
Abstract
Papillomaviruses (PVs) are well recognized to cause human oral squamous cell carcinomas (SCCs). However, there is currently little evidence that PVs similarly cause oral cancer in dogs. In the present case, a dog developed an invasive SCC and multiple in situ carcinomas within the mouth. Cell changes consistent with PV infection were prominent within the neoplasms and the surrounding gingiva. Immunohistochemical staining revealed PV antigens and intense p16CDKN2A protein (p16) immunostaining within the invasive SCC. Papillomaviral DNA sequences were amplified from the invasive and in situ carcinomas. Sequencing revealed that the DNA was from a novel PV that appears most closely related to canine PV-2 and -7. To the authors’ knowledge, multiple carcinomas have not been previously reported in the mouth of a dog. Additionally, the current study describes PV cytopathology in a canine oral SCC. Whether the PV infection influenced neoplasm development cannot be definitively determined in this case. However, the presence of p16 immunostaining and the development of multiple oral carcinomas support a role of the PV in tumorigenesis in this dog.
Squamous cell carcinomas (SCCs) are the second most common canine oral malignancy and typically appear as a raised ulcerated gingival mass.7,17 As oral SCCs are typically infiltrative, they are a significant cause of morbidity and mortality in dogs. 7
While no cause can be identified for most canine oral SCCs, well-established risk factors for oral SCCs in human beings include exposure to tobacco and alcohol and infection by “high-risk” alpha human papillomaviruses (HPVs). 4 Up to 20% of human oral SCCs are caused by HPVs, 5 and the recognition of the role of these viruses in both oral and genital cancers has led to the widespread use of HPV vaccines in many Western countries. Fifteen fully classified Canine papillomavirus (CPV) types are recognized to infect domestic dogs. 19 While CPV-1 (formerly Canine oral papillomavirus) and CPV-13 cause self-resolving oral papillomas in dogs,2,8 there is currently little evidence that PV infection causes canine oral neoplasia.
Herein, we describe a dog with an invasive SCC and multiple in situ carcinomas of the oral cavity that contained prominent PV-induced cell changes. To the authors’ knowledge, this is the first report of multiple oral carcinomas in a dog. Additionally, prominent PV cytopathology is described in a canine oral SCC, and DNA sequences from a novel PV type were amplified from the carcinomas.
A 7-year-old intact male Labrador dog developed excessive salivation and an approximately 1.5 cm in diameter exophytic gingival mass caudal to the right upper canine tooth (Fig. 1). The mass was not ulcerated and had a roughened surface. Radiology revealed osteolysis of the underlying maxilla, and a sample of the mass was taken for histology. In addition to the exophytic mass, 7 raised, pale, roughened plaques were visible within the right buccal gingiva. The sessile appearance of these plaques was in contrast to the normally exophytic appearance of a canine oral papilloma.
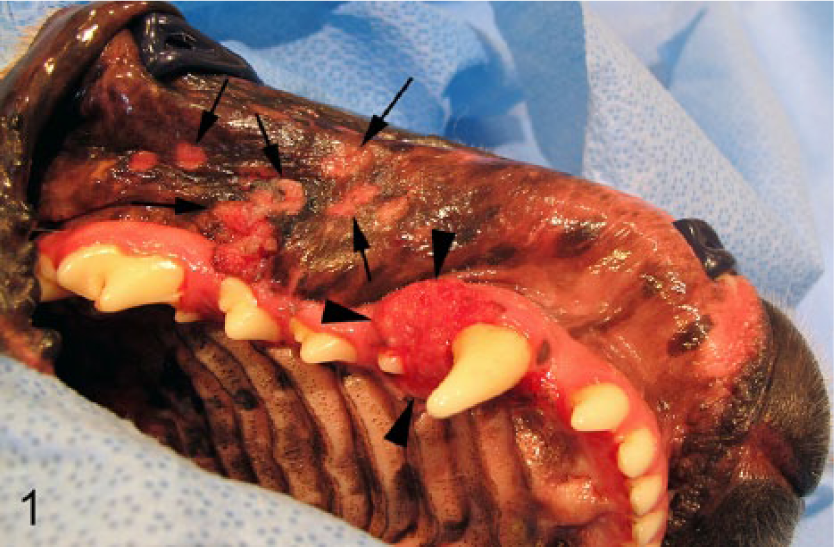
A large exophytic mass is visible immediately adjacent to the upper canine tooth (arrowheads) with multiple pale sessile plaques visible within the buccal gingiva (arrows).
Histology of the maxillary mass showed a proliferation of large polygonal cells arranged in nests and trabeculae extending into the underlying submucosa. Keratinization was often prominent in the center of the nests of neoplastic cells. Scattered throughout the neoplasm were numerous neoplastic cells that were enlarged and had blue-gray slightly granular cytoplasm and nuclei that were swollen and contained eosinophilic material. These cells were most common toward the center of the cell nests and were often accompanied by clumping of keratohyalin granules. Less frequently, clusters of large cells with dark shrunken nuclei and perinuclear halos (consistent with koilocytes) were also visible. The epithelium surrounding the neoplasm was thickened and dysplastic with increased numbers of crowded small irregular keratinocytes visible within the deeper layers. Cells with blue-gray cytoplasm and koilocytosis were also visible within the superficial layers of the dysplastic epithelium. The submucosa underneath the dysplastic epithelium contained moderate lymphoplasmacytic inflammation and numerous macrophages containing melanin. The histological diagnosis was oral SCC with prominent PV-induced cytopathology.
To further investigate the presence of a PV within the SCC, total genomic DNA was extracted, and PV DNA was amplified using the FAP59/64 and the MY09/11 consensus primer sets as previously described. 25 Both consensus primer sets amplified DNA, which was then sequenced and compared to sequences within GenBank as previously described. 15 Comparison of the 404-bp sequence amplified by the FAP59/64 primers (GenBank accession no. KM086731) revealed the greatest similarity to CPV-2 with 73% similarity over 401 bp. The sequence was 75% similar over 310 bp to CPV-7 but was dissimilar to CPV-1. The 342-bp sequence amplified by the MY09/11 primers (KM086732) was also dissimilar to CPV-1, but was 73% similar over 336 bp to CPV-2 and 72% similar over 332 bp to CPV-7.
Ten days after initial presentation, a maxillectomy was performed to remove the SCC. At this time, a sample of buccal gingiva containing 2 visible plaques was also surgically excised. Histology of the examined maxilla confirmed the presence of an invasive SCC (Fig. 2). As in the earlier sample, numerous cells within the neoplasm contained histological evidence of PV infection (Fig. 3). The presence of PV antigen within the nuclei of keratinized cells was confirmed by immunohistochemical staining, a which was also used to detect p16CDKN2A protein (p16), b revealing intense cytoplasmic and nuclear immunostaining within approximately 60% of the neoplastic cells (Fig. 4). Immunostaining was consistently present within the cells at the periphery of the neoplastic cell nests, but tended to be reduced as keratinocytes became more keratinized. Histological examination of sections of buccal gingiva revealed multiple foci of epithelial hyperplasia and dysplasia. Changes within these foci were similar to those observed within epithelium surrounding the initially submitted SCC, and the dysplastic cells exhibited abnormal keratinization and often contained blue-gray cytoplasm, consistent with PV infection (Fig. 5). Although the dysplastic epithelium extended into the underlying submucosa within broad papillary projections, there was no invasion of the basement membrane, and a diagnosis of multiple in situ carcinomas was made.
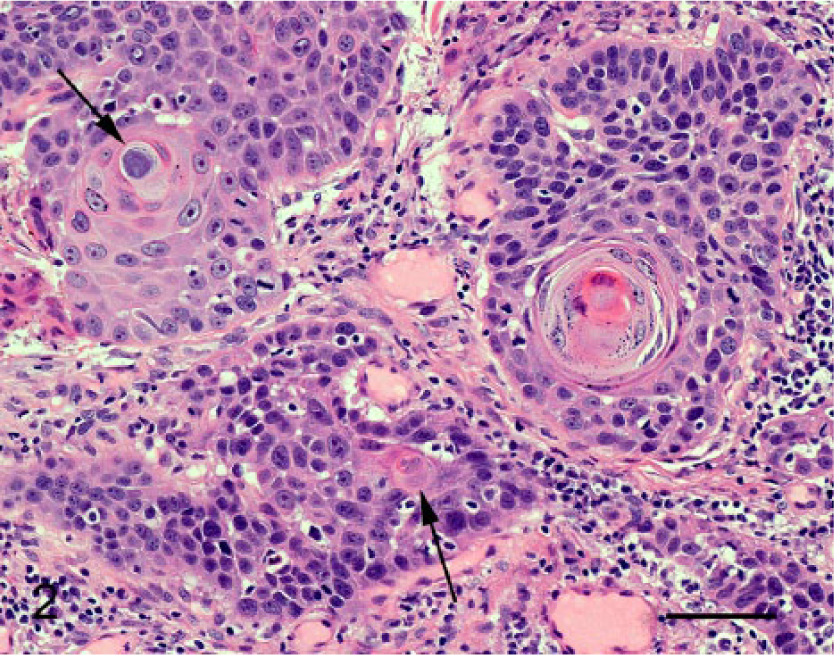
Section of maxillary squamous cell carcinoma showing nests and trabeculae of neoplastic epithelial cells within the submucosa. Evidence of papillomavirus infection is visible in some cells (arrows). Hematoxylin and eosin. Bar = 60 µm.
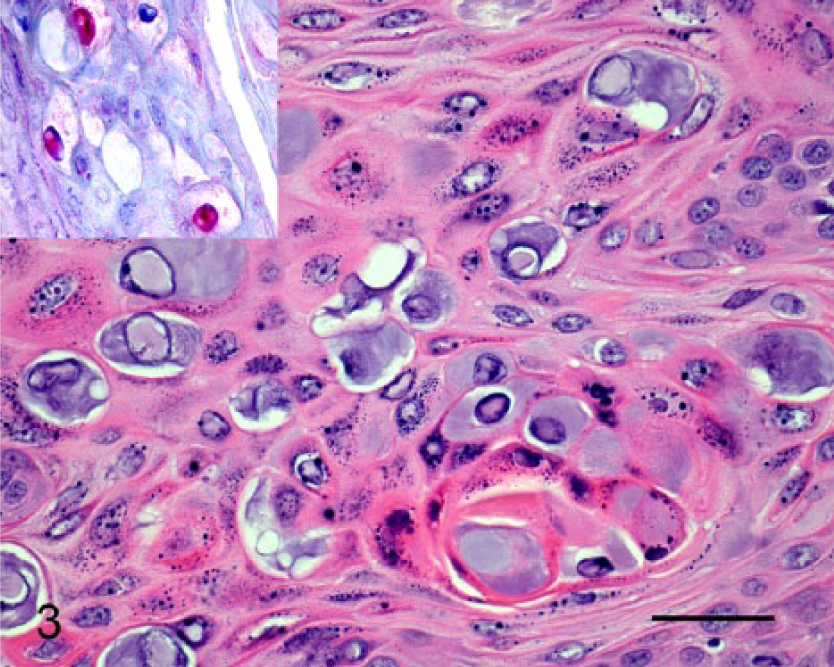
Section of maxillary squamous cell carcinoma. Note the presence of enlarged cells with blue-gray cytoplasm and nuclei that are expanded by eosinophilic material. The papillomavirus (PV) cytopathology is most prominent in keratinized cells close to the center of the neoplastic cell nests. Hematoxylin and eosin. Bar = 30 μm. Immunohistochemical staining using anti-PV L1 antibodies reveals intranuclear immunostaining (inset). Enhanced V-Red detection kit. c
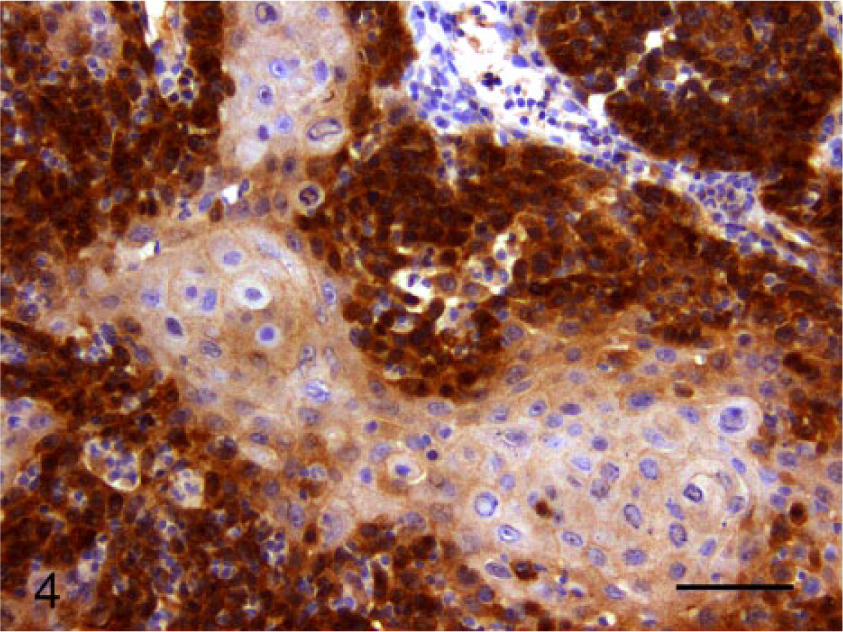
Section of maxillary squamous cell carcinoma showing intense cytoplasmic and nuclear immunostaining using anti-p16CDKN2A antibodies. Bond Refine Detection staining kit. d Bar = 55 μm.
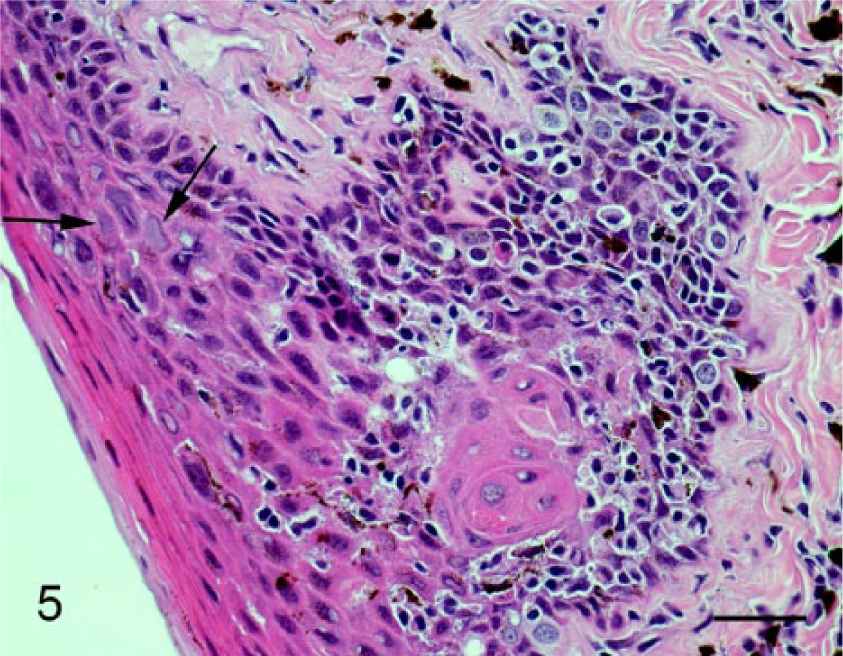
Section of buccal mucosa. Note the papillary projection of the epithelium into the underlying submucosa, the presence of marked epithelial cell dysplasia, and abnormal keratinization. Cells showing evidence of papillomavirus infection are visible within the dysplastic foci (arrows). Hematoxylin and eosin. Bar = 50 µm.
The same novel PV sequences were amplified from the in situ carcinomas. The final diagnosis was an invasive SCC and multiple in situ oral carcinomas with concurrent infection by a novel PV.
While oral SCCs are common in dogs, multicentric carcinomas have not been previously reported in the canine oral cavity. In contrast, up to 7% of people with oral SCCs will either have multiple SCCs at presentation or develop an additional SCC after treatment. 23 The increased risk of additional neoplasm development is because the carcinogenic factors that caused the initial oral SCC (e.g., tobacco and alcohol) also predispose the rest of the mouth to cancer development. This so-called “field cancerization” 20 is visible histologically as an increase in epithelial dysplasia throughout the oral cavity. 23 In the present dog, the development of an invasive SCC and multiple in situ carcinomas is consistent with field cancerization and suggests that the oral cavity was exposed to a carcinogen.
The widespread histological and molecular evidence of PV infection in the oral carcinomas suggests that the field cancerization in this dog could have been due to infection by the novel PV. Papillomaviruses are an established cause of human cancer, and there is accumulating evidence that they are also a significant cause of neoplasia in some veterinary species.11,14 However, the only previously published evidence supporting a role of PVs in canine oral SCCs is the observation that a SCC developed in an area of oral papillomatosis in a young dog, 26 the amplification of CPV-1 DNA from 3 of 29 canine oral SCCs, 22 and the amplification of unclassified non–CPV-1 PV E1 gene sequences from 4 of 17 gingival SCCs. 27 The detection of a PV within the multiple oral carcinomas in the present case provides additional evidence that these viruses could influence oral neoplasia in dogs. However, as asymptomatic PV infections are detectable in the mouth of 38% of dogs, 10 simply detecting a PV does not prove that the PV caused the neoplasia and, in the present case, it cannot be excluded that an unidentified factor caused both the neoplasia and an increased susceptibility to PV infection.
The “high-risk” human PVs cause cancer by altering well-defined pathways in cell cycle regulation. These mechanisms of PV-induced carcinogenesis are so consistent that a PV etiology of a neoplasm can be determined by detecting changes in the cell regulatory proteins. In human PV-induced oral SCCs, degradation of the retinoblastoma protein by the PV E7 protein has been shown to increase cellular p16, and the presence of intense cytoplasmic and nuclear p16 immunostaining indicates a PV etiology. 21 A similar association between p16 immunostaining and the presence of PV DNA has also been demonstrated in feline skin SCCs.12,13 In dogs, scant p16 immunostaining within a small proportion of cells has been previously reported within some neoplasm types. 1 However, the frequent intense nuclear and cytoplasmic p16 immunostaining that was observed in the present case has not, to the authors’ knowledge, been previously reported in a canine neoplasm. As the p16 immunostaining pattern observed in the canine oral SCC is consistent with the immunostaining patterns reported in PV-induced human oral SCCs, this provides additional support for a possible role of the PV in cancer development.
The PV sequences amplified in the current case are from a novel canine PV type. Although complete classification is not possible without determining the complete L1 gene sequence, the PV sequence was most similar to CPV-2 and CPV-7. CPV-2 has been associated with cutaneous SCC development in treated severe combined immunodeficiency (SCID) dogs, 6 and CPV-7 has been detected in a cutaneous in situ carcinoma. 9 As both CPV-2 and -7 appear to have some oncogenic potential, the similarity of the novel PV to these PVs suggests it may also be able to influence neoplasia development.
If the dog in the current study did develop oral SCCs due to infection by the novel PV, it has to be explained why evidence of this PV in canine oral SCCs has not been previously reported. While it is possible that infection by this PV is rare, most PVs are well adapted to their hosts allowing frequent asymptomatic infection.10,16 Therefore, if the novel PV did cause the oral cancer in this dog, an unusual host reaction to the PV may be most likely. This is supported by studies of the relationship between PVs and both human and canine cutaneous SCCs, which suggest that an abnormal host reaction is the most important determinant of disease.6,18,24 However, if an abnormal host reaction to the novel PV did predispose to oral SCC, the dog showed no other evidence of immunosuppression.
The presence of viral cytopathology and PV L1 antigen in the canine oral SCCs suggests that viral replication was present in the neoplasms. While PV replication was also reported in a series of CPV-2–associated SCCs in treated SCID dogs, 6 integration of the PV DNA into the host genome generally prevents PV replication in human PV-induced SCCs. 3
In conclusion, the dog in the present report developed an invasive oral SCC and multiple oral in situ carcinomas that contained DNA sequences from a novel PV. While the precise role of the PV remains uncertain, the development of multiple neoplasms in the mouth of a dog is highly unusual suggesting that the PV infection could have influenced lesion development. Further studies are required to determine why this dog developed this disease, but it is hypothesized that an inappropriate host response to the PV predisposed to oral neoplasia in this dog. If the development of canine oral SCCs is influenced by PV infection, evidence from human studies suggests this may allow the behavior of a canine oral SCC to be more accurately predicted. In addition, it may be possible to decrease neoplasia development by reducing PV infection of the oral cavity.
Footnotes
a.
Anti-human PVs 1, 6, 11, 16, 18, and 31; Lifespan Biosciences, Seattle, WA.
b.
Mouse anti-human p16 monoclonal antibody, BD Biosciences, San Jose, CA.
c.
Enhanced V-Red detection kit, Ventana Medical Systems Inc., Tucson, AZ.
d.
Bond Refine Detection staining kit, Leica Microsystems Inc., Buffalo Grove, IL.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.