
Abstract
Eastern equine encephalitis virus (EEEV) is classified as a select agent and is capable of causing mortality in humans and a number of veterinary species. Herein, we describe 3 cases of EEE in puppies in Michigan and New York. Two puppies were euthanized following an acute history of seizures and obtundation. A littermate of one of these puppies died 2 wk earlier following a history of anorexia and fever. All 3 puppies lacked significant gross anatomic lesions at autopsy and tested negative for rabies virus. In all 3 puppies, histologic examination revealed necrotizing, neutrophilic, lymphoplasmacytic meningoencephalitis with strong positive immunohistochemical labeling for EEEV antigen in neurons and glial cells. The diagnosis of EEE was confirmed by PCR in one puppy and by plaque reduction neutralization testing in the other 2 dogs. EEE is rare in dogs, and has only been reported in puppies. The initial clinical signs of EEE in puppies are typically nonspecific, including anorexia, fever, and diarrhea, but rapidly progress to severe neurologic disease characterized by seizures and recumbency. Although rare, EEE should be considered as a differential diagnosis for neurologic disease in puppies, especially after more common diseases, such as canine distemper, rabies, and toxoplasmosis have been ruled out.
Species Eastern equine encephalitis virus (EEEV; family Togaviridae, genus Alphavirus) is capable of causing disease in a number of mammalian and avian species, and is the most lethal of the naturally occurring encephalitic alphaviruses of North America, with mortality rates in humans and horses of 50–75% and 70–90%, respectively.14,18 The U.S. Departments of Agriculture and Health and Human Services classify EEEV as a select agent in the Federal Select Agent Program, a program responsible for supervising the possession of biological agents and toxins determined to have the potential to pose a severe threat to public, animal, or plant health or to the products of animals or plants (https://www.selectagents.gov/SelectAgentsandToxinsList.html).
The virus is distributed throughout the southeastern United States and extends up the Eastern Seaboard into Canada and throughout portions of the Midwest. 18 EEEV was initially isolated from horses in Virginia and New Jersey in 1933, but has been demonstrated to cause disease in a variety of domestic and wild animals, including swine, cattle, white-tailed deer, alpacas, emus, and pheasants.2,7,8,11,13,15,17 EEEV is primarily maintained in a transmission cycle between birds and mosquitoes, predominantly by the mosquito Culiseta melanura. However, mosquitoes within the genera Aedes, Culex, and Coquillettidia feed on both mammals and birds, and are therefore vital for transmission of the virus to humans and domestic animals (so-called “bridge vectors”).1,18
In a study in the southern United States, 35% of wild snakes surveyed were seropositive for EEEV. 5 A second study determined that when inoculated with the virus, garter snakes maintain a longer infectious viremic period than birds. 16 Data from the study also showed that garter snakes have the potential to remain viremic throughout hibernation, providing evidence that snakes may provide an overwintering host for EEEV. 16
An 8-wk-old female Boxer puppy (puppy 1) was presented to the Michigan State University Veterinary Diagnostic Laboratory (Lansing, MI) for autopsy following a 2-d history of lethargy, weakness, and possible seizures. The dog had been acting aggressively toward littermates, but otherwise avoided interaction. Upon presentation to the referring veterinarian, the dog was thin, with profound ataxia and weakness. Diarrhea and mild mucoid nasal discharge had been noted by the owner the previous night. The puppy was unable to stand, and began to have seizures shortly after arrival. Both pupils were miotic, and there was bilateral lack of tracking, menace, and direct and consensual pupillary light reflexes. The dog continued to convulse, and euthanasia was elected. Littermates were reportedly healthy. At autopsy, the puppy was thin and moderately dehydrated. Mucopurulent discharge drained from both nares, and light brown, liquid feces were smeared on the perineum. No other significant abnormalities were noted.
A 4-mo-old female St. Bernard puppy (puppy 2) died overnight in a kennel following an acute clinical history of fever and anorexia. The body was frozen and stored by the referring veterinarian. Two weeks after the death of this puppy, a second 4-mo-old male St. Bernard puppy (puppy 3) from the same litter was euthanized after an acute history of anorexia and fever that progressed to seizure-like activity and obtundation. Both puppies were submitted to the Cornell University College of Veterinary Medicine (Ithaca, NY) for autopsy. No significant gross anatomic lesions were found in either puppy.
In all 3 puppies, microscopic examination of the cerebrum revealed discrete-to-coalescing foci of necrosis and rarefaction (Fig. 1). Necrotic foci were infiltrated by moderate numbers of viable and necrotic neutrophils and fewer gitter cells. Multifocally within affected areas, neurons were shrunken with pyknotic nuclei (necrosis) and were frequently accompanied by satellitosis and neuronophagia (Fig. 2). Multiple small blood vessels contained fibrin thrombi, and Virchow–Robin spaces were frequently mildly to moderately expanded by mixed infiltrates of lymphocytes, plasma cells, neutrophils, and macrophages. Perivascular inflammatory cell infiltrates were the predominant lesion in puppies 2 and 3, with less involvement of the parenchyma than in puppy 1. Similar inflammatory infiltrates, with slightly fewer neutrophils, multifocally expanded the leptomeninges, including within the cerebellum of puppies 2 and 3. Gliosis varied among sections.
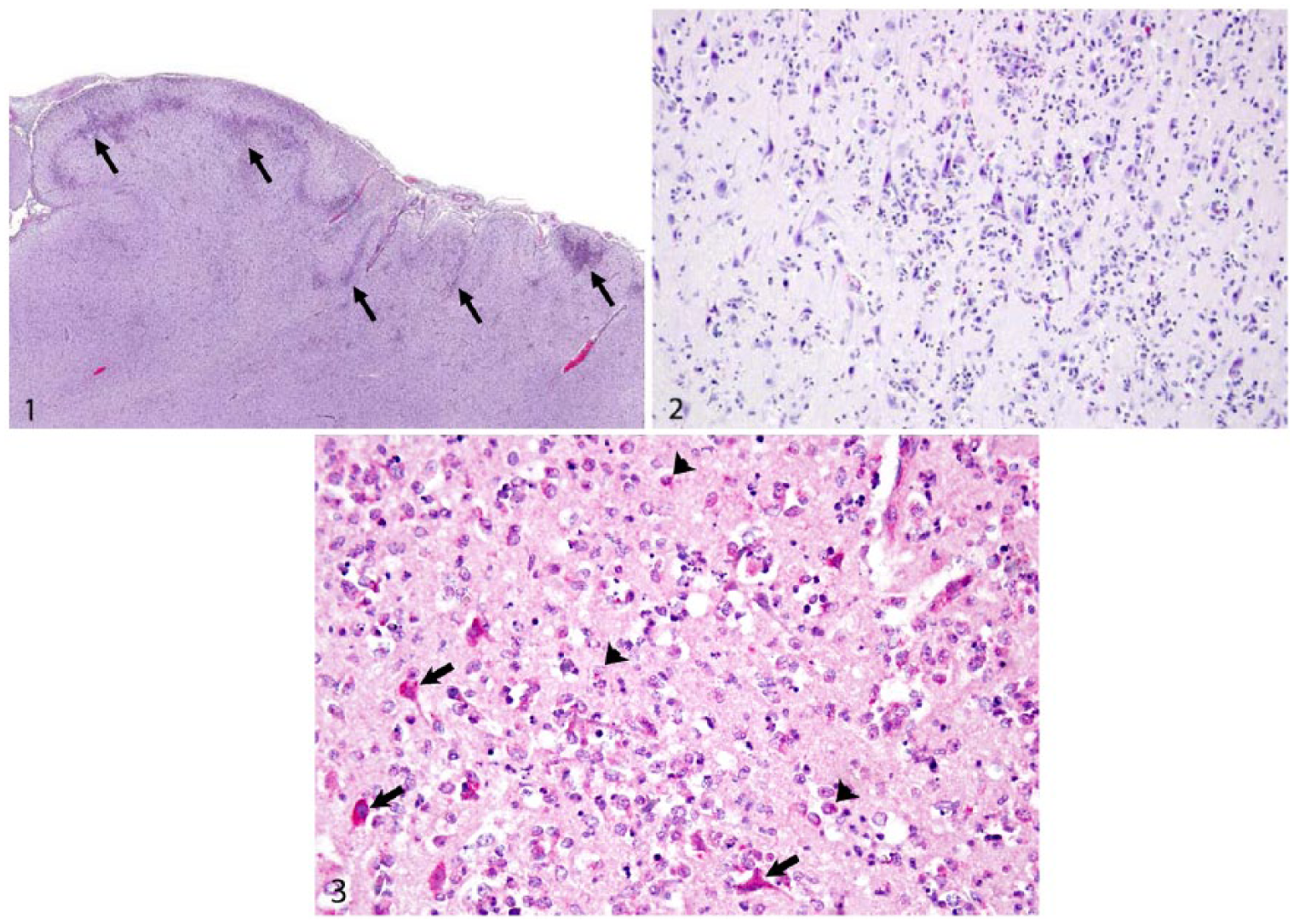
Necrotizing meningoencephalitis in the cerebrum of a puppy, caused by eastern equine encephalitis virus infection.
Immunohistochemistry detected EEEV antigen in neurons and glial cells in sections of cerebrum from all 3 puppies (Fig. 3). The diagnosis of EEE was confirmed by PCR in puppy 1 and by plaque reduction neutralization testing in puppies 2 and 3. Fluorescent antibody testing for rabies virus was negative in all 3 puppies. Puppies 1 and 3 were also tested for West Nile virus and canine distemper virus, both of which were not detected by PCR (puppy 1) or immunohistochemistry (puppy 3). PCR for Toxoplasma gondii was also negative in puppy 1. Based on the collective postmortem findings, the puppies were diagnosed with moderate-to-severe, necrotizing, neutrophilic, lymphoplasmacytic-to-lymphohistiocytic meningoencephalitis with neuronophagia caused by EEEV infection.
Although rare, EEE has been described in dogs. Twelve cases of EEE were reported over a 12-y period from a veterinary diagnostic laboratory in the state of Georgia, in puppies aged 10 d to 6 mo representing 6 different breeds. The dogs initially were presented because of fever, diarrhea, and anorexia; however, these signs progressed to seizures, nystagmus, altered mentation, and recumbency within 24–36 h. The brains of these dogs were grossly unremarkable, with the exception of meningeal congestion in 2 animals. Histologic lesions included gliosis, hemorrhage, neuronal necrosis, and mixed perivascular infiltrates of inflammatory cells. 3
In human cases of EEE, gross anatomic lesions of the brain include hemorrhage, encephalomalacia, leptomeningeal congestion, and edema. Histologic lesions in acute human cases include neuronal necrosis, vasculitis, thrombosis, perivascular inflammatory cuffs, gliosis, meningitis, and infiltration of the neuropil by macrophages and neutrophils. Interestingly, although mice infected with the virus develop severe encephalitis, vasculitis is not typically a prominent histopathologic finding. 14 Histologic lesions within the brains of nonhuman primates and horses acutely infected with EEEV are similar to those in humans, and gross anatomic lesions are frequently absent.6,14
Within 2 wk following the deaths of puppies 2 and 3, 4 additional puppies from the same kennel were diagnosed with EEE. 9 Horizontal transmission of EEEV has been demonstrated experimentally in emus and turkey poults (Brown et al. Eastern equine encephalitis virus–induced enteritis in turkey poults: reproduction by oral inoculation and spontaneous horizontal transmission. Proc Am Coll Vet Pathol; Nov 1992; San Diego, CA), and EEEV has been isolated from the feces of pheasants and emus, as well as from regurgitated material in emus.10,15 To our knowledge, shedding of EEEV has not been investigated in canine feces or vomitus, and these materials were not tested for EEEV in any of the cases reported herein. The 4 puppies were also housed outdoors, which could have made them more available for mosquito transmission of EEEV. However, instead of individual viral inoculation by mosquito, an oral route of transmission may have resulted in the spread of EEEV between the affected puppies housed within the same kennel in New York.
Interestingly, the year the 6 puppies from New York were diagnosed with EEE (2011) also saw the highest number of equine cases of EEE in 20 y in New York State, 11 of 12 of which originated in the same or adjacent county to the puppies with EEE. 9 This highlights the typical geographic and temporal nature of EEE epizootics and epidemics.1,9 EEE is known to occur in swampy areas given their proximity to mosquito vectors. The 2 New York counties in which the canine and majority of the equine cases of EEE occurred in 2011 are part of a 4-county area of central New York historically recognized to have both the majority of detected cases of EEEV infection and often the first detection of EEEV in the state in a given year. The high activity of the virus in this area has been attributed to 2 large swamp complexes that serve as reservoirs for C. melanura and, as a result, EEEV (New York State Department of Health, 2012, Mosquito Borne Illness Surveillance and Response Plan. Available at: https://www.health.ny.gov/diseases/west_nile_virus/docs/2012_mosquito_borne_illness_surveillance_and_response_plan.pdf). Transmission of the virus is typically during the summer and early fall, and concordantly, puppies 1–3 developed EEE in July. 1 However, winter transmission has been rarely reported in subtropical areas such as Florida. 12 Outbreaks of EEE have been correlated with wet, warm summers. 4 The Palmer Hydrological Drought Index, which has been used to estimate the inundation of wetlands favored by C. melanura, indicated very to extremely moist hydrologic conditions in this area of New York from April through June 2011, falling slightly to moderate to very moist conditions in July 2011 (https://www.ncdc.noaa.gov/temp-and-precip/drought/historical-palmers/phd/201209-201308). 13 Although not a definitive cause, such wet conditions during the 2011 EEEV transmission season in this area may have increased C. melanura populations and promoted transmission of EEEV. Weather conditions conducive to EEEV transmission may become more frequent in some areas as a result of climate change. 4 Climate change is predicted to alter the epidemiology of vector-borne diseases such as EEE by increasing viral transmission, expanding the geographic range and abundance of relevant vectors, and extending the season for virus transmission.1,4
The clinical signs, age, lack of gross anatomic lesions within the brain, and histologic features in the cases reported herein are consistent with previously described cases of canine EEE. 3 EEE should be considered as a differential diagnosis in cases of neurologic disease in puppies, especially when more common diseases, such as rabies, canine distemper, and toxoplasmosis, have been ruled out.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.