
Abstract
A 10-y-old Watusi (Bos taurus africanus) steer housed at a drive-through game park in Winston, Oregon developed severe clinical illness including fever, marked nasal discharge, injected scleral and conjunctival membranes, plus oral hemorrhages and erosions. The animal responded poorly to supportive treatment and was euthanized. Additional gross findings at postmortem examination included papules and erosive lesions on the tongue, hemorrhagic large intestine, and multifocal cardiac hemorrhages. Histopathologic findings included multifocal lymphoplasmacytic vasculitis plus fibrin exudation in heart and tongue. Total DNA obtained from the splenic samples was positive for alcelaphine gammaherpesvirus 1 (AlHV-1) as tested by a multiplex PCR for malignant catarrhal fever (MCF) viruses. The AlHV-1 detection was further confirmed by amplification and sequencing of a viral DNA polymerase gene fragment, which was identical to AlHV-1 sequences in GenBank. This was the first diagnosis of clinical wildebeest-associated MCF on these premises, although wildebeest have been held at the park for over 25 y. This disease is sporadic in North America and should be considered as a differential diagnosis for febrile illness with ulcerative oral lesions in ruminants.
Malignant catarrhal fever (MCF) is a lymphoproliferative syndrome that affects a wide range of species in the order Artiodactyla and is linked to multiple gammaherpesviruses of genus Macavirus (order Herpesvirales, family Herpesviridae, subfamily Gammaherpesvirinae). 3 The prototypic MCF viruses are species Alcelaphine gammaherpesvirus 1 (AlHV-1), which is responsible for wildebeest-associated MCF (WA-MCF), and species Ovine gammaherpesvirus 2 (OvHV-2), which causes sheep-associated MCF (SA-MCF). SA-MCF has been sporadically diagnosed in cattle, bison, and other ruminant species in North America, and severe outbreaks have been reported, especially in American bison. 9 In zoological gardens and captive wildlife facilities, timely diagnosis of MCF with confirmation of the causative agent is challenging because outbreaks may involve various other MCF viruses, which are carried by different reservoir species. 10 A number of WA-MCF cases involving exotic hoofstock, such as greater kudus (Tragelaphus strepsiceros), banteng (Bos javanicus), and gaurs (Bos gaurus) have occurred in zoos and wildlife parks in the United States. 5 However, diagnosis of most of these cases was based on clinical signs, histopathologic and serologic findings, plus direct or indirect epidemiologic evidence of exposure to wildebeest. Until recently, confirmation of MCF by virus identification was rarely documented, but the development of laboratory assays that allow detection and identification of each of the MCF viruses known to cause disease now provides a reliable way to confirm MCF cases. We describe the diagnosis of clinical WA-MCF in a Watusi steer held in an Oregon drive-through game park.
The affected animal was a 10-y-old Ankole-Watusi steer (Bos taurus africanus) that had been imported from a facility in California as a 5-mo-old calf. It was one of a herd of 10 adult Watusi of various ages. Other hoofstock held in this area of the park included white-bearded wildebeest (Connochaetes taurinus albojubatus), gemsbok (Oryx gazella), scimitar-horned oryx (Oryx dammah), waterbuck (Kobus ellipsiprymnus), and eland (Taurotragus oryx, syn. Tragelaphus oryx), as well as zebras (Equus burchellii), giraffes (Giraffa camelopardalis), and rhinoceroses (Ceratotherium simum). All hoofstock are free to move about the ~485,000 m2 enclosure and share access to various feeding and watering stations.
In October 2015, the steer was found separated from the herd, mildly ataxic, panting, and had abundant nasal discharge. The animal was anesthetized using an intramuscular (IM) dart injection (Pneu-dart, Williamsport, PA) of cocktail of detomidine hydrochloride (Dormosedan [10 mg/mL], Orion, Espoo, Finland), carfentanil (3 mg/mL, Zoopharm, Laramie, WY), and ketamine (200 mg/mL, Zoopharm), followed by hand injections of ketamine (IM), xylazine (intravenous [IV]; AnaSed [100 mg/mL], Lloyd Laboratories, Shenandoah, IA), and propofol (IV; PropoFlo [10 mg/mL], Abbott Laboratories, North Chicago, IL) as needed. Physical examination findings included marked conjunctival and scleral hyperemia (Fig. 1) and pyrexia (41.3°C, normal range: 38.0–39.2°C). Papules and erosive lesions were noted on the tongue (Fig. 2). Blood was collected for possible serologic testing.
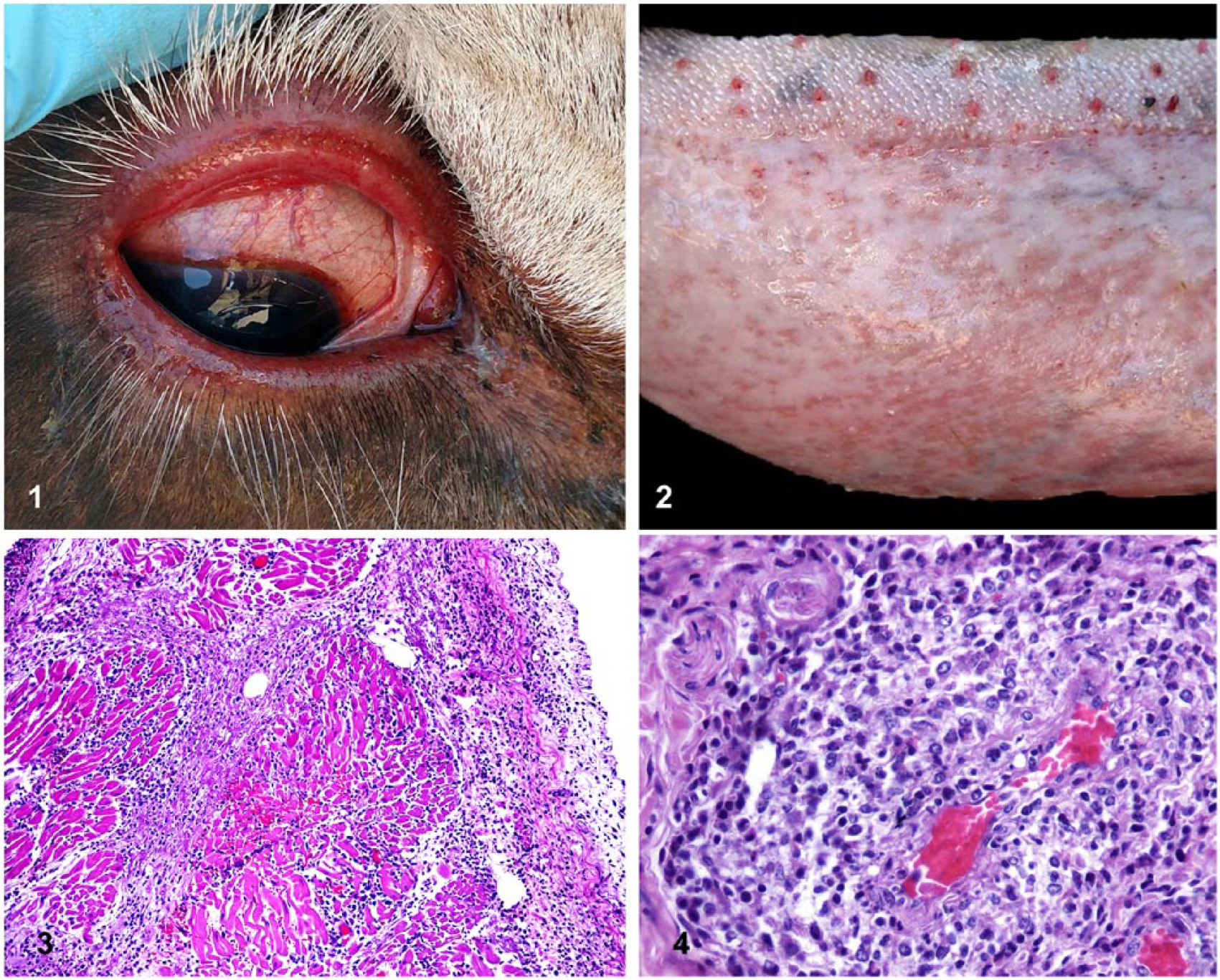
Various lesions in an Ankole-Watusi steer (Bos taurus africanus) with malignant catarrhal fever.
Differential diagnoses included bovine viral diarrhea (BVD), bluetongue (BT), epizootic hemorrhagic disease (EHD), MCF, infectious bovine rhinotracheitis, and vesicular diseases such as foot-and-mouth disease. During the previous year, EHD-related mortalities had occurred in multiple yak (Bos grunniens) at the facility, and those animals had marked scleral injection with pyrexia. Therefore, EHD was considered the prime differential diagnosis. An IV injection of flunixin meglumine (Flunixamine, Zoetis, Florham Park, NJ) and supportive IV fluid therapy was initiated and resulted in a decrease of temperature to 39.7°C but no other clinical improvement. Given the poor prognosis, the steer was euthanized with IV barbiturate within 2 h of initial examination.
In addition to the oral lesions, autopsy findings included multifocal epicardial hemorrhages, pulmonary congestion, and hemorrhage of the colonic mucosa. Various tissues were collected in 10% neutral-buffered formalin for histologic examination. Fresh samples of several organs were also collected.
Histopathologic findings were most striking in the heart, in which there was generalized congestion with multifocal hemorrhage plus multifocal myocardial infiltrates of large lymphocytes, macrophages, and plasma cells, sometimes with mild fibrin exudation. Atrial tissue had more extensive infiltration, expanding endocardial and epicardial tissue with more fibrin, and small numbers of neutrophils joining the leukocytic population (Fig. 3). Multiple vessels had edematous medial tunics, and lymphoblastic cells were occasionally seen in adventitial layers of veins. A section from non-ulcerated glossal tissue contained foci of lymphohistiocytic vasculitis in the subepithelial stroma (Fig. 4). This tissue was markedly congested with fibrin thrombi in a few venules. There was light vacuolation of the basal epithelial layer with small numbers of infiltrating lymphocytes and macrophages. A few apoptotic keratinocytes were seen in the stratum spinosum. The spleen was congested with marked depletion of white pulp. Liver featured diffuse intracellular cholestasis. In addition to light lymphoplasmacytic periportal infiltrates, one quadrant contained a large vein loosely cuffed by pleomorphic lymphocytes and partially occluded by fibrin. The tracheal epithelium had sloughed, but the subjacent stroma contained large numbers of lymphocytes and plasma cells. A section of skeletal muscle included a few fibers with segmental sarcoplasmic coagulation and loss of striations. Autolysis prevented proper assessment of most levels of the gastrointestinal tract. Samples of brain and eye were not available for examination.
Spleen, lung, and rumen were inoculated onto BHK-DVL 494P/495P and DRK 052613 7P/8P cell lines at the Oregon State University Veterinary Diagnostic Laboratory (OSUVDL), but these virus isolation attempts were unsuccessful. Serum tested negative for BT via competitive (c)ELISA) and EHD via agar gel immunodiffusion at the OSUVDL. Samples of spleen were submitted to the Washington Animal Disease Diagnostic Laboratory (WADDL) for polymerase chain reaction (PCR) testing for MCF, BT, and EHD viruses. At WADDL, total DNA and RNA were extracted from the spleen using the Ambion MagMax AM1836TM-96 viral isolation kit (Thermo Fisher Scientific, Waltham, MA). BTV and EHDV assays were performed using a previously described reverse transcription quantitative (RT-q)PCR assay. 17 Real-time TaqMan PCR to detect BVDV was performed using the ABI 7500 Fast real-time PCR system (Applied Biosystems, Foster City, CA) and ABI AgPath-ID BVDV reagent kit (Applied Biosystems). Splenic DNA was subjected to OHV-2 qPCR as described previously, 6 followed by a multiplex PCR specific for the known MCF viruses causing clinical disease. 2 All assays for EHD, BT, BVD, and OvHV-2 viruses were negative. The multiplex PCR for MCF viruses was also negative for OHV-2, caprine gammaherpesvirus 2 (CpHV-2), CpHV-3, AlHV-2, and Ibex-MCFV, but yielded positive for AlHV-1. These results in association with epidemiologic, clinical, and histopathologic data supported a diagnosis of AlHV-1-induced MCF.
To further investigate the identity of the AlHV-1 detected by the multiplex PCR, 865 bp from a portion of the herpesviral DNA polymerase gene was amplified from DNA obtained from the steer spleen using AlHV-1–specific primers (forward: 5’-CCAGGGTGCCACCGTGATC-3’; reverse: 5’-GACCTCCTCGTCTCGCAGC-3’). The amplified DNA was cloned into a vector (pCR4-TOPO, Thermo Fisher Scientific) and sequenced using the M13 forward and reverse primers. The sequence obtained showed 100% homology to a portion of AlHV-1 DNA polymerase gene (GenBank AF005370.1) using BLAST analysis (http://blast.ncbi.nlm.nih.gov/Blast.cgi).
Until recently, confirmation of WA-MCF cases has been difficult because of the lack of molecular diagnostic tools, although a number of MCF cases have occurred where wildebeest were present at zoological facilities. 12 Interestingly, a report of WA-MCF at a facility in the United Kingdom documents targeting of 3 Watusi-Ankole cattle 16 despite a variety of other exotic hoofstock on the premises. Some of the gross changes described in that outbreak (conjunctivitis, cardiac hemorrhages, pulmonary edema and congestion, gastrointestinal congestion and hemorrhage) were also found in our case. However, oral lesions were not seen, in contrast to the more classic “head and eye” form of MCF seen in our case. Histopathologic findings of the U.K. outbreak included more widespread classic arteritis than seen here.
The role of the reservoir species is well recognized in both SA-MCF 7 and WA-MCF, and it is generally acknowledged that most wildebeest are infected with AlHV-1 by a few months of age.13,18 It is believed that virus shedding is mainly via oculonasal secretions of calves and by cows at the time of parturition. Wildebeest calves are the major source for viral transmission.1,18 Yet, despite housing wildebeest for over 25 y, and the birth of multiple wildebeest calves on the premises, this park had not had a diagnosis of clinical MCF prior to this case. The AlHV-1 status of the herd when it was first established is unknown. However, 6 mo prior to this Watusi WA-MCF case, serum collected from an adult male wildebeest tested for AlHV-1 by virus neutralization at the National Veterinary Services Laboratory in Ames, Iowa yielded a positive titer. This animal was 1 of 2 breeding animals added to the herd 6 y earlier and represented the last introduction to the herd. As AlHV-1 causes lifelong infection in wildebeest, at least 1 infected animal had been present in the herd since that introduction. It is noteworthy that no wildebeest calvings had occurred in the first 5 y following the arrival of this breeding pair. However, 2 calves were born in July 2015 and one of these was the result of the mating of the imported breeding pair. Therefore, AlHV-1 was likely being shed during the 3 mo leading up to clinical MCF in the Watusi steer. Efficient transmission of MCF viruses via infected secretions of a reservoir host to a clinically susceptible host is favored by close contact, and because all hoofstock could intermingle, the exposure of Watusi cattle to virus through close contact is certainly possible. Indeed, staff at the park report that Watusi are protective of the calves of other hoofstock species, defending them against zebras, which sometimes attack the young of other species. Occurrence of WA-MCF in this single animal might reflect multiple factors contributory to viral transmission or disease progression, including dose and opportunity for exposure to infective virus, the role of fomites, and stress factors or immune status of susceptible hosts. Transmission of the virus between members of non-reservoir host species is not believed to occur. No other clinical cases of WA-MCF have been diagnosed in the park during the 10 mo following the death of this animal.
Transmission of AlHV-1 to domestic cattle in pastures neighboring the park was considered unlikely, as direct contact is the usual means of spread. However, AlHV-1 transmission has been reported when animals were separated by at least 100 m, 18 and transmission of OvHV-2 from sheep to bison over significant distances has been documented. 11 As per regulations, the State veterinarian was informed of the diagnosis.
There are currently no recommended treatments or vaccines available for MCF. Establishment of AlHV-1–free wildebeest populations is extremely difficult, so control often centers on the segregation of parturient cows and their calves from other hoofstock. This facility does not currently require any replacement stock for the wildebeest; therefore, all fertile males have been eliminated and no calvings are anticipated for the next few years. In addition, the wildebeest are now segregated into a quadrant housing zebra and rhinoceroses but no ruminants. Serum will be collected from all herd members and tested for AlHV-1 titers to better define the extent of viral infection, but it is anticipated that all animals will be seropositive. Research aimed at the development of MCF vaccines is in progress, and new control methods may become available in the near future.4,8,14,15,18
Some cases of WA-MCF may be underdiagnosed as a result of a lack of widespread classic vascular histopathologic change, and it should be recognized as a differential diagnosis in potentially exposed ruminants with febrile disease. Newer detection tests allow identification of the MCF viruses involved through confirmation of the presence of specific viral nucleic acid sequences in tissues.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: H Li and CW Cunha disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: USDA-ARS CWU 2090-32000-032-00D.