
Abstract
N-terminal pro–B-type natriuretic peptide (NT-proBNP) has been shown to have clinical utility as a biomarker in dogs with heart disease. There were several limitations associated with early diagnostic assay formats including a limited dynamic range and the need for protease inhibitors to maintain sample stability. A second-generation Cardiopet® proBNP enzyme-linked immunosorbent assay (IDEXX Laboratories Inc., Westbrook, Maine) was developed to address these limitations, and the present study reports the results of the analytical method validation for the second-generation assay. Coefficients of variation for intra-assay, interassay, and total precision based on 8 samples ranged from 3.9% to 8.9%, 2.0% to 5.0%, and 5.5% to 10.6%, respectively. Analytical sensitivity was established at 102 pmol/l. Accuracy averaged 102.0% based on the serial dilutions of 5 high-dose canine samples. Bilirubin, lipids, and hemoglobin had no effect on results. Reproducibility across 3 unique assay lots was excellent with an average coefficient of determination (r2) of 0.99 and slope of 1.03. Both ethylenediamine tetra-acetic acid plasma and serum gave equivalent results at time of blood draw (slope = 1.02, r2 = 0.89; n = 51) but NT-proBNP was more stable in plasma at 25°C with median half-life measured at 244 hr and 136 hr for plasma and serum, respectively. Plasma is the preferred sample type and is considered stable up to 48 hr at room temperature whereas serum should be frozen or refrigerated when submitted for testing. Results of this study validate the second-generation canine Cardiopet proBNP assay for accurate and precise measurement of NT-proBNP in routine sample types from canine patients.
Introduction
B-type (or brain) natriuretic peptide (BNP) is stored in cardiomyocytes as a prohormone (proBNP) that is released in response to stretch or strain on heart muscle. On release, proBNP is cleaved into a biologically active hormone (carboxy-terminal C-BNP) and an inactive amino-terminal fragment (NT-proBNP). BNP is actively removed from the bloodstream in addition to passive clearance via glomerular filtration and proteolysis. In dogs, the half-life of C-BNP is approximately 90 sec in plasma, 15 which poses a challenge to accurately measure circulating plasma levels. Clearance of NT-proBNP is restricted to passive mechanisms alone, resulting in a longer half-life in plasma as well as making circulating NT-proBNP more amenable to measurement for clinical applications. NT-proBNP is released in proportion to the amount of stretch and stress on the myocardium, and the concentration often increases with the severity of heart disease in canine patients.1,10 In addition, studies have shown that the presence of elevated levels of NT-proBNP may be an indicator to assist in predicting the first onset of congestive heart failure in dogs with mitral valve disease as well as prognostic information on survival.8,9,11,12,17
A first-generation immunoassay for the quantitative measurement of NT-proBNP in canine plasma a provided reproducible results from ethylenediamine tetra-acetic acid (EDTA) plasma samples in a range of 50–3000 pmol/l with coefficients of variation (CVs) for intra- and interassay precision of <15% across the full range of the assay.1,14 The enzyme-linked immunosorbent assay (ELISA) utilized 2 affinity-purified sheep anti-canine NT-proBNP polyclonal antibodies, one on the solid phase capture and another in the liquid detection reagent. The 2 antibodies bound different epitopes on the NT-proBNP; however, the 2 epitopes were separated by putative proteolytic cleavage sites on the peptide leading to rapid degradation in some samples when stored at room temperature. 7 To mitigate the risk of sample degradation, the original product required the use of a specialized protease inhibitor tube for sample transport. Alternatively, samples could be stored and shipped frozen to reduce degradation.
The upper limit of the reportable range of the first-generation assay was 3,000 pmol/l. Dogs with heart disease may have circulating levels of NT-proBNP well more than 3,000 pmol/l, and this truncated dynamic assay range prevented the measurement of NT-proBNP across the full range of biological variation in dogs with heart disease. This constraint limited the use of the test for monitoring NT-proBNP levels during disease progression or in response to treatment. Routine utilization of the assay was also hindered by the need for the specialized protease inhibitor tube.
The current study describes the analytical method validation of an improved, second-generation canine NT-proBNP assay. The new assay eliminates the need for the specialized protease inhibitor blood collection tube by using new antibodies that target a more stable contiguous fragment of NT-proBNP and offers an expanded dynamic range with an upper reporting limit of 10,000 pmol/l.
Materials and methods
Measurement of NT-proBNP
The second-generation canine NT-proBNP assay is a sandwich ELISA. As in the first-generation assay, the capture antibody is immobilized on 96-well microtiter plates, and the detection antibody is conjugated to horseradish peroxidase. To improve assay precision, the second-generation assay includes an increased number of calibrators (6) with increasing levels of NT-proBNP peptide in a protein buffer base as well as 3 controls (low, medium, and high) that are routinely analyzed and provide internal quality control for each assay run.
To perform the second-generation assay, calibrators, controls, and samples are diluted 1:6 using a sample dilution buffer. An aliquot of the premixture is added to duplicate microtiter wells coated with anti–NT-proBNP antibody, and the plates are incubated at 25°C for 1 hr. Plates are washed 5 times with 1× wash solution in an automatic plate washer, an aliquot of detection antibody–horseradish peroxidase conjugate (a second anti–NT-proBNP antibody) is added to each well, and the plates are incubated at 25°C for 1 hr. Plates are washed as above, 3,3′,5,5′-tetramethylbenzidine (TMB) substrate is added to each well, and the plates are incubated at 25°C for 15 min. Stop solution is then added to each well, and the optical density (OD) values are obtained with a spectrophotometer based on absorbance at a wavelength of 450 nm (OD450). A calibration curve is fit with a second-order polynomial trend line, and the concentration of NT-proBNP in each control and patient sample is interpolated using the equation of the line. The reportable range of the assay is 250–10,000 pmol/l. The preferred sample type for the second-generation assay is EDTA plasma but serum is also acceptable for use. The predilution of the sample plus the 2-step assay format minimizes the risk of sample matrix effects on assay results.
Sample collection
Canine plasma samples were collected in EDTA tubes, and serum samples were collected in red-top or serum-separator tubes. Plasma samples were provided as EDTA plasma or as EDTA plasma transferred into protease inhibitor tubes. Samples were obtained from IDEXX Reference Laboratories, licensed contract research organizations, universities, and veterinary clinics. All samples were shipped on dry ice and stored frozen until the time of testing.
Analytical validation methods
Methods used to perform the analytical validation testing were based on industry standard guidance documents published by the U.S. Food and Drug Administration (http://www.fda.gov/downloads/Drugs/Guidances/ucm070107.pdf) and the Clinical and Laboratory Standards Institute2–6 as well as on internal best practices. Data analysis was performed using commercial software.b–d
Precision testing was performed using 4 native canine EDTA plasma pools (486, 992, 3,797, and 7,785 pmol/l) and 4 manufactured samples containing purified NT-proBNP in a protein buffer base (466, 976, 3,981, and 8,036 pmol/l). Each sample was tested in 3 sets of duplicate wells per plate using 3 independent sample dilutions. Three operators tested 2 plates from each of 3 unique assay lots on each of 3 days. The total number of dose values generated for each sample was 162, and each dose was the average of duplicate wells. For each sample, the mean, standard deviation (SD), and CV were calculated for total, intra-assay, and interassay precision.
Analytical sensitivity of the assay was determined by measuring the limit of blank (LOB) and limit of detection (LOD) on 3 unique lots of the second-generation assay. The LOB was measured by testing 60 replicates of a negative calibrator and calculating the dose at 1.645 times the SD of the 60 OD values. The LOD was measured by testing 60 replicates of manufactured low-dose samples containing purified NT-proBNP in a protein buffer base (10 replicates each of 6 low-dose positive samples ranging from 30 to 242 pmol/l of NT-proBNP). The LOD was calculated using the following equation: LOD = LOB + cβ (SD of sample readback), where cβ = 1.645/(1–1/(4 × f)), where f = degrees of freedom.
Accuracy and dilutional linearity were evaluated using 2-fold serial dilutions of 5 canine EDTA plasma pools with NT-proBNP concentrations >8,000 pmol/l. Dilutions were prepared using a low-dose EDTA plasma pool containing 432 pmol/l of NT-proBNP. Neat and diluted samples were tested in duplicate wells on 3 independent runs on each of 3 unique assay lots for a total of 18 replicates per sample dilution. The averaged results were used to determine the measured dose for each sample dilution. For each sample, the measured dose of the lowest dilution factor (neat or 1:2) that ran below the upper limit of the assay (10,000 pmol/l) was used to calculate the expected dose values for the related sample dilutions. The percent recovery of measured dose compared to expected dose was calculated for each sample dilution. Expected dose values were plotted against measured dose values, and linear regression was used to calculate the slope between the measured and expected dose values.
To determine if increased concentrations of commonly occurring sample matrix components would interfere with the accuracy of the second-generation NT-proBNP assay, the effect of elevated hemoglobin, lipids, and bilirubin was evaluated. Each substance was spiked into a low dose (1,210 pmol/l) and a high dose (4,058 pmol/l) EDTA plasma pool at increasing concentrations, and the NT-proBNP dose was measured and compared to unspiked sample results. Hemoglobin e was spiked at concentrations ranging from 150 to 520 mg/dl. Bilirubin f was spiked at concentrations ranging from 3.9 to 17.6 mg/dl. Lipid g was spiked to OD660 values ranging from 2.7 to 7.9. Three sets of duplicate wells were tested on a single assay lot, and results were analyzed by 1-way analysis of variance using an α risk of 0.05.
Assay reproducibility was measured by testing 296 EDTA plasma samples on each of 3 unique assay lots. Passing–Bablok regression was used to compare results between the 3 lots (lot 1 vs. lot 2; lot 1 vs. lot 3; lot 2 vs. lot 3).
Agreement between the first- and second-generation assays was compared using a set of 168 individual native canine EDTA or protease-inhibited (PI) plasma samples with NT-proBNP concentrations falling within the dynamic ranges of both assays. Samples were tested on 3 distinct lots of the second-generation assay and on 1–3 lots of the first-generation assay, depending on available sample volume. A Bland–Altman analysis was performed using the mean values of the first-generation and second-generation assays, and the bias between methods was determined.
NT-proBNP recovery and stability in EDTA plasma versus serum
NT-proBNP measurement in EDTA plasma and serum was compared by testing 51 matched pairs of EDTA plasma and serum samples with dose values covering the entire dynamic range of the assay. The measured NT-proBNP dose of EDTA plasma samples was plotted against the NT-proBNP dose of the matching serum samples, and Passing–Bablok regression was used to analyze the results.
Forty sets of paired EDTA plasma and serum samples with sufficient volume were evaluated for analyte integrity over time at 4°C and 25°C storage. Each sample was divided into single-use volumes. Aliquots were stored at 4°C and 25°C, and a single set of aliquots was stored at −20°C to serve as a baseline control. For each storage temperature (4°C and 25°C), aliquots were transferred to −20°C after 24 hr at temperature, after 48 hr at temperature, and after 72 hr at temperature. Once all aliquots had been refrozen, samples were thawed and tested together in a single test event. The NT-proBNP dose of each temperature-stressed aliquot was compared to the dose of the −20°C baseline control, and the percent recovery of baseline was calculated. In addition, 4°C and 25°C first-order decay curves for natural log-transformed NT-proBNP concentration versus time were constructed for each dog by sample type. For each decay curve, the half-life (t1/2) was calculated as
where λ z is the slope of the first-order decay curve. 16
Results
Analytical validation
Across 8 samples with NT-proBNP dose values from 466 to 8,036 pmol/l, the total percent CV ranged from 5.5% to 10.6%, the intra-assay (within-plate) percent CV ranged from 3.9% to 8.9%, and the interassay (between-plate) percent CV ranged from 2.0% to 5.0% (Table 1). Based on 60 replicates of a negative calibrator, the LOB ranged from 16 to 76 pmol/l. Based on 60 replicates of low-dose samples (<242 pmol/l), the LOD ranged from 32 to 102 pmol/l. Across 5 sample dilution series, the average percent recovery of measured dose value against expected value was 102% ± 1.7%. Linear regression analysis of expected dose values plotted against measured dose values generated slope values ranging from 0.998 to 1.001 (Fig. 1). The analysis of interfering substances showed no statistically significant difference between unspiked plasma samples and samples containing hemoglobin at concentrations up to 520 mg/dl (P = 0.713 for the low-dose sample, and P = 0.430 for the high-dose sample), bilirubin at concentrations up to 17.6 mg/dl (P = 0.244 for the low-dose sample, and P = 0.060 for the high-dose sample), or lipids up to an OD660 of 7.9 (P = 0.429 for the low-dose sample, and P = 0.073 for the high-dose sample). Comparing results of 296 EDTA plasma samples between 3 kit lots (lot 1 vs. lot 2; lot 1 vs. lot 3; lot 2 vs. lot 3), the slopes determined by Passing–Bablok regression were 1.02, 1.04, and 1.03 with r2 values of 0.986, 0.988, and 0.985, respectively (Fig. 2). Comparing the average results of 168 samples, a statistically insignificant (P = 0.1475) bias of 61 pmol/l was measured between the first- and second-generation assays (Fig. 3).
Second-generation canine N-terminal pro–B-type natriuretic peptide (NT-proBNP) assay precision results for 4 manufactured samples and 4 native canine ethylenediamine tetra-acetic acid (EDTA) plasma samples (162 values per sample, tested over 3 days by 3 technicians using 3 manufactured kit lots).*
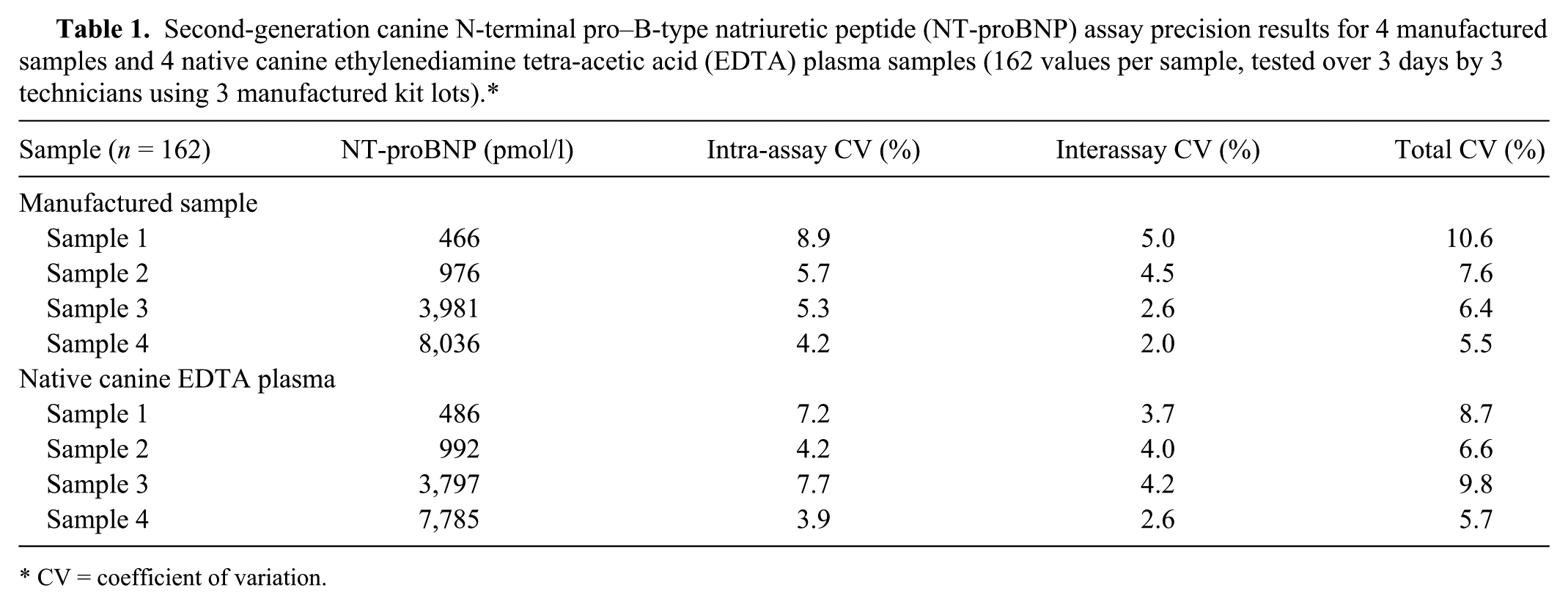
CV = coefficient of variation.
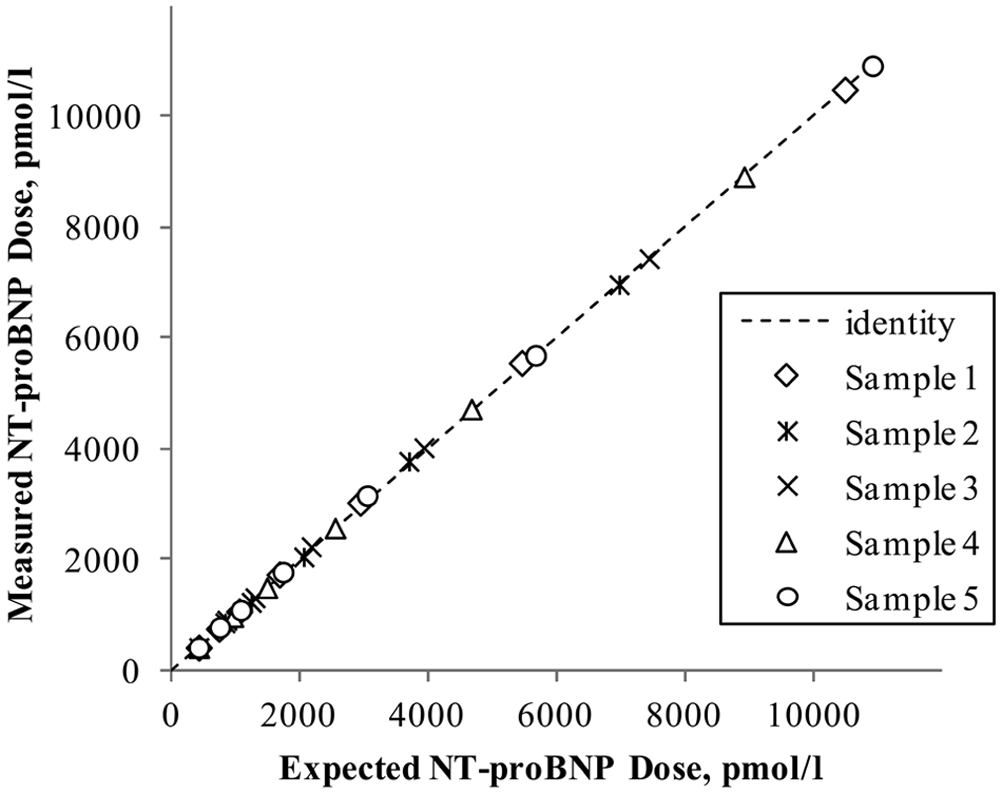
Measured versus expected concentrations determined by the second-generation canine N-terminal pro–B-type natriuretic peptide (NT-proBNP) assay based on serial dilutions of 5 high-dose canine samples. For each dilution series, the following slopes were determined by linear regression: sample 1, slope (m) = 1.000; sample 2, m = 1.001; sample 3, m = 0.999; sample 4, m = 1.000; sample 5, m = 0.998.
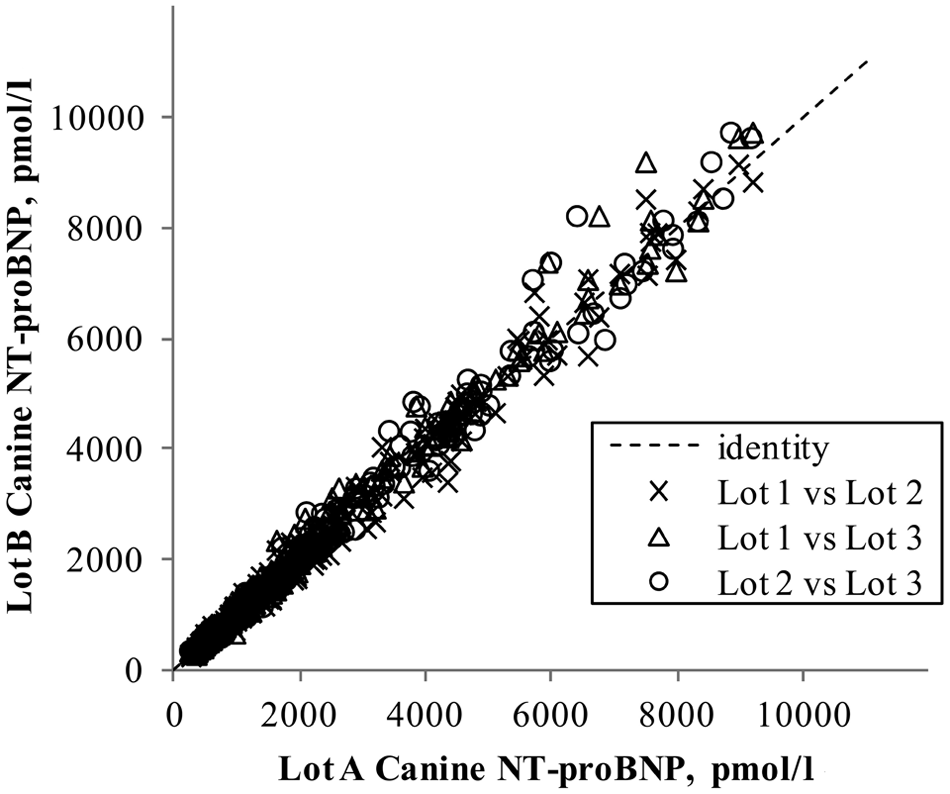
Reproducibility of 296 canine samples across 3 unique lots of the second-generation canine N-terminal pro–B-type natriuretic peptide (NT-proBNP) assay. Equations for Passing–Bablok regression fit and coefficients of determination (r2) for the 3 lot pairings were: lot 1 vs. lot 2, y = 1.02 + 15, r2 = 0.986; lot 1 vs. lot 3, y = 1.04 – 2, r2 = 0.988; lot 2 vs. lot 3, y = 1.03 – 19, r2 = 0.985.
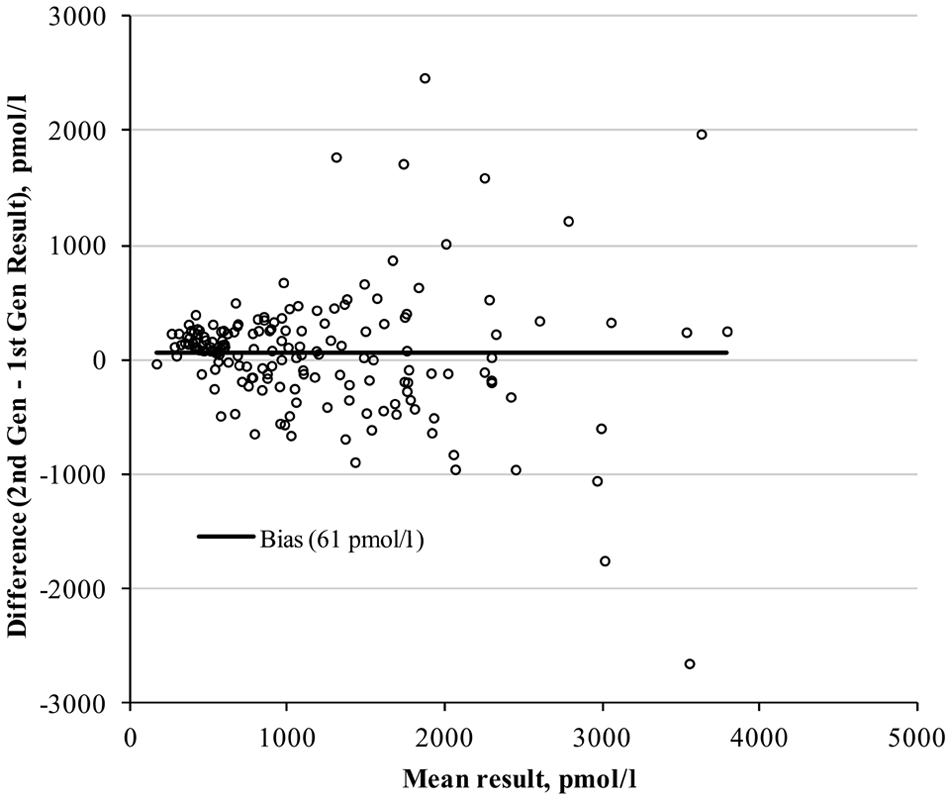
Bland–Altman difference plot for 168 canine samples that ran within the dynamic range of both first- and second-generation canine N-terminal pro–B-type natriuretic peptide assay methods. The determined bias is 61 pmol/l (P = 0.1475).
NT-proBNP recovery and stability in EDTA plasma versus serum
Passing–Bablok regression analysis of results from 51 matched pairs of EDTA plasma and serum samples produced a slope of 1.02 and r2 value of 0.89 (Fig. 4). NT-proBNP analyte stability measured in 40 matched pairs of EDTA plasma and serum samples showed that after 72 hr of storage at 4°C, EDTA plasma retained 98% of baseline and serum retained 93% of baseline, on average (Fig. 5A). For samples stored at 4°C, the median half-life of NT-proBNP was 1,662 and 881 hr for EDTA plasma and serum, respectively. When stored at 25°C, EDTA plasma retained 96% of baseline at 24 hr, 90% at 48 hr, and 81% at 72 hr, on average. Average recovery of baseline NT-proBNP for serum stored at 25°C was 85% at 24 hr, 76% at 48 hr, and 65% at 72 hr (Fig. 5B). The median half-life of NT-proBNP in samples stored at 25°C was 244 and 136 hr for EDTA plasma and serum, respectively.
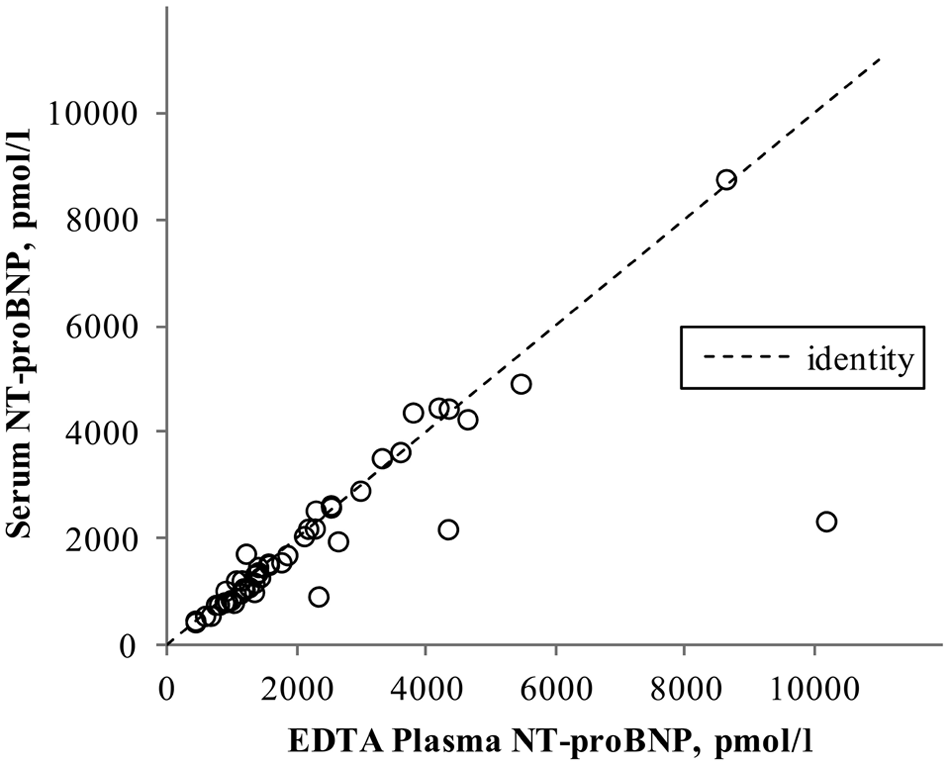
Comparison of 51 matched pairs of serum and ethylenediamine tetra-acetic acid (EDTA) plasma samples on the second-generation canine N-terminal pro–B-type natriuretic peptide (NT-proBNP) assay. The equation for Passing–Bablok regression fit was y = 1.02 – 59, r2 = 0.89.
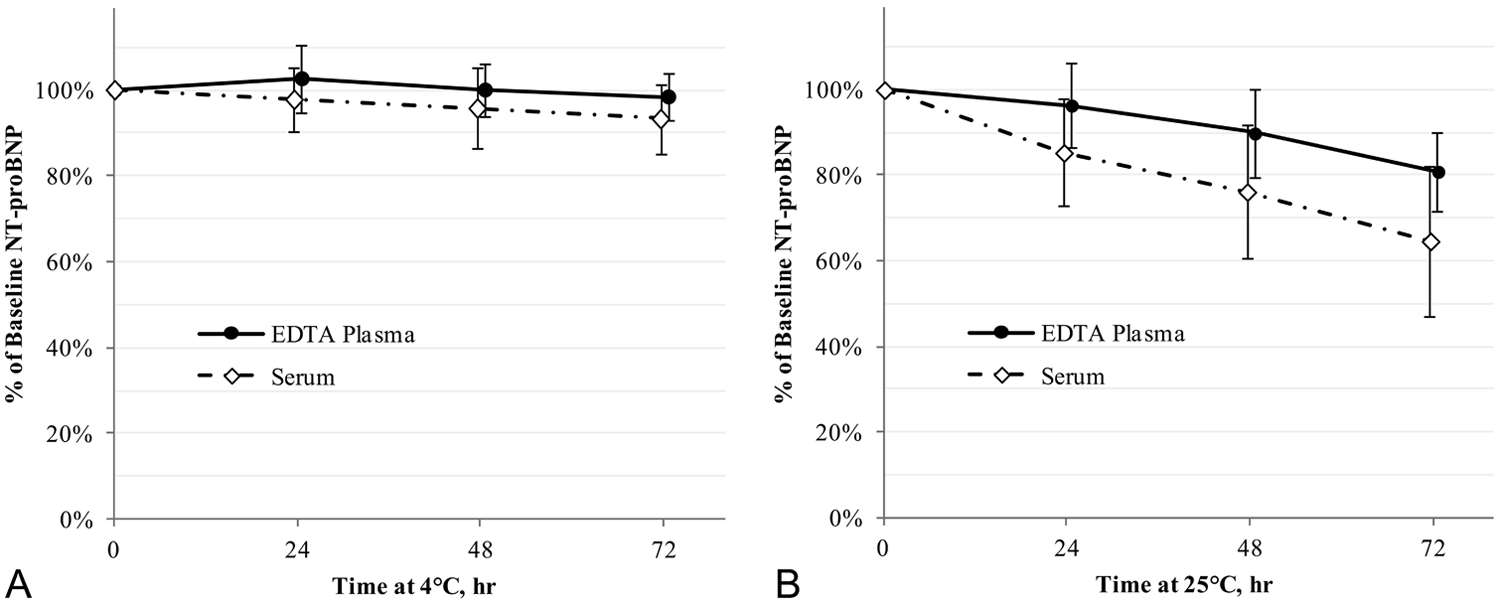
Stability of N-terminal pro–B-type natriuretic peptide (NT-proBNP) over 72 hr in ethylenediamine tetra-acetic acid (EDTA) plasma and serum samples (n = 40) when stored at (
Discussion
A previous first-generation assay for canine NT-proBNP utilized 2 sheep anti-canine NT-proBNP polyclonal antibodies that detected epitopes in serum or plasma with limited room temperature stability. This resulted in the need for special handling of the samples during transport from the veterinary clinic to the reference laboratory. The sample was required to be either kept frozen or transferred to a special protease inhibitor tube during transport in order to preserve the integrity of the sample and ensure an accurate result. Furthermore, because the assay used 2 sheep antibodies, samples could produce false elevated results in the absence of NT-proBNP due to the presence of anti-sheep immunoglobulin G heterophilic antibodies. Such antibodies have been identified in canine samples and reported in the literature to interfere in this manner with similar assays. 13 The second-generation assay utilizes 2 unique anti-canine NT-proBNP antibodies that are specific to distinct epitopes of canine NT-proBNP. These antibodies recognize different epitopes in a more stable region 18 of the NT-proBNP molecule compared with the antibody pair used in the first-generation assay. The change in epitope recognition eliminates the need for the protease inhibitor tube. In addition, the 2 antibodies utilized in the second-generation assay originate from different host species, which minimizes the risk of interference due to heterophilic antibodies.
The first-generation NT-proBNP assay also offered insufficient dynamic range (50–3,000 pmol/l) to measure NT-proBNP across the full range of biological variability found in dogs with heart disease. Studies have demonstrated that NT-proBNP concentration can be an indicator for first onset of congestive heart failure in dogs with mitral valve disease and may provide prognostic information on survival. A previous study 11 showed that small breed dogs with mitral valve disease and NT-proBNP of >1,500 pmol/l were at increased risk of entering congestive heart failure within the next 12 months. That study utilized the first-generation assay for measuring NT-proBNP, and the authors noted the inability to fully evaluate risk stratification for dogs with severe mitral valve disease due to the assay’s limited dynamic range. The improved, second-generation assay described in the current study has an upper reporting limit of 10,000 pmol/l, which enables more granular stratification of risk for congestive heart failure within the next 12 months and allows prediction of occurrence within 3 or 6 months, compared with 12 months. The extended dynamic range of the second-generation assay also offers more potential to support studies evaluating the utility of NT-proBNP for monitoring of disease progression and response to drug therapy. 17
In addition to the expanded dynamic range, the second-generation assay provides the benefit of sample stability without the need for frozen storage or use of a protease inhibitor tube. EDTA plasma and serum sample types produce equivalent results with limitations. At time of blood draw, there is no significant bias in the NT-proBNP concentration measured between sample types. However, a difference in NT-proBNP stability is observed between the sample types, especially at room temperature. EDTA plasma samples were shown to retain ≥98% of baseline NT-proBNP concentration after 72 hr of storage at 4°C. Serum samples retained ≥93% of baseline NT-proBNP concentration after 72 hr of storage at 4°C. When stored at 25°C, EDTA plasma retained, on average, 96% of baseline after 24 hr, 90% after 48 hr, and 81% after 72 hr. Serum stored at 25°C retained, on average, 85% of baseline after 24 hr, 76% after 48 hr, and 65% after 72 hr. It should be noted that these sample integrity studies were conducted under controlled environmental conditions. Data has not been generated to evaluate NT-proBNP integrity at temperatures >25°C to which samples may be exposed during ambient shipping in warmer climates. Ideally, ambient EDTA plasma samples should be transported to the reference lab within 48 hr. It is recommended that serum samples are shipped on ice packs, which will keep the samples cold until receipt at the lab. However, should the shipment be delayed and the cold packs thaw, it is possible that the NT-proBNP concentration measured in the serum sample may be decreased.
The observed difference in room temperature stability between EDTA plasma and serum is most likely related to the role of EDTA as a protease inhibitor. EDTA functions as an anticoagulant by chelating calcium and hence inhibiting proteases (trypsins) involved in the clotting cascade and could offer secondary inhibition of proteases involved in NT-proBNP degradation, extending the amount of time that circulating NT-proBNP can be measured. In serum samples, no EDTA is present, and the cleavage of the NT-proBNP molecule may be hastened by proteases that are activated during the clotting cascade as well as other proteases that would otherwise be inhibited in the presence of EDTA.
Ethyylenediamine tetra-acetic acid plasma samples were used to compare performance between the first- and second-generation assays. Based on a population of 168 samples, Bland–Altman analysis resulted in no statistically significant bias between the 2 assays, indicating that the clinical decision points established for the first-generation assay remain valid for the second-generation assay. Despite the absence of a statistical difference between the 2 assays, method differences may be observed for a small number of individual dogs. NT-proBNP concentrations for individual dogs may differ when comparing results from the first- and second-generation assays. The within-individual method differences are most likely due to biochemical modifications of the peptide that affect the availability of epitopes (increased or decreased) targeted by the different antibodies used in each assay generation. Whenever an immunoassay for peptide markers such as NT-proBNP is redesigned, there is rarely a 1-to-1 relationship for all individuals when testing a sample on old and new assays. In cases where dogs are being tested for NT-proBNP concentration over time, a shift in results may be observed when transitioning between the first- and second-generation assays. Therefore, it will be important to establish a new baseline value for any dogs with previous results generated on the first-generation assay.
The second-generation assay demonstrates accurate and precise measurement of canine NT-proBNP and, in combination with the extended dynamic range, will better support the long-term monitoring of NT-proBNP to assess disease progression or evaluate response to treatment. However, when using the assay to monitor changes in NT-proBNP over time, it is recommended that practitioners always submit the same sample type due to differences observed in room-temperature stability between EDTA plasma and serum.
The validation data described in the current study demonstrates that the second-generation assay has marked improvements compared to the first-generation canine Cardiopet® proBNP assay with extended dynamic range and compatibility with routine EDTA plasma and serum sample types. These enhancements increase the utility of NT-proBNP as a cardiac biomarker in veterinary medicine, especially for prognostic applications, and make the assay easier to implement in a clinical setting.
Footnotes
Acknowledgements
The authors thank Dr. John MacGregor, Portland Veterinary Specialists, Portland, ME, and Dr. Steve Rosenthal, Chesapeake Valley Cardiology Associates, Towson, MD.
a.
Canine Cardiopet® proBNP test kit, IDEXX Laboratories Inc., Westbrook, ME.
b.
Excel, Microsoft Corp., Redmond, WA.
c.
Analyse-it Software Ltd., Leeds, United Kingdom.
d.
JMP 10, SAS Institute Inc., Cary, NC.
e.
Bovine hemoglobin, Sigma-Aldrich, St. Louis, MO.
f.
Ditaurobilirubin disodium salt, JBL Scientific, San Luis Obispo, CA.
g.
Intralipid 30% IV solution, VWR International, Radnor, PA.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors are employees of IDEXX Laboratories Inc., Westbrook, Maine.
Funding
The author(s) received no financial support for research, authorship, and/or publication of this article.