
Abstract
A 10-y-old Irish Setter was presented with a history of recurrent episodes of regurgitation and vomiting, with more recent development of tachypnea. Megaesophagus had been diagnosed in the dog 2 y prior to this presentation. A solitary polypoid mass present immediately rostral to the lower esophageal sphincter was biopsied during percutaneous endoscopic gastrostomy tube placement. Barrett esophagus was diagnosed based on the observation of a polypoid mass with intestinal metaplasia that arose from the surrounding esophagus. Histology of the polypoid mass demonstrated squamous-to-columnar metaplasia, hyperplasia, dysplasia, and carcinoma in situ.
Barrett esophagus (BE), which is characterized by intestinal metaplasia of the distal esophagus, is well recognized as the most important risk factor for the development of esophageal adenocarcinoma in humans.1–3,11,16 As such, it has been investigated extensively both in humans and animals, and it has been induced experimentally in rodent, canine, and primate models.1,2,6,11 Spontaneous development of BE in dogs has been described only rarely.4,5,10,15
Megaesophagus (ME) is a disorder characterized by diffuse esophageal dilation with decreased peristalsis or esophageal hypomotility that causes regurgitation and progressive loss of body condition.12,17,18 Congenital and acquired forms have been described, with the acquired form either idiopathic or secondary to various diseases. 17 Disease processes in which secondary ME has been reported include neuromuscular, immune-mediated, endocrine, gastrointestinal, paraneoplastic, and toxic causes. 12 The underlying mechanism by which these disease processes result in ME has yet to be determined, although some studies have suggested a defect in the afferent neural response to esophageal distention.8,9
In humans, esophageal dysmotility, lower esophageal sphincter (LES) dysfunction, and gastric dysmotility or delayed emptying have all been shown, either alone or in combination, to lead to gastroesophageal reflux disease (GERD). 14 GERD in turn leads to esophagitis, which can result in esophageal dysmotility and BE. 13 We describe herein an esophageal carcinoma in situ identified in a background of BE, in an Irish Setter with chronic ME.
A 10-y-old castrated male Irish Setter was presented to Massey University Veterinary Teaching Hospital (MUVTH) because of recurrent episodes of regurgitation and vomiting, along with recent development of tachypnea. The patient was previously diagnosed with ME, and had been regurgitating intermittently over the preceding 2-y period, despite supportive management for ME. Following initial stabilization, the patient underwent endoscopic placement of a 16Fr percutaneous endoscopic gastrostomy (PEG) tube (MILA International, Florence, KY). During esophagoscopy, diffuse esophageal dilation was appreciated, along with a solitary polypoid mass (Figs. 1, 2) identified immediately cranial to the LES. This structure appeared lobulated, with reddening and ulceration of both the mass and the adjacent mucosa. Following successful PEG tube placement, the mass and the surrounding mucosa were biopsied using endoscopic guidance.
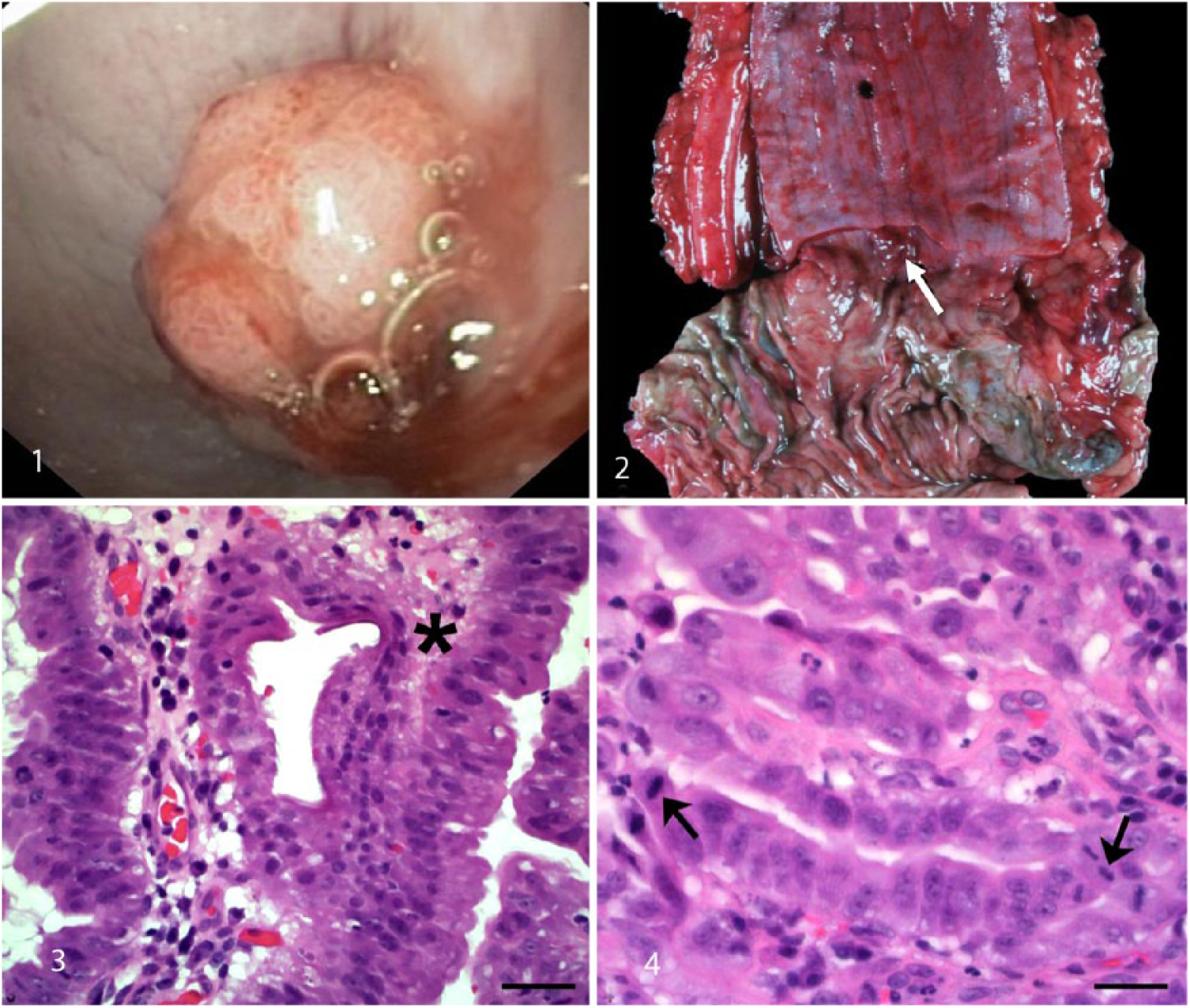
Endoscopic, gross, and histologic images of an esophageal mucosal mass in a dog.
Histologically, the cauliflower-like, densely cellular, polypoid tissue was composed of complex exophytic villous projections supported by loose collagenous stroma. Large columnar epithelial cells occasionally piled up and covered the villous projections. Evaluation of the mass revealed areas that exhibited features of hyperplasia, dysplasia, and carcinoma in situ (Figs. 3, 4). Within the areas of hyperplasia, the columnar epithelium was tall and had distinct cell borders and moderate amounts of pale eosinophilic cytoplasm. The cells each had a single large basilar nucleus with vesicular-to-stippled chromatin and a single inconspicuous nucleolus. In areas of dysplasia, the cells were rounded, had lost polarity, had small amounts of eosinophilic cytoplasm and large round nuclei with vesicular chromatin, and 1–4 round basophilic nucleoli. Foci that were considered to be carcinoma in situ contained epithelial cells that were large, round-to-polygonal, had loss of nuclear polarity, and contained 1–4 large nuclei with vesicular chromatin and 1–4 round, prominent basophilic nucleoli. Severe anisocytosis, anisokaryosis, and karyomegaly with 12 mitotic figures in ten 400× fields were also evident in this area. Multifocally, there were areas of epithelial erosion and flattening (attenuation), along with infiltration of small numbers of intraepithelial lymphocytes and neutrophils. Small-to-moderate numbers of neutrophils, lymphocytes, and plasma cells infiltrated the subjacent submucosa that was edematous and contained small blood vessels lined by prominent, reactive endothelium.
The dog died 3 d later, and autopsy revealed that leakage of the PEG tube had resulted in marked cellulitis in the surrounding subcutaneous tissue. Sections of lung contained intravascular bacterial colonies, confirming development of septicemia prior to death. Dilation of the distal half of the esophagus was visible. The dilation became more severe distally within the esophagus, and the esophagus was dilated to 8 cm diameter at the thoracic inlet. A 1-cm multilobular, polypoid, red mass was visible within the esophagus 0.5 cm proximal to the gastric cardia (Fig. 2). The mass appeared to be confined to the mucosal surface of the esophagus, with no visible evidence of invasion through the wall of the esophagus. The remainder of the gastrointestinal tract appeared within normal limits.
Histologic lesions in the mass did not differ from lesions observed in the biopsy. A diagnosis of carcinoma in situ was confirmed. Squamous epithelium was visible adjacent to the polyp, thus confirming origin from the esophagus rather than the stomach. The diagnosis of BE was based on the observation of intestinal metaplasia.
An underlying mechanism for the disease process was not identified in either the first or second reported cases of canine BE.5,10 A 2017 report documented the presence of an esophageal adenocarcinoma that contained prominent intestinal metaplasia in an adult male Bulldog; however, no potential pathomechanism was described. 4 A case report described an adenosquamous carcinoma of the esophagus in a dog, which was suspected to have developed from BE, based on the presence of both neoplastic and non-neoplastic columnar epithelial cells. 15 Reflux esophagitis with associated metaplastic columnar esophageal epithelium was described in a series of 3 cats, with suspected underlying causes including cardial incompetence and sliding hiatal hernia. 7 However, no evidence of neoplasia was reported in these cats.
In our case, we propose that the development of BE and carcinoma in situ was secondary to chronic esophagitis. Chronic esophagitis is hypothesized to develop as a result of chronic GERD, because of the underlying esophageal dysmotility that is present in cases of acquired ME. 12 As ME is common in dogs, it is uncertain why BE is not observed more frequently with this disease process. One explanation would be that it is technically demanding to biopsy the esophagus and thus this procedure is not performed routinely. A possible alternative reasoning is that dogs with ME are not closely evaluated for BE at autopsy. Further studies are required to more accurately evaluate prevalence of BE, and it is possible that postmortem evaluation of the distal esophageal mucosa in dogs will reveal that BE is a common change. In our case, BE was considered to be subclinical, and thus not the cause of clinical disease at the time of diagnosis.
Replacement of the normal squamous epithelium with metaplastic columnar epithelium in BE constitutes the first phase in the development of esophageal adenocarcinoma. 1 Dysplasia and the development of carcinoma in situ follow and constitute the next phases in the sequence. The 2 criteria necessary for diagnosis of BE include endoscopic evidence of change in the distal esophageal mucosa above the gastroesophageal junction and confirmation of intestinal metaplasia on histology.5,10,16 Our case, along with the spontaneous cases of BE in dogs noted above,4,5,10,15 suggests that the incidence of BE may in fact be higher than currently believed.
Footnotes
Acknowledgements
We thank Dr. Robert J. Bahr for evaluation of the thoracic radiographic images, and Dr. Nicholas J. Cave for critical input into case management.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.