
Abstract
We evaluated 43 published cases of dogs with confirmed Pneumocystis infection regarding the value of clinical parameters indicating the presence of the disease as well as tools for the detection of the pathogen. The assessed parameters included clinical signs, laboratory findings, results of thoracic radiography, autopsy, histopathology, methods for the detection of Pneumocystis, as well as medical therapy. Pneumocystosis was diagnosed most often in certain breeds (Cavalier King Charles Spaniel, Miniature Dachshund) with a predisposition for impaired immunity. The median age of the dogs was 1 y. Chronic therapy-resistant respiratory signs, such as tachypnea, dyspnea, and cough, along with leukocytosis, neutrophilia, and hypogammaglobulinemia, were the most frequently described clinical and clinicopathologic abnormalities. Pneumocystosis can be masked by coinfections with other respiratory pathogens, and the successful detection of Pneumocystis organisms is of major relevance. Several detection methods have been used in the past, but only a few provide reliable results. In 2017, the cytologic evaluation of Giemsa-stained bronchoalveolar lavage samples is generally used, even if sensitivity is only moderate. More reliable results can be achieved using special stains or sensitive molecular techniques. Fast and reliable detection of Pneumocystis is the essential basis for appropriate treatment and higher survival chances for dogs.
Introduction
The genus Pneumocystis comprises a group of highly diversified opportunistic yeast-like fungi that are adapted to type I pneumocytes of various mammalian hosts and cause pneumonia when immunologic host resistance is impaired. 1 Prevalence or incidence data for Pneumocystis in dogs are not available, to our knowledge, and cases of clinically evident Pneumocystis pneumonia have been reported only sporadically (Fox R. A case of suspected Pneumocystis carinii pneumonia in a Cavalier King Charles Spaniel. Clinicopathological Newsl 2012;30. Available from: https://goo.gl/xCQhkt).6,7,12,14,16–18,20–22,29,32,34,35,38,41 Depending on the severity of infection, pneumocystosis has variable nonspecific respiratory signs ranging from cough 6 to tachypnea and dyspnea. 28 For these reasons, a fast and correct clinical diagnosis is problematic, and inappropriate treatment is often associated with high mortality. A large variety of clinical and laboratory findings has been published. However, diagnostic relevance is of low significance given that most of the findings are nonspecific. The aim of our meta-analysis was the evaluation of 17 published Pneumocystis studies and case reports including 43 dogs in order to determine the relevance of certain clinical and laboratory parameters and the value of several methods for the detection of the organisms. In addition, we assessed different treatment options regarding the number of surviving animals as well as the survival period.
Meta-analysis
We evaluated signalment, medical history, clinical signs, laboratory findings (leukogram, serum biochemical analysis), results of thoracic radiography, autopsy, methods for the detection of Pneumocystis spp. (cytology, histopathology, special staining methods, electron microscopy, immunofluorescence, immunohistochemistry [IHC], in situ hybridization [ISH], PCR), as well as data regarding the treatment of 43 dogs reported in 17 publications (mainly case reports and case series: Table 1).The available references are listed including breed, age, and sex of the assessed dogs. Evaluated parameters, numbers of dogs showing the respective clinical sign or result per number of citations of the respective parameter, and references are presented (Tables 2–7).
Meta-analysis of breed, age, and sex predisposition of dogs with confirmed pneumocystosis.
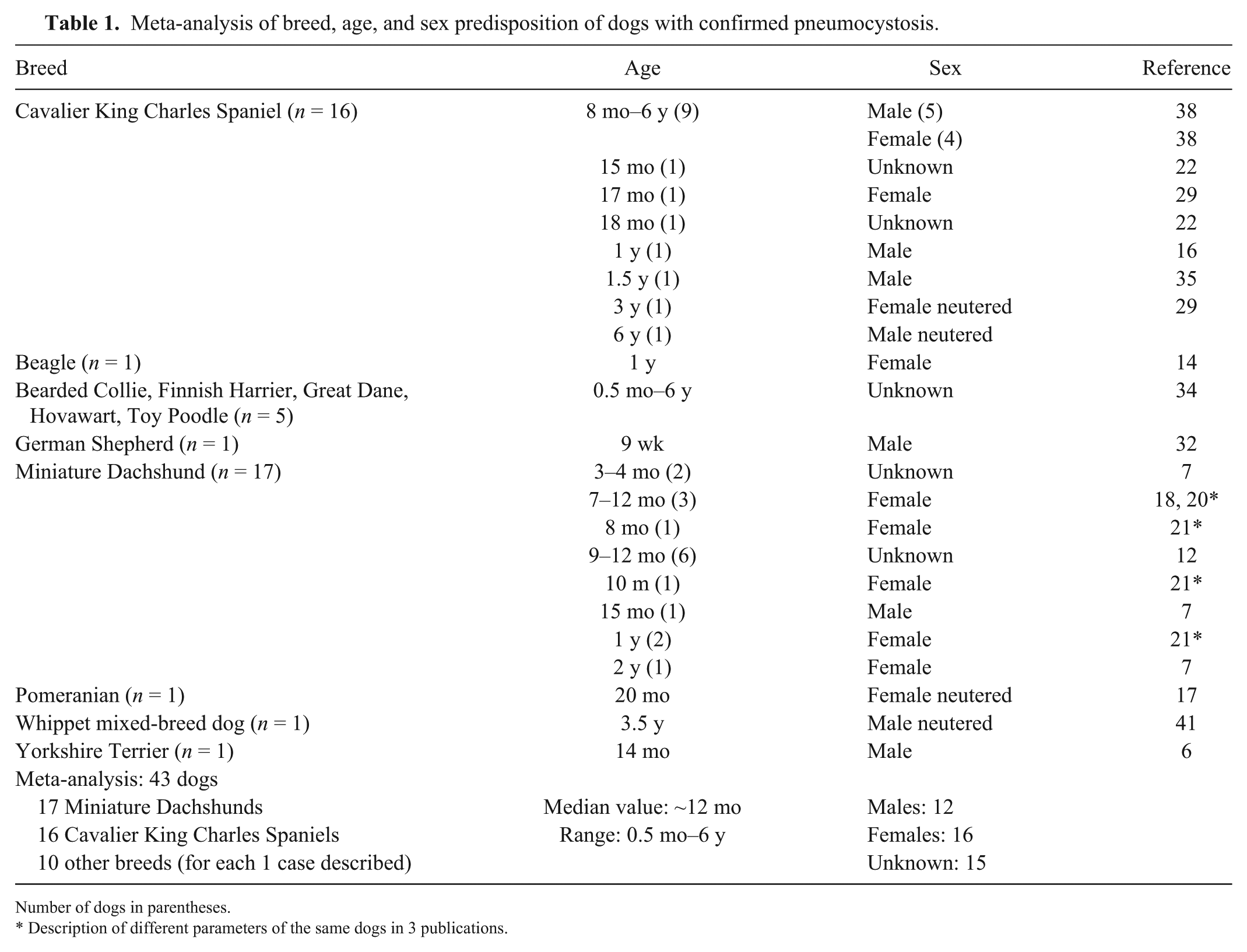
Number of dogs in parentheses.
Description of different parameters of the same dogs in 3 publications.
Meta-analysis of clinical signs and survival rates of dogs with pneumocystosis.
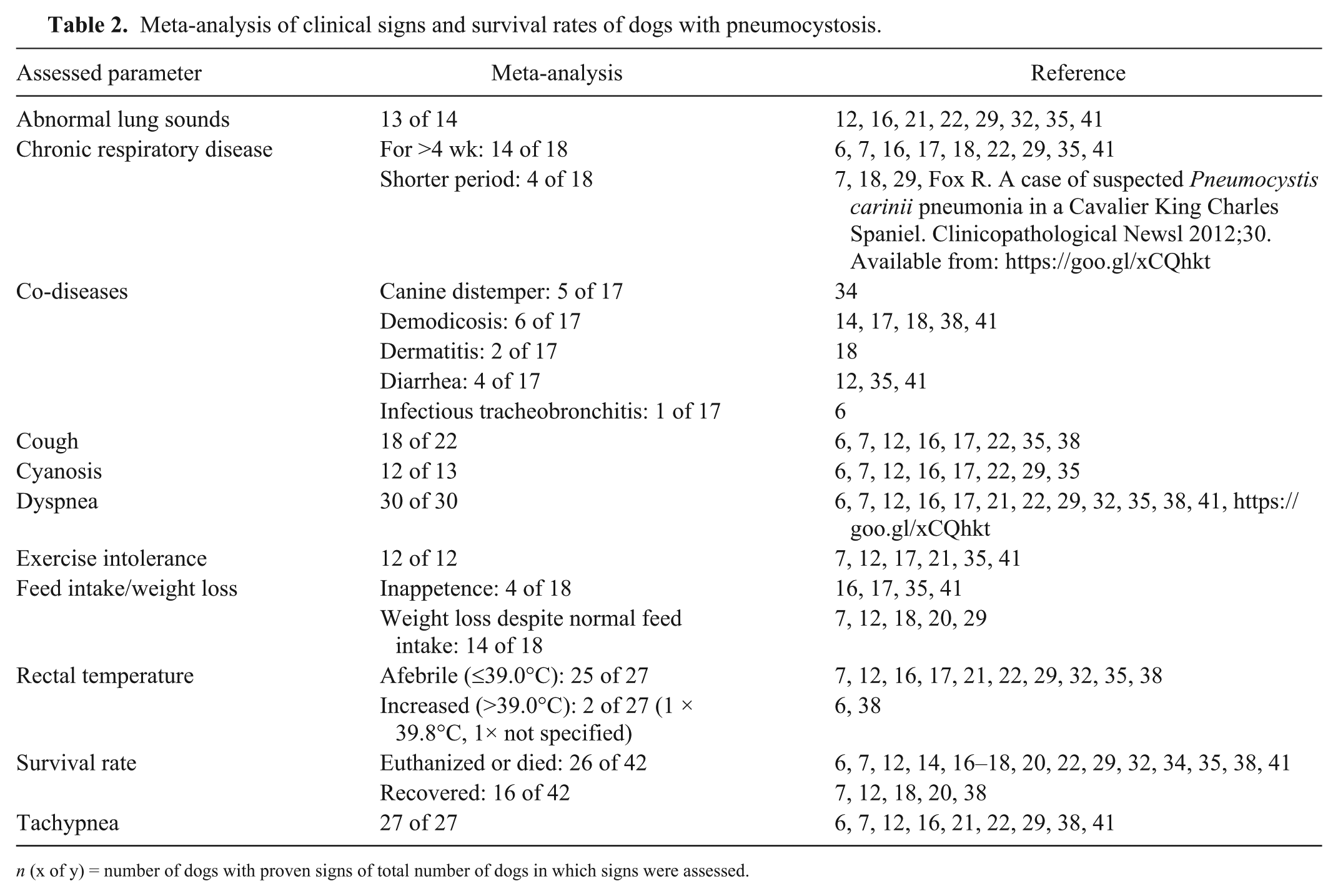
n (x of y) = number of dogs with proven signs of total number of dogs in which signs were assessed.
Meta-analysis of leukogram and serum biochemical parameters of dogs with pneumocystosis.
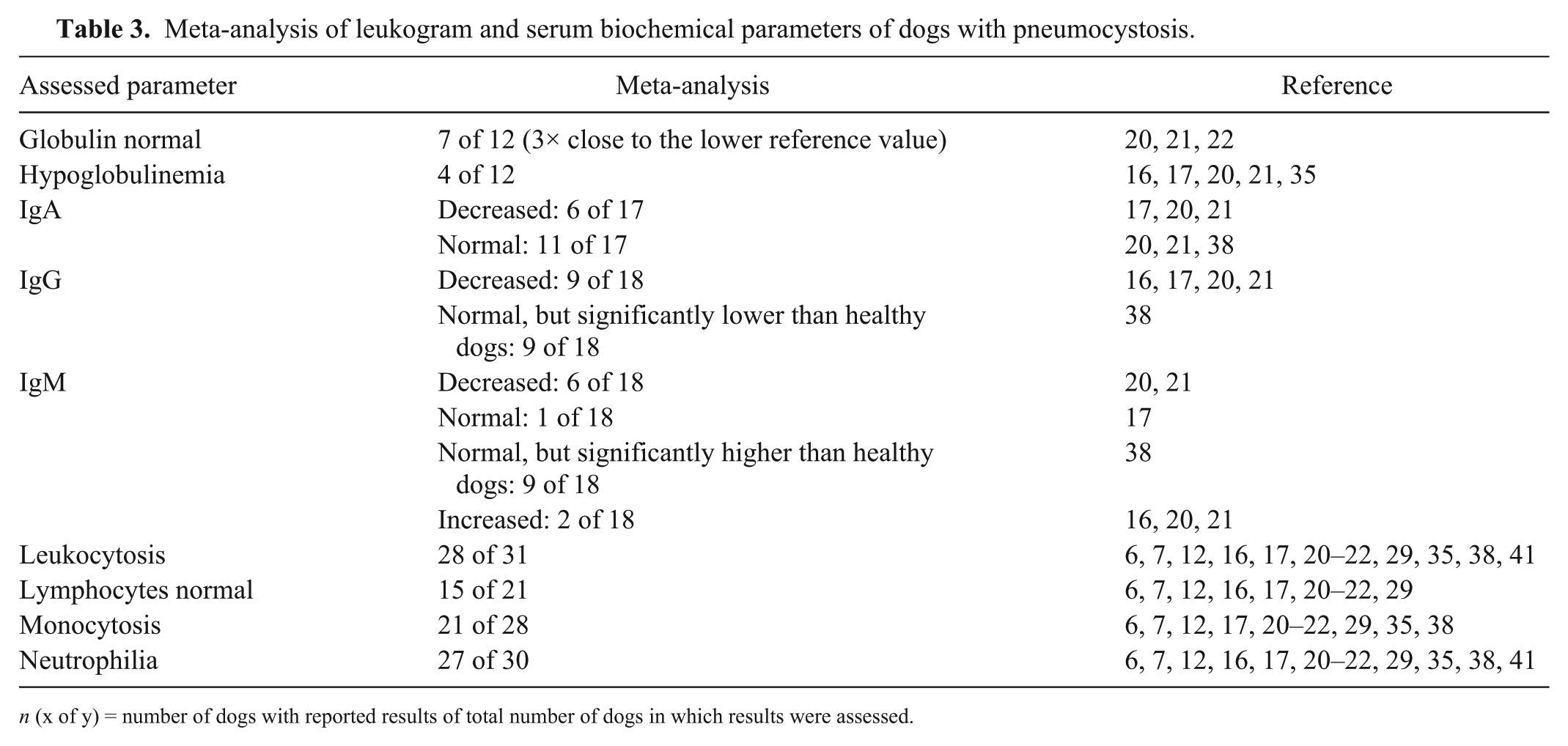
n (x of y) = number of dogs with reported results of total number of dogs in which results were assessed.
Meta-analysis of the thoracic radiography findings of dogs with pneumocystosis.
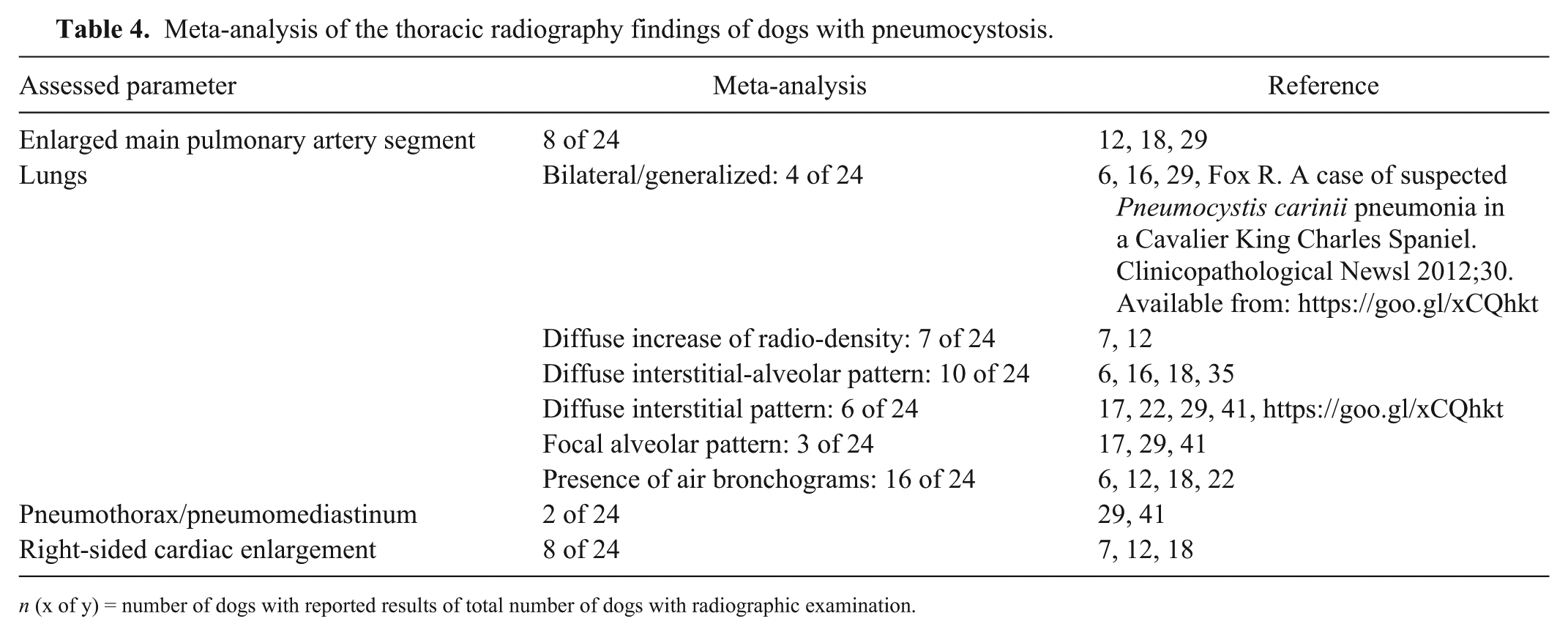
n (x of y) = number of dogs with reported results of total number of dogs with radiographic examination.
Meta-analysis of cytologic results in various sample matrices from dogs with pneumocystosis.
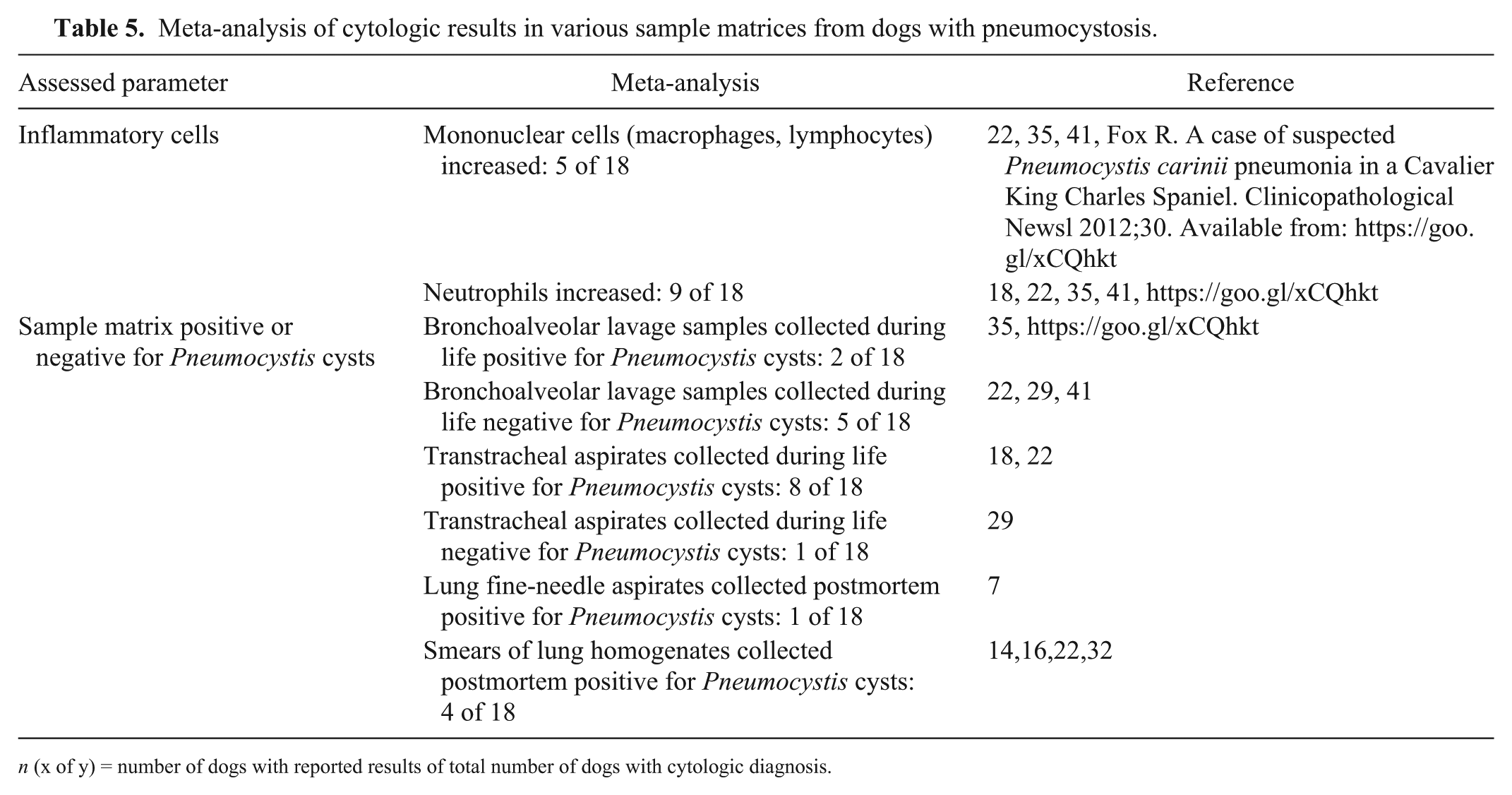
n (x of y) = number of dogs with reported results of total number of dogs with cytologic diagnosis.
Meta-analysis of histopathology results and special stains of the lungs from dogs with pneumocystosis.
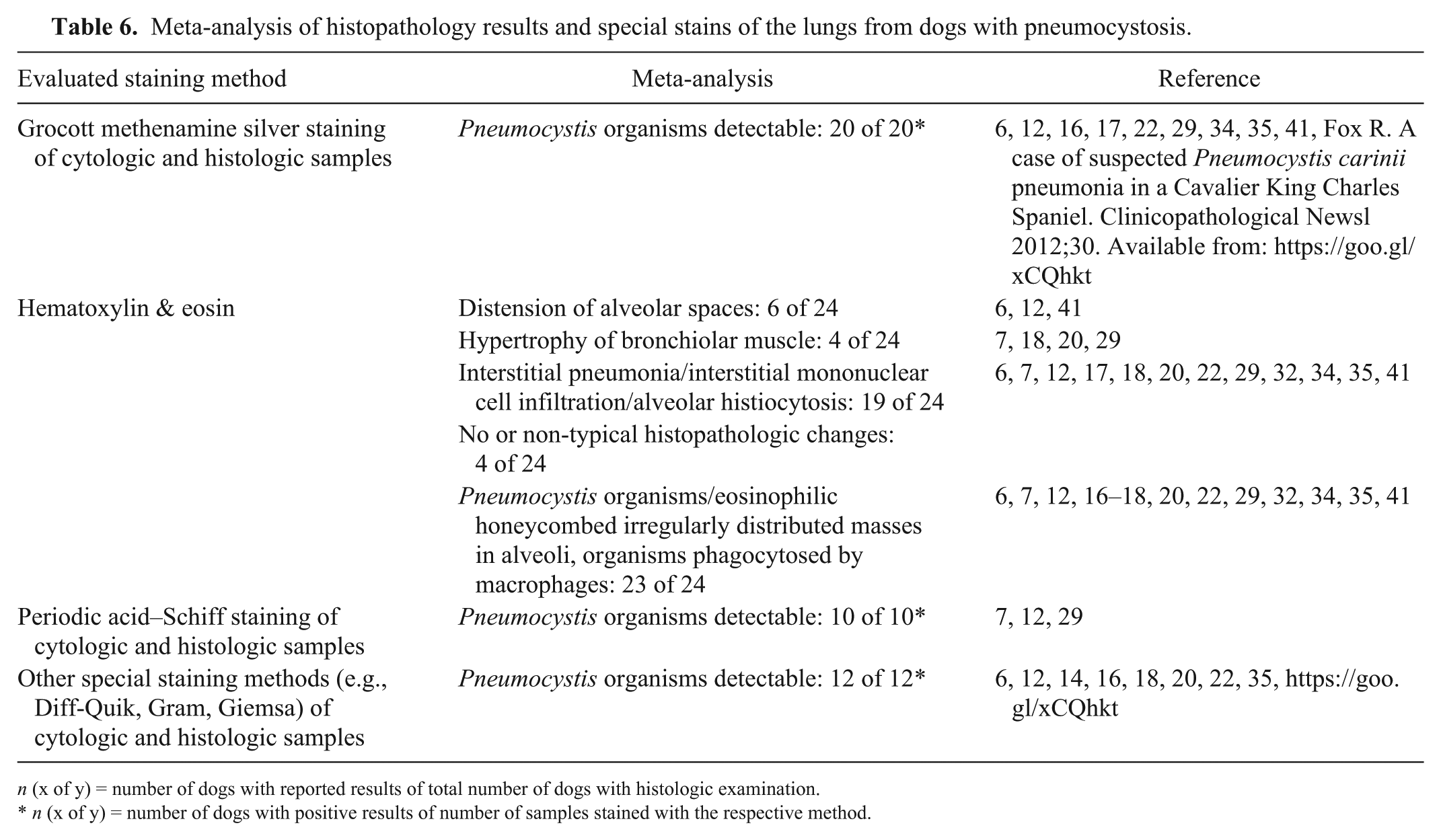
n (x of y) = number of dogs with reported results of total number of dogs with histologic examination.
n (x of y) = number of dogs with positive results of number of samples stained with the respective method.
Meta-analysis of therapy schemes used for dogs with pneumocystosis.
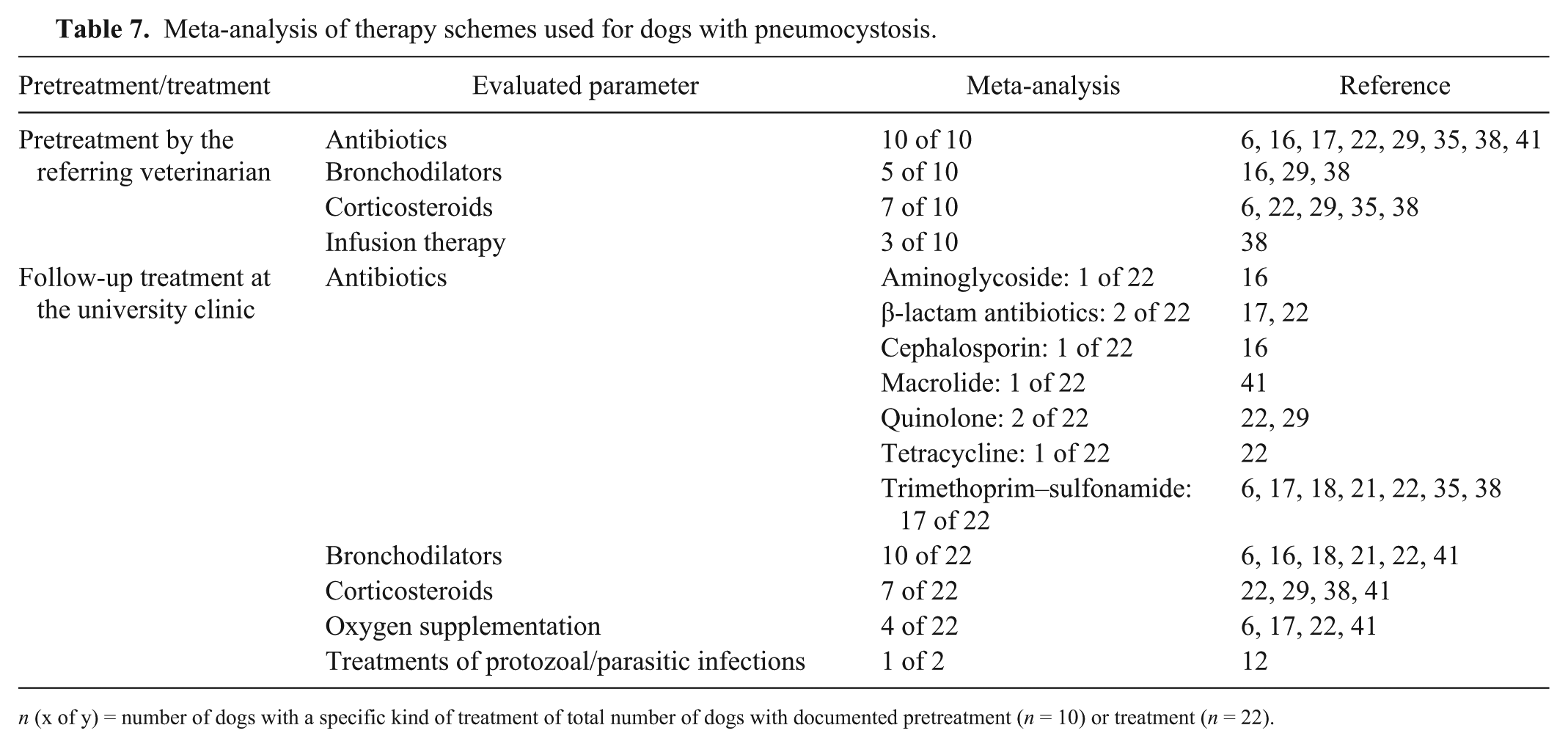
n (x of y) = number of dogs with a specific kind of treatment of total number of dogs with documented pretreatment (n = 10) or treatment (n = 22).
Signalment, medical history, and clinical signs
Seventeen of the evaluated cases were Miniature Dachshunds, followed by 16 Cavalier King Charles Spaniels. Each of the remaining 10 cases belonged to a different breed (Table 1). A breed predisposition for Miniature Dachshunds and Cavalier King Charles Spaniels is evident (SPSS Statistics v.24, IBM, Armonk, NY; χ2 test: p < 0.001). Dachshunds are reported to have a predisposition for combined B- and T-cell immunodeficiency, and typical clinical after-effects, such as severe respiratory tract infections, are documented. 20 Given that Cavalier King Charles Spaniels were more susceptible to pneumocystosis than other breeds, a similar impairment of immunity was also assumed, 38 but has not yet been confirmed. In a 2009 study, 22 2 King Charles Cavalier Spaniel littermates were affected by pneumocystosis, which also supports suspicions of an underlying heritable immunodeficiency in this breed. Nevertheless, the 10 dogs from other breeds, which do not have a known genetic defect in immunity, were also affected by pneumocystosis. In those cases, the underlying immunodeficiency could partly be traced back to chronic coinfections such as demodicosis or canine distemper (Table 2). Pneumocystosis has been described in dogs between 0.5 mo and 6 y old (Table 1). In contrast to the general assumption that infection emerges most commonly among young animals, our meta-analysis showed that older dogs were also affected relatively often. Miniature Dachshunds were infected with Pneumocystis predominantly before 1 y of age.
Clinical signs that were described in association with confirmed Pneumocystis infections included altered lung sounds, cough, cyanosis, dyspnea, exercise intolerance, increased rectal temperature, reduced feed intake, tachypnea, and weight loss (Table 2). In many cases (14 of 18), a long history of respiratory disorders had been documented. According to the dogs’ anamnesis, pretreatment by the referring veterinarian had either brought only temporary partial improvement6,22,38 or had failed completely16,17,29,38,41 for the following reasons: Pneumocystis infection was not considered as a probable differential diagnosis of chronic respiratory disorders,6,16,17,22 or cytologic examination did not identify Pneumocystis as a cause of the dog’s respiratory distress.29,41 Frequently observed clinical signs were nonspecific and included weight loss despite normal feed intake (14 of 18) and exercise intolerance (12 of 12). Signs associated with impairment of the respiratory tract included dyspnea (30 of 30), tachypnea (27 of 27), cyanotic mucous membranes (12 of 13), and cough (18 of 22). Most of the dogs were afebrile (25 of 27), and only 2 dogs had an increased body temperature, but only in 1 dog was it exactly defined (39.8°C). 6 Consequently, pneumocystosis in dogs is not commonly associated with a fever. This parameter is primarily influenced by coinfections. The results of auscultation of the lungs were too variable to draw further conclusions. However, clinical signs might be masked by other conditions caused by various infectious agents. Given the lack of specificity of clinical signs, further testing is essential for confirmation of Pneumocystis infections in dogs.
In the studies evaluated, 26 dogs had died or were euthanized and 16 had recovered (Table 2). Long-term outcome of recovery was only available for 5 dogs.21,29,38 One of them was re-examined 4 mo after the first presentation, and respiratory signs had resolved completely. 21 The second dog died 10 wk after the initial development of signs, but the cause of death was not specified. 29 Dogs in a 2006 study 38 were alive at least 2.5 y after diagnosis and treatment; 2 of the dogs had several recurrences of signs of respiratory dysfunction and were responsive to sulfonamide therapy, although a definitive diagnosis of recurrent pneumocystosis was not confirmed. The survival rate of the dogs included in our meta-analysis was estimated based on all dogs declared as “recovered” and was generally low (~38%).
Laboratory parameters
Leukocytosis (28 of 31) and neutrophilia (27 of 30) were detected most commonly (Table 3). Additionally, monocytosis was observed in many cases (21 of 28). The lymphocyte counts of the documented dogs were too variable to draw conclusions; 15 of 21 dogs had counts within the reference interval. In humans, attempts were initiated to find variables significantly associated with the lethal outcome of Pneumocystis pneumonia. Total protein, serum albumin, gamma globulins, and C-reactive protein have been associated with an increased risk of in-hospital mortality and have been helpful in identifying patients at risk.3,11,30 We cannot definitively suggest the usefulness of most of these parameters in dogs because of the limited data available in our meta-analysis.16,17,22,35 However, we did confirm the diagnostic value of hypoglobulinemia or hypogammaglobulinemia, which was present in 4 of 12 cases; additionally, 3 of 12 dogs had globulin levels close to the lower reference value. The determination of immunoglobulin levels is useful and can be recommended. IgG levels were reported to be decreased (9 of 18) or normal, but lower than in healthy dogs (9 of 18). IgM levels were decreased (6 of 18), normal (1 of 18), normal, but higher than in healthy dogs (9 of 18), or increased (2 of 18). The reason for this immunologic pattern is the so-called class-switching immune defect that results in a selective defect in IgG production with low serum concentrations of this immunoglobulin. 38 Dogs infected with Pneumocystis mount an IgM response instead of an IgG response, which is a sign of the inability of antigen-activated B-cells to efficiently switch to IgG production. Also, after response to therapy or vaccination, IgG levels remain low in these dogs. 38 The liver enzymes alanine aminotransferase and alkaline phosphatase were increased in dogs that received appropriate treatment for their Pneumocystis infection.16,41 Reasons for increased liver enzyme activities are either long-term medication with trimethoprim–sulfonamide 31 or extrapulmonary pneumocystosis with liver involvement. 5 Another recommended parameter is serum lactate dehydrogenase, which has been reported to have prognostic value in humans. High initial activities during treatment correlate with a worse prognosis, but can also result from various non–Pneumocystis-related etiologies.27,45 There is no experience with this parameter in dogs, to our knowledge.
Thoracic radiography
In dogs with suspected disorders of the lower respiratory tract, thoracic radiography should be performed routinely to exclude certain differential diagnoses and to estimate the extent of lung lesions. Typically, the disease results in bilateral, diffuse, symmetrical reticular or granular opacities. 10 Nevertheless, this classical pattern does not occur obligatorily, and opacities can also be seen unilaterally, focally, and asymmetrically. In our meta-analysis, radiographic examination was carried out in 24 of 43 dogs. The thoracic radiography findings of the lung were relatively nonhomogeneous (Table 4). Thus, radiographic findings associated with a Pneumocystis infection are rather nonspecific. However, radiographic examination of the thorax is an essential prerequisite in the diagnostic work-up of suspected cases of pneumocystosis, in particular to evaluate the presence of pneumomediastinum or pneumothorax, which are rather common complications of Pneumocystis pneumonia in humans.10,25 In cases with non-traumatic pneumothorax or pneumomediastinum, Pneumocystis infection should get higher significance in the list of the most probable differential diagnoses.
Autopsy
Autopsy was carried out in 19 of 43 dogs. Findings were similar in most of the assessed cases, and lungs were usually described as firm or consolidated (15 of 19),7,12,17,18,22,29,35 discolored (11 of 19).12,18,22,35 pale (9 of 19),12,18 or rubbery (8 of 19).7,12,35 Several authors described a miliary pattern (4 of 19).6,29,32,35 Pleural reactions were seen only sporadically (2 of 19).6,22
Detection of the pathogen by cytology, histopathology, and special staining methods
In human medicine, bronchoscopy with collection of bronchoalveolar lavage fluid (BALF) is considered the “gold standard” diagnostic procedure for pneumocystosis. 44 In the cytologic specimen, the pathogen appears as large numbers of multinucleate bodies, approximately the size of red blood cells, containing 8 nuclei. Foamy, slightly eosinophilic, empty globular structures can also be observed. Total cell counts and the number of inflammatory cells, mainly neutrophils, are also commonly increased. Moreover, in humans, the pathogen is not visualized in 32–80% of pneumocystosis cases. 33 Evaluation of Giemsa-stained cytology slides requires experience, especially when the numbers of Pneumocystis organisms are low, because the typical structures can be missed easily. Unfortunately, Pneumocystis has not been detected reliably in BALF of dogs.22,29,35 In our meta-analysis, lung fine-needle aspirates or smears collected either from canine lungs postmortem or from the trachea antemortem were positive in nearly all cases, whereas BALF samples were more commonly negative (Table 5).
The histologic examination of H&E-stained slides (Table 6) typically detected interstitial pneumonia with infiltrates of macrophages, lymphocytes, and plasma cells. Hyperplastic type II pneumocytes and syncytia lined alveolar spaces, which were variably filled with foamy eosinophilic material or eosinophilic spherical bodies. These spherical bodies were found both free in the alveolar space and intracellularly within alveolar macrophages. Only the internal structures of the cysts stain weakly with H&E; cyst walls and trophozoites remain unstained (Fig. 1A). 15 The fungus has a foamy, honeycomb-like appearance, and the identification of only a few intra-alveolar aggregates may be problematic. Furthermore, Pneumocystis may be indistinguishable from edema fluid, which can have a similar finely granular appearance. 4 This may explain why infections with Pneumocystis are sometimes overlooked on histologic examination. Although H&E stain is a useful tool for the histologic evaluation of tissue samples, it is inappropriate for reliable detection of Pneumocystis.
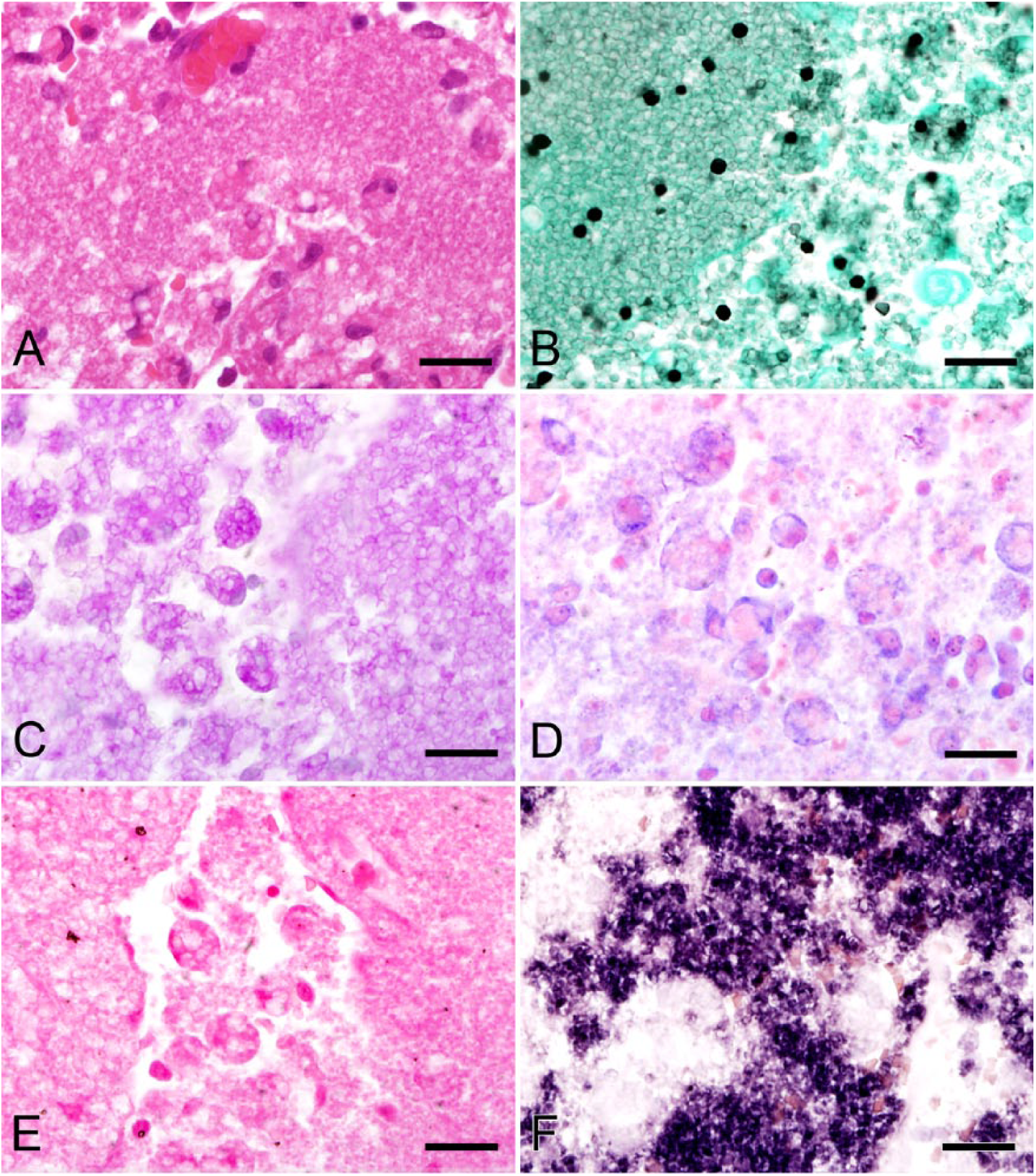
Lung of a dog with a severe pneumocystosis; the pulmonary architecture is effaced; alveoli are diffusely filled with Pneumocystis organisms, which are predominantly free or phagocytosed by macrophages.
In cytology and histopathology, special stains are mandatory to confirm the presence of Pneumocystis organisms, 39 but staining results are variable. In cytologic smears as well as in paraffin-embedded tissue samples, standard Giemsa, Wright, or H&E stain should be supplemented by Grocott methenamine silver (GMS) stain,12,22,29 which is known to be more sensitive. 40 GMS-stained slides are probably easier to evaluate than slides stained with any other method, because of a higher color contrast of the black cyst walls against the mainly green background (Fig. 1B). However, the disadvantage is that only cysts are stained positively, whereas the larger proportion of Pneumocystis organisms, the trophozoites, remain unstained, which could be a problem in cases with a low number of organisms present. 15 Also with periodic acid–Schiff (PAS) stain, only cell walls of cystic stages are captured (Fig. 1C). Additionally, the evaluation is more complex because cell walls and surrounding tissue are both stained in different shades of pink and red. 15 Polychrome stains, such as Giemsa (Fig. 1D) and Diff-Quik, 9 stain the nuclei pink-purple and the cytoplasm blue and are, for this reason, probably easier to evaluate. Pneumocystis cell walls are not stained and appear as a clear halo around the cystic forms. The biggest advantage of these methods lies in staining trophic forms, which remain unstained in GMS and PAS stains. 9 In Gram stain, the nuclei of Pneumocystis cysts are stained gram-negative; cytoplasm and cell walls remain unstained (Fig. 1E). 13 Compared to GMS, Diff-Quik 26 and Gram stain 13 have a significantly lower sensitivity, but are relatively simple procedures that give quick results. 13 In 2017, Giemsa, Diff-Quik, and Gram stains are used most commonly for cytology purposes. 9 Application of an appropriate special staining method enhances a correct cytologic or histologic diagnosis. However, these methods are only useful for screening purposes. The reliability of results is limited, even in the hands of experienced laboratory personnel. PCR testing of BALF or lung aspirates has proved useful in dogs and pigs8,42 and should probably be attempted more often, as the requirement to perform open lung biopsies to secure a diagnosis is unnecessarily invasive.
Further methods for the detection of the pathogen
According to our meta-analysis, electron microscopy (10 of 10),6,12,29,35 immunofluorescence (1 of 1), 14 IHC (3 of 3),29,35 ISH (1 of 1), 41 and PCR (5 of 5)14,16,17,35,41 are reliable methods for the confirmation of Pneumocystis infection. Pneumocystis can be identified easily by electron microscopy. Cystic and trophic stages can be distinguished, and, additionally, structural tissue lesions can be further evaluated. However, compared to other procedures, this method is expensive, time-consuming, and requires access to a specially equipped facility.
Immunofluorescence has only been reported once for the detection of canine Pneumocystis. 14 In humans, advantages and disadvantages of this technique have been investigated thoroughly. Compared to GMS stain, immunofluorescence has higher sensitivity. 23 Compared to PCR analysis, sensitivity and specificity are lower. 36 A fluorescence microscope is required for sample evaluation, whereas IHC and ISH samples can be analyzed using a standard light microscope.
IHC has been introduced to improve sensitivity as well as specificity of Pneumocystis detection. This technique is cost-effective, fast, and simple to perform. Moreover, the presence of the pathogen can be correlated with histologic lesions. However, antibodies validated for detection of canine Pneumocystis are not available commercially. An IHC kit established for the detection of Pneumocystis jirovecii in humans has been used successfully for the detection of Pneumocystis in dog lung samples. 35 Unfortunately, no data about sensitivity or specificity are available, to our knowledge.
ISH is simple to establish, has higher sensitivity and specificity, especially compared to cytologic and histologic methods, and allows detection of both Pneumocystis cysts and trophozoites (Fig. 1F).4,41 This method uses probes to detect specific nucleic acids while preserving tissue morphology so that the morphology of the fungus and the tissue reaction to the organism can be visualized. The probes target unique, organism-specific ribosomal RNA, which is distributed throughout the fungus in large amounts, providing ample opportunity for hybridization. 4
Another very convenient method for pathogen detection is PCR.41,42 In contrast to ISH, which is limited to tissue sections, PCR can also be used for BALF samples, and invasive surgical interventions can be avoided. Furthermore, the high sensitivity of PCR analysis may be of advantage if Pneumocystis cannot be determined cytologically in BALF samples. 41
Treatment of pneumocystosis
In dogs with Pneumocystis pneumonia, immediate treatment is essential for recovery. A missed or delayed diagnosis can lead to progression of disease with severe respiratory dysfunction. Our meta-analysis revealed that successful antimicrobial therapy was most commonly trimethoprim–sulfonamide (Table 7); 11 of 17 dogs treated with this therapeutic regimen survived.18,20,38 During the course of pneumonia, alveolar macrophages generate various mediators that potentiate the inflammatory response towards Pneumocystis. 37 This massive release of mediators may increase pulmonary injury and respiratory impairment. 43 Respiratory disease and death correlate more closely with the extent of lung inflammation than with the burden of Pneumocystis organisms 19 and, for this reason, severe pneumocystosis responds favorably to a combination of corticosteroids and antimicrobial drugs. 24 The dosage of applied corticosteroids has to be considered carefully; low anti-inflammatory doses improve pulmonary function and increase the chance of survival, whereas high immunosuppressive levels facilitate replication of the fungus. 2 In our meta-analysis, corticosteroids were only administered in single studies either during pretreatment by the referring veterinarian or follow-up treatment at the university clinic; 3 of 7 dogs treated with corticosteroids survived. In these 3 dogs, prednisolone was administered orally at a dosage of 0.5 mg per kg body weight. 38 However, the same anti-inflammatory dose was administered to dogs from 2 other studies in which both dogs died.35,41 The administration of an immunosuppressive dose of prednisolone of 15 mg q12h has only been described once in a Cavalier King Charles Spaniel. 22 Because pneumocystosis occurs only rarely in dogs, there is little experience with the regulation of corticosteroid concentrations and the balance between immunosuppression and proliferation of the fungus. Additionally, predisposition for Pneumocystis infections of dog breeds with inherited immunodeficiency20,38 should be considered in the choice of an appropriate therapy.
Conclusion
Our meta-analysis objectively evaluates findings from various case reports and studies regarding confirmed Pneumocystis infections in dogs. Distinct breeds of dogs with a predisposition for impaired immunity are affected more often than dogs from immunologically stable breeds (p < 0.001). Nevertheless, immunodeficiency caused by coinfections is of equal importance for infections with Pneumocystis. One-y-old dogs are most commonly, but not exclusively, affected. The factors of breed, age, evidence of impaired immunity, presence of chronic coinfections, as well as a history of chronic therapy-resistant respiratory disorders are essential considerations for placing pneumocystosis on a clinical differential list or for making a presumptive clinical diagnosis. Clinically, affected dogs commonly have nonspecific respiratory signs, exercise intolerance, and cyanotic mucous membranes. Most often, dogs with Pneumocystis infection do not have a fever. Thoracic radiographic findings are variable, and alterations are not pathognomonic for pneumocystosis. According to our meta-analysis, hematologic alterations seen with Pneumocystis pneumonia are leukocytosis, neutrophilia, and monocytosis. Gamma globulin (hypogammaglobulinemia with decreased IgG and increased IgM values) was the only changed biochemical parameter. The investigation of BALF samples represents a promising and noninvasive method. Because cytologic examination using routine staining methods is frequently negative, specific staining methods, such as GMS, can essentially improve detection sensitivity. If Pneumocystis cannot be identified cytologically in BALF samples, the more sensitive PCR analysis is indicated. However, in case of a non-diagnostic lavage sample, the collection of lung biopsy samples can be considered as a final option for a definitive diagnosis during life. Additionally, this sample matrix allows the histologic investigation of lung lesions as well as the performance of other sensitive detection methods, such as ISH. Evaluation of therapy schemes showed that the prompt use of trimethoprim–sulfonamide combined with low anti-inflammatory doses of corticosteroids substantially increases the survival chances of affected dogs.
Footnotes
Acknowledgements
We thank Karin Fragner and Klaus Bittermann for their excellent technical support.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.