
Abstract
Cats with cholestatic liver disease experience significant morbidity and mortality when they undergo invasive procedures under anesthesia. Although inadequate adrenal response might account for these outcomes, adrenal function in cats with cholestatic liver disease has not been documented, to our knowledge. The goal of our study was to describe adrenal function in these cats. Twenty-seven cats with a serum bilirubin >230 µmol/L (3 mg/dL) and serum alanine aminotransferase >2 times the upper limit of normal had pre– and 60-min post–adrenocorticotropic hormone (ACTH) cortisol analysis after administration of 5 µg/kg cosyntropin intravenously. The change in cortisol concentrations (delta cortisol) was calculated. Pre- and post-ACTH cortisol concentrations were compared to reference values. Pre-ACTH, post-ACTH, and delta cortisol values were compared between cats surviving to discharge or for 30 d postdischarge. Mean pre-ACTH cortisol levels (205 ± 113 nmol/L [7.4 ± 4.2 µg/dL]) and post-ACTH cortisol levels (440 ± 113 nmol/L [15.9 ± 4.1 g/dL]) in cholestatic cats were significantly greater than reference values in clinically normal cats. There was no association of pre- or post-ACTH cortisol with survival. Cats with a delta cortisol <179 nmol/L (6.5 µg/dL) were more likely to be non-survivors at 30 d post-discharge (p = 0.037) than cats with delta cortisol >179 nmol/L (6.5 µg/dL). Results indicate that cats with cholestasis have high basal and ACTH-stimulated cortisol values. A delta cortisol <179 nmol/L (6.5 µg/dL) defines a population of cats that have decreased 30-d survival.
Introduction
Cats with cholestatic disorders frequently have conditions such as parenchymal liver disease, extrahepatic bile duct obstruction, choleliths, and long-term anorexia that require invasive procedures such as laparotomy, hepatic biopsy, and placement of enteral nutrition tubes. This population of cats, however, does not tolerate the stress of anesthesia and/or surgery well.5,7,22 For example, perioperative morbidity and mortality in hyperbilirubinemic cats undergoing surgery for bile duct obstruction has been reported to be as high as 68%.5,23 Studies, however, have failed to demonstrate risk factors associated with this high mortality.
Activation of the hypothalamic–pituitary–adrenal (HPA) axis and increased release of cortisol is crucial to a successful response to stress. Increasing evidence in people with cirrhosis or obstructive jaundice suggests that this homeostatic mechanism is disrupted. 13 A condition known as the hepatoadrenal syndrome marked by a relative adrenal insufficiency (RAI), in which there are inadequate cortisol levels for the severity of illness, occurs in non–critically ill human patients with liver disease.1,14,15,25,41 This syndrome, which is present in 31–60% of people with cirrhosis, is associated with greater short-term mortality and increased susceptibility to sepsis and circulatory and renal complications. 1 Clinically, these patients have nonspecific symptoms such as tiredness, fatigue, and weakness.13,25 During times of stress, however, the relative HPA axis suppression leads to suboptimal adrenal reserves to meet the body’s needs and these patients become seriously ill with what has been called critical illness–related corticosteroid insufficiency (CIRCI).9,20,21 The hallmark of CIRCI is hemodynamic instability, particularly refractory hypotension.9,20,21 Because up to 70% of cholestatic cats with biliary obstruction undergoing surgery experience perioperative refractory hypotension,5,23 it is possible that a similar hepatoadrenal syndrome may occur in cats. To date, however, adrenal function in cats with cholestasis has not been characterized.
The primary goal of this pilot study was to describe adrenal function in cats with cholestatic liver disease by determining basal and post–adrenocorticotropic hormone (ACTH) stimulation cortisol levels. A secondary goal was to determine if measures of adrenal function, pre- or post-ACTH cortisol levels, or the magnitude of the change in cortisol after ACTH stimulation (delta cortisol) were correlated with survival or indicators of liver function.
Materials and methods
Cats were prospectively enrolled from cases hospitalized at the Foster Small Animal Hospital at the Cummings Medical Center at Tufts University (Grafton, Massachusetts). All owners gave informed consent, and the study was approved by the Cummings School of Veterinary Medicine at Tufts University Companion Science Review Committee. Inclusion criteria included serum bilirubin >230 µmol/L (3 mg/dL), packed cell volume (PCV) >25% (to exclude anemic cats that could have a prehepatic cause of hyperbilirubinemia), and an increase in serum alanine aminotransferase (ALT) >2 times the upper limit of normal. Exclusion criteria included the use of trilostane, corticosteroids, progesterone, anabolic steroids, or ketoconazole within 2 mo prior to presentation, or the use of etomidate within 24 h of ACTH testing.
In order to measure adrenal function, the lowest dose of ACTH capable of eliciting maximal stimulation of cortisol in healthy cats was chosen.18,28–30,32,33,35–37 Two studies have evaluated serum cortisol responses after incremental doses of cosyntropin in clinically normal cats.11,30 In these studies, ACTH stimulation testing with intravenous administration of cosyntropin at 5 µg/kg resulted in peak serum cortisol concentrations that were equivalent to those achieved with administration of 125 µg/cat. Thus, we used 5 µg/kg of cosyntropin a in our studies.
Each cat had a 2-sample (pre- and post-) ACTH stimulation test performed within 48 h of hospital admission. The post sample was submitted 60 min after intravenous administration of cosyntropin. Serum was prepared and frozen at −80°C until analysis. Samples were submitted to IDEXX Laboratory (North Grafton, Massachusetts) for serum cortisol by a validated chemiluminescent assay. The difference between the basal and post-ACTH cortisol was recorded as the delta cortisol. Each cat had a complete blood cell count and biochemistry profile submitted to the Foster Hospital, Clinical Pathology Laboratory at Tufts University within 12 h before the stimulation test.
Signalment, laboratory parameters (PCV, white blood cell count [WBC], total bilirubin, serum liver enzyme activity: alkaline phosphatase [ALP], ALT, aspartate aminotransferase [AST], gamma glutamyl transpeptidase [GGT], blood glucose, and cholesterol) were recorded for each case. At the time of the stimulation test, rectal temperature, and pulse, heart, and respiratory rates were taken; blood pressure was determined by an indirect Doppler method. Hypotension was defined as systolic blood pressure <80 mm Hg. Cats were given a diagnosis of systemic inflammatory response syndrome (SIRS) if they had 3 or more of the following: temperature >40°C or <37.7°C, heart rate >225 or <140 bpm, respiratory rate >40/min, and a WBC count >19.4 × 109/L, <5 × 109/L, or >5% bands. 10
Pre- and post-ACTH serum cortisol levels were recorded and compared to reference values. Data distributions were evaluated for normality using tests for skewness and kurtosis as well as by inspection of histogram and box plots. To meet our primary goal, means or medians were compared to reference intervals by student t-test for normally distributed data or Mann–Whitney test for nonnormally distributed data. Pre-ACTH, post-ACTH, and delta cortisol values were compared between cats that survived to discharge and for 30 d using Student t-test. Logistic binary regression was performed comparing delta cortisol with the dependent variable of either death at 30 d (0) or survival at 30 d. 6 Correlations between basal, post-ACTH, and delta cortisol and baseline physiologic status (blood pressure, heart and respiratory rate, blood glucose, PCV, WBC) and indicators of severity of hepatobiliary disease (serum bilirubin, ALT, ALP, cholesterol, glucose) were examined with Pearson correlation coefficient after log transformation, if necessary. Fisher exact test was used to compare categorical data. A p value <0.05 was considered significant. Bonferroni correction was applied for multiple comparisons.
Results
Twenty-seven client-owned hospitalized cats were prospectively enrolled. The population included 16 spayed females and 11 neutered males. The median age was 11 y (range: 3–17 y). All cats had increases in serum bilirubin and serum ALT, AST, and ALP. Serum GGT was increased in 17 of 27 cats (Table 1). Rectal temperature was increased in 3 of 27 cats and decreased in 6 of 27 cats. Heart rate was decreased in 1 cat and respiratory rate increased in 2 cats. The median systolic blood pressure at the time of ACTH stimulation was 114 mm Hg (70–158 mm Hg). This blood pressure was significantly lower than has been previously reported in normal healthy cats (131–134 mm Hg).4,19,26,27 However, only 3 of 27 cats were hypotensive (systolic blood pressure <80 mm Hg). No cats were hypertensive.
Population parameters of 27 cats with cholestasis.*
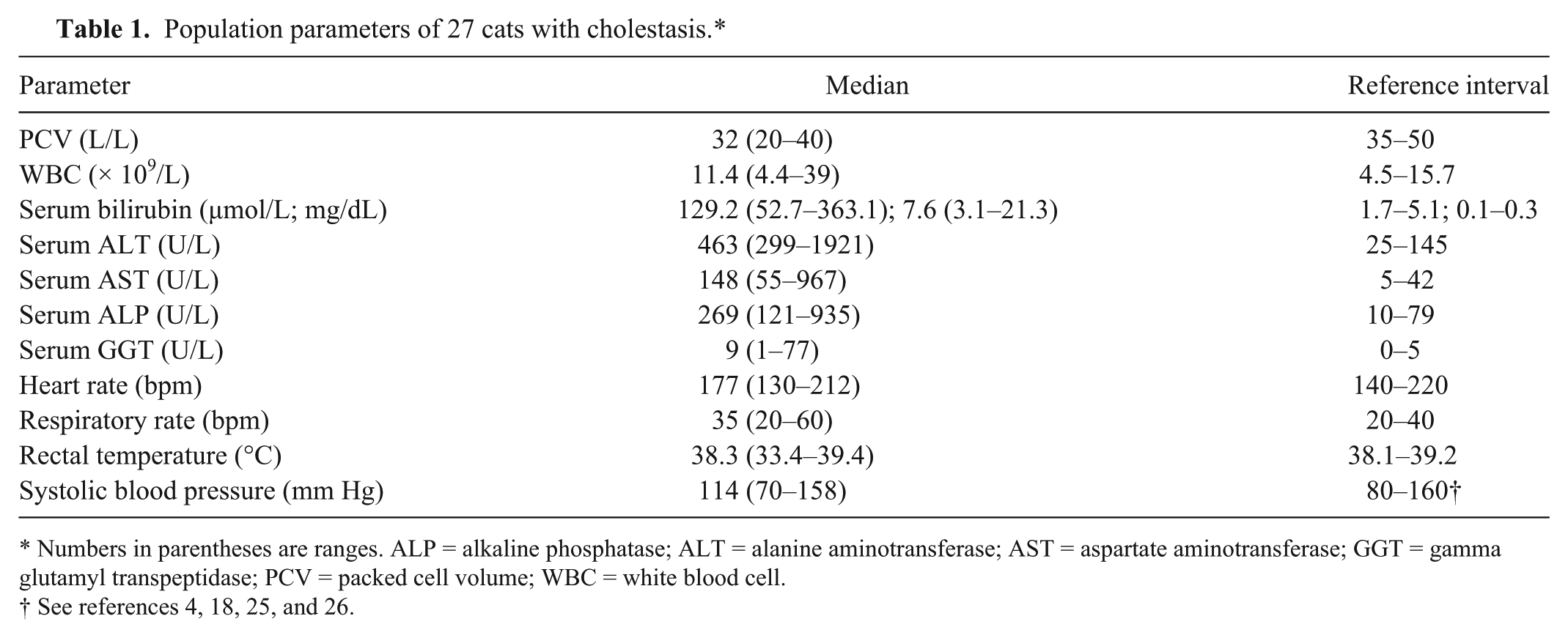
Numbers in parentheses are ranges. ALP = alkaline phosphatase; ALT = alanine aminotransferase; AST = aspartate aminotransferase; GGT = gamma glutamyl transpeptidase; PCV = packed cell volume; WBC = white blood cell.
See references 4, 18, 25, and 26.
The underlying cause of liver disease was determined in 25 of 27 cats by evaluation of cytologic preparations (n = 2) or hepatic biopsies (n = 20), or was based on evidence of drug-induced liver disease (n = 3). Diagnoses included hepatic lipidosis (10 of 25), cholangitis (8 of 25), neoplasia (7 of 25), hepatotoxicity (3 of 25), and congenital ductal plate abnormality (1 of 25). Some cats had multiple diagnoses, including 3 cats with both neoplasia and lipidosis and 1 cat with lipidosis and cholangitis. Neoplastic diagnoses included biliary adenocarcinoma (n = 3), lymphoma (n = 2), and 1 each of hepatic carcinoma and gastrointestinal epithelial carcinoma. Extrahepatic bile duct obstruction was present in 7 of 27 cats. The cause of obstruction included cancer (3 of 7), choleliths (2 of 7), and inflammatory sediment (2 of 7).
Pre- and post-ACTH stimulation serum cortisol levels in cats with cholestatic liver disease were significantly greater than reference values, with 3.4- and 1.6-fold increases, respectively (p < 0.001 for both pre- and post-ACTH stimulation cortisol). The means for pre– and post–basal cortisol were 205 ± 115 nmol/L (7.4 ± 4.2 µg/dL) and 440 ± 113 nmol/L (15.9 ± 4.1 µg/dL), respectively; reference values were 61 ± 72 nmol/L (2.2 ± 2.8 µg/dL) and 276 ±118 nmol/L (10.1 ± 4.3 µg/dL), respectively. b Tests of adrenal function were compared with survival to discharge and short-term mortality (30 d). Five of the 27 cats did not survive to discharge, and 13 of 27 died within 30 d. The mean pre-ACTH and post-ACTH stimulation and delta cortisol were not different between cats that did and did not survive to discharge or for 30 d (Tables 2, 3). Five cats had basal cortisol values that were >2 times the upper limit of normal (276 nmol/L [10 µg/dL]). Three of these 5 cats with high basal cortisol values did not survive to discharge, while only 2 of 22 cats with basal cortisol values <2 times the upper limit of normal died prior to discharge. This difference was significant (p = 0.03).
Pre– and post–adrenocorticotropic hormone (ACTH) stimulation and delta cortisol values in cats with cholestasis and survival to discharge.*
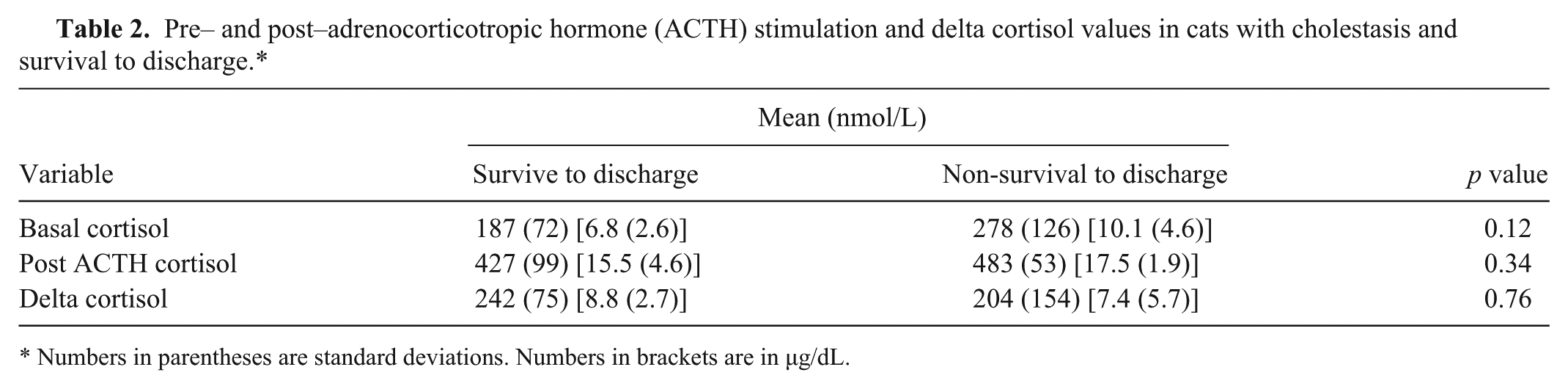
Numbers in parentheses are standard deviations. Numbers in brackets are in μg/dL.
Pre– and post–adrenocorticotropic hormone (ACTH) stimulation and delta cortisol values in cholestatic cats and 30-d survival.*
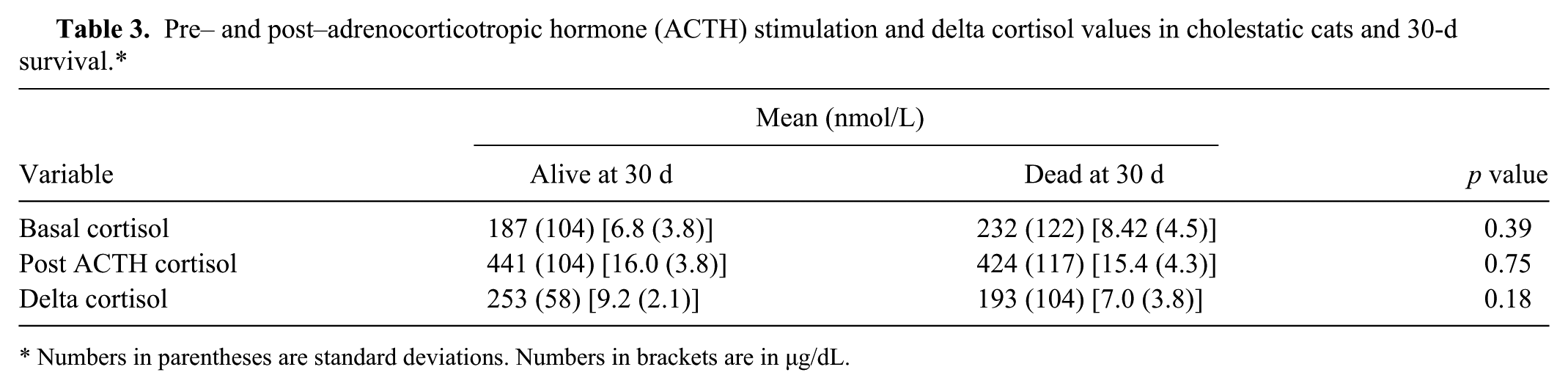
Numbers in parentheses are standard deviations. Numbers in brackets are in μg/dL.
Binary logistic regression demonstrated that delta cortisol was not associated with death before discharge; however, using this method of comparison, delta cortisol was significantly associated with survival <30 d (odds ratio = 1.21, confidence interval = 1.03–1.52, p = 0.045; Fig. 1). When these data were binned into thirds based on histogram analysis, cats with a delta cortisol <179 nmol/L (6.5 µg/dL) were less likely to survive for 30 d (relative risk = 2.8, confidence interval = 1.02–5.09, p = 0.03, Fisher exact test) than cats with a delta cortisol >179 nmol/L (6.5 µg/dL).
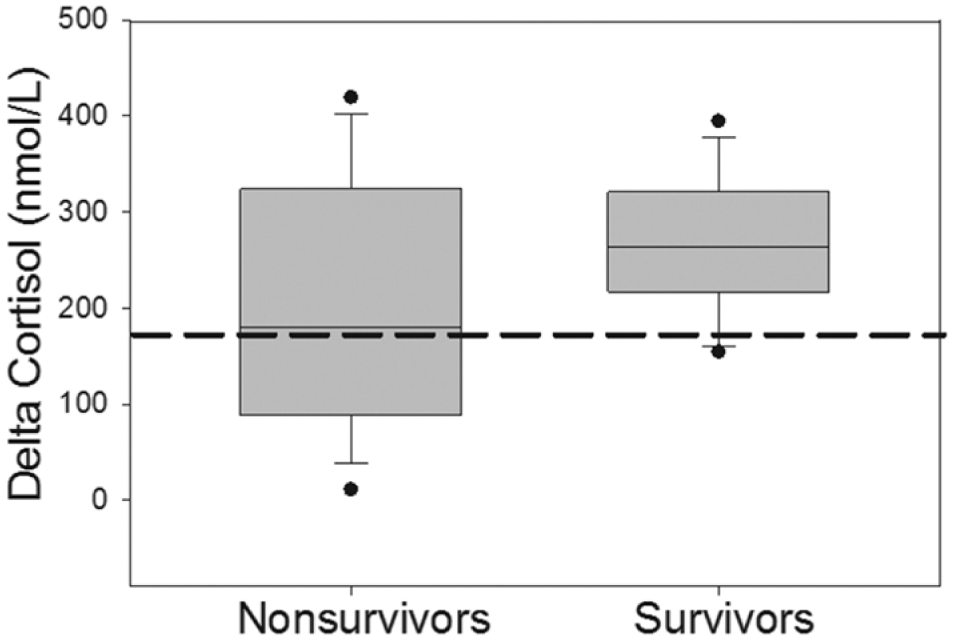
Adrenal response in cats that did and did not survive 30 d postdischarge. Delta cortisol values were calculated from pre– and post–adrenocorticotropic hormone (ACTH) stimulation tests done in cats with various cholestatic hepatobiliary diseases. The delta cortisol values are depicted in cats that did survive (n = 14) and did not survive (n = 13) for 30 d after discharge. The dotted line represents the delta cortisol value (<179 nmol/L) that predicted an increased risk of non-survival by binary logistic regression.
Survival was not associated with duration of hospitalization. The median duration for all cats was 3 d (range: 1–15 d). There was no difference between the median duration of hospitalization for the cats that did (4 d) and did not (2 d) survive to discharge (p = 0.228), or in the duration of hospitalization in cats that did (3 d, range: 1–14 d) and did not (4 d, range: 1–8 d) survive for 30 d postoperatively (p = 0.828).
Three cats had refractory hypotension; 2 of these cats died within 30 d. Mean delta cortisol in these cats (151 ± 132 nmol/L [5.5 ± 4.8 µg/dL]) was not significantly different (p = 0.18) from that seen in the normotensive cats (245 ± 99 nmol/L [8.8.7 ± 3.6 µg/dL]). The mean delta cortisol for 3 cats with SIRS (139 ± 110 nmol/L [5.03 ± 4.0 µg/dL]) was not significantly different (p = 0.09) than that seen in cats without SIRS (246 ± 99 nmol/L [8.9 ± 3.6 µg/dL]). There was no correlation between the delta cortisol and baseline serum bilirubin, cholesterol, glucose, or ALT, systolic blood pressure, or WBC (data not shown).
Discussion
High basal cortisol values in cats with cholestatic disease are a risk factor associated with poor short-term survival. Although increases in basal and ACTH-stimulated cortisol values are necessary for an animal’s response to the stress of illness, studies in chronically ill humans 34 and septic dogs 8 show that sustained HPA hyperactivity eventually becomes detrimental and is correlated with decreased survival. Whether the same is true in cats is unknown. Further studies will be needed to see if these high basal cortisol levels may contribute to the increased morbidity and mortality seen in this population of cats when they undergo stressful procedures.5,7
There is a paucity of published information on basal cortisol values in sick cats. Similar to the cats with cholestasis in our study, cats with hyperthyroidism and critically ill cats have basal cortisol levels greater than those seen in clinically normal cats.32,43 However, in studies evaluating cats with chronic cholangiohepatitis, hepatic lipidosis, or chronic interstitial cystitis, median basal cortisol values were similar to those seen in control cats.3,42 The reasons for the discrepancies between these studies is unclear but could be related to the use of different cortisol assays, variations in the severity and duration of illness in the cats tested, or a consequence of circadian variation in cortisol levels throughout the day. 35
Increased basal cortisol levels in cats with cholestatic liver disease could be the result of a variety of factors beyond those related to appropriate activation of the HPA. In humans and laboratory rodents, cholestatic liver disease alters the activity of cortisol-metabolizing enzymes.2,24,31,39 Increases in serum bile acids accompanying cholestatic disease inhibit 5-β-reductase in the liver, an enzyme that catalyzes the conversion of cortisol to inactive cortisone. 24 In addition, inflammatory cytokines, such as tumor necrosis factor–α and interleukin-1–β, which are elevated in cholestasis, increase the activity of 11-β-hydroxysteroid dehydrogenase (11β-HSD) type 1 in the liver (increasing the conversion of inactive cortisone to active cortisol) and inhibit 11β-HSD type 2 in the kidney (preventing the metabolism of cortisol to cortisone).17,24,38 Inflammatory cytokines can also increase corticotropin-releasing hormone (CRH) and ACTH release. 38 Further investigation into the effect of cholestasis on the activity of CRH, ACTH, and cortisol-metabolizing enzymes in cats is necessary.
In our study, cats with a delta cortisol <179 nmol/L (6.5 µg/dL) had a 30-d mortality (7 of 9 cats) that was significantly higher than the mortality in cats with delta cortisol >179 nmol/L (6.5 μg/dL; 5 of 18 cats). This suggests that a relative lack of adrenal reserve could play a role in mortality in cats with cholestasis and warrants further consideration. Mounting evidence in people with stable liver disease suggests that they may have some degree of subclinical adrenal insufficiency that places them at increased risk for CIRCI when undergoing stressful events.13,25 There is an association of low delta cortisol values with hypotension and mortality in people and evidence for its association with morbidity in dogs.6,9,20,22 In the scant literature available in cats, in a single case report, a cat with polytrauma, hyperbilirubinemia, and refractory hypotension had a delta cortisol of 88 nmol/L (3.2 µg/dL) and showed marked clinical improvement after administration of physiologic doses of dexamethasone 12 ; this case suggests that CIRCI may exist in cats.
It will be important to identify if cats with cholestasis and refractory hypotension have inadequate adrenal reserves, because this population may benefit from corticosteroid supplementation.9,12,20 Studies on the effect of corticosteroid administration in people with cirrhosis and RAI have yielded variable results. Many confirm hemodynamic stabilization after administration of corticosteroids, however, some fail to show a consistent effect on survival.13,15,25,40 In a single study in dogs undergoing surgery for congenital portosystemic shunts, 6 of 16 had suboptimal changes in cortisol after ACTH stimulation testing, and 2 of these dogs with refractory hypoglycemia and prolonged anesthetic recovery times responded to intravenous corticosteroid therapy. 16 A study directed at evaluation of a large number of cats with cholestasis with clinical signs of RAI will be necessary to determine the role of this syndrome in the morbidity that cats with cholestasis experience during invasive procedures requiring anesthesia. Ideally, this would entail serial assessment of ACTH response tests in cats undergoing stressful procedures in order to document if cats with cholestatic hepatobiliary disease show a gradation of response from initial hypercortisolemia to eventual habituation of the HPA and insufficient adrenal response. Only then can recommendation on the therapeutic administration of corticosteroids in these cats be evaluated.
Our study had several limitations. Designed as a pilot study, the small sample size limited the power of the study to examine casual relationships. Although all cats in the study were cholestatic with hyperbilirubinemia and high serum liver enzyme activity, it was a heterogeneous population of cats in terms of the cause of each cat’s hepatobiliary disease and how seriously ill the cats were. We also did not have a group of sick control cats that underwent ACTH stimulation testing. Indeed, there is a paucity of information available on pre- and post-ACTH cortisol values in sick cats without cholestatic disease.3,32,42,43 These values will need to be defined to determine if cats with cholestasis are unique in having such high pre-and post-ACTH cortisol levels. The HPA axis could have been better characterized by determination of endogenous levels of ACTH levels and CRH and the performance of serial ACTH response tests, especially in cats undergoing invasive procedures. In humans, the determination of free cortisol rather than total cortisol is advocated in patients with hepatobiliary disease.13,20 Because cortisol is highly protein bound, changes in the concentration of serum albumin and cortisol-binding proteins that accompany hepatic disease can lead to overestimation of the diagnosis of RAI. Measurement of free cortisol, however, is cumbersome and expensive and has not been validated in the cat. In our study, none of the cats had hypoalbuminemia and thus this may not be a consideration. Although all cats in this study were examined by abdominal ultrasound, future studies should be more systematic in determining adrenal size and whether adrenal abnormalities exist.
Footnotes
Authors’ contributions
FI Buckley contributed to acquisition, analysis, and interpretation of data, and critically revised the manuscript. O Mahony contributed to analysis and interpretation of data, and critically revised the manuscript. CRL Webster contributed to acquisition, analysis, and interpretation of data, and drafted the manuscript. All authors contributed to conception and design of the study; gave final approval; and agreed to be accountable for all aspects of the work in ensuring that questions relating to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
a.
Cortosyn, Amphastar Pharmaceuticals, Canton, MA.
b.
Reference ranges for IDEXX Laboratories, Westbrook, ME.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Companion Animal Health Fund in the Department of Clinical Science at the Cummings School of Veterinary Medicine at Tufts University.