
Abstract
A 21-day-old Thoroughbred colt was euthanized following a history of recurrent colic. A 4.5 cm in diameter, occlusive, submucosal cyst was identified in the duodenum at necropsy. Histologically, the cyst was surrounded by a smooth muscle wall and was lined by both squamous and attenuated cuboidal to columnar epithelium. A diagnosis of an esophageal cyst was made based on the gross and histologic findings.
Congenital foregut malformations (CFMs) are a broad group of rare embryologic developmental anomalies that may manifest as organ agenesis, atresia, or fistulation; tubular duplications; or cysts of foregut derivation.14,19 Cystic malformations can be closely associated with any portion of the alimentary or respiratory tracts, or can be indiscriminately isolated in the mediastinum, retroperitoneal connective tissue, or various internal organs.5,9,19
A 21-day-old male Thoroughbred foal was submitted to the University of Kentucky Veterinary Diagnostic Laboratory (Lexington, Kentucky) for necropsy. The foal had a history of recurrent colic. At 6 days of age, the foal underwent colic surgery for an intact mesodiverticular band that had resulted in small intestinal compromise. Thirteen days following surgery, the foal again developed colic, and duodenal distension was identified by ultrasonography. The owner declined further treatment, and the foal was euthanized.
A 72.6-kg foal was submitted for necropsy in good body condition and fair postmortem preservation. The duodenum was completely occluded by a well-demarcated, taut, 4.5 cm in diameter, fluid-filled, unilocular, submucosal cyst that was located 5 cm from the pyloric sphincter (Fig. 1). The occlusive exterior surface of the cyst was lined by normal small intestinal mucosa, and the interior cystic surface was smooth, pink, and shiny. Approximately 40 ml of nonviscous white cloudy fluid filled the cyst lumen. There was no evidence of communication between the cyst and the intestinal lumen, the duodenal papillae, or the bile duct. The seromuscular layer of the cyst was continuous with the adjacent duodenum. Additionally, a marked amount of ingesta distended the stomach and proximal duodenum cranial to the cyst, and multifocal small variably sized and shaped ulcers were located in the squamous mucosa of the stomach. The small intestine distal to the cyst lacked content; no other abnormalities were evident. Sections of the cyst and other major organs were placed in phosphate buffered 10% formalin, allowed to fix for 24 hr, routinely processed, and stained with Harris hematoxylin and eosin for microscopic evaluation.
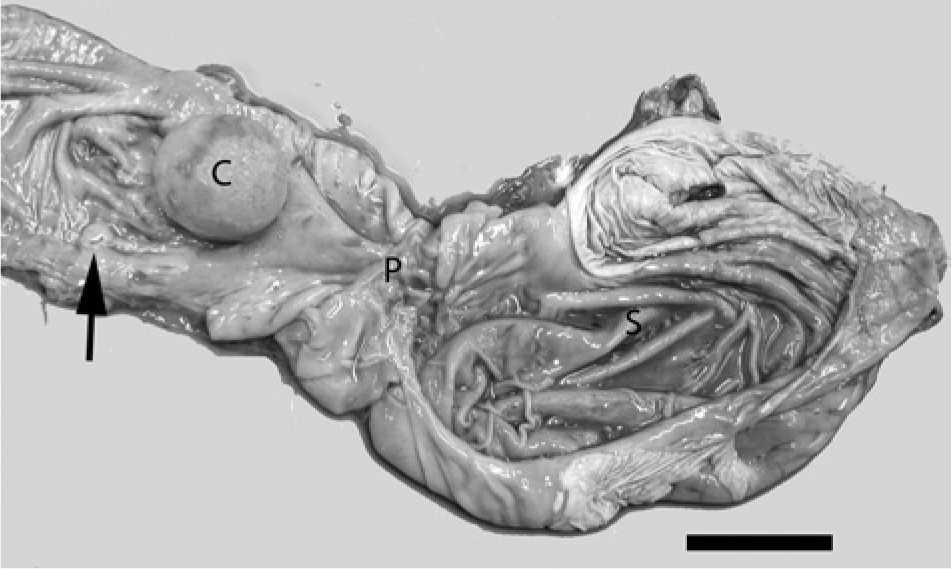
Stomach and duodenum; equine. A well-demarcated spherical cyst (C) elevates the mucosa and obstructs the proximal duodenum. The cyst is located in close proximity to the pyloric sphincter (P) and the major duodenal papilla (arrow). S = stomach. Bar = 5 cm.
Histologically, a well-demarcated cyst extended from the deep submucosa to the tunica muscularis (Fig. 2). The interior cyst wall was lined by simple attenuated cuboidal to columnar epithelium (Fig. 3A) and stratified squamous epithelium (Fig. 3B). A moderate smooth muscle wall surrounded the cyst. Duodenal mucosa superjacent to the cyst was distorted, lost, and multifocally replaced by a small amount of fibrous connective tissue. Within distorted areas, small intestinal villi were rarely evident; there were decreased numbers of crypts; and the fibrous connective tissue and lamina propria were infiltrated by low numbers of lymphocytes, plasma cells, and macrophages. Gastric ulceration was histologically confirmed in the squamous mucosa.
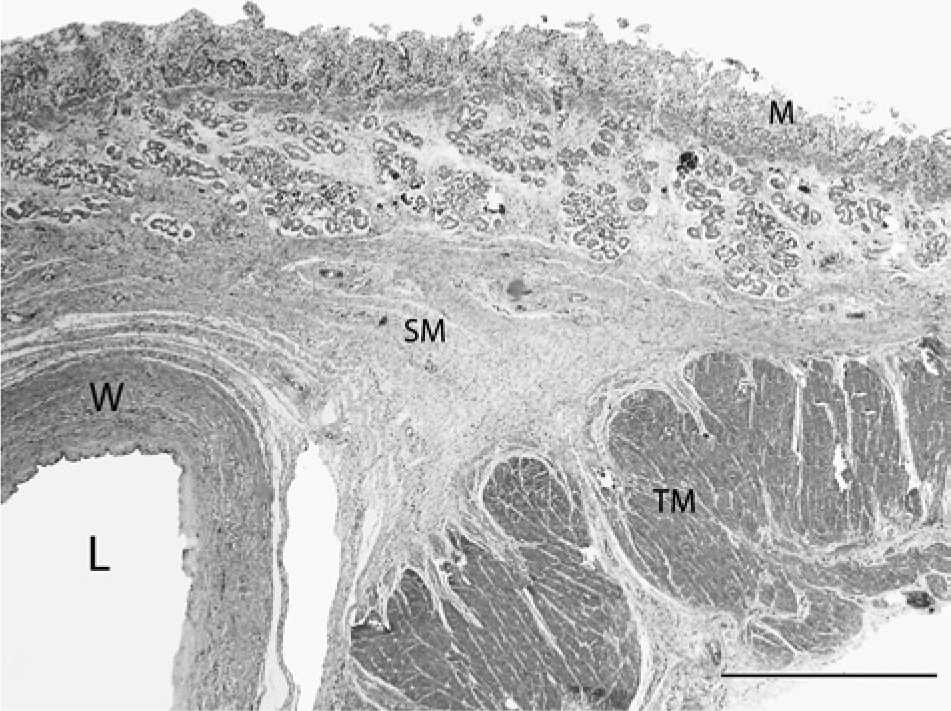
Duodenum; equine. A well-demarcated cyst expands the deep submucosa (SM). L = lumen; W = cyst wall; M = mucosa; TM = tunica muscularis. Hematoxylin and eosin. Bar = 1 mm.
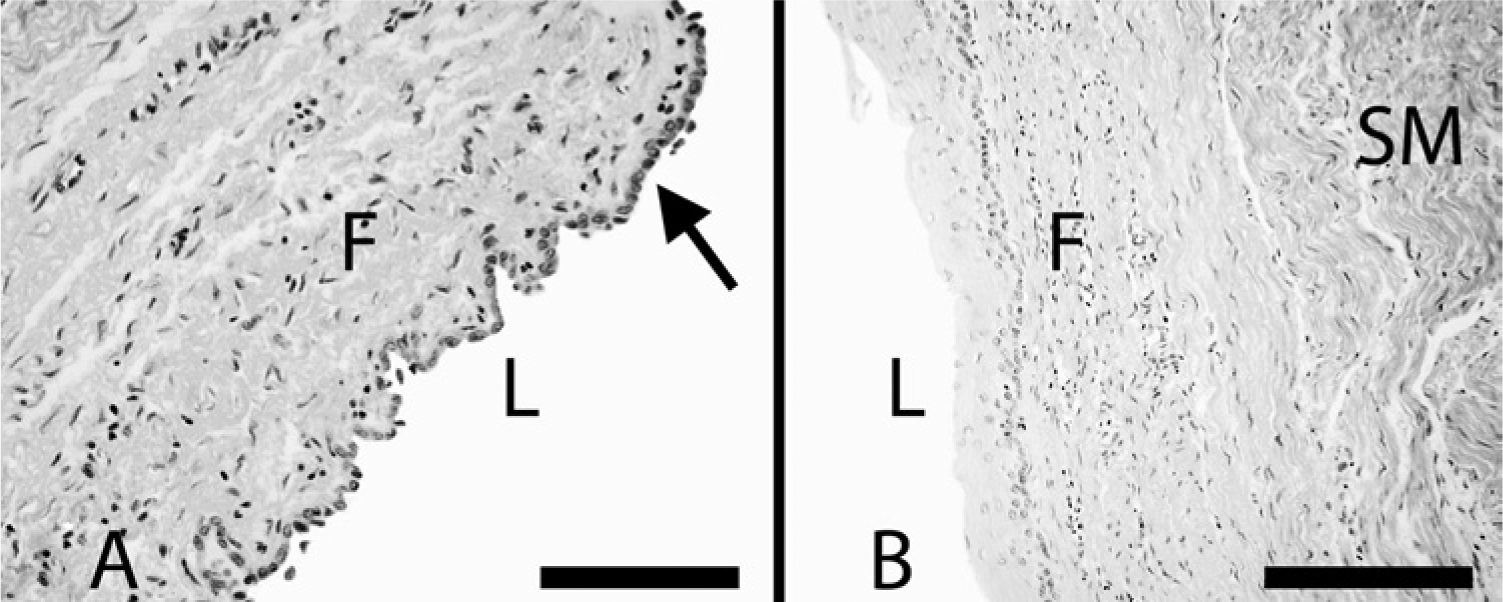
Esophageal cyst; equine. The cyst is lined by simple cuboidal, attenuated, and stratified squamous epithelium that is supported by a subepithelial layer of fibrous connective tissue (F) and an outer layer of smooth muscle (SM). L = lumen.
An esophageal cyst was diagnosed based on the foregut cystic malformation algorithm proposed by Gómez Mateo et al. 8 This histologic algorithm categorizes 6 different foregut cysts (ciliated foregut, bronchogenic, esophageal, gastric, enteric, or enterogastric) based on features of the cyst wall and epithelial lining. Cysts with a smooth muscle wall include enteric, enterogastric, esophageal, and gastric cysts; cysts with wall features of cartilage, with or without respiratory glands and smooth muscle, are classified as bronchogenic cysts; and cysts that lack cartilage or smooth muscle are categorized as ciliated foregut cysts. Additionally, ciliated foregut and bronchogenic cysts are lined by ciliated epithelium that may or may not be associated with goblet cells; esophageal cysts are lined by squamous, columnar, mixed squamous and columnar, or ciliated epithelium with or without goblet cells. Gastric, enteric, and enterogastric cysts are lined by normal gastric, enteric, or mixed gastric and enteric mucosal epithelium, respectively.
The nomenclature proposed by Gómez Mateo et al. was utilized because of inconsistencies with naming cystic foregut malformations in the medical literature.5,8,19 Traditionally, foregut malformations have been named based on various embryologic, anatomic, pathologic, and surgical parameters. 19 This has led to erratic and frequently inappropriate diagnoses that confound the true incidence of these malformations in the medical literature. 19 Terminology inconsistencies are particularly evident as they pertain to isolated cystic CFM, because these can be located in various locations and can be lined by any type of endodermally derived foregut epithelium. Some of the terms used in the literature to describe cystic CFM have included the following: bronchogenic cysts, bronchogenic foregut cystic malformations, bronchopulmonary foregut malformations, choristomas, congenital duplication cysts, cysts of foregut origins, cysts with intestinal epithelium, cystic duplications, duplication cysts, enteric cysts, enterocystomas, epithelial cysts, esophageal cysts, esophageal duplication cysts, foregut cysts, foregut duplications, gastric cysts, gastrointestinal cysts, and neurenteric cysts. 19
The current case was a diagnostic challenge because of the unique location and epithelial lining of the cyst and because of nomenclature inconsistencies. Initial differential diagnoses included choledochal cyst, accessory pancreatic duct cyst, and enteric duplication cyst. Both choledochal and accessory pancreatic duct cysts were excluded because of the lack of communication with the bile and accessory pancreatic ducts, respectively. The cyst could have been misdiagnosed as a number of previously referenced foregut cystic malformations based on the location and gross pathological characteristics. However, the presence of a smooth muscle wall and mixed squamous and columnar epithelial lining are consistent with a diagnosis of an esophageal cyst located in the duodenum.
The mechanism by which CFMs develop has not been elucidated, but a number of potential theories have been proposed. 19 The endoderm is the innermost embryonic germinal layer formed during gastrulation and is responsible for the development of epithelium associated with the pancreas, alimentary and respiratory tracts, yolk sac, allantois, mandibular and sublingual salivary glands, liver, urogenital sinus, thyroid, middle ear, thymic stroma, and parathyroid gland. 12 Disruption of spatial placement and endodermal organogenesis within the developing embryo may theoretically result in a number of congenital anomalies. 12
Cystic CFMs have been described in cats, cattle, dogs, horses, and monkeys.1-4,6,7,10,11,13-18,20 These malformations have been identified in various locations, have a wide range of wall features and epithelial linings, and have been named by various denominations (Table 1). The esophageal cyst, in the foal reported herein, differed from those previously described in the veterinary literature in that the cyst was located in the duodenum and the cyst was lined by mixed squamous and simple cuboidal to columnar epithelium. Similar to most equine cases, the foal in the current report developed clinical signs associated with alimentary tract occlusion.
Cystic congenital foregut malformations reported in the veterinary literature.
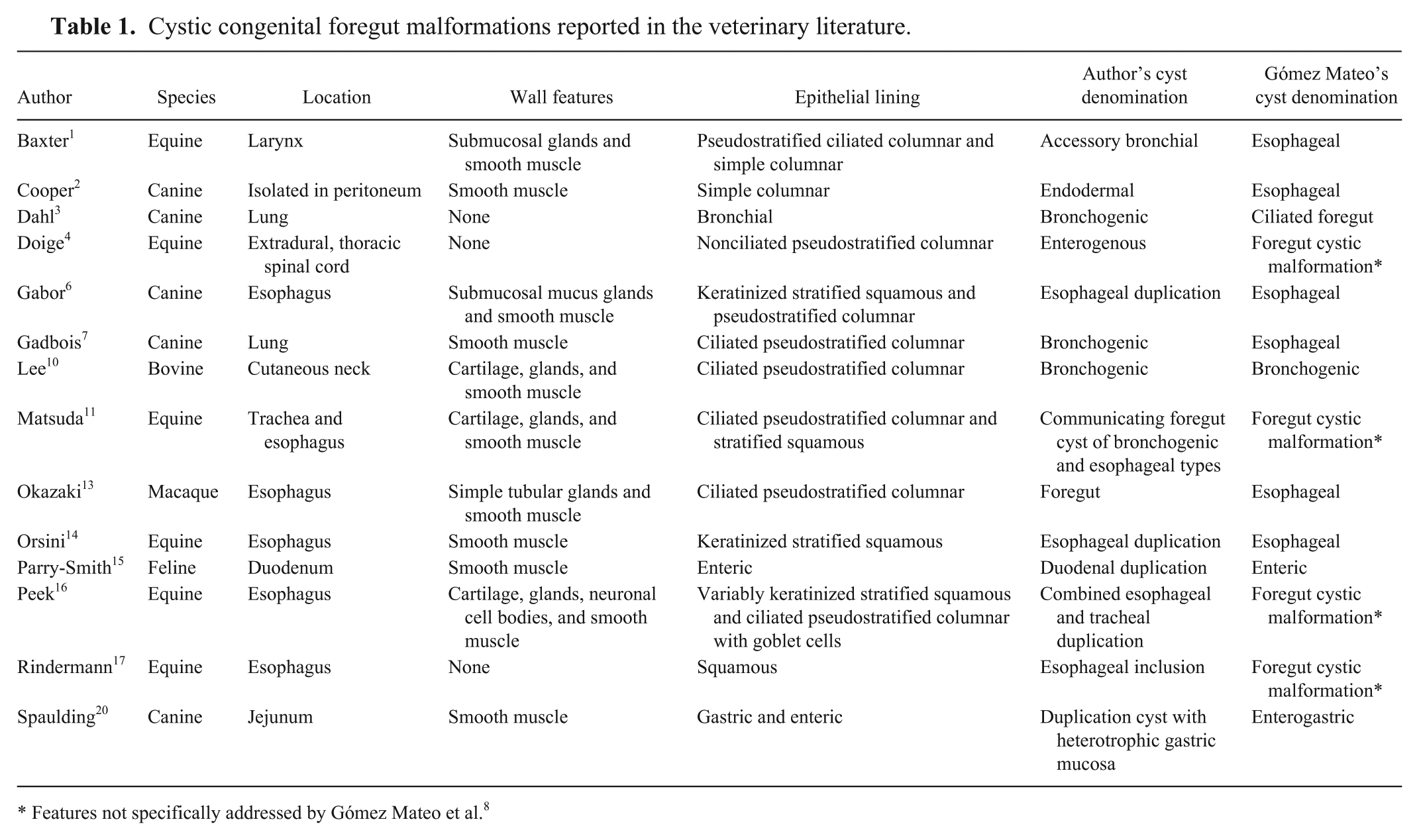
Features not specifically addressed by Gómez Mateo et al. 8
A cystic CFM should be considered as a differential diagnosis in foals with a cystic lesion within the alimentary tract or other internal organs. Histologic features of the cyst wall and epithelial lining should be utilized to assure a precise diagnosis is made to help identify the true prevalence of these rare developmental anomalies.
Footnotes
Acknowledgements
The author thanks Dr. Neil Williams for critical review of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.