
Abstract
Inflammatory bowel disease (IBD) is a common disorder of ferrets (Mustela putorius furo) that may progress to lymphoma. Although routine histology is used to distinguish between these diseases, misclassifications may occur. Immunohistochemistry (IHC) is commonly used to distinguish between IBD and lymphoma in small animals. The objective of our study was to determine the agreement in the diagnosis reached solely using hematoxylin and eosin (HE)-stained, full-thickness sections versus using a combination of HE and IHC. Enteric sections from 44 ferrets previously diagnosed with IBD or intestinal lymphoma and 3 control ferrets were analyzed by pathologists with expertise in ferrets. A pathologist blinded to the original diagnosis assessed the same HE-stained sections. Analysis was then repeated using HE sections in parallel with sections stained using antibodies against CD3 and CD79a. No significant difference was found between the original HE diagnosis and the HE diagnosis reached by the blinded pathologist (p = 0.91) or between the blinded pathologist’s HE versus HE with IHC diagnosis (p = 0.16). In the 2 cases where disagreement was present, IHC was pivotal in reaching a final diagnosis. There was no significant age (p = 0.29) difference between diagnoses; however, significantly more male ferrets were affected with IBD than females (p = 0.004). Immunophenotype of the lymphoma was not correlated with predilection for location in the intestinal wall (p = 0.44). Results suggest that although IHC is not necessary to distinguish IBD from intestinal lymphoma in ferrets, it can be useful a definitive diagnosis in cases of severe IBD.
Introduction
Inflammatory bowel disease (IBD) is a common, chronic disorder of the gastrointestinal (GI) tract in ferrets (Mustela putorius furo) older than 1 year. 6 Histologically, IBD is characterized by shrinkage and blunting of the intestinal villi and by an inflammatory infiltrate of the mucosa. The inflammatory cells present in IBD are predominantly lymphocytes and plasma cells, but less commonly, an eosinophilic component is present. 6 Clinically, IBD is a subtle disease that may not be noticed by the trained eye of the clinician or owner until it is severe. Although the exact etiology of IBD is unknown, many hypotheses exist, including genetic background, hypersensitivity reaction, or an atypical immune response. 22 There is speculation that severe GI inflammation could be caused by commercial ferret diets, as seen in small animals with cases of diet-responsive, chronic enteropathy. 17 Because ferrets are strict carnivores, they require a diet of high fat and protein, with low carbohydrate and fiber content. Many commercial pelleted ferret diets contain greater amounts of carbohydrates and fiber, 3 which, with chronic exposure, could lead to irritation and/or inflammatory effects on the GI mucosa.
The GI tract of domestic animals is rich in lymphoid tissue. 36 Overstimulation or lack of regulation of intestinal lymphocytes may lead to 2 of the most common diseases seen in the intestinal tract of ferrets: IBD and lymphoma. Multiple, full-thickness GI biopsies are used antemortem to distinguish between these 2 lymphoproliferative diseases and to guide optimal therapeutic management. The treatment for IBD generally consists of suppression of the inflammatory response with azathioprine or corticosteroids, 6 whereas chemotherapy and radiation are generally used for the treatment of lymphoma. 21 Misdiagnosis could lead to unnecessary and potentially life-threatening, drug side effects (such as immune suppression or hematopoietic destruction) and disease progression.
In 2008, the World Small Animal Veterinary Association (WSAVA) published a histologic grading system for gastrointestinal inflammation in the dog and cat. 9 To date, there is no grading system utilized when analyzing ferret intestinal samples to distinguish between severe IBD and lymphoma, leading to possible disparity between pathologists. Because of the lack of clear standards or classification of the histology, it is difficult to clearly separate the stages of IBD from each other, and misclassification between severe IBD and lymphoma may occur. The current theory is that chronic, prolonged exposure to GI irritants, such as an abnormally large amount of carbohydrates, could induce a spectrum of disease severity ranging from mild, moderate, to severe IBD, eventually leading to lymphoma.5,6 A similar correlation has been established in ferrets between chronic Helicobacter mustelae–associated gastritis and gastric lymphoma. 12
Lymphoma is the most common malignant neoplasm in the ferret.13,21,38 In order to classify the specific type of GI lymphoma in ferrets, as in other species, further immunophenotyping diagnostics, such as immunohistochemistry (IHC), are often performed. Immunophenotyping of lymphoma in ferrets shows a predominance of T-cell lymphomas in the GI tract.1,18,31 Because of the lack of clonality assays in the ferret, IHC is the current “gold standard” for making a definitive diagnosis when a histologic diagnosis of neoplasia is difficult to make based solely on hematoxylin and eosin (HE)-stained sections, because IHC can distinguish between reactive and heterogeneous, or neoplastic and monomorphic, lymphoid populations. Despite the importance of IHC when examining intestinal sections in ferrets, no studies, to the authors’ knowledge, have characterized the immunophenotype of severe IBD or determined whether IHC is necessary in distinguishing IBD from lymphoma.
It is commonly believed that T-cell lymphomas of the GI tract tend to exhibit epitheliotropism, and neoplastic cells are often located in the lamina propria, whereas B-cell lymphomas arise from the germinal center of Peyer patches, 20 which in the ferret span the mucosa and submucosa (Fig. 1).
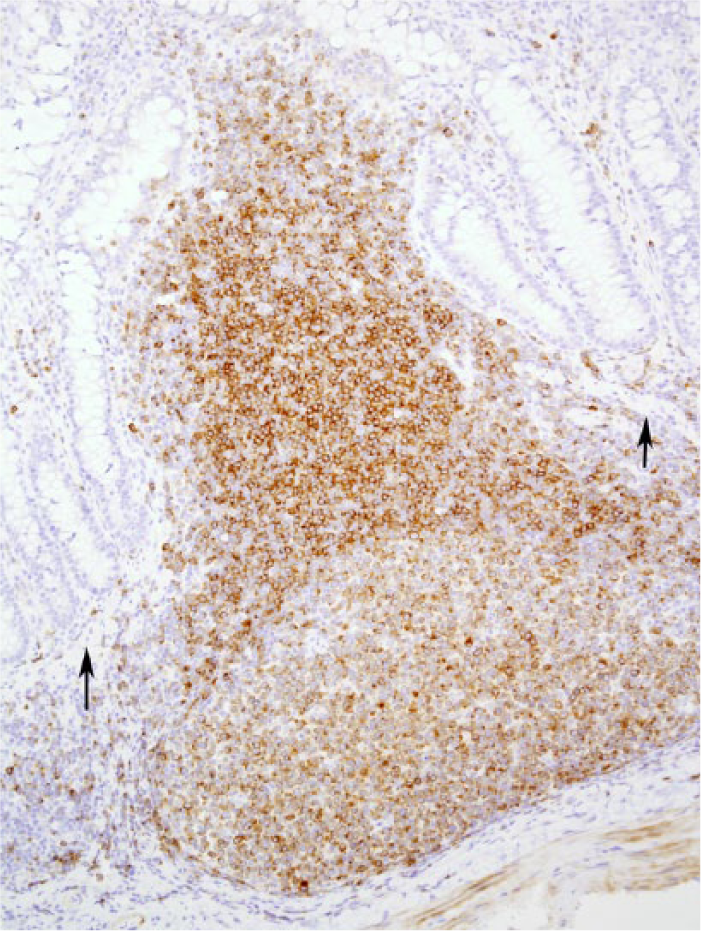
Peyer patch in the small intestine of the control ferret (Mustela putorius furo). CD79a-positive cells span the lamina propria and submucosa, breaching the muscularis mucosa (arrows). Immunohistochemistry for CD79a with hematoxylin counterstain.
The purpose of this study was to investigate the diagnostic accuracy of tissue analysis using HE staining alone or in combination with IHC to reach a final diagnosis of IBD or intestinal lymphoma in the ferret. We hypothesized that: 1) there is interpathologist variation in diagnoses using the same criteria; 2) there is a difference in diagnoses between intestinal samples using HE alone or those in conjunction with IHC; and 3) HE staining alone significantly underdiagnoses lymphoma because lymphocyte infiltrates are more easily identified in IHC-labeled sections compared to HE-stained sections alone. 36
Usually, IBD is diagnosed in adult animals; the mean age for IBD for both dogs and cats was found to be between 6 and 7 years. 24 Neoplasia is most commonly diagnosed in geriatric patients; for feline alimentary lymphoma, the range is between 10 and 12 years old, 2 and the mean age for canine lymphoma varies between 6 and 8 years old. 34 Age was determined to be a risk factor for neoplasia in nondomestic ferrets. 26 Similarly, older ferrets seem to be more predisposed to neoplasia. 27 For these reasons, we also hypothesized that IBD would be more prevalent in middle-aged animals, whereas lymphoma would be more common in older animals, with no difference in the sex of animals with regard to either diagnosis.
Although IBD tends to affect the more mucosal layers of the intestine (i.e., lamina propria and submucosa), regardless of the layer of origin, lymphoma would ultimately infiltrate most layers of the intestine. 14 For this reason, we expected that the percentage and distribution of T and B lymphocytes in the various intestinal layers would differ in IBD, and in T- versus B-cell lymphoma cases. Furthermore, we hypothesized that the location of the lymphocytes within the intestinal wall would be a good predictor for neoplasia and immunophenotype, because typically, T lymphocytes are mainly in the mucosa, whereas B lymphocytes are equally present in the mucosa and the submucosa.25,33
Materials and methods
Study population
Intestinal sections from ferrets that were diagnosed as having IBD or lymphoma by a veterinary pathologist with expertise in ferret pathology were included in this study. Criteria for the diagnosis of intestinal IBD or lymphoma by HE slide examination was based on a previous study. 14 Briefly, IBD was diagnosed when varying degrees of mucosal and submucosal infiltration by inflammatory cells (mainly small lymphocytes and plasma cells) were observed. Lymphoma was diagnosed when there was mucosal infiltration and expansion, and when there was infiltration into deeper intestinal wall layers by lymphocytes. A heterogeneous population of lymphocytes, with mild to moderate numbers of plasma cells and eosinophils, was considered most consistent with inflammation, whereas a more monomorphic population of lymphocytes, with only rare other inflammatory cells, was considered most consistent with neoplasia. Additionally, a higher lymphocyte mitotic index, intraepithelial nests, and the presence of atypical lymphocytes in the blood vessels were also considered supportive of a diagnosis of lymphoma.
Only samples in adequate condition were included; if the histologic section was too small, incomplete, autolyzed, or contained large artifacts, it was excluded from this study. Forty-seven ferrets were ultimately included in this retrospective study (44 clinical cases and 3 controls). Forty-one of the specimens had been submitted to the Zoo/Exotic Pathology Service (Sacramento, California), 3 had been submitted to the Massachusetts Institute of Technology (Cambridge, Massachusetts), and 3 intestinal sections from healthy ferrets were used as controls. Specimens included full-thickness biopsy samples from the intestine. Often multiple intestinal sections were available from the same ferret; however, because small intestine was more consistently available, we elected to limit our study to this part of the intestinal tract. Based on histology only, all ferrets had been diagnosed as either IBD (27 cases) or intestinal lymphoma (17 cases) at the institutions of origin by board-certified, veterinary pathologists with expertise in ferret pathology. Among the 27 cases of IBD, 8 cases were considered severe, 5 were moderate to severe, 10 were moderate, and 4 were mild. In 4 ferrets, intestinal lymphoma and IBD were diagnosed concurrently in different sections of intestine. For those cases, only neoplastic sections were analyzed. Clinical history was available in the majority of the clinical cases evaluated and included a variety of clinical signs ranging from weight loss, anorexia, and diarrhea, to sudden death. For the majority of cases, the age and sex of the animal were also available. Age and sex distribution for included cases are shown in Table 1. Ferrets less than 1 year of age were excluded from the study, because IBD is usually diagnosed in ferrets older than 1 year. 6
Age and sex distribution of the population of ferrets included in this study. Total cases are based on final diagnosis after inclusion of immunohistochemistry results. All ferrets less than 1 year of age were excluded from analysis.*
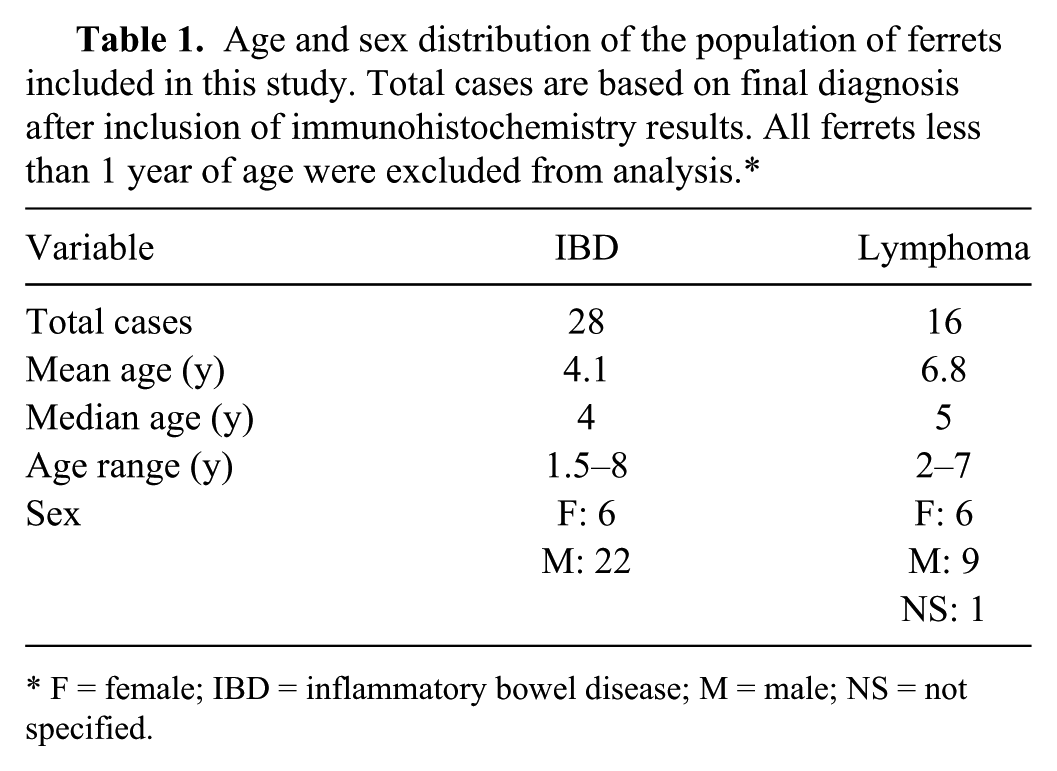
F = female; IBD = inflammatory bowel disease; M = male; NS = not specified.
Histology
Full-thickness biopsies from the small intestine were available for all ferrets included in the study. For all cases, formalin-fixed, paraffin-embedded samples were available for HE and IHC. Tissue samples embedded in paraffin were routinely processed and sectioned at ~5 μm thickness. All tissue sections were stained with HE.
Immunohistochemistry
Serial sections were deparaffinized and rehydrated for routine IHC to detect cytoplasmic expression of cluster of differentiation (CD)3 (1:800 dilution; polyclonal rabbit anti-human CD3 antibody [A0452] a ) for T cells, and cytoplasmic expression of CD79a (1:50 dilution; monoclonal mouse anti-human CD79αcy clone HM57 [M7051] a ) for B cells. Antigen retrieval methods consisted of heat-induced epitope retrieval (HIER) using citrate buffer at a pH of 6.0. b Endogenous peroxidase was blocked using 3% hydrogen peroxide. c Protein blocking b was performed. Positive immunohistochemistry controls consisted of formalin-fixed, paraffin-embedded canine tonsil and lymph node, as well as lymphoid tissues within each ferret slide, which always showed some positive cells. As a negative control, the primary antibody was eliminated and substituted with purified rabbit immunoglobulin d or purified mouse immunoglobulin d for CD3 and CD79a, respectively. Slides were reviewed using light microscopy.
Case evaluation
Histologic sections of small intestine stained with HE were evaluated by a board-certified veterinary pathologist blinded to the original diagnosis made by the veterinary pathologists with expertise in ferret pathology, and based on the appearance of the most severely affected section, a diagnosis of IBD or lymphoma was made. The specimens were categorized according to Evans et al., as described under Study Population. 14 The HE-stained sections were analyzed a second time, in parallel with the serial IHC preparations for CD3 and CD79a, and without knowledge of the previous results. These markers were chosen based on previous studies using IHC in intestinal lymphoma in ferrets.1,18,31 A diagnosis of IBD or lymphoma was made again based on the combination of HE and IHC. The diagnosis based solely on HE reached at the original institution and the new HE results were compared; furthermore, the new diagnosis reached by HE only and those made after immunophenotyping by the same blinded pathologist were also compared. All of the lymphoma cases were classified using the Revised European-American Lymphoma (REAL) classification scheme for lymphoma in domestic animals published by the World Health Organization (WHO) 35 and as described previously. 32 The classification was based on both HE and IHC sections.
For each case, the age and sex of the animal were compared with the final diagnosis (obtained with the aid of IHC) to see if a correlation was present. Subjective percentages of B and T lymphocytes, identified by IHC, that were present in the epithelium, lamina propria, submucosa, and tunica muscularis were also recorded. Percentages based on cell counts per field could not be performed because of the tremendous variation between fields; therefore, relative distribution of T and B lymphocytes was assessed in each intestinal layer and scored by approximate percentages (0 = none present, 1 = 1–25%, 2 = 26–50%, 3 = 51–75%, 4 = 76–100%) of the infiltrating cells. The main location of lymphomas in the intestinal wall was also recorded. If the infiltrate extended throughout all layers, the case was labeled “transmural.”
Statistical analysis
Statistical analyses were performed using the computing environment R, version 3.0 (http://CRAN.R-project.org/doc/FAQ/R-FAQ.html). An unweighted Cohen kappa test was used to assess the agreement between the diagnosis obtained using HE alone versus the diagnosis achieved using a combination of HE and IHC, as well as agreement between diagnosticians. The percentage of agreement between diagnoses (IBD, lymphoma) using the 2 methods (IHC, HE) was also calculated. A Wilcoxon rank sum test (Mann–Whitney test) was used to evaluate differences in ferret age and diagnosis (IBD vs. lymphoma). A Fisher exact chi-square test was used to evaluate associations between ferret sex and diagnosis (IBD vs. lymphoma), whereas an Exact binomial test was used to examine the sex ratio in ferrets that were diagnosed with IBD and lymphoma, respectively. A Wilcoxon rank sum test was used to evaluate differences in the ranked percentage of T or B cells among lymphocytes present in different layers of the intestine for both IBD and lymphoma. For the lymphoma cases, a Fisher exact test was used to determine if an association was present between neoplastic cell location and the immunophenotype determined by IHC. For all statistical tests, the p value considered statistically significant was p < 0.05.
Results
Sixteen cases were ultimately diagnosed with lymphoma. Based on IHC, 9 were T-cell lymphomas (56.25%), and 5 were B-cell lymphomas (31.25%), with one of the cases ultimately classified as a diffuse large B cell of immunoblastic nuclear type, having a large T-cell component. Two cases (12.5%) did not stain with either antibody and were diagnosed as a null cell lymphoma. The WHO/REAL classifications for each of the lymphomas are shown in Table 2.
Classification of the lymphoma cases based on the World Health Organization (WHO)/Revised European-American Lymphoma classification scheme.*
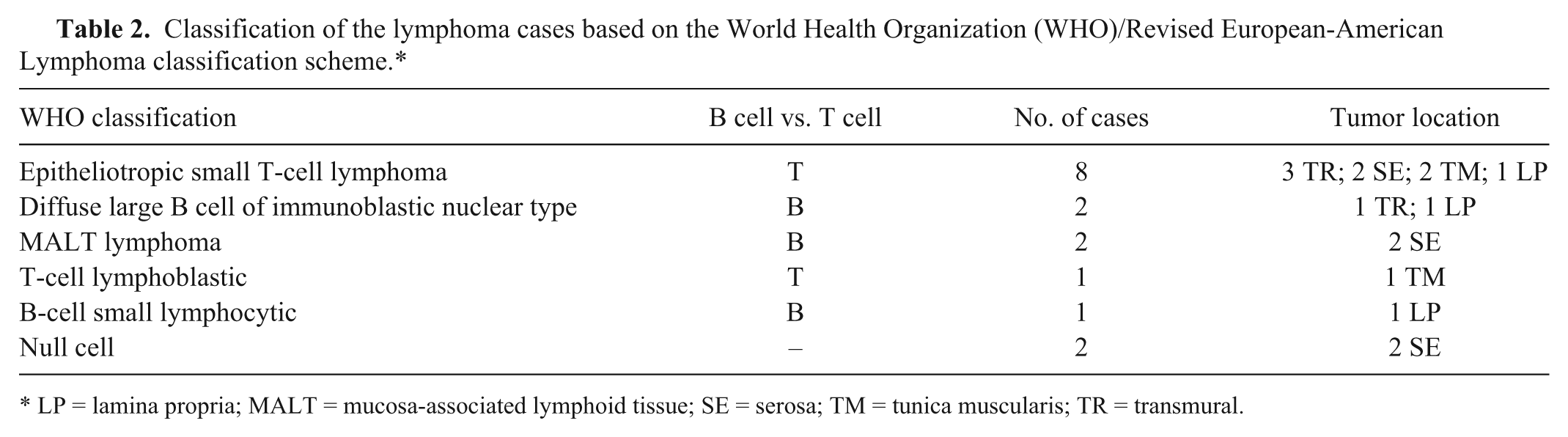
LP = lamina propria; MALT = mucosa-associated lymphoid tissue; SE = serosa; TM = tunica muscularis; TR = transmural.
Original diagnoses by pathologists with experience in ferret pathology were compared to the blinded pathologist in our study in order to assess interpathologist variation when using the same criteria for diagnosis. 14 There was no significant difference between pathologist diagnoses (p = 0.91). No significant difference was present between the diagnosis made by using only HE and the diagnosis made with the aid of IHC (Cohen kappa, z = 1.14, p = 0.16). In only 1 case was the diagnosis changed (from lymphoma to IBD); a transmural infiltrate of relatively monomorphic lymphocytes by HE was identified by IHC to be a pleomorphic population of predominantly CD3+ lymphocytes that did not differ in relative prevalence from the adjacent, inflamed mucosa (Fig. 2). The diagnosis agreement between HE and the combination of HE and IHC was 93.7% for the cases ultimately diagnosed as lymphoma, indicating a 6.3% (1/16) disagreement between cases originally diagnosed as IBD that were reclassified as lymphoma after IHC testing, and 96.4% for the cases ultimately diagnosed as IBD, indicating a 3.6% (1/28) disagreement between cases originally diagnosed as lymphoma that were reclassified as IBD after IHC (Table 3). In one of these cases, IHC supported the diagnosis made by the ferret expert, whereas in the other, IHC supported the diagnosis made by the blinded pathologist. In both of those cases, the inflammation was considered as severe by the pathologist with expertise in ferrets.
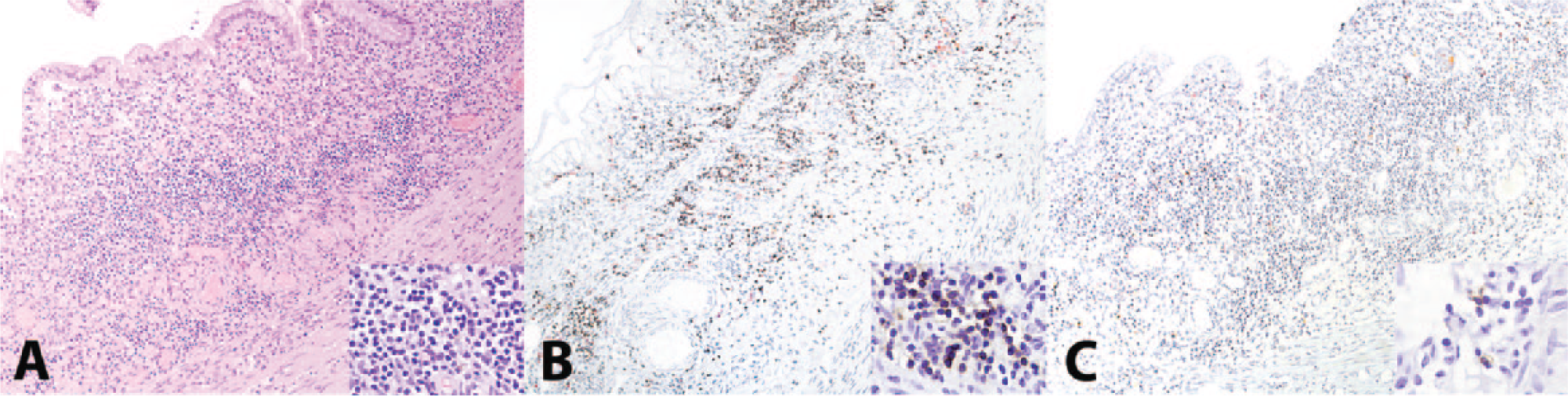
Severe inflammatory bowel disease in the small intestine of a ferret (Mustela putorius furo). In this case, immunohistochemistry (IHC) was useful in correcting a previous diagnosis of intestinal lymphoma made as a result of the diffuse nature of a monomorphic, small lymphocyte population that expanded the mucosa and extended to the serosa. Hematoxylin and eosin (
Agreement between original diagnosis and study diagnosis based on hematoxylin and eosin (HE) alone and in combination with immunohistochemistry (IHC). There were 2 cases in which disagreement was present.*
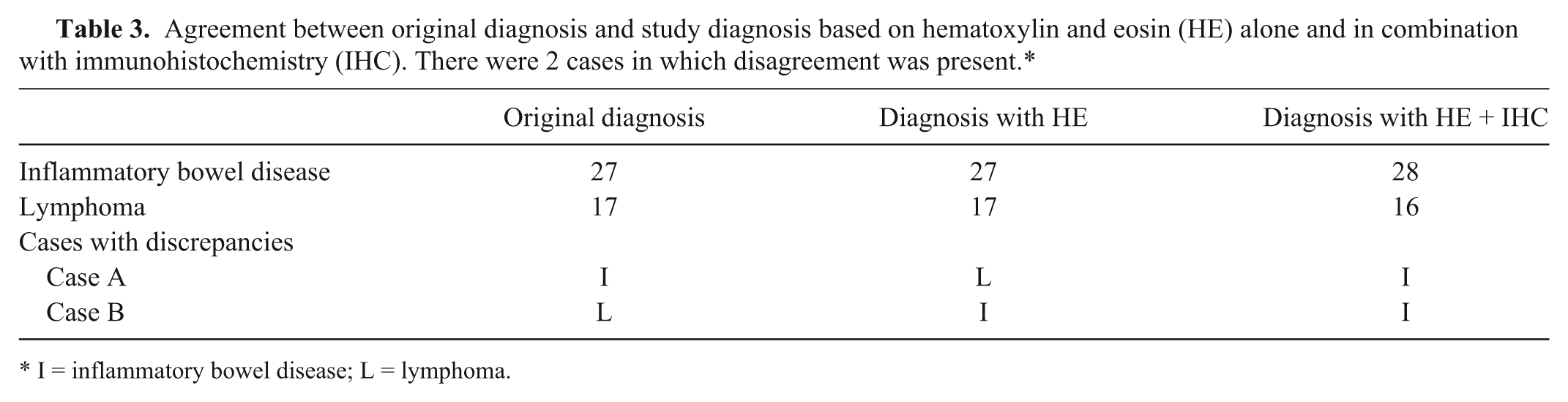
I = inflammatory bowel disease; L = lymphoma.
There was no significant age (Wilcoxon rank sum test, W = 133.5, p = 0.29) or sex (Fisher exact test, p = 0.26) association between cases ultimately diagnosed as IBD or lymphoma by IHC. Although there were more male ferrets diagnosed with lymphoma, the larger confidence interval associated with our small sample size may have masked our ability to see a statistically significant difference. However, there was a significant difference in the male-to-female ratio with regards to the diagnosis of IBD (exact binomial test, p = 0.004), and males predominated.
As depth of lymphocyte infiltration is a criterion for the diagnosis of intestinal lymphoma, 14 the relative percentage of CD3+ T cells and CD79a+ B cells was examined for each layer of the intestinal wall in all lymphoma cases. The mean percentage of CD3+ T cells as assessed by score was not different between B- and T-cell lymphomas in any layer of the intestinal wall except for the lamina propria (p = 0.05, see Table 4, Wilcoxon rank sum test), indicating that reactive T lymphocytes were present in all cases of B-cell lymphoma (Fig. 3). However, the mean percentage of CD79a+ B cells was significantly different in the submucosa and tunica muscularis between B- and T-cell lymphomas, with B cell percentages greater in the B-cell lymphomas (see Table 4 for p values and Fig. 4), indicating that T-cell lymphomas were not typically accompanied by inflammatory B cells. No significant differences were identified with either lymphocyte type with regards to location in the intestinal wall in IBD cases, with the exception of the mucosal epithelium, which only contained T lymphocytes.
Mean score (0 = none present, 1 = 1–25%, 2 = 26–50%, 3 = 51–75%, 4 = 76–100%) of CD3+ T cells and CD79a+ B cells in ferret lymphomas (n = 16) and inflammatory bowel disease (n = 28) cases.*
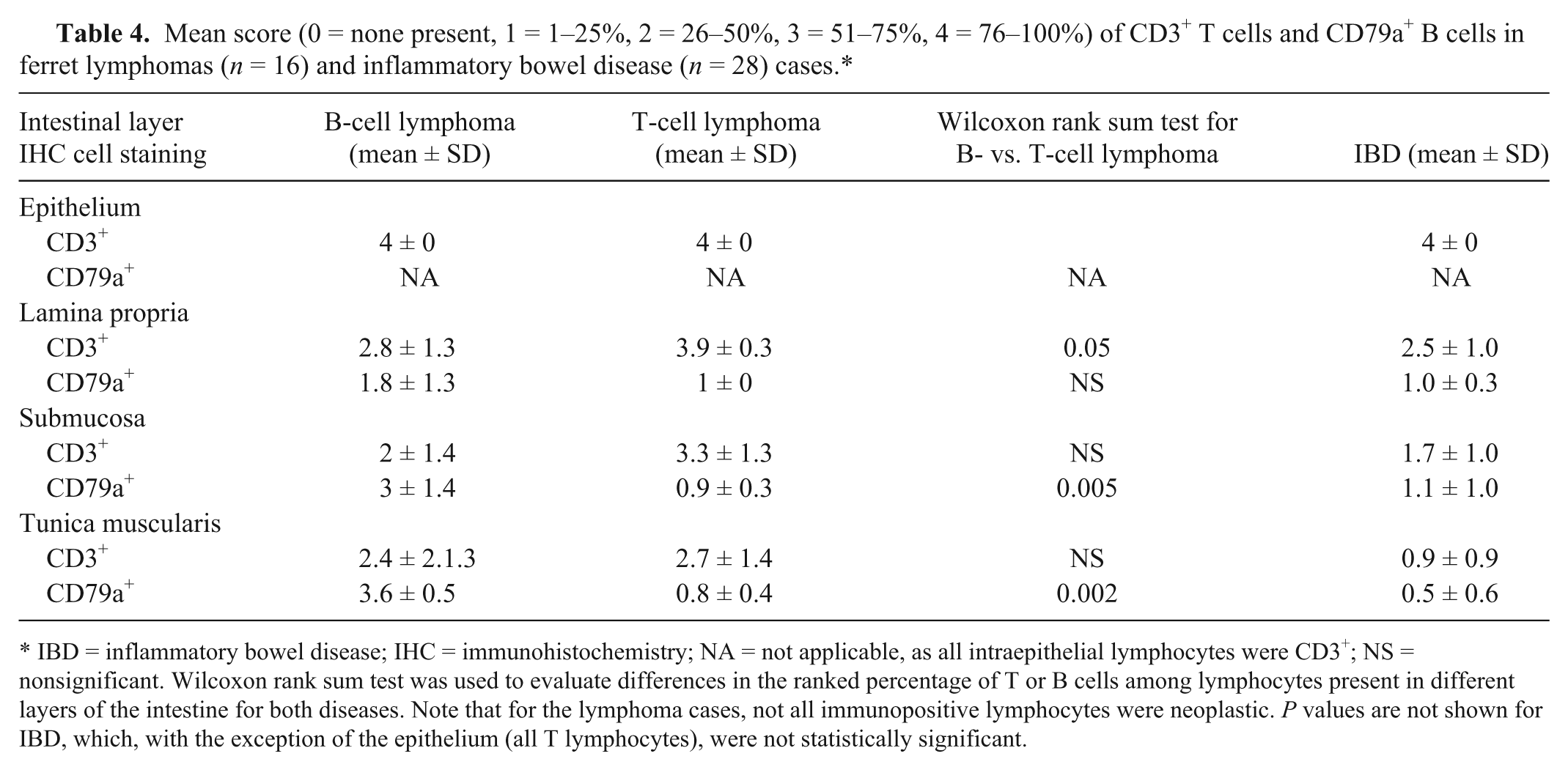
IBD = inflammatory bowel disease; IHC = immunohistochemistry; NA = not applicable, as all intraepithelial lymphocytes were CD3+; NS = nonsignificant. Wilcoxon rank sum test was used to evaluate differences in the ranked percentage of T or B cells among lymphocytes present in different layers of the intestine for both diseases. Note that for the lymphoma cases, not all immunopositive lymphocytes were neoplastic. P values are not shown for IBD, which, with the exception of the epithelium (all T lymphocytes), were not statistically significant.
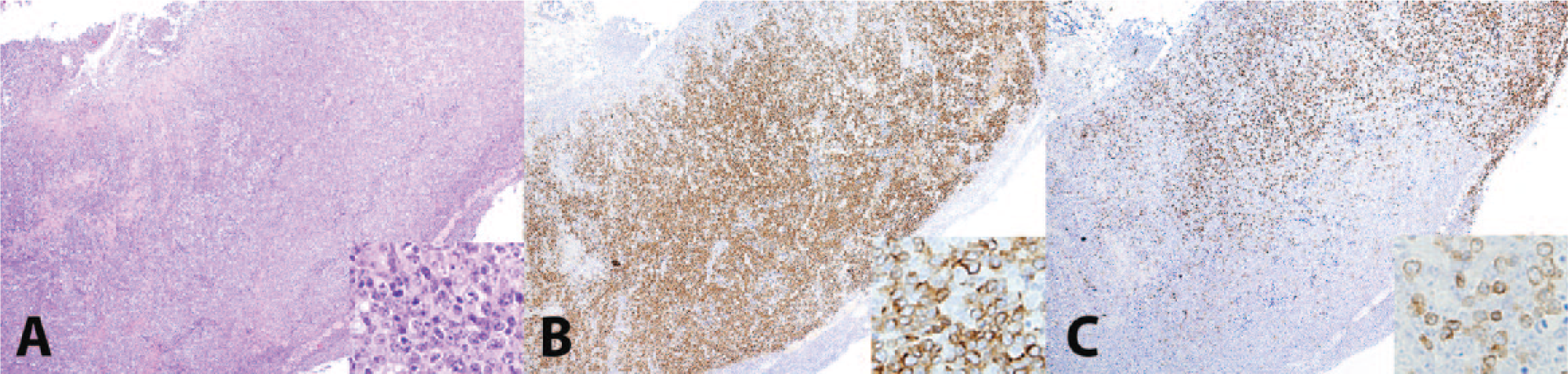
Intestinal B-cell lymphoma in the small intestine of a ferret (Mustela putorius furo). In intestinal B-cell lymphomas (
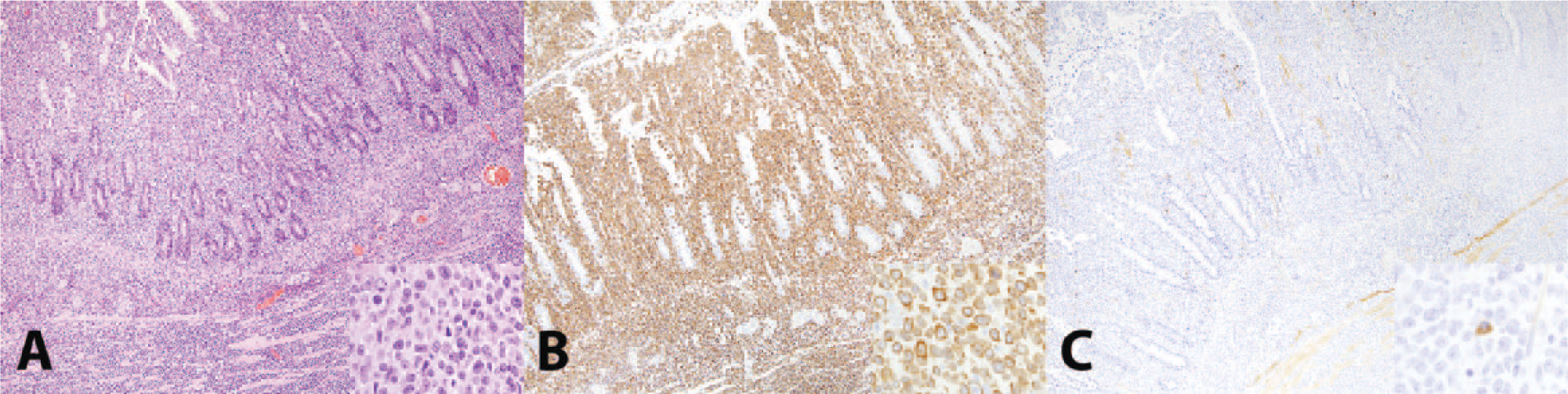
Intestinal T-cell lymphoma in the small intestine of a ferret (Mustela putorius furo). In intestinal T-cell lymphomas (
In the lymphoma cases, the location of the main mass was detected (Table 2). Among the cases diagnosed as T-cell lymphoma, in 1 case, the neoplasm was mainly localized in the lamina propria, 2 were localized in the serosa, 3 in the tunica muscularis, and in 3 cases the neoplasia was transmural. Among the cases diagnosed as B-cell lymphoma, in 2 cases the mass was mainly in the lamina propria, in 2 cases in the serosa, and in 1 case the neoplasia was transmural. In both cases of null cell lymphoma, the tumor was mainly localized in the serosa. There was no significant correlation (Fisher exact test, p = 0.44) between T- and B-cell lymphomas with regard to a predilection for location in the intestinal wall.
Discussion
No statistical difference was present between the diagnosis obtained via HE alone and the diagnosis obtained with the addition of IHC. Although not statistically significant, there was a 6.3% (1/16) disagreement between cases originally diagnosed as IBD that were reclassified as lymphoma after IHC testing, and conversely, a lower percentage of cases (3.6%; 1/28) that were originally diagnosed as lymphoma that were reclassified as IBD after IHC. These results are consistent with another study in cats in which lesions previously diagnosed as lymphomas were reclassified as severe inflammation based on IHC findings. 37 It is important to note that in both of the cases where disagreements between diagnoses were present, the inflammation was considered severe by the pathologist with expertise in ferrets. This is not surprising because IHC is usually only used in severe cases of IBD, where confusion on the definitive diagnosis might exist. One limitation of the present study was the small sample size, and a statistical significance may be seen in a larger study. These results indicate that although IHC is not routinely required to make a diagnosis of IBD or lymphoma from full-thickness intestinal biopsies in ferrets, its use may be crucial for a small percentage of animals for which a definitive diagnosis is difficult to reach based on HE staining only, particularly in cases with small, monomorphic lymphocytic infiltrates. For this reason, the use of IHC should be considered in cases in which a HE diagnosis is uncertain; otherwise, the lesion may be misdiagnosed.
Our findings are consistent with a 2011 study in cats that recommended a diagnostic algorithm that first uses histologic assessment, followed by immunophenotyping, and then PCR to determine clonality of the lymphocytes to more accurately differentiate between intestinal lymphoma and IBD. 25 Follow-up IHC after histologic diagnosis was recommended in ferrets in a 2012 study. 28 Clonality studies have not yet been performed or validated on lymphoma in ferrets.
The predominance of T-cell lymphomas, particularly epitheliotropic small T-cell lymphoma, in the ferrets in our study is consistent with the results of other studies.8,18,19,31 Gastrointestinal lymphoma in dogs is commonly of T cell origin. 29 Although findings are variable in cats, when analyzing lymphomas affecting only the intestine, T cells are also the predominant cell type.7,25 Unfortunately, there were not enough cases in our study to identify whether different WHO classifications of lymphomas were associated with a predilection for a particular part of the intestinal wall.
In our study, age was not a determining factor for lymphoma. Only animals older than 1 year of age were used in this study because both IBD and lymphoma are not commonly diagnosed in animals less than 1 year old, whereas infectious causes of enteritis might be present.23,27 The range of ages of the animals included in this study was 1.5–8 years of age. With a reported lifespan of 5–11 years, 16 our samples cover at least part of the typical life expectancy. We expected a positive correlation between mean group age and neoplasia, as in general, older animals are more likely to have a neoplastic transformation in the lymphocyte population. Additionally, studies on domestic and nondomestic ferrets indicated age as a risk factor for neoplasia26,27; however, no statistically significant correlation between age and diagnosis was observed. This could be related to bias introduced by sample population and size. A lack of sex predilection for lymphoma was expected, as no sex predominance has been identified for lymphoma in ferrets18,27 or other domestic animals. 11 However, more males were affected with IBD, which was surprising given a 1992 study 24 that showed no sex predisposition for IBD in either dogs or cats. It is important to note, however, that this finding may be merely a reflection of male bias in our small sample population.
There was no significant difference between the percentages of CD3+ T lymphocytes present in the various layers of the intestine in B- or T-cell lymphomas, except for the lamina propria. Even when the final diagnosis was B-cell lymphoma, a T lymphocyte component was always present. This finding is in agreement with a previous study on ferret lymphoma, 18 as well as a study in cats, 4 and is most likely a result of the normal predominance of T lymphocytes in the intestinal mucosa. 25 In contrast, B lymphocytes in the intestine are usually confined to the mucosa and submucosa, 33 and their presence in the different intestinal layers was only significantly correlated with B-cell lymphomas (i.e., B cells were rare in T-cell lymphomas).
Despite the location of normal intestinal B and T lymphocytes, no statistically significant correlation was seen between locations of B- and T-cell lymphomas in the intestinal wall. This result differed slightly from a 2012 study on feline gastrointestinal lymphoma, where the majority of the T-cell lymphomas had a mucosal distribution. 30 Despite the majority of our T-cell lymphomas being epitheliotropic, by the time of diagnosis, most of these cases were already transmurally distributed. The present study indicates that the location of the neoplasm in the intestine cannot be used as a predictor for immunophenotype in ferrets.
Along with the speculation that IBD may lead to lymphoma, it is also hypothesized that if diagnosed and treated early, the disease progression from IBD to lymphoma may be prevented. Unfortunately, clinical signs are often nonspecific or undetected. Ferrets are frequently diagnosed with IBD by histology with no clinical signs noted by the owner. This leads to the clinical conundrum of whether to treat clinically silent animals, as well as whether to empirically treat clinically affected animals without a definitive diagnosis. Treatment with prednisone alone before instituting chemotherapy in lymphoma cases can reduce the efficacy and median survival times. 21 Other therapies for treatment of IBD, such as azathioprine or metronidazole as a first line, may be indicated. However, in human medicine, there appears to be an increased incidence of non-Hodgkin lymphoma in IBD patients on immunosuppressive therapy. 15
Clinically, IBD is a diagnosis of exclusion. A definitive diagnosis is only obtained by histology; however, in ferrets, these findings may not correlate with clinical signs. Often, an abdominal exploratory surgery is performed in an attempt to diagnose or treat primary GI disease, and for this reason, full-thickness gastrointestinal biopsies are recommended during any laparotomy procedure in a ferret. However, in many mildly affected ferrets, owners are less likely to proceed with aggressive diagnostics, such as exploratory surgery, and a definitive diagnosis may not be obtained. Gastroscopy, although often underutilized, has also been described in ferrets in order to examine the gastric mucosa, as well as obtain endoscopic biopsies. 10
Limitations to our study include a limited sample size and select populations of ferrets. In some of the ferrets, different tissue samples were involved in the original diagnosis, contributing to a diagnosis of lymphoma; however, our study only analyzed samples from the small intestine, as this was the tissue that was most consistently available. The future direction of this study will involve testing the existing scoring system for IBD in small animals on ferret intestinal sections and to compare the results with the clinical severity of disease. This may encourage standardization of histologic examination of IBD in ferrets and may help link histologic diagnosis to clinical relevance. A 2011 study 25 underlined the importance of using PCR as part of the diagnostic algorithm to differentiate lymphoma from IBD in feline intestinal biopsies. Unfortunately, this was not possible in our study because PCR for clonality of lymphoid populations has not yet been developed for ferrets. For this reason, the possibility of imprecise diagnosis cannot be completely excluded in our study. In conclusion, although IHC is not necessary to distinguish IBD from lymphoma in ferret intestinal samples, it is useful when a definitive diagnosis is difficult to reach by routine histology.
Footnotes
Acknowledgements
We thank Dr. He for providing control ferret samples, Drs. Frontera Acevedo and Sophie Aschenbroich for their help in sample collection, and Ms. Butler and the University of Georgia Histology Laboratory for the histologic and immunohistochemical slide preparation. Finally, thank you to Dr. Wilson Yau for his last-minute help with our photomicrographs.
Authors’ note
MK Watson and P Cazzini equally contributed to this article. Inquiries regarding research materials can be made to the corresponding author.
Author’s contributions
MK Watson contributed to conception of the study and drafted the manuscript. P Cazzini contributed to conception and design of the study; contributed to acquisition and interpretation of data; and drafted the manuscript. J Mayer contributed to conception of the study and critically revised the manuscript. N Gottdenker contributed to acquisition and interpretation of data and critically revised the manuscript. D Reavill and N Parry contributed to acquisition and analysis of data and critically revised the manuscript. JG Fox contributed to interpretation of data and critically revised the manuscript. K Sakamoto contributed to conception and design of the study; contributed to analysis and interpretation of data; critically revised manuscript; gave final approval; and agreed to be accountable for all aspects of the work in ensuring that questions relating to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
a.
Dako North America Inc., Carpinteria, CA.
b.
HK086-9K, Power Block (HK085-5K); BioGenex Laboratories Inc., San Ramon, CA.
c.
H312-500, Fisher Scientific, Fair Lawn, NJ.
d.
NC495H, NC494H; Biocare Medical LLC, Concord, CA.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.