
Abstract
Citrobacter freundii is considered a ubiquitous organism and an opportunistic pathogen. Reports of C. freundii–associated disease in mammals have been very limited. We report an outbreak of C. freundii septicemia and encephalitis in sheep, with a high mortality rate; 13 adult sheep were found dead over a 6-d period on a farm in central China that housed ~1,370 sheep. Three animals were autopsied and showed septicemia, congestion of meningeal vessels, and pleural effusion. C. freundii was isolated in abundance in pure culture from 19 of 21 organs. All 3 C. freundii isolates had similar antimicrobial resistance phenotypes for 10 of the 11 agents tested, and were sensitive to 8 of the 11 agents. We reproduced C. freundii infection in sheep experimentally by oral or subcutaneous inoculation routes, and recovered the challenge organism from all of the experimentally infected sheep. Intramuscular injection of enrofloxacin protected sheep against an otherwise fatal challenge. Our results suggest that C. freundii played a major role in this disease outbreak.
Keywords
Citrobacter freundii (genus Citrobacter, family Enterobacteriaceae) is classically considered a ubiquitous and opportunistic pathogen. In humans, C. freundii causes urinary tract infections, diarrhea, pneumonia, and, rarely, meningitis and intracranial abscesses.9,16,17,20 During the past few years, there have been reports indicating that C. freundii is associated with fatal infections in reptiles and aquatic animals.5,7,8 In addition, C. freundii is highly pathogenic in young and immunosuppressed avian hosts, causing septicemia and hepatitis. 10 However, reports of the pathogenicity of C. freundii in mammals have been very limited and have involved non-lethal infections.1,6,15 We describe herein sheep with severe septicemia and encephalitis caused by systemic infection with C. freundii.
Our cases originated on a large-scale farm housing ~1,370 small-tail Han sheep in 7 breeding barns, in Henan province in central China (114.81°E, 34.69°N). When the disease occurred, 461 ewes were housed in 3 adjacent open-sided breeding barns year-round. All sheep were in good body condition, and no significant health problems had been detected prior to the fatal outbreak.
On January 6, 2014, 4 of the sheep (females, ~10-mo-old) in 1 breeding barn showed depression, anorexia, ataxia, and cyanosis of the visible mucous membranes and axillary skin. The animals were treated with benzylpenicillin potassium (30,000 units per kg, intramuscularly [IM], once daily). Within ~2 h of antibiotic treatment (3 h after the initial clinical signs were noted), the condition of the sheep began to deteriorate. The animals exhibited neck rigidity, nasal discharge, and lacrimation. An intense pain reaction to abdominal touch was also evident; gentle stroking of the abdomen caused high-pitched bellowing. Seizures, blindness, and signs of other cranial nerve deficits were not observed. Ataxia was confined to the hindquarters, and rapidly progressed to complete recumbency or immobility. Patellar, perineal, and hindlimb withdrawal reflexes were absent.
At 1 h after the initial clinical signs, the rectal temperatures of the diseased sheep were 41.2–41.4°C (normal: 38.0–40.0°C), and the heart rates were ~110 beats per min (normal: 70–80 beats/min) with mild arrhythmia. In addition, the sheep had dyspnea, abdominal respiratory effort, and a respiratory rate of 50 breaths per min (normal: 12–30 breaths/min). After ~5 h of antibiotic treatment (6 h after the initial clinical signs were noted), 2 of the 4 diseased sheep died suddenly. Considering that penicillin might not be effective, the other 2 sheep were immediately treated with enrofloxacin (2.5 mg/kg, IM, twice daily). After 4 d of enrofloxacin treatment, the sheep began to improve gradually, and recovered completely.
In the same week as the above cases were beginning, 13 more sheep (all female, ~10-mo-old) with similar clinical signs were found dead in the same barn. All 13 dead animals were in good body condition. All sheep in the same barn (defined as sharing an air space with the dead sheep) were treated with enrofloxacin (2.5 mg/kg, IM, twice daily) for 5 d beginning on January 11, 2014. No more sheep died after this treatment began.
Three of the dead animals (that were not treated with antimicrobials and died on January 8–11, 2014) were presented for postmortem examination; all 3 had similar gross lesions of septicemia. Red clear liquid (~400 mL) was found within the thoracic cavity. Other lesions included congestion of meningeal vessels; severe congestion and diffuse hemorrhages in the lungs; diffuse hemorrhages in the spleen; petechial epicardial hemorrhages; minor hemorrhages in the liver, kidneys, and small large intestine; and swelling of mesenteric lymph nodes.
Tissue samples were processed routinely for histology and stained with hematoxylin and eosin. Microscopically, congestion and hemorrhage were observed in lungs, heart, and spleen. In addition, there were minor hemorrhages in the liver, kidneys, small and large intestine, and mesenteric lymph nodes. Nonsuppurative encephalitis was present.
Samples of heart blood, lung, brain, liver, spleen, kidney, and mesenteric lymph nodes, collected during postmortem examination, were cultured on trypticase soy agar (TSA; Difco, Becton Dickinson, Sparks, MD) containing 5% bovine serum, and on MacConkey agar (Solarbio, Beijing Solarbio Science and Technology, Beijing, China). The plates were incubated for ≥24 h at 37°C in aerobic conditions. The TSA plates for 19 of 21 samples yielded a pure growth of gray, opaque, convex, moist, smooth round colonies of 1.5–2.0 mm diameter. The corresponding MacConkey agar plates had a pure growth of pink colonies. The only samples that did not yield growth were the liver of animal 2 and the kidney of animal 3. Microscopic observation of the isolates showed gram-negative bacilli typical of family Enterobacteriaceae. Identification (Bact-IST auto microbial ID/AST analyzer, DL Biotech, Zhuhai, China) demonstrated that all 19 isolates from the 3 dead sheep were C. freundii.
The identity of the 3 isolates from heart blood was further confirmed by 16S ribosomal (r)DNA gene amplification and sequencing using universal primers 27F (5′-AGAGTTTGATCMTGGCTCAG-3′) and 1493R (5′-TACGGTTACCTTGTTACGACTT-3′). 11 Amplification involved initial denaturation at 94°C for 4 min, followed by 30 cycles of denaturation at 94°C for 30 s, an annealing temperature of 55°C for 30 s, and extension at 72°C for 1.5 min. The final extension was performed at 72°C for 10 min. The almost complete 16S rDNA gene (1,440 nucleotides) of 3 isolates (LK-1, LK-2, and LK-3) was obtained by sequencing the PCR product (GenBank accessions KP068655, KP224273, and KP224274). A comparison of these sequences with those available from GreenGenes using BLAST (http://www.greengenes.lbl.gov) revealed that the 3 isolates were genotypically identical and were >99.8% similar to the 6 C. freundii strains A11-1, An16-1, w1, JCM 24061, JCM 24004, and DSM 30039 (GreenGenes accessions AB244300.1, AB244451.1, FJ544405.1, AB548826.1, AB548577.1, and NR_028894.1).
All 3 C. freundii isolates were tested for their in vitro susceptibility to 11 antimicrobial agents by the disk diffusion method on Mueller–Hinton agar. The performance and evaluation of the susceptibility tests were in accordance with the recommendations of the Clinical and Laboratory Standards Institute (CLSI).3–5 After inoculating the bacteria onto Muller–Hinton agar and placing the antibiotic disks, the plates were incubated at 37°C for 24 h. The disks were supplied by one source (GYZ-15e, Binhe Microorganism Reagent, Hangzhou, China) except for the disks for furazolidone and enrofloxacin (Tianhe, Hangzhou, China). According to the inhibition zone around the disks, the results were categorized and reported in 3 groups: susceptible (S), intermediate susceptibility (I), and resistant (R).2,3,4 The interpretation criteria used for ampicillin, amoxicillin, kanamycin, tetracycline, trimethoprim–sulfamethoxazole, norfloxacin, enrofloxacin, ofloxacin, and ciprofloxacin were those recommended by the CLSI for Enterobacteriaceae.2-4 For spectinomycin, the criteria used were those recommended by the CLSI for Neisseria gonorrhoeae.2,3 For furazolidone, the criteria used were those of the disk manufacturer’s recommendations for veterinary pathogens (Table 1). Escherichia coli ATCC 25922 and Staphylococcus aureus ATCC 25923 were used as quality control reference organisms in all susceptibility tests. The 3 isolates had similar antimicrobial resistance phenotypes to 10 of the 11 drugs in our study, differing only for amoxicillin (Table 1). The C. freundii isolates were sensitive to 8 antimicrobial agents, including aminoglycosides, fluoroquinolones, tetracycline, and were intermediate to 2, ampicillin and furazolidone.
Susceptibility of 3 Citrobacter freundii isolates to 11 antimicrobials.
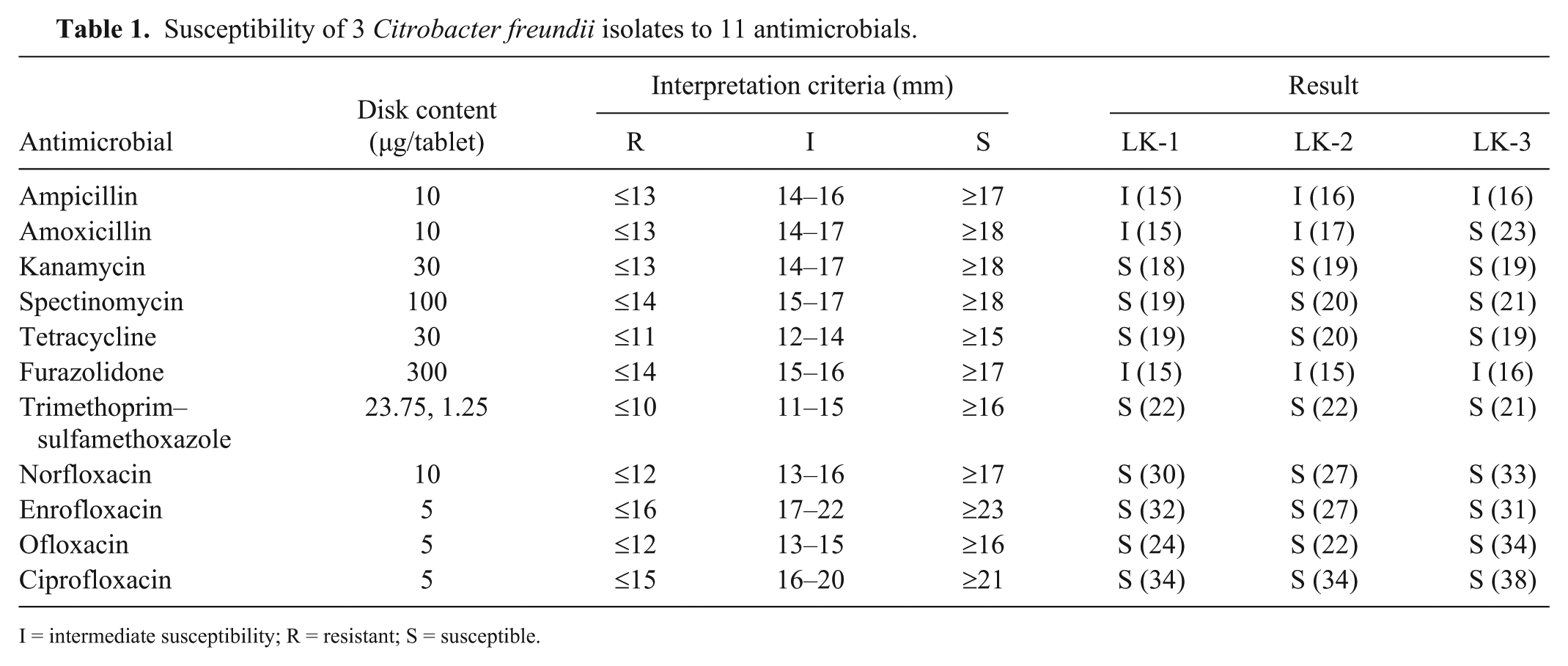
I = intermediate susceptibility; R = resistant; S = susceptible.
Because the ability to reproduce C. freundii infection in sheep would further confirm the role of the organism in natural infections in sheep, we conducted the following study. Animal handling and other procedures were approved by the Biosafety and Animal Welfare Committee of Henan University of Science and Technology. Fifteen 30–35 kg, healthy small-tail Han sheep ~8-mo-old (born in the same flock within the same lambing season from synchronized ewes) were randomly assigned to 4 groups (A1–A4; n = 4, 3, 4, 4, respectively), numbered and housed in separate rooms. For oral infection, isolate LK-1 was cultured in trypticase soy broth for 16 h and enumerated by a spread plate method. 14 The 4 animals in group A1 were deprived of food and water for 4 h and were then infected orally with 2.2 × 109 colony-forming units (CFU) of isolate LK-1 diluted in 50 mL of phosphate-buffered saline (PBS); food and water were returned 1 h after oral administration. 14 As a negative control, the 3 animals from group A2 were each given 50 mL of PBS by the same method. For subcutaneous infection, groups A3 and A4 were inoculated subcutaneously in the neck with 1 mL of LK-1 suspension that contained 2.2 × 109 CFU of bacteria. Simultaneously, the 4 animals in group A4 were each treated with enrofloxacin (2.5 mg/kg, IM, twice daily) for 7 d. The animals were observed 3 times daily until 14 d post-infection (dpi). The sheep in group A2 remained in good health and condition after PBS administration. In addition, no obvious signs of disease were observed during the entire experimental period in the animals of group A4 (Table 2). However, the animals in groups A1 and A3 developed the same clinical signs as those seen in naturally infected sheep, 36 and 48 h after experimental infection, respectively. Furthermore, there were no survivors in these 2 groups; the sheep died 3–7 dpi with wild-type C. freundii LK-1, with peak of mortality on day 4 (Table 2). The lesions in these sheep were similar to those observed when infection occurred naturally. In addition, C. freundii was recovered from heart blood, brain, lungs, spleen, and liver of these infected sheep, suggesting that C. freundii was the pathogen that caused the deaths of these sheep.
Results of oral or subcutaneous experimental infection of sheep with Citrobacter freundii LK-1.
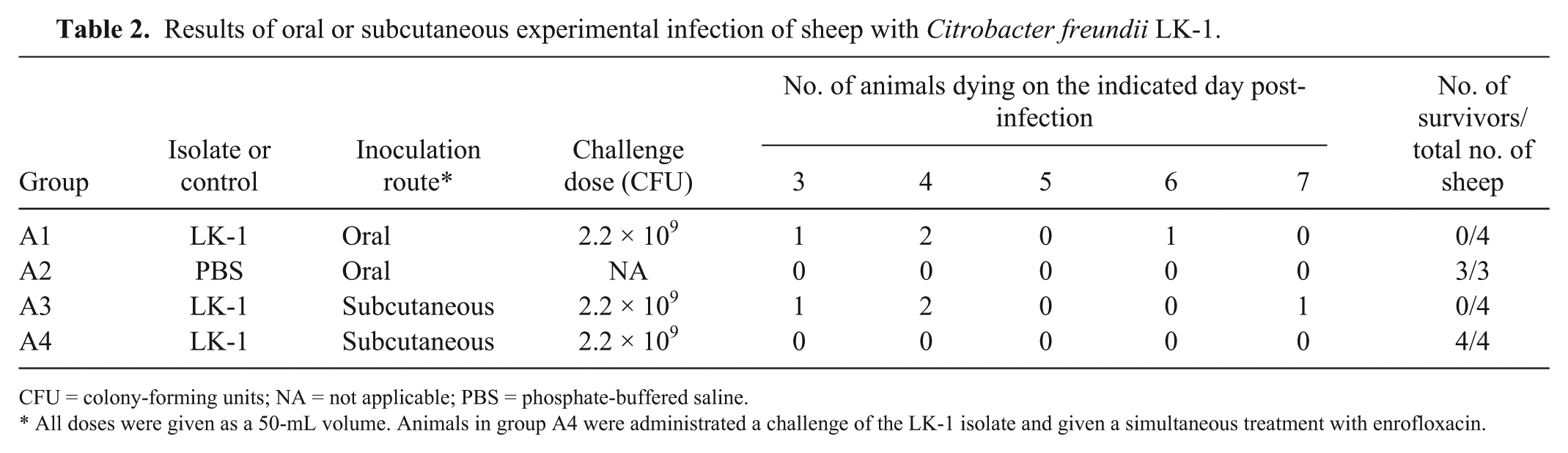
CFU = colony-forming units; NA = not applicable; PBS = phosphate-buffered saline.
All doses were given as a 50-mL volume. Animals in group A4 were administrated a challenge of the LK-1 isolate and given a simultaneous treatment with enrofloxacin.
The gross lesions described above, in association with the microbiologic identification of C. freundii from heart blood and organs of infected sheep, led to a diagnosis of acute bacterial septicemia, encephalitis, and septic shock. No other pathogenic bacteria were isolated from these cases, and experimental infection of sheep reproduced the clinical signs of disease that occurred in naturally infected sheep. In addition, C. freundii was recovered from these experimentally infected sheep. The pathogenic mechanism was not determined here, and this needs to be addressed in further studies.
The differential diagnosis of sudden death in sheep includes clostridiosis, which causes gastric bleeding, bloat, ulcerative colitis, nephropathy, hepatic necrosis, and diarrhea in lambs. 13 Septicemia and encephalitis can also be associated with other neurologic diseases such as listeriosis, polioencephalomalacia, rabies, and tetanus. Listeriosis and polioencephalomalacia can cause ataxia, recumbency, and depression, but affected animals will usually have cranial nerve deficits and central blindness. Rabies may cause disorders of consciousness. Tetanus can cause spasmodic muscle contractions of part or the whole body. 13 Escherichia coli, Pasteurella spp., and Streptococcus equi subsp. zooepidemicus can also lead to bacteremia and encephalitis.12,18,19 Therefore, a definitive diagnosis of C. freundii infection requires isolation and identification of C. freundii.
Footnotes
Acknowledgements
We thank Zijun Yang for excellent technical assistance during autopsy, and Zhijun Liu for advice on the histology review. We appreciate the assistance and interest of the following colleagues: Yang Wang, Hongjun Li, and Mei Liu.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by grants from the National Natural Science Foundation of China (31302106, 31001051, and 31672530), the National Key R&D Program (2016YFD0500700), and the Research and Development Foundation of Henan University of Science and Technology (2015ZDCXY04).