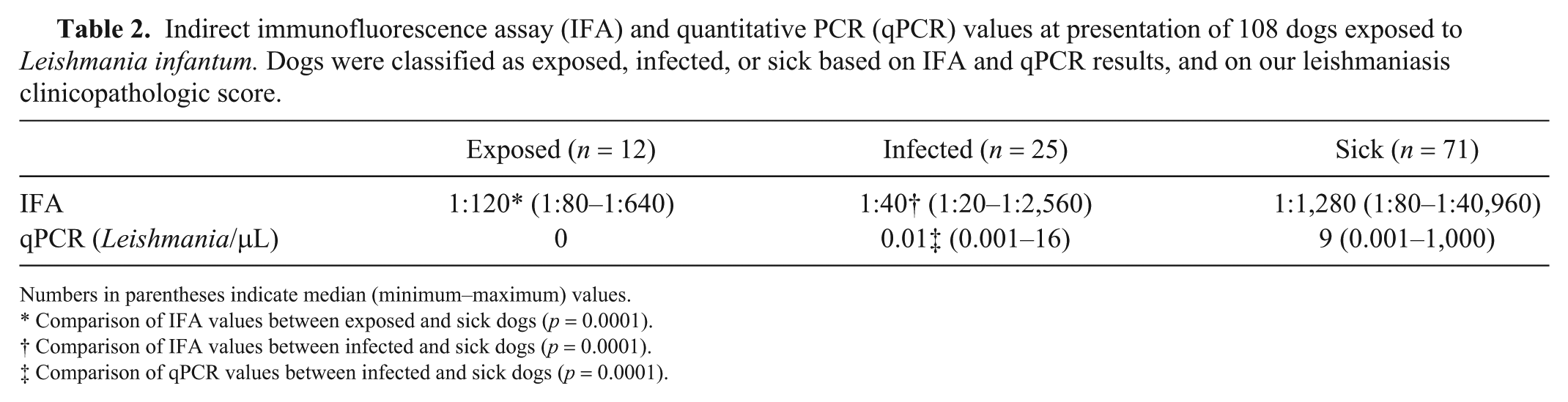
Numbers in parentheses indicate median (minimum–maximum) values.
Comparison of IFA values between exposed and sick dogs (p = 0.0001).
Comparison of IFA values between infected and sick dogs (p = 0.0001).
Comparison of qPCR values between infected and sick dogs (p = 0.0001).
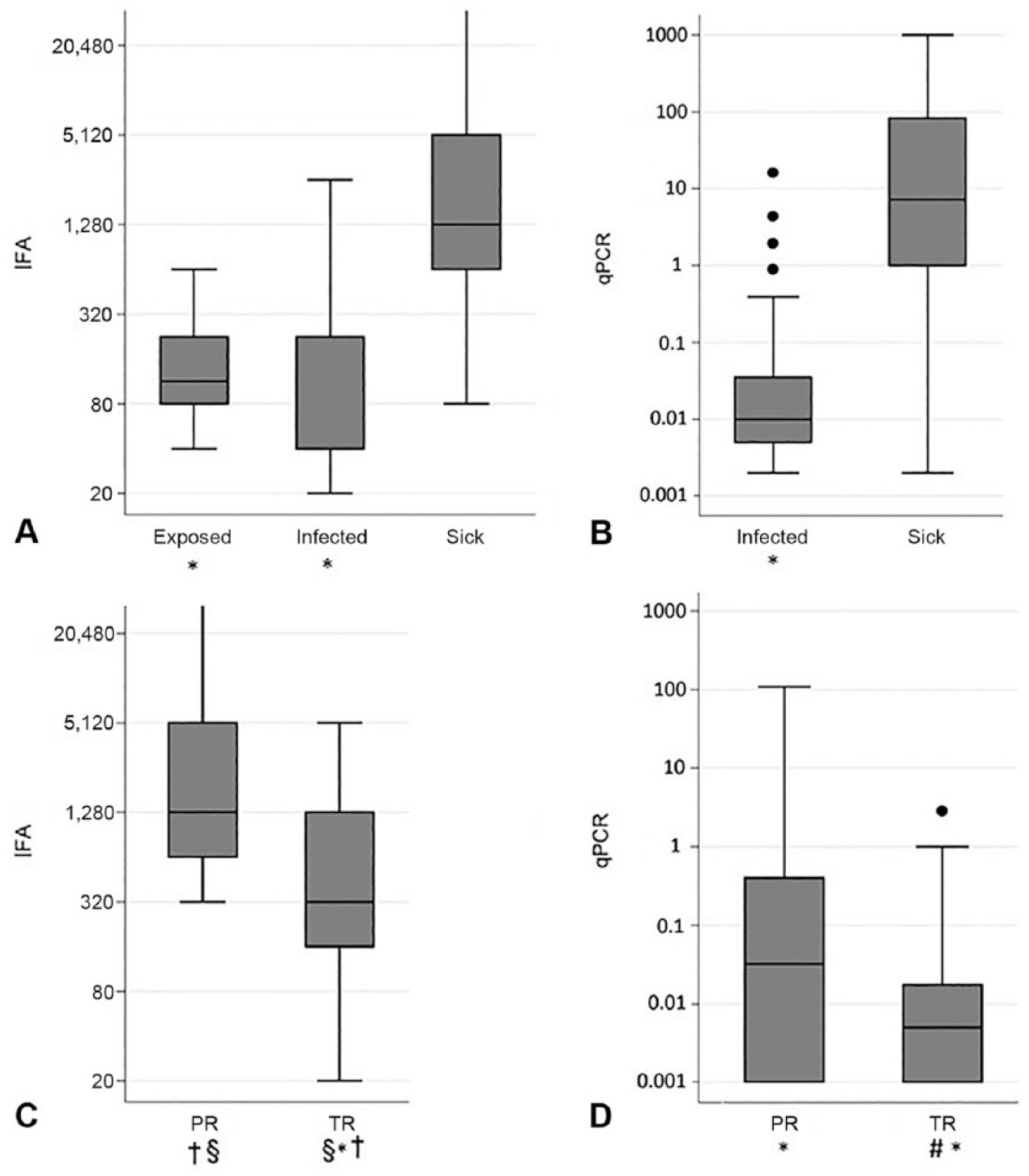
Box plot of the logarithmic distribution of IFA and qPCR values in the 3 groups of 108 dogs at presentation: 12 exposed, 25 infected, 71 sick dogs, and in the 2 subgroups of 50 sick animals following treatment at 2 different times (PR, TR).
Fifty of the 71 sick dogs received treatment: allopurinol alone in 8 of 50, allopurinol and meglumine antimoniate combined in 5 of 50, and allopurinol and miltefosine combined in 37 of 50. Of these 50 sick dogs, 41 were classified as PR at follow-up visit 30–90 d after the end of treatment, and 37 as TR at follow-up visit 90–180 d after completion of treatment (Table 3).
Follow-up indirect immunofluorescence assay and quantitative PCR values of 50 sick dogs infected with Leishmania infantum after treatment. Dogs with chronic disease were classified as “total remission” although the clinicopathologic score was >0, because of irreversible injury resulting from chronic illness.
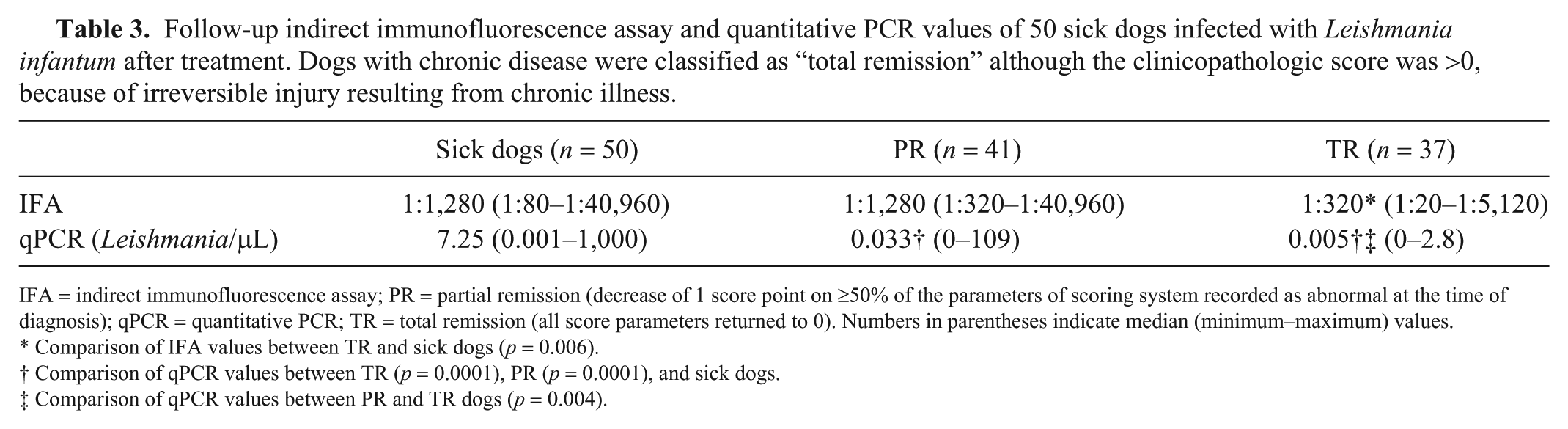
IFA = indirect immunofluorescence assay; PR = partial remission (decrease of 1 score point on ≥50% of the parameters of scoring system recorded as abnormal at the time of diagnosis); qPCR = quantitative PCR; TR = total remission (all score parameters returned to 0). Numbers in parentheses indicate median (minimum–maximum) values.
Comparison of IFA values between TR and sick dogs (p = 0.006).
Comparison of qPCR values between TR (p = 0.0001), PR (p = 0.0001), and sick dogs.
Comparison of qPCR values between PR and TR dogs (p = 0.004).
The quantile multivariate regression model showed statistically significant differences in IFA values among the 3 groups, with lower values for TR dogs than sick (p < 0.01) and PR (p < 0.01) dogs, but no differences between PR and sick dogs (p = 0.98). Analysis of qPCR results by a random-effects model showed a progressive decrease in parasitic load from sick to TR dogs, with a statistically significant difference at every follow-up assessment visit [sick vs. PR (p < 0.01), sick vs. TR (p < 0.01), and PR vs. TR (p < 0.01)].
The linear regression model used to test the relationship between the total score and the IFA and qPCR value showed an inverse linear relation such that a decrease of 1 score point corresponded to an average decrease of 1.3 Leishmania/μL qPCR (p < 0.01) and an average decrease of 1:42 in IFA (p < 0.01). IFA values for PR and TR dogs were higher than those for exposed and infected dogs (PR vs. exposed: p < 0.01; PR vs. infected: p < 0.01; TR vs. exposed: p < 0.05; TR vs. infected: p < 0.01). Quantitative PCR values for the TR dogs were lower than those for infected dogs (p < 0.01), whereas no statistically significant difference in qPCR values was found between PR and infected dogs (p = 0.95; Fig. 1).
As expected, important differences in qPCR and IFA values were found between the dogs classified as sick versus those classified as exposed or infected. Median IFA values were 10 and 30 times higher in sick dogs compared to exposed and infected dogs, respectively, and 16 times higher than the maximum laboratory reference range (IFA 1:80), without overlap between groups (Fig. 1). Despite the marked differences between symptomatic and asymptomatic dogs, some sick dogs were noted to have very low IFA values (1 dog had 1:80 and 2 dogs had 1:160). Because not all dogs seroconvert after infection, 10 a very high antibody titer could be consistent with leishmaniasis, whereas a low titer may need further evaluation to confirm disease, such as the tissue identification of parasites.9,15
The median qPCR value for sick dogs was 900 times greater than that for infected dogs, with minimal overlap between groups at higher values. Dogs with clinical signs suggestive of leishmaniasis have significantly higher parasite loads than infected dogs. As reported in previous studies, parasite load and antibody titer are related to the severity of leishmaniasis and the degree of clinical and pathologic abnormalities.4,12
For the second objective of our study, dogs were reclassified as PR or TR based on clinical and laboratory improvements after therapy. To standardize and objectively evaluate dogs affected by leishmaniasis, the most common clinical signs and laboratory alterations reported in the literature were combined with a numeric value to create a score.9,15 The advantage of this score, compared with those reported previously,4-7,12 is the combination of clinical signs and laboratory alterations typical of leishmaniasis that is applicable in dogs with different clinical presentations, including those without dermatologic signs or with minimal laboratory abnormalities. Reduction in clinical signs corresponded to a significant decrease in parasite load, with an average decrease of 1.3 Leishmania/μL for each point decrease in score. The correlation with qPCR makes the proposed clinicopathologic score useful for monitoring sick dogs, and provides the clinician with an objective tool to measure improvement and suggest a trend in parasitic load.
The dogs with total remission of clinical signs and laboratory abnormalities had significantly lower qPCR values than infected dogs. After treatment, a marked decrease in parasite load usually indicates effective control of disease but not parasitologic cure in Leishmania infection, because most dogs remain infected for life. Even dogs with a qPCR of zero can have fluctuations in parasite burden over time (data not shown).2,8 However, a progressive increase in parasite load detected at the follow-up visit by serial monitoring of qPCR could potentially identify a dog at risk of relapse. Further studies to evaluate this possibility are warranted.
There was also a direct correlation between antibody level and clinicopathologic score, with an average decrease of 1:42 of IFA for each score point. It has been reported that a decrease in parasite load is revealed early by PCR assay in dogs responding to treatment, whereas antibody titers have demonstrated contrasting results. Some studies have found that it is not useful to monitor antibody levels soon after treatment because a significant decrease is seen only after 6 mo. A 2016 article reported a considerable decrease in ELISA titer as early as 30 d of therapy in dogs treated with meglumine antimoniate and allopurinol. 17 Our study showed no difference in IFA values between sick and PR dogs, although the TR dogs had a significantly lower antibody level than either of the other 2 groups. We also noted that the antibody level took time to decrease after treatment. Our findings may differ because we used a different method to measure the IgG antibody level (IFA vs. ELISA), and the majority of our dogs were treated with miltefosine, which can take longer to result in clinical improvement. 6
Our study has several limitations, including its retrospective design with incomplete follow-up data (not all sick dogs could be classified as PR or TR), multiple therapeutic regimens, and non-standardized follow-up examination after completion of therapy. Another limitation is the lack of long-term data on how many PR dogs reached TR status, at what time, and how many relapsed.
Our findings indicate that the clinical and pathologic status of dogs affected by leishmaniasis is closely related to parasite load and antibody level both before and after treatment. However, a decrease in the clinicopathologic score in PR dogs was associated with a significant decrease in qPCR values, whereas a difference in IFA titer was not found between PR and sick dogs. This clinicopathologic score could potentially provide guidance on patients’ parasite burden while monitoring the effect of treatment. Prospective studies that track the performance of this novel clinical score, and IFA and qPCR results, in dogs with a relapse should be pursued.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.