
Abstract
Total serum bilirubin (TBIL) is used as a prognostic factor in chronic hepatitis (CH) in human beings. To date, the authors are unaware of any studies looking at the value of TBIL as a prognostic factor in idiopathic canine CH. The objective of the current study was to assess if TBIL is a negative prognostic factor in idiopathic canine CH, and to identify other prognostic factors. Thirty-nine dogs with histologically confirmed idiopathic CH admitted to 2 referral centers between 1999 and 2010 were included in the study. Patients with concurrent diseases that could affect TBIL or the survival time were excluded. Total serum bilirubin was measured prior to liver biopsy, and CH was diagnosed according to standardized histological criteria. Survival time was calculated from time of diagnosis to time of death or euthanasia. Cox proportional hazard analysis was performed to identify prognostic factors. The mean survival time for the 39 dogs included in the analysis was 197 days (1–2,677), and the mean total serum bilirubin was 11 μmol/l (2–265). Total serum bilirubin was statistically significantly associated with survival (odds ratio = 1.082, P = 0.047) as were weight (odds ratio = 1.028, P = 0.028) and the presence of ascites (odds ratio = 6.758, P = 0.013). The current study demonstrates that TBIL could be used as an additional prognostic factor in canine CH.
Introduction
Chronic hepatitis (CH) is the most common liver disease in dogs 41 and is defined histologically by the presence of hepatocellular apoptosis or necrosis, a variable mononuclear or mixed inflammatory cell infiltrate, regeneration, and fibrosis. 36 Although immune-mediated mechanisms, 23 infectious diseases,1,5,26 or metabolic disorders, including copper accumulation,14,27 have been associated with the development of CH in dogs, the etiology remains idiopathic in the majority of the cases.3,24,32,39
Abdominal ultrasonography and hepatic cytology can help to exclude other causes for the presenting clinical signs and the raised hepatobiliary enzymes, but such tests lack specificity and sensitivity for diagnosis of idiopathic CH.10,13,37,38 Hence, definitive diagnosis is made on histology of hepatic biopsies. 9 Treatment is supportive and nonspecific as the cause is usually unknown. A wide variety of treatments have been proposed15,39 but, to date, there are no prospective studies to determine the most effective treatment in dogs with idiopathic CH.
The prognosis of canine CH is variable, and, as in human CH, likely depends on the underlying etiology.2,19 Ascites has been found to be a negative prognostic indicator in canine idiopathic CH 25 as well as other factors such as anorexia and hypoglobulinemia, 30 presence of cirrhosis on histology,24,33 and hypoalbuminemia and a left shift leukogram. 24 In human beings, total serum bilirubin (TBIL) has been found to be an independent negative prognostic indicator in CH due to a variety of etiologies,16,18,21 and it is currently used to predict survival in human beings with end-stage liver disease.7,17
Hyperbilirubinemia can occur due to prehepatic (usually hemolysis), posthepatic (due to obstructive or functional cholestasis), or hepatic causes. Hyperbilirubinemia in hepatic disease is caused by decreased uptake of unconjugated bilirubin and/or decreased conjugation by the hepatocytes. 28 Therefore, hyperbilirubinemia is usually associated with a severely impaired hepatic function.
Total serum bilirubin was not correlated with prognosis in a population of Labrador Retrievers, 30 and the presence of jaundice was found to negatively affect survival in dogs with primary hepatitis, either acute and chronic. 24 Total serum bilirubin has not been evaluated as a prognostic factor in other breed of dogs with idiopathic CH. The aim of this retrospective study was to assess whether raised TBIL was a negative prognostic indicator in idiopathic canine CH.
Materials and methods
Dogs with histologically confirmed CH were included in the study. The cases were selected from 2 different referral centers (center A: Department of Veterinary Medicine, University of Cambridge, Cambridge, United Kingdom; and center B: Dick White Referrals, Six Mile Bottom, United Kingdom) between January 1999 and December 2010. In addition to a histological confirmation of idiopathic CH, additional inclusion criteria included 1) no evidence of concurrent pancreatitis or other disease that could cause extrahepatic biliary obstruction; and 2) no evidence of hemolysis. The presence of pancreatitis was excluded when there was no clinical suspicion (e.g., lack of vomiting, abdominal pain), the pancreas had a normal ultrasonographic appearance, and/or pancreatic lipase immunoreactivity was within the reference interval. Dogs that underwent postmortem examination and had pancreatitis confirmed histologically were excluded from the study. Extrahepatic biliary obstruction was excluded by abdominal ultrasound 6 and/or exploratory laparotomy or laparoscopy. The absence of hemolysis was based on a normal hematocrit (i.e., >0.35 l/l) and a normal reticulocyte count. None of the serum samples used for measurement of TBIL was hemolyzed. In addition, dogs that had a severe concurrent illness at the time of diagnosis (e.g., malignant neoplasia or other diseases that could affect the survival time) or dogs that died due to unknown or liver-unrelated causes were also excluded from the study.
Data was obtained from the medical records and included signalment, clinical signs, physical examination findings, laboratory findings (including complete blood cell count and serum biochemistry), results of diagnostic imaging, and histology. In all cases, the concentration of TBIL was obtained within 1 week prior to liver biopsy, and the date of blood sampling was considered day 0 when calculating the survival time. Serum biochemistry was performed using 2 different automated chemistry analyzers (Beckman CX5 a in center A from January 1999 to January 2009; and Olympus AU400 b in center B during the entire study period and in center A since February 2009). To adjust for the different reference intervals between automated analyzers, the absolute values for TBIL were divided by the value corresponding to the upper limit of the reference interval. A value of 1 indicated that the parameter was within the reference interval, whereas a value of >1 indicated an elevation in the parameter. The same calculation was applied to alanine transaminase (ALT) and alkaline phosphatase (ALP) values. For the serum albumin, the same calculation was performed but the lower end of the normal range was divided by the absolute value of the albumin. A value of 1 indicated that the albumin was within the reference interval, whereas a value of >1 indicated a decrease in the parameter (i.e., the higher the relative value, the lower the albumin level). None of the cases included in the present study had an increased serum albumin. The date of death and cause of death were obtained from the clinical records or via telephone conversation with the referring veterinary center. Dogs that were lost to follow up were excluded from the study.
Liver biopsies were performed under general anesthesia either surgically (laparoscopy or laparotomy), by ultrasound-guided percutaneous Tru-cut–like (needle size was <16 gauge in all cases), or at postmortem examination. The biopsy method was elected by the attending clinician. Idiopathic CH was diagnosed according to standardized histological criteria devised by the World Small Animal Veterinary Association’s Liver Standardization Group. 36 Rubeanic acid or rhodanine stains were requested in all cases. For these cases, the previously published semiquantitative scoring system 30 was used. All tissues were scored as 0 (absence or rare copper-positive cells), 1 (few random copper-positive cells), 2 (moderate numbers of copper-positive cells) and 3 (many copper positive cells in all zones). Patients with score ≥2 of copper were excluded from the study. Leptospira titers (by microscopic agglutination test and performing convalescence titers 14 days thereafter) were performed in cases where there was a clinical suspicion of leptospirosis (e.g., acute onset of clinical signs, rural environment), vaccination status was unknown, and where there was a history of exposure. Only dogs in which all these tests were negative were included in the study.
The survival time was calculated from the time of blood sampling until the time of euthanasia or death. A multivariate analysis using Cox proportional hazard analysis was also performed to look for variables that could contribute to the prognosis. The relative values were used for the serum albumin, ALT, ALP, and TBIL. A cutoff value of 30 days was chosen to differentiate between short- and long-term survivors as it has been previously used as a cutoff indicative of short survival time in dogs with idiopathic CH.6,33 All of the statistical calculations were performed using commercial statistical software. c
Results
Eighty-two cases were diagnosed with CH on histology in 2 centers in the study period, but 43 dogs were excluded as they did not meet the inclusion criteria (10/43 had concurrent pancreatitis, 7/43 had severe concurrent disease in another organ, 1/43 had concurrent hemolytic anemia, 5/43 were lost to follow up, 6/43 had incomplete clinical data, 6/43 were diagnosed with copper storage disease, 5/43 died of causes other than liver disease, and for 5/43 the cause of death was unknown). Of the 39 dogs included in the study, 22 were females (15 neutered and 7 entire) and 17 were males (11 neutered and 6 entire) with a median age of 7 years (range: 17 months–13 years). The median bodyweight was 23.2 kg (range: 7–91 kg). Nineteen different breeds were represented, with Labrador Retrievers (10/39), English Springer Spaniels (6/39), and English Cocker Spaniels (4/39) being overrepresented. Other breeds included fewer than 3 dogs each.
Clinical signs included lethargy (19/39), anorexia (6/39), ascites (12/39), vomiting (12/39), jaundice (10/39), polyuria and polydipsia (9/39), weight loss (4/39), diarrhea (5/39), and melena (1/39). Four dogs presented with no clinical signs, and liver disease was suspected on the basis of raised hepatobiliary enzymes on serum biochemistry performed as a general health screening prior to a general anesthesia for a routine procedure.
An overview of the TBIL, hepatobiliary enzymes, and the serum albumin concentration for the study group is summarized in Table 1 and Figure 1. The median of the relative and absolute TBIL values was 1.0 (range: 1.0–22.1) and 0.64 mg/dl (range: 0.12–15.50 mg/dl), respectively. Twelve out of 39 dogs (31%) had an elevated TBIL. Thirty-three dogs (85%) had both an elevated ALT and ALP. One dog had normal hepatobiliary enzyme values and presented with ascites as the only clinical sign.
Relative and absolute values of the cases included in the current study (n = 39).*
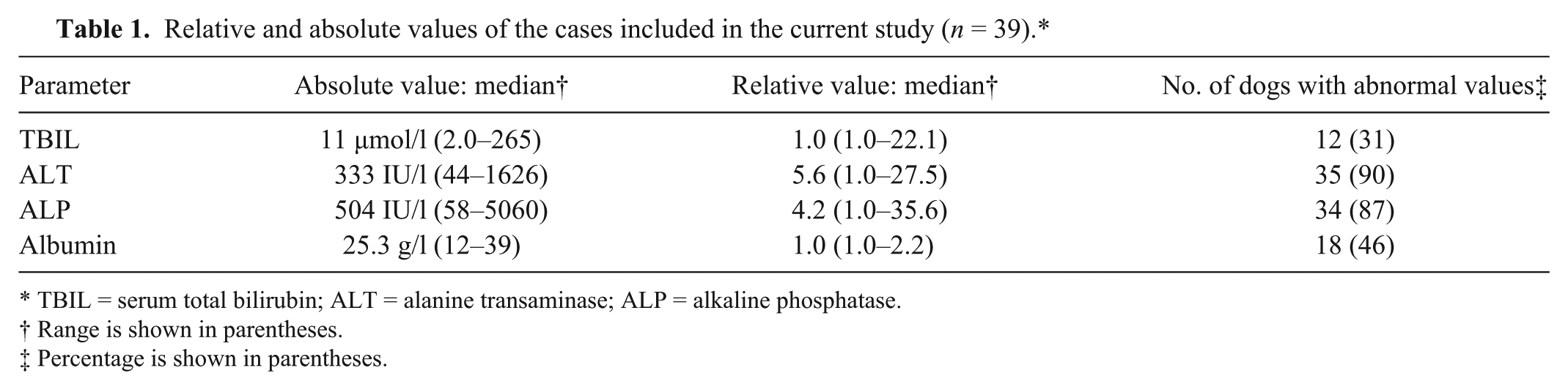
TBIL = serum total bilirubin; ALT = alanine transaminase; ALP = alkaline phosphatase.
Range is shown in parentheses.
Percentage is shown in parentheses.
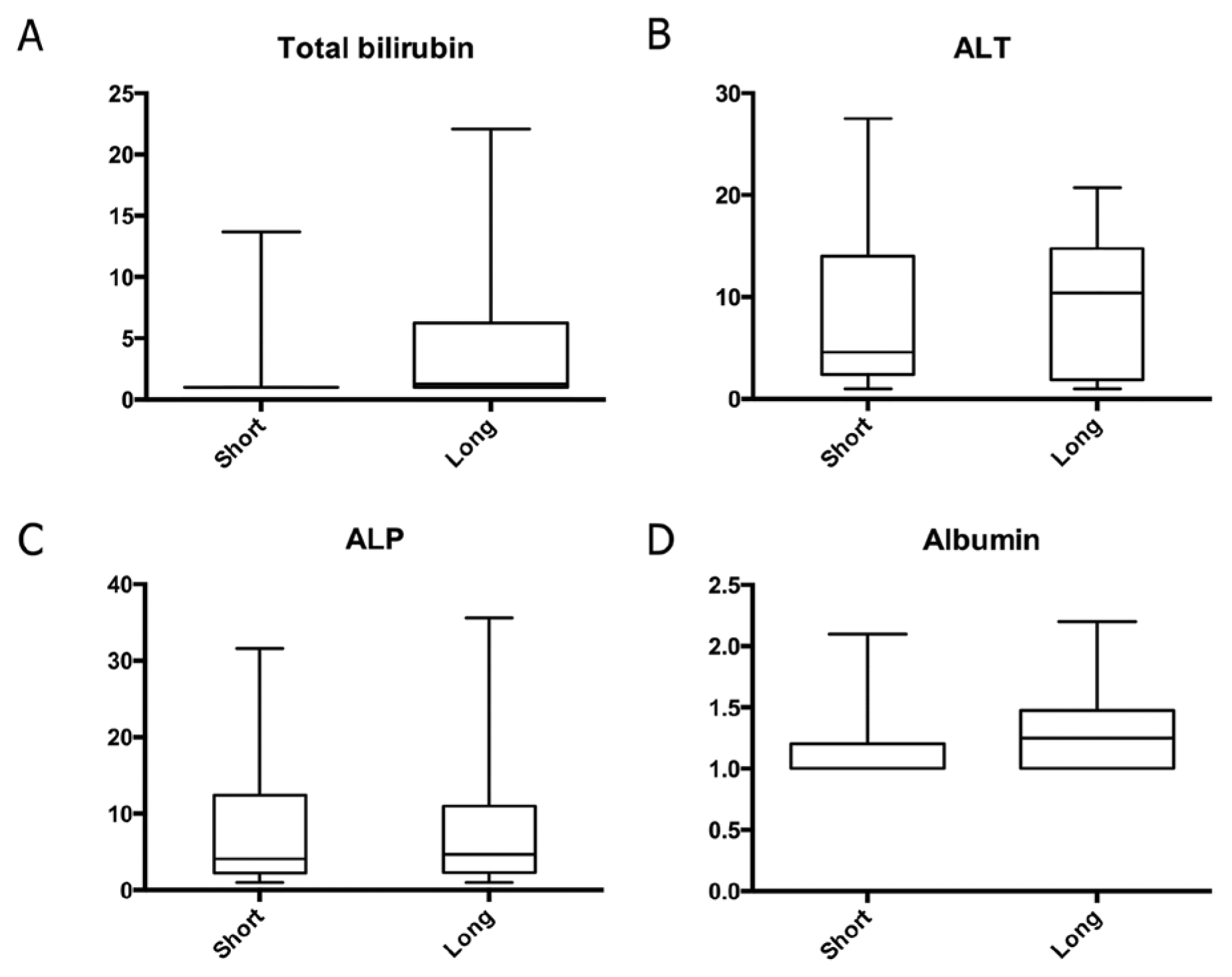
Whisker and box plot of the relative values (y axis) for the total bilirubin (TBIL;
Abdominal ultrasound was performed in all dogs by, or under the supervision of, a board-certified diagnostic imager. There were visible acquired multiple portosystemic shunts in 4 dogs of which 3 presented with ascites. Liver biopsies were obtained from all dogs by ultrasound-guided Tru-cut–like (12 dogs), by laparoscopy (13 dogs), and by laparotomy (13 dogs). In 1 dog, biopsies were taken at postmortem examination. Bile or liver culture or both were performed in 5 dogs, including the only dog where Leptospira titers were requested, and all the results were negative. Leptospira titers were normal for the serovars analyzed in that single dog. Rubeanic acid or rhodanine stains for copper accumulation assessment were performed in all cases, and only those cases with no evidence of copper storage disease were included in the study.
The dogs included in the current study received a wide variety of treatments depending on the clinician preference, and the presence or absence of clinical signs indicative of either hepatic encephalopathy or portal hypertension. Most of the treatments were started once the results of the biopsies were available, and many of the patients were treated and reexamined regularly at the referring center rather than at the referral center. Hence, there was not complete information available for all the treatments that the dogs received, the length of time the treatments were administered, or the response to treatment. No standardized treatment regime was used so it was not possible to assess the effects of treatment on survival.
Six out of 39 cases were alive at the end of the study but were included in the analysis. The median survival time for the remaining 33 dogs was 128 days (range: 1–2,677 days) and the mean survival time for all dogs was 197 days (range: 1–2,677 days). The results of a Cox proportional hazard analysis are shown in Table 2. Total serum bilirubin (P = 0.047), weight (P = 0.028), and presence of ascites (P = 0.013) were found to contribute statistically significant effects on survival, with odds ratios of 1.082, 1.028, and 6.758 respectively.
Cox proportional hazard survival analysis (n = 39).*
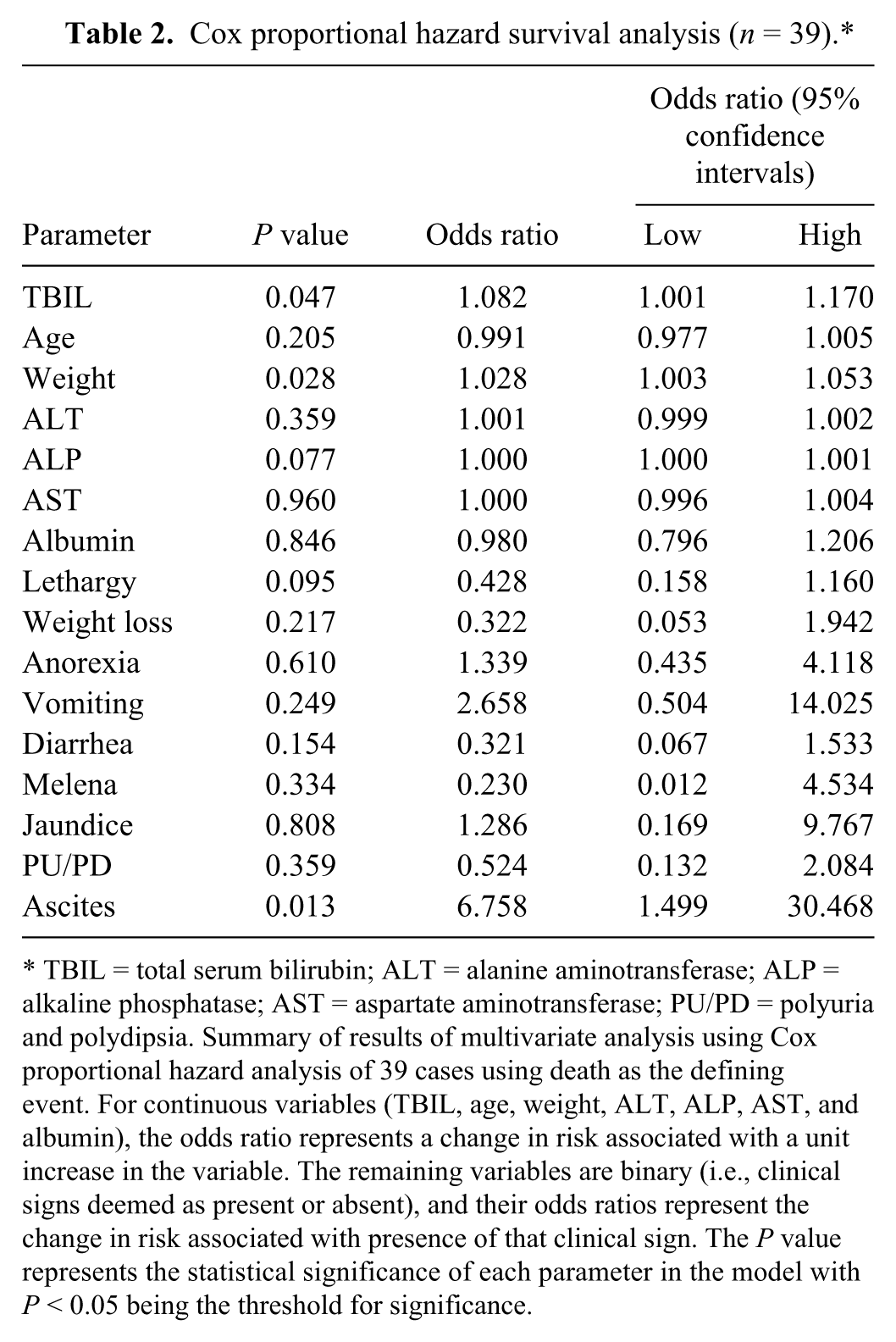
TBIL = total serum bilirubin; ALT = alanine aminotransferase; ALP = alkaline phosphatase; AST = aspartate aminotransferase; PU/PD = polyuria and polydipsia. Summary of results of multivariate analysis using Cox proportional hazard analysis of 39 cases using death as the defining event. For continuous variables (TBIL, age, weight, ALT, ALP, AST, and albumin), the odds ratio represents a change in risk associated with a unit increase in the variable. The remaining variables are binary (i.e., clinical signs deemed as present or absent), and their odds ratios represent the change in risk associated with presence of that clinical sign. The P value represents the statistical significance of each parameter in the model with P < 0.05 being the threshold for significance.
Discussion
The current study shows that TBIL is a negative prognostic indicator in dogs with idiopathic CH, similar to the situation in human beings.7,16-18,21 For every unit increase in TBIL at the time of diagnosis, there is an additional 1.082 chance of death. This could reflect decreased hepatic uptake or conjugation as would be expected in advanced liver disease. Ascites and increased weight were also found to increase the likelihood of short survival. Ascites has been described previously as a negative prognostic indicator in canine CH 25 and this was attributed to advanced liver disease and increased morbidity in patients with ascites. According to the multivariate analysis, increased weight increased the risk of death. This could be due to the effect of ascites on the weight of the patient. The multivariate analysis did not find an influence of the serum albumin levels on the survival time in this study group. This probably correlates to the ascites being caused mainly by the presence of portal hypertension in dogs with idiopathic CH rather than just hypoalbuminemia, so a direct cause–effect with the albumin is not seen.
In the dogs included in the current study, causes of pre- or posthepatic increased TBIL were excluded as much as possible to ensure that idiopathic CH was the only cause of increased TBIL in these cases. Pancreatitis is a recognized cause of posthepatic biliary obstruction8,35 and this was excluded on the basis of normal appearance of the pancreas on ultrasound examination and at laparotomy or laparoscopy where performed. It is possible that, due to the difficulty in diagnosing pancreatitis, some dogs included in the present study had concurrent pancreatitis.31,40 However, it is unlikely that pancreatitis could have significantly affected the survival time or the TBIL values in this study population if the disease was mild enough not to be detected by the diagnostic tests performed.
The cause of CH was not found in any of the dogs included in the study. Further tests were performed in some cases, when it was felt necessary by the attending clinician. Not all these tests were performed in every dog so it is possible that some dogs did not have idiopathic CH. None of the dogs included in the study had copper storage disease. Leptospira infection has been reported as a cause of CH in a colony of Beagles 1 and in a colony of American Foxhounds, 5 but the infection remains as a rare cause of CH in dogs. Most cases present with acute hepatitis and concurrent renal disease. 34 Some dogs may have had unrecognized bacterial cholangitis concurrently with CH. However, bacterial cholangitis is considered uncommon in dogs and is usually associated with visible abnormalities in the gall bladder and biliary tract on ultrasound,11,22 which were not found in cases in the current study. Most cases of CH in dogs remain idiopathic, although many possible causes have been hypothesized, including viral, autoimmune, and genetic factors. 3 Considering the wide variety of breeds included in the study, and the wide range of survival times, it is quite possible that breed-specific etiologies exist. The breeds identified in the present study were consistent with the expected breed predisposition to CH seen in the United Kingdom. 4 Total serum bilirubin may be a better prognostic indicator if individual etiologies or breeds affected with CH were isolated for statistical analysis. There were insufficient numbers in the present study to allow breed-specific analysis. Nonetheless, the survival time in the study group was similar to the survival time in a group of Labrador Retrievers 30 but TBIL was not associated with a shorter survival time. In another study, 24 the presence of jaundice was associated with a shorter survival time in dogs with primary hepatitis, both acute and chronic. However, TBIL was not measured in all the patients. The survival time of dogs with idiopathic CH was shorter than in the current study group.
Another important limitation of the present study is its retrospective nature. No information regarding length of treatment, dosages, and changes on the medication or response to treatment was available, and only the medication prescribed by the referral center at the time of discharge could be recorded. Certainly, the treatment could affect the survival time 33 but, to date, there are no prospective randomized clinical studies to confirm this. In human beings, CH is treated according to the etiology, 12 but the treatment of the canine disease remains unspecific and supportive. An additional significant confounding variable in a retrospective canine study is the decision to request euthanasia. Unlike studies in human medicine, in the current study, most liver-related deaths were due to euthanasia performed at the owners’ request. Many factors, including quality of life and financial and emotional factors can affect this decision, and time at euthanasia may not therefore represent the true “endpoint” of the disease,20,42 but this is usually the case in veterinary patients.
The change in the TBIL was unknown for several dogs included in the study. It would be interesting to evaluate this parameter over time and assess the effect of treatment or disease progression, and hypothesize if a decline in TBIL after treatment is correlated with a good response to treatment and hence survival time.
In conclusion, for this population of dogs with idiopathic CH, TBIL was found to significantly increase the risk of death. Further studies into the etiology of CH are needed so that specific treatment can be given and prognostic implications of TBIL can be assessed for individual etiologies.
Footnotes
a.
Beckman Coulter (UK) Ltd, High Wycombe, United Kingdom.
b.
Olympus Europa SE & Co. KG, Hamburg, Germany.
c.
SPSS 17.0, SPSS Inc., Chicago, IL.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.