
Abstract
Carcinosarcomas are biphasic malignant tumors composed of 2 distinct neoplastic cell populations, epithelial cells and mesenchymal cells. A 13-y-old, female, mixed-breed goat was presented with a 1-wk history of anuria and lethargy. Transabdominal ultrasonography showed an irregular and heterogeneous structure in the region of the bladder and uterus and changes in the echogenicity of both kidneys. Given the poor prognosis, euthanasia was elected. Autopsy revealed a large mass within the uterine cervix and confirmed the changes in the urinary tract. Histopathology and immunohistochemistry revealed a mixed, anti-cytokeratin AE1/AE3–positive epithelial, and vimentin-positive mesenchymal neoplasm consistent with a homologous carcinosarcoma, also called malignant mixed Müllerian tumor, with areas of double-labeling. We highlight the complexity of the diagnosis of uterine neoplasms in domestic animals and in goats in particular.
Introduction
The prevalence of neoplasia in goats is reported to be as high as 8.7%. The most common neoplasms are lymphoma, squamous cell carcinoma, thymoma, and mammary adenocarcinoma. 25 In the same study of 100 goats, 6% of the neoplasms were tumors of the reproductive tract, and the most common tumors were leiomyoma (3) and adenocarcinoma (3). 25 A collision tumor of an adenocarcinoma and a leiomyosarcoma, with metastasis of the epithelial component to the lungs, has been reported. 12 Clinical signs of uterine neoplasia in small ruminants include pollakiuria, tenesmus, weight loss, lethargy, depression, and abdominal pain.11,33,41 Uterine carcinosarcoma (UCS) is a rare tumor, which is reported sporadically in veterinary species. To our knowledge, uterine carcinosarcoma has not been reported in goats. Carcinosarcomas are biphasic malignant tumors composed of 2 distinct neoplastic cell populations: epithelial (or carcinomatous) cells, and mesenchymal (or sarcomatous) cells. These tumors are believed to have a monoclonal origin from a common multipotential progenitor stem cell. Herein we report a case of UCS in a goat and review the literature on UCS.
A 13-y-old, female, mixed-breed goat was presented to the Cornell University Hospital for Animals (Ithaca, NY) with a 1-wk history of lethargy and anorexia and a 1-d history of recumbency. The goat had been treated by the referring veterinarian with flunixin meglumine and antibiotics for a possible cervical abscess, and had not been observed to urinate for 1 wk. The goat had no other history of illness and had never been bred; however, the owners noted that the doe’s mammary gland had always been prominent.
On presentation, the goat exhibited mild tachycardia and increased respiratory effort. Mucous membranes were white (FAMACHA score 5) 22 with a prolonged capillary refill time. The body condition score was 3 of 5 (Langston University scale). There was a palpable abdominal wave, and the mammary glands were hot and swollen, with 2 palpable, firm subcutaneous nodules just caudal to the udder.
Initial bloodwork revealed several significant derangements. The doe was severely anemic, with a packed cell volume of 0.09 L/L (reference interval [RI]: 0.25–0.40 L/L) and hemoglobin of 30 g/L (RI: 80–120 g/L). Lactate was elevated (3.6 mmol/L, RI: <2.0 mmol/L), and the goat was severely azotemic (creatinine 1,511.6 μmol/L, RI: 35–194; urea >18 mmol/L, RI: 1.4–3.4 mmol/L). The electrolyte abnormalities, including hyponatremia (128 mmol/L, RI: 140–150 mmol/L), hypochloridemia (92 mmol/L, RI: 99–110 mmol/L), and high normal potassium (4.3 mmol/L, RI: 1.9–4.7 mmol/L), were also consistent with acute kidney injury. The hemogram revealed leukocytosis (17.9 × 109/L, RI: 4.0–13.0 × 109/L) as a result of neutrophilia (13.5 × 109/L, RI: 1.2–7.2 × 109/L), and monocytosis (1.2 × 109/L, RI: 0–1.0 × 109/L), consistent with inflammation.
Transabdominal ultrasonography was performed to assess the architecture of the kidneys and to evaluate a possible mass in the caudal abdomen. The left kidney was enlarged (8 × 9 cm), with irregular, mixed echogenicity that obscured the normal renal architecture. The presence of hypoechoic fluid surrounding the left kidney was interpreted as perirenal edema. The right kidney was also enlarged (7 × 9 cm), and the pelvis was dilated, suggesting hydronephrosis. The remainder of the renal parenchyma was hyperechoic, with no cortical-medullary distinction. A large amount of free peritoneal fluid was visualized in the right caudoventral abdomen, and the omentum appeared edematous. Just cranial to the pelvic inlet, an irregular and heterogeneous structure with mixed hypoechoic and hyperechoic regions was identified in the region of the bladder and uterus. The bladder could not be definitively identified on ultrasonography. During transabdominal ultrasonography, a large volume of thick, white fluid exuded from a ruptured abscess in the right mammary gland, just cranial and proximal to the right teat.
Abdominocentesis of the free peritoneal fluid yielded a large volume of red, turbid fluid. Analysis of the peritoneal effusion yielded electrolyte abnormalities similar to those in the peripheral blood. The total protein (18 g/L) and total nucleated cell count (0.6 × 109/L) were within normal limits.
Transvaginal digital palpation revealed a firm, irregular thickening in the region of the cervix. The goat resented palpation of the region, and a vaginal speculum examination was not performed. A urinary catheter was passed into the bladder, and 2 mL of dark red-to-brown, foul-smelling fluid was expressed. Given the poor prognosis, euthanasia was elected, and a postmortem examination was performed.
Gross examination revealed ~3 L of thin, yellow, red-tinged fluid, admixed with a large (5 × 5 × 10 cm) mass composed of black-red, friable, amorphous blood clots in the abdominal cavity. The mesenteric root was diffusely expanded by a large amount of clear edema fluid. Within the mesentery, adjacent to the left kidney, were 4 large blood clots (5–8 cm diameter), surrounding the branches of the cranial mesenteric artery. The left kidney was enlarged (6 × 9 × 13 cm) and diffusely pale tan. The left renal pelvis was dilated and filled with blood clots, with compression of the medulla and brown discoloration of the renal papillae (pressure necrosis). The left kidney was surrounded by an ~2 cm thick layer of clotted blood filling and expanding the capsule, and extending from a small full-thickness tear within the adjacent mesentery. The right kidney measured 5 × 8 × 13 cm, and the pelvis was diffusely dilated and filled with small blood clots. Bilaterally, the cortex-to-medulla ratio was severely reduced (~ 2:1). The right and left ureters were dilated up to 0.5 cm diameter and filled with clear fluid (bilateral hydroureter). The urinary bladder was within normal limits, and empty, with a catheter in the lumen. In the cervix, a large (4 × 5 × 9 cm), polypoid mass extended into and occluded the cervical lumen (Fig. 1). The mass was brown-to-white and firm with a smooth surface. The cut surface was mottled white-to-brown. The uterus was diffusely dilated and filled with thin, brown fluid (bilateral hydrometra). The ovaries were unremarkable. Randomly distributed throughout the capsule and parenchyma of the liver were hundreds of pinpoint, well-demarcated petechiae. Within the cranial mediastinum was a 4 × 6 × 7 cm, multinodular, firm, smooth, gray mass. On cut surface, the mass contained variably sized cystic spaces, filled with clear, watery fluid.
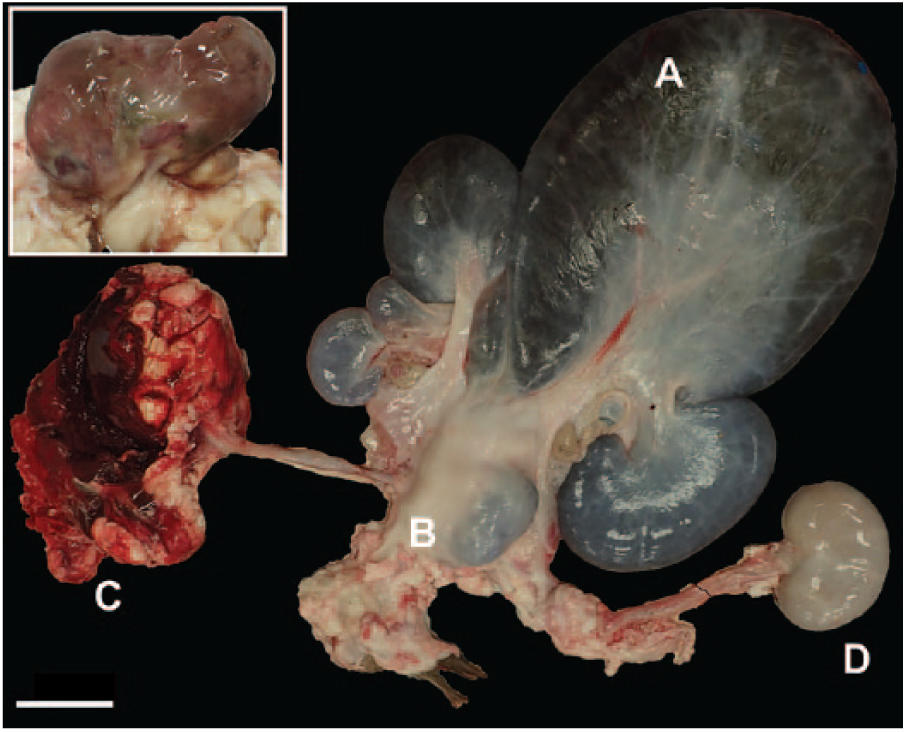
Uterus with dilated proximal portion of the uterine horns (
The tissues were fixed in 10% neutral-buffered formalin and embedded in paraffin as per routine procedures. Immunohistochemistry for cytokeratin AE1/AE3 (mouse monoclonal IgG1, clone AE1/AE3, broadly reacting cocktail of 2 monoclonal antibodies, M3515, Dako North America, Carpinteria, CA), alpha–smooth muscle actin (α-SMA; mouse monoclonal IgG2a, clone alpha sm-1, PA0943, Leica Biosystems, Newcastle Upon Tyne, UK), and vimentin (mouse monoclonal IgG2a, clone Vim 3B4, Dako), was performed based on standard laboratory guidelines.
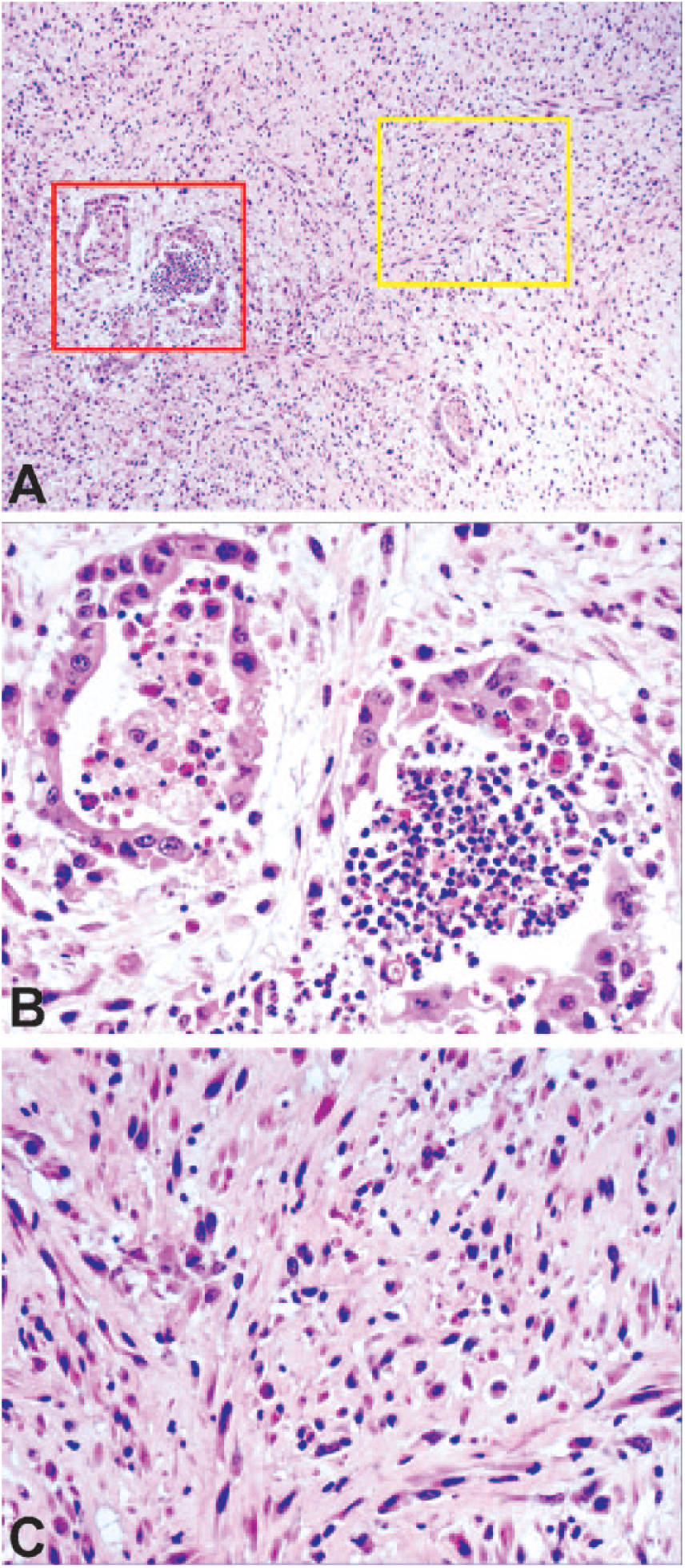
Microscopic examination of the cervical mass revealed a multilobulated, moderately cellular, moderately invasive, uterine neoplasm composed of intermingled mesenchymal and epithelial cells populations (Fig. 2A). Small lobules of epithelial cells were arranged in trabeculae and irregularly shaped ducts, regularly dispersed throughout the neoplasm (Fig. 2B). Multifocally, small nests or individual neoplastic epithelial cells were embedded within streams and bundles of neoplastic spindle-shaped cells and bands of dense fibrous connective tissue (Fig. 2C). The neoplastic epithelial cells were low columnar-to-cuboidal, rarely squamous, and had indistinct margins, scant-to-moderate granular eosinophilic cytoplasm, and an oval nucleus with vesicular chromatin, and a single large, prominent magenta nucleolus. Neoplastic mesenchymal cells consisted of a homogeneous population of fusiform-to-polygonal cells with moderate amounts of pale eosinophilic cytoplasm and round-to-elongate nuclei with up to 2 nucleoli. These cells were arranged in streams and bundles with a small amount of fibromyxomatous extracellular matrix. Anisocytosis and anisokaryosis were marked in both the epithelial and mesenchymal cells, with numerous karyomegalic cells in the spindle cell population, and 7 mitotic figures per ten 400× fields. Ductular spaces frequently contained amorphous eosinophilic or amphophilic material, karyorrhectic debris, foamy macrophages, neutrophils, and rare erythrocytes. Within the mass, locally extensive areas of necrosis were characterized by loss of cellular detail, and replacement by amorphous, eosinophilic material. The endometrium was otherwise unremarkable.
Microscopically, in both kidneys, ~70% of the tubular epithelial cells were lined by a single layer of attenuated epithelial cells with loss of nuclear detail. Multifocally, the tubular lumina were filled with pale, eosinophilic, flocculent material. Diffusely, the interstitium was expanded by clear edema fluid with small clusters of plasma cells and lymphocytes. Attached to the capsule of the left kidney was an extensive area of hemorrhage, and the capsule was diffusely thickened, up to 0.3 mm in width, by dense fibrous connective tissue.
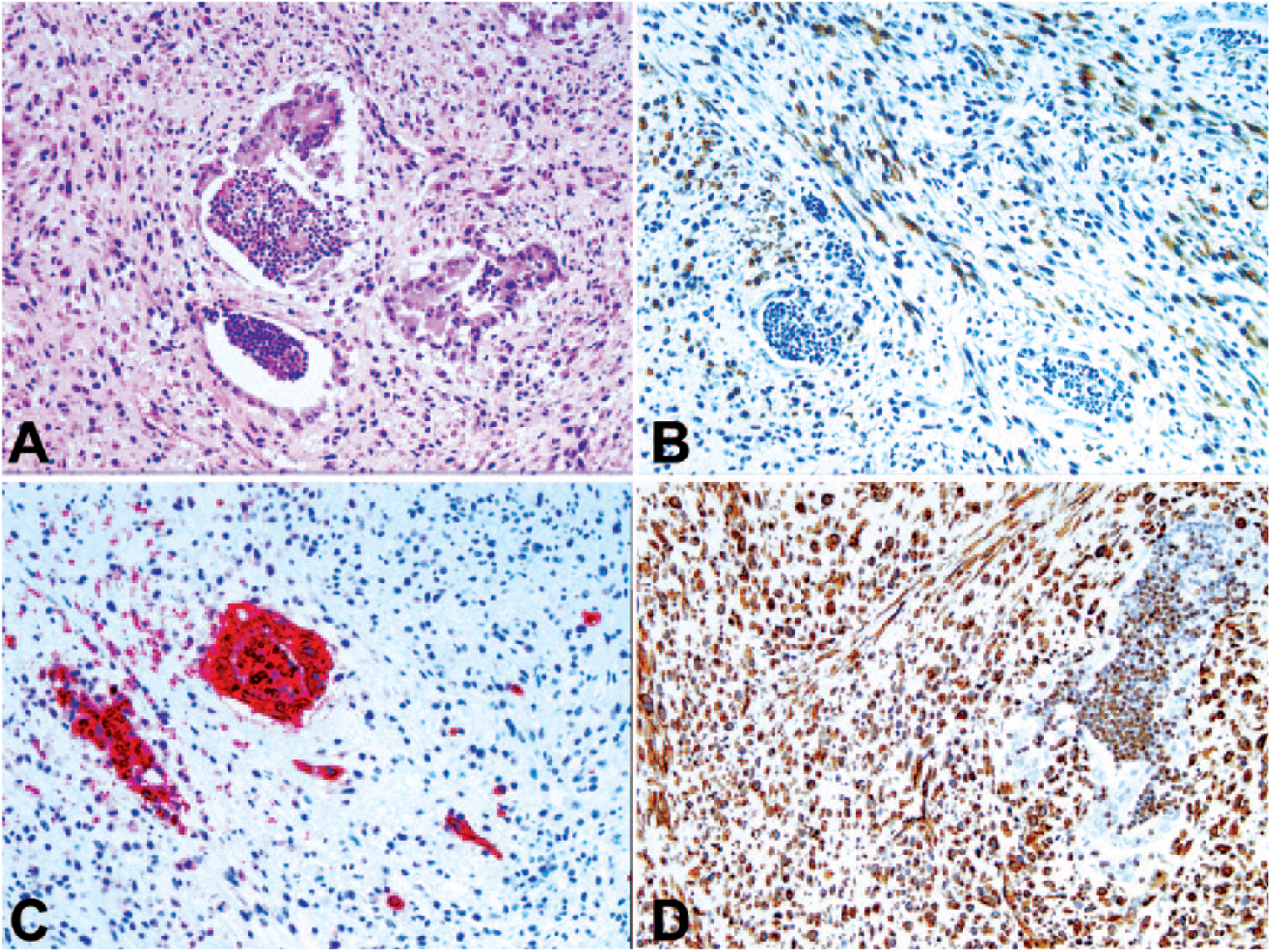
The 2 neoplastic cell populations, observed with hematoxylin and eosin staining (Fig. 3A), were further classified using immunohistochemistry. With α-SMA, for smooth muscle, ~60–100% of the spindle cell population displayed moderate-to-strong intracytoplasmic immunopositivity with great variation among the sections (Fig. 3B). With cytokeratin AE1/AE3, an epithelial marker, all of the epithelial neoplastic cells displayed strong intracytoplasmic immunopositivity. Approximately 10–60% of the mesenchymal population exhibited weak-to-moderate intracytoplasmic immunopositivity with great variation among the sections. In the sections with the weakest signals in the spindle cell component, most of the immunopositive cells were distributed around the epithelial components (Fig. 3C). With vimentin, a mesenchymal cell marker, the fusiform cells diffusely displayed strong intracytoplasmic immunopositivity, and ~20–30% of the epithelial component displayed moderate-to-strong intracytoplasmic immunopositivity (Fig. 3D). Based on the histologic and immunohistochemical findings, the diagnosis was a cervical UCS. The presence of stromal components showing differentiation to tissues seen in normal endometrium classifies this tumor as homologous.
Uterine carcinosarcoma.
The cervical neoplasm caused mechanical obstruction of the urinary and reproductive tracts with subsequent bilateral hydrometra, hydroureters, hydronephrosis, and renal rupture. The combination of renal parenchymal loss, because of compression, and severe perirenal hemorrhage explains the severe anemia. The mass in the cranial mediastinum was a thymoma, which is a common and usually incidental finding in aged goats. 19 The abnormal bladder echogenicity was the result of the close spacing of the urinary bladder and the cervical mass, which may have impaired the examination.
UCS has various names in the literature, including malignant mixed Müllerian tumor (MMMT), malignant mixed mesodermal tumor, and uterine metaplastic carcinoma, all reflecting the duality of the neoplastic tissue, and referring to specific body location or pathogenesis. MMMT is specifically a carcinosarcoma of the female genital tract and the name is based on its embryogenesis. Epithelial and mesenchymal structures normally arise from the pluripotent cells of the Müllerian (paramesonephric or female) duct and therefore may arise from any location along the female genital tract ducts. 40 Because the exact pathogenesis of these tumors is not known, the preferred term, according to the World Health Organization (WHO) classification, 39 is uterine carcinosarcoma.
In humans, UCSs are very aggressive tumors and comprise ~5% of uterine malignancies.7,26 Grossly, the tumors are bulky, hemorrhagic, and necrotic polypoid masses that fill the uterine lumen and often involve the cervix. Vaginal bleeding is the most common presenting complaint. 26 The tumors are graded according to the high-grade endometrial carcinoma scheme, rather than the sarcoma grading scheme.7,26,27
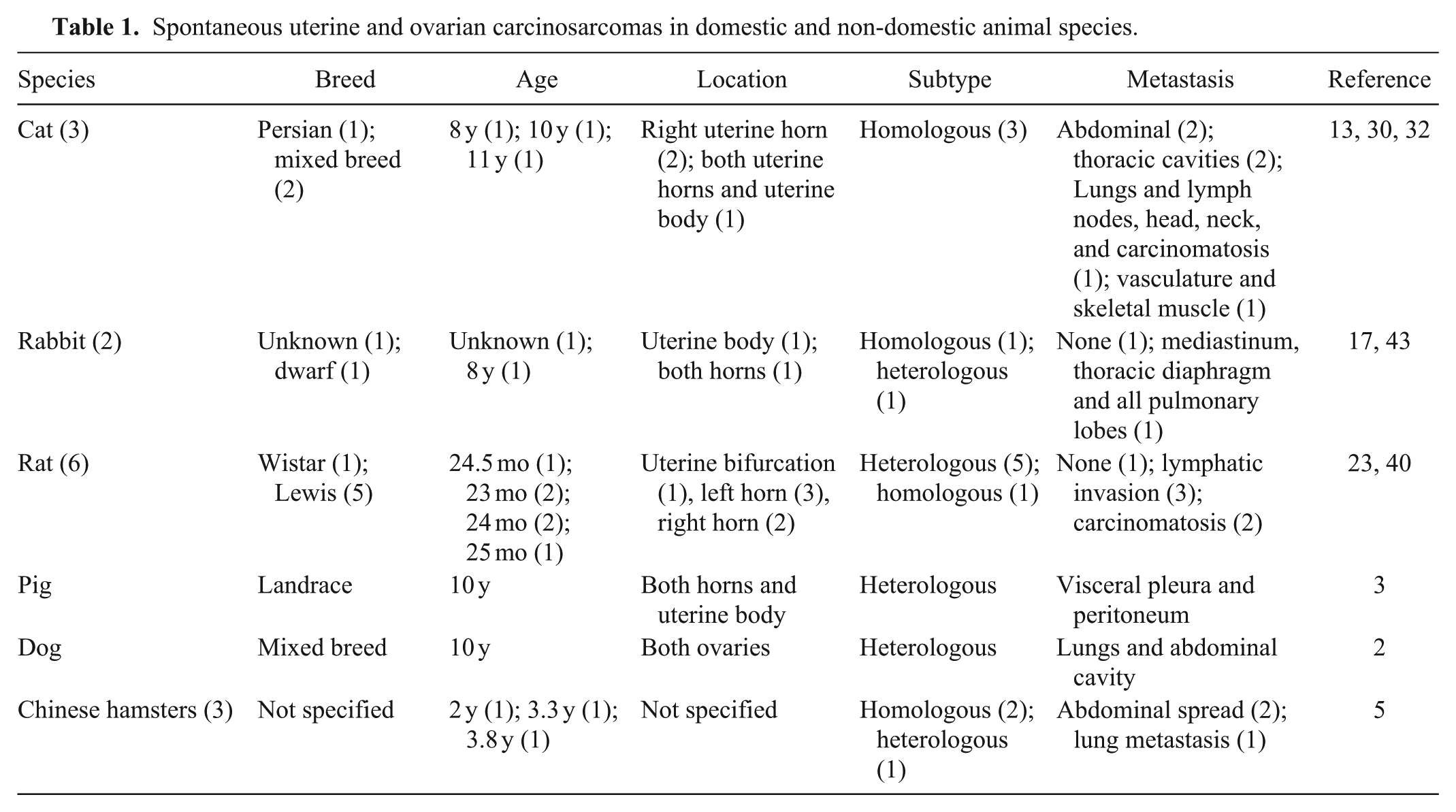
In goats, carcinosarcoma has not been reported in any organ, to our knowledge. In other animal species (i.e., mice and rats, 34 dogs,4,8,15 cats, 31 a rabbit, 36 and a gray squirrel 37 ), most cases are mammary carcinosarcomas (Table 1). Feline carcinosarcomas have also been reported in the uterus,13,30,32 lung, 14 biliary system, 9 pancreas, 42 and salivary gland. 24 In dogs, sites of carcinosarcoma also include the salivary gland, 1 head, 35 thyroid, 18 and ovary. 2 There is a report of a prostatic carcinosarcoma in a white rhinoceros. 38 Mixed tumors of the female genital tract, with both epithelial and mesenchymal components, are rare in veterinary medicine, but are reported in a few domestic and nondomestic species (Table 1). Metastases are reported in all but 2 cases, highlighting the aggressive clinical behavior of these tumors. It is worth noting that a uterine adenosarcoma, in which only the mesenchymal population is malignant and the epithelial population is benign, has also been described in a 10-y-old domestic shorthaired cat. 29
Spontaneous uterine and ovarian carcinosarcomas in domestic and non-domestic animal species.
Carcinosarcomas are malignant tumors composed of 2 distinct neoplastic cell populations: epithelial cells and mesenchymal cells. Various hypotheses have been proposed to explain these unusual tumors. In some cases, carcinosarcomas may represent collision tumors, wherein cells from 2 distinct neoplasms become intermingled. Carcinosarcomas may also arise from a single pluripotent stem cell that gives rise to both the epithelial and mesenchymal components. 7 Alternatively, a neoplastic population may undergo mutations that lead to transformation from an epithelial to a mesenchymal phenotype (epithelial–mesenchymal transition). 7 Finally, an epithelial tumor may induce changes in the surrounding mesenchymal cells leading to a pseudosarcomatous or sarcomatous reaction (conversion theory). 7 Carcinosarcomas have been reported in multiple organs, and the pathogenesis may be site-specific.
To date, UCSs are believed to originate from a uterine carcinoma with areas of malignant sarcomatoid differentiation. The epithelial component of the mass, derived from a single progenitor cell, is thought to induce changes in the mesenchymal cell population. Therefore, UCSs primarily spread via lymphatics to regional lymph nodes and the lungs, similar to endometrial carcinomas. However, the mesenchymal component can metastasize to the lungs via the hematogenous route. 16 This conversion theory of UCS pathogenesis is accepted and supported by similar chromosomal aberrations, cytogenic aspects, concordant loss of heterozygosity, identical p53/Kras mutations, and matching X-inactivation patterns, 7 which make the theory of 2 distinct neoplastic populations unlikely. Several immunohistochemical studies also confirm the epithelial origin of these tumors, such as higher degree of apoptosis in the mesenchymal population using DNA nick-end immunostaining, higher levels of expression of CD34, VEGF, and MMP-7, and a higher mitotic index in the epithelial component, contributing to growth and invasion, respectively. 26 Therefore, in human medicine, UCSs are considered a type of endometrial carcinoma.
Histologically, these neoplasms are characterized by a combination of carcinomatous (epithelial) and sarcomatous (mesenchymal) elements. The mesenchymal and epithelial populations are sharply demarcated and both typically exhibit features consistent with high-grade malignancy, namely greater cellularity and significant pleomorphism, an increased mitotic count, foci of necrosis, and an infiltrative growth pattern.8,16 The epithelial population, composed of cuboidal-to-polygonal cells with round, central nuclei, typically forms irregular and ill-defined tubular structures, nests, and islands separated by the mesenchymal population, composed of fusiform-to-polygonal cells, with fusiform-to-polygonal nuclei.
The UCS mesenchymal component can display a variety of histologic patterns allowing further differentiation into homologous and heterologous subtypes. In the homologous subtype, the mesenchymal element consists predominantly of fibrous tissue, smooth muscle, and/or endometrial stroma-like tissue (i.e., tissues seen in normal endometrium). In the heterologous subtype, the mesenchymal element includes foci of striated muscle, cartilage, bone (sometimes covered by plump osteoblasts), and/or adipose tissue (i.e., tissue types not normally present in the uterus). These foci also often display malignant features. 40 The prognostic significance of these histologic subtypes is unclear.20,26
Immunohistochemistry is required to confirm the presence of the 2 predominant neoplastic populations and can be helpful in identifying the other cell types seen in the homologous and heterologous subtypes. Immunohistochemically, UCSs typically express epithelial (cytokeratins and epithelial membrane antigen) and stromal lineage markers (vimentin, CD10, CD34) in relation to their histologic appearances 33 ; areas of double labeling, with co-expression of cytokeratins and vimentin in the mesenchymal and epithelial elements, are frequent and highly suggestive of a mixed tumor. 33 UCSs also express other markers, consistent with the morphologic appearance, such as α-SMA in smooth muscle differentiation, or S100 in areas with chondroid or lipomatous differentiation. Other markers useful to differentiate UCS from carcinomas and malignant myoepitheliomas are calponin, p63, and CK14. Carcinomas and myoepithelial cells are positive for these markers, whereas carcinosarcomas are negative for calponin, p63, and CK14. 16
In humans, numerous markers, including p27, p53, p16, c-KIT, COX-2, EGFR, HER2/neu, the oncogene AKT, the PIK3C gene, and the PAX8 paired gene, are expressed in UCS and have been studied to identify potential markers and therapeutic targets. 28 Particularly, p53 staining highlights the monoclonal origin of both mesenchymal and epithelial cell populations, given that several studies showed a concordance of p53 staining, either absent or present in both components. 27 Moreover, in a study that compared the immunoreactivity pattern between p53 and p16 in UCS, results show that p16 immunoreactivity is significantly more intense and diffuse than p53 immunoreactivity in both components of the tumor, suggesting that alteration of the p16-Rb pathway plays an important role in the pathogenesis of these tumors. 6 The same group also found that p16 and p53 immunoreactivity were concordant between the 2 neoplastic populations of the same UCS in 90% and 83% of cases, respectively. 6 Finally, in 62 cases of human UCS, a concordant expression of p16, p53, and PAX8 was observed in both neoplastic populations of the same UCS, further supporting the monoclonal theory of UCS tumorigenesis. 10 PAX8, a member of the PAX family of paired-box, is a useful immunohistochemical marker, used in human medicine to identify epithelial neoplasms of Müllerian tract origin, being expressed in the carcinomatous components of nearly all UCS (37 of 38 cases; 97%), with more variable expression in the sarcomatous components. PAX8 can be used to identify the uterine origin of the carcinomatous metastases. 21
Therefore, even though histologic features can be typical, immunohistochemical characterization of the tumor is useful for definitive diagnosis. Areas of double-labeling with cytokeratins and vimentin, and immunohistochemical staining for p16, p53, and PAX8, may be helpful in establishing a diagnosis of UCS.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.