
Abstract
Over a 5-year period, 13 saffron finches (Sicalis flaveola) housed in mixed aviaries at the Bronx Zoo (Bronx, New York) were examined with feather loss and dermatitis, primarily affecting the nape, neck, and dorsum. Feather loss, hyperkeratosis, epidermal hyperplasia, and mixed granulocytic and mononuclear inflammation were identified in biopsies from live birds and tissue sections from postmortem specimens. In 10 of 13 cases, sections of arthropod parasites were seen histologically within feather follicles and along the surface of affected skin. Based on morphological characteristics, mites recovered from samples of formalin-fixed skin in 4 birds were identified as Microlichus americanus, an epidermoptid mite infrequently reported from wild birds and hippoboscid flies. Gross and histological lesions strongly implicate M. americanus as the cause of dermatitis affecting practically all saffron finches in the collection.
The saffron finch (Sicalis flaveola) is a small, bright yellow neotropical passerine native to South America, ranging from Argentina to Venezuela. Introduced populations also exist in other locales, including Puerto Rico, Jamaica, and Hawaii. The birds travel in pairs or small flocks, forage on the ground for insects and seeds, and visit feeders in suburban backyards. 14 Based on molecular studies, saffron finches and other species in the genus Sicalis were recently transferred from the Emberizidae family (buntings and New World sparrows) to the Thraupidae family and are now taxonomically affiliated with tanagers (Remsen JV, et al., Version 03-06-2015, A classification of the bird species of South America, Part 10, Proposal 93. Available from: http://www.museum.lsu.edu/~Remsen/SACCBaseline10.htm).
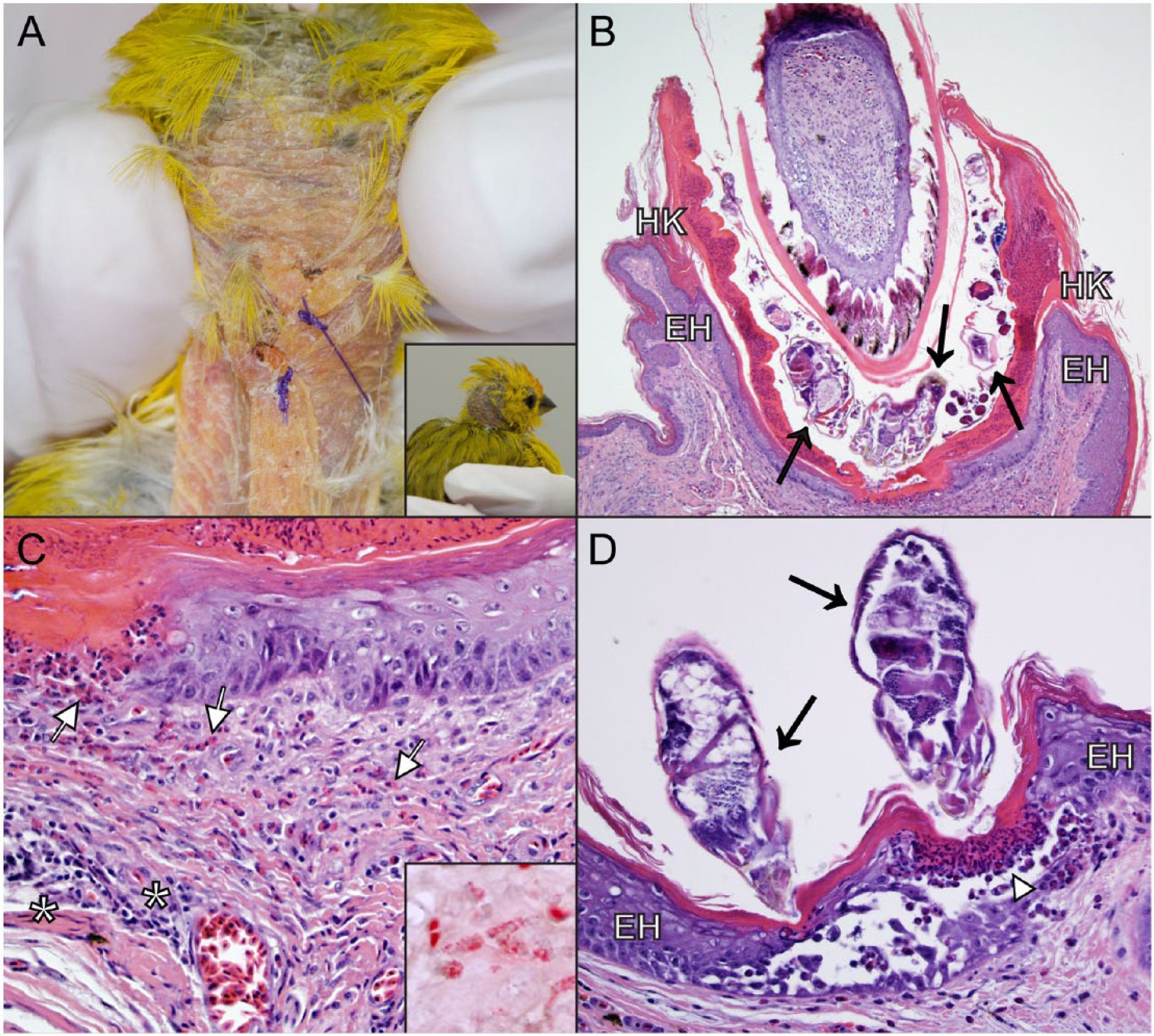
In October 2009, a group of 15 smuggled, presumably wild-caught saffron finches were confiscated in Connecticut. No notable skin lesions were observed on arrival and throughout a 30-day quarantine period at the Wildlife Conservation Society’s (WCS) Central Park Zoo (New York). Following quarantine, the birds were placed in various exhibits at the Bronx Zoo (Bronx, New York) where many bred successfully. From 2010 through 2014, most finches developed progressive feather loss over the nape, crown, and neck (Fig. 1A, inset) and of those, 13 were individually examined by WCS clinical veterinarians (finches 1–4) and/or pathologists (finches 1, 5–13). The index cases were 2 finches housed together in a small exhibit with multiple other bird species. The birds were moved into a small box cage for veterinary treatment when abnormal feathering over the nape and crown was first seen (finches 1 and 2). Ten other birds (finches 3–12) were on exhibit in a large free-flight mixed aviary and were either examined opportunistically when trapped (finches 3 and 4) or were found dead (finches 5–12). A single saffron finch was housed in a third bird exhibit before it was moved to a smaller enclosure for treatment of bacterial dermatitis (finch 13).
Dermatitis associated with Microlichus americanus infestation in saffron finches (Sicalis flaveola).
Four live saffron finches were clinically evaluated at the Bronx Zoo for dermatitis (finches 1–4). All birds initially had feather loss along the nape and neck, with thickened and rugose skin in the affected region (Fig. 1A). No other clinical signs or abnormal physical examination findings were noted in any of these birds. Finches 1 (female) and 2 (male) were adults, estimated to be ~3 years old, were housed together as a pair, and had almost identical feather loss along the nape of the neck, exposing yellow-orange, corrugated skin. Skin biopsies were obtained from both birds under anesthesia with isoflurane a in oxygen via facemask. Despite treatment with ivermectin b (0.2 mg/kg orally every 10 days for 3 doses initially, then every 14 days for 6 additional doses), lesions on the head and neck progressed in both birds. When yeast were identified on histology, a combination of itraconazole c (10 mg/kg orally every 24 hr for 120 days on food) and topical 1% chlorhexidine d solution (every 24 hr for 120 days) were initiated followed by a course of treatment with voriconazole e (10 mg/kg orally every 24 hr on food for 45 days), but none of these treatments resulted in any improvement. After 8 months, all treatments were discontinued. Finch 1 died 1 month after discontinuing treatments and was submitted for postmortem examination, at which time no mite fragments were present in the skin sampled (see below). Finch 2 was lost to follow-up.
Finches 3 and 4, adult males housed in a large free-flight aviary, were noted to have feather loss of unknown duration and were examined when opportunistically caught. Both birds had feather loss on the back of the head, nape, and neck with thickening but no discoloration of the underlying skin. The birds were anesthetized with isoflurane a in oxygen via facemask for collection of skin biopsies of the affected region and were treated with ivermectin b (0.4 mg/kg topically every 14 days for 3 treatments). Finch 3 regrew all the feathers over the head, nape, and neck within 4 weeks posttreatment. Finch 4 was found dead of traumatic injuries after the third ivermectin treatment with minimal signs of feather regrowth.
During the period between January 2010 and July 2014, 15 saffron finches that were found dead on exhibit were submitted for postmortem evaluation. Ten of these birds were found to have dermatitis including the previously described finch 1 and 9 additional birds (finches 5–13; 4 fledglings, 5 adults). The nape and neck were typically affected. Histologic features of skin from the biopsied and necropsied birds were similar. The epidermis and follicular epithelium were moderately thickened (hyperplasia), and the stratum corneum was moderately to markedly thickened by compact to basket-weave, orthokeratotic keratin (hyperkeratosis; Fig. 1B). Follicular ostia were frequently void of feathers and often dilated by orthokeratotic hyperkeratosis. Granulocytic and mononuclear inflammatory cells were present within the dermis and surrounding dermal vessels amid variable amounts of fibrosis. Granulocytes also multifocally infiltrated the epidermis and follicular epithelium (Fig. 1C), occasionally forming small aggregates (Fig. 1D). Histochemical staining (Luna stain) highlighted a granulocyte subpopulation with red-orange granule reactivity, consistent with eosinophils (Fig. 1C, inset). In 11 of the 13 (84.6%) examined cases, complete or partial arthropod segments were present within feather follicles (Fig, 1B) or, rarely, along the surface of the stratum corneum (Fig, 1D). In finch 12, a focal, chronic epidermal ulcer was present in the skin of the caudal dorsum that was histologically characterized by similar inflammation and the presence of associated arthropod segments. Serial sections of skin samples of finches 4 and 13 did not reveal mite fragments. In conjunction with the mites, surface-associated bacteria (n = 5) or ovoid yeast (n = 3) were noted in a subset of cases. In one of the cases where no mites were identified (finch 13), granulomatous dermatitis with intralesional, acid-fast–positive bacilli, consistent with cutaneous mycobacteriosis, was diagnosed. Acid-fast–positive bacilli and/or granulomatous dermatitis were not noted in any other finch.
Other postmortem findings in these 10 finches included air sacculitis and/or pneumonia (n = 3), proventricular parasitism and inflammation (n = 2), hepatitis (n = 1), and trauma (n = 1). Dermatitis was not believed to be the cause of death in any bird, although debilitation secondary to chronic skin inflammation may have predisposed the birds to other disease conditions. Seven birds were in good body condition, while 3 birds were noted to be thin.
Samples of formalin-fixed skin from 4 birds (finches 5, 6, 8, and 10) were submitted for digestion using 3 g of potassium hydroxide dissolved in 2 mL of water and placed on a slide warmer at 45°C for 2 hr; parasite identification was performed using morphology based on published species descriptions. Mites were present in all samples (Fig. 2). Morphological features, including a long dorsal palpal tibial seta with a conical base, chitinous crescentic band posterior to the anus uninterrupted, shape of epimera I–IV, extent of punctured area of the epimera, and length and width of the body, were all diagnostic for a small mite, Microlichus americanus (order Sarcoptiformes, family Epidermoptidae).1,4
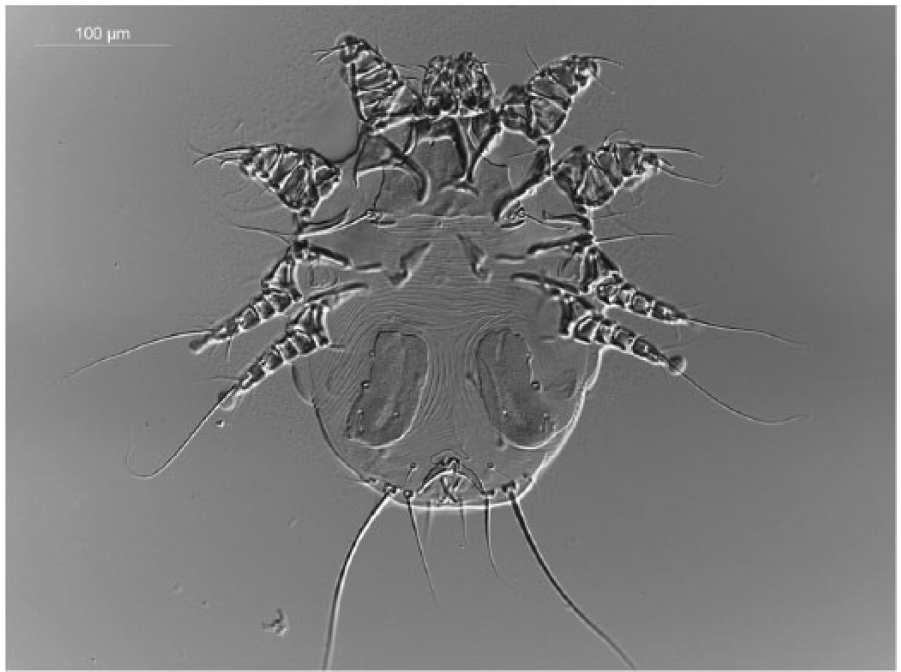
Dorsal view of a female Microlichus americanus digested with potassium hydroxide from affected, formalin-fixed saffron finch (Sicalis flaveola) skin. Bar = 100 μm.
The Epidermoptidae is a family of mites that occur in or on the skin of birds, and many species can cause avian mange. The family was recently expanded to include scaly face and leg mites in the Knemidokoptinae subfamily, formerly the Knemidokoptidae family.8,10 Mites of the genera Microlichus and Myialges are closely related and can cause dermatitis in birds. These mites have evolved a peculiar relationship with ectoparasitic insects that feed on their avian host. While male and juvenile mites live on the skin surface in epidermal burrows or feather follicles of the bird, mature gravid females disperse on avian ectoparasites, typically hippoboscid flies. Female Myialges mites are hyperparasites that attach to flies, feed on fly hemolymph, and lay clusters of eggs on their hosts that hatch into larvae. In contrast, females of genus Microlichus studied to date are merely phoretic and use hippoboscid flies for dispersal to other avian hosts, and, as such, the host range of Microlichus is a function of their hippoboscid hosts.1,8,9,12
There are several species in the genus Microlichus. Microlichus americanus is closely related to and may be a subspecies of Microlichus avus. 4 These minute mites (length of 170–390 µm) are easily overlooked on visual inspection, especially in the absence of skin lesions.1,4,5 Accounts of avian dermatitis caused by M. americanus, or other Microlichus species, are rare compared with those caused by Myialges spp. and knemidokoptine mites. Both M. avus and M. americanus have been associated with similar skin lesions in birds, including crateriform ulcers, feather loss, and severe mange.1,4,12 Microlichus americanus dermatitis was reported in 2 captive but recently imported birds at the Antwerp Zoo, a California quail (Lophortyx californicus; syn. Callipepla californica) and a baywing (Molothrus badius), as well as from an asymptomatic wild rusty blackbird (Euphagus carolinus) and a wild grey catbird (Dumetella carolinensis) in the United States. 4 Microlichus americanus has also been recovered from polyxenous hippoboscid flies (Ornithomyia fringillina) collected from a Swainson’s thrush (or, olive-backed thrush; Catharus ustulatus swainsoni), a common grackle (Quiscalus quiscula), and a field sparrow (Spizella pusilla) in Rhode Island. 12 Microlichus mite infestation without visible skin lesions has been reported in several other avian species, and M. americanus in particular has been found on asymptomatic spectacled weavers (Ploceus ocularis), lesser masked weavers (Ploceus intermedius), and red bishops (Euplectes orix) in Africa.1–3,6,7,11,13
In none of the few documented M. americanus reports is dermatitis described in multiple birds within a flock or collection. In contrast, 10 of 15 (66.7%) saffron finches submitted to the WCS pathology department for postmortem evaluation between 2010 and mid-2014 had gross or histologic evidence of acariasis. The distribution of feather loss, epidermal hyperplasia, hyperkeratosis, and inflammation over the head, nape, and dorsum was strikingly similar in all birds. This may reflect a site predilection of the mites, or more likely an inability or restricted ability for the birds to preen or reach this area. Crateriform lesions, although previously reported in birds with Microlichus acariasis, were rare in the birds in this study (1/13, 7.7%).1,4
The saffron finches in this case series were either confiscated birds, for which there was no prior history, or the progeny of those birds. It is suspected that the finches were infested with mites on arrival despite the absence of observable lesions. Characteristic skin lesions were only noted in these finches after they were moved to various indoor exhibits and aviaries. The absence of hippoboscid flies in an indoor captive setting may have hindered dispersal of gravid female mites and led to unusually heavy individual mite burdens, which resulted in increased expression of pathogenicity or morbidity. Affected saffron finches were housed in exhibits with a variety of other small passerines, including red-cheeked cordonbleu finches (Uraeginthus bengalus), red-headed finches (Amadina erythrocephala), red-faced crimson-wing finches (Cryptospiza reichenovii), African fire finches (Lagonosticta rubricata), strawberry finches (or, red avadavat; Amandava amandava), Togo paradise whydahs (Vidua togoensis), and bananaquits (Coereba flaveola), as well as several ground-dwelling birds such as blue ground doves (Claravis pretiosa), tambourine doves (Turtur tympanistria), crested partridges (Rollulus rouloul), and cinnamon teals (Anas cyanoptera), none of which ever showed evidence of dermatitis. African ploceid weavers have been reported to harbor M. americanus mites with no obvious skin inflammation, and it may be that estrildid and viduid finches are more tolerant of this mite than saffron finches. 7 However, given the peculiar mode of dispersal of M. americanus, we hypothesize that transmission of mites from saffron finches to other aviary bird species was negligible due to the lack of hippoboscid vectors. Acariasis in both adult saffron finches and captive-born progeny suggests that direct transmission among saffron finches occurred when birds were in close contact, as in the nest.
Three birds (finches 1–3) with acariasis were treated with ivermectin, but in only 1 bird (finch 1) were posttreatment biopsies obtained. Mites were not present in tissue sections posttreatment (finch 1) and 1 finch (finch 3) regrew all feathers, suggesting ivermectin was efficacious in eradicating the mites. However, resolution of clinical signs and regrowth of feathers was not noted in finches 1 and 2 despite 8 months of treatment. Severe, extensive, and likely irreversible damage to follicles, as identified histologically, and secondary bacterial and fungal infection may explain why feather loss and dermatitis persisted. Treatment with 0.2 – 0.4 mg/kg of ivermectin every 14 days for 2 – 3 treatments seemed to be effective.
In summary, this report documents chronic acariasis and dermatitis in a captive population of saffron finches, characterized by active eosinophilic, heterophilic, and lymphoplasmacytic infiltration of the skin and feather follicles, with intralesional mites. Microlichus americanus was strongly incriminated as the cause of disease in these birds.
Footnotes
Acknowledgements
We thank the Wildlife Conservation Society’s Department of Ornithology, Special Animal Exhibits, and clinical medical staffs for their exceptional care, Alfred Ngbokoli and Daniel Friedman for slide preparation, and the additional pathologists who provided diagnostic support in the above cases (Drs. Alisa Newton, Ken Conley, and Carlos Rodriguez).
a.
MWI Veterinary Supply Inc., Boise, ID.
b.
Norbrook Laboratories Ltd., Co. Down, Ireland.
c.
Centocor Ortho Biotech Products, Ravitan, NJ.
d.
Fort Dodge Animal Health, New York, NY.
e.
Sigma-Aldrich, St. Louis, MO.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support was provided by the Wildlife Conservation Society for the publication of this article.