
Abstract
A 25-year-old pregnant American Quarter Horse mare presented with a 1-week history of progressively worsening vaginal discharge. Transrectal ultrasound revealed increased thickness of the combined uterus and placenta with evidence of chorioallantoic edema but no placental separation. A thickened amnion was visible on transabdominal ultrasound. Abortion occurred 2 days after presentation despite medical treatment. At necropsy, the chorioallantois had variable but diffuse thickening with focally extensive browning of the chorionic surface in the right horn and adjacent body. There were fluid-filled sacculations on the allantoic surface of the umbilical cord, allantoamnion, and chorioallantois associated with diffuse perivascular fluid microscopically. A nonbranching acid-fast bacterium identified as belonging to the genus Mycobacterium Runyon group IV was isolated from the chorioallantois and uterine fluid. Ziehl–Neelsen stain confirmed the presence of intracellular acid-fast bacilli in trophoblasts of the gravid horn and the cervical star area. The current case is unique in that the mycobacteria did not initiate a significant granulomatous inflammatory response in the chorion unless villar necrosis occurred. Sequence analysis of the 16S ribosomal RNA gene and the rpoβ gene, encoding the β subunit of RNA polymerase, indicated that the strain of mycobacteria isolated in this case belonged to a novel species of rapidly growing mycobacteria and not to an established species. Mycobacteria are an uncommon and sporadic cause of placentitis and abortion, but should be suspected in cases of chronic placentitis that are not restricted to the cervical star area.
Placentitis is a leading cause of pregnancy loss and therefore an economic detriment to the horse industry. 8 Placentitis may cause insufficient transfer of nutrient and fetal waste products across the placenta, leading to compromised fetal growth. 23 Ascending placentitis is caused by introduction of bacteria across the cervical barrier and causes inflammation, thickening, and separation of the chorioallantois adjacent to the internal cervical os. 8 One report of reproductive loss in 3,527 Kentucky mares identifies ascending placentitis as the cause for over 30% of premature births and foal losses within the first 24 hr of life. 8 This information has been contradicted in more recent publications, as nocardioform placentitis has been identified as the most common type of placentitis in central Kentucky. 5 The most common bacterium isolated in cases of ascending placentitis is Streptococcus equi subspecies zooepidemicus, but Escherichia coli, Pseudomonas spp., and Klebsiella spp. are also implicated in high numbers.8,11 Nonascending placentitis, where inflammation is not localized to the cervical star region of the chorioallantois, is often designated as mucoid or nocardioform placentitis. Nocardioform placentitis initiates as a focus of chronic bacterial infection that is usually distributed on the body or horns of the chorioallantois. Soil-borne bacteria previously identified as causing nocardioform placentitis include Crossiella equi, 6 Amycolatopsis sp., 3 Streptomyces sp., 15 and Cellulosimicrobium cellulans. 2 Three reports of equine mycobacterial abortion have demonstrated a chronic course of disease similar to the clinical presentation of nocardioform placentitis.4,9,22 In 2 of the 3 reports, Mycobacterium avium was the causative agent.4,9 Unlike previous reports of equine mycobacterial placentitis, in the current case, a novel species of mycobacteria replicated primarily within trophoblasts and resulted in placental circulatory failure and abortion.
A 25-year-old American Quarter Horse mare at 6 months gestation was presented to the JT Vaughn Large Animal Teaching Hospital at Auburn University’s College of Veterinary Medicine (Auburn, Alabama). The chief complaint was increasing purulent vaginal discharge of 1-week duration. The mare was bred by natural cover in 2005 and delivered a full-term stillborn foal in 2006 following a minor dystocia. The mare was rebred by natural cover to the same stallion and foaled uneventfully in 2007. She was again rebred by natural cover in 2008, but this pregnancy ended with an undiagnosed abortion between 60 and 100 days. A breeding soundness exam following this loss was performed in March 2009. Cytologic analysis of the endometrium was normal. Uterine bacterial and fungal cultures were not performed. An endometrial biopsy showed slight, infrequent periglandular fibrosis, mild cystic gland distension, and very slight, chronic, diffuse inflammation consisting of lymphocytes in the stratum compactum. The sample also showed moderate to severe endometrial gland atrophy that was atypical of the season. The mare was classified as a category IIB with the modified Kenney–Doig method giving her a 10% to 50% chance of supporting a pregnancy to term. 13 The owner declined alternative reproductive options such as embryo transfer and elected to breed the mare by natural cover and allow her to carry the foal to term. The mare became pregnant following 2 attempts without veterinary intervention and was confirmed pregnant via transrectal ultrasonography at 30 days post breeding.
On presentation at approximately 180 days gestation, the general physical examination of the mare was unremarkable other than a small amount of slightly thickened, white to yellow vaginal discharge located on her tail and vulva. Transrectal ultrasound revealed an increased combined thickness of the uterus and placental tissues of 5.8 mm, indicating placental edema. 18 No evidence of placental separation was detected. The allantoic fluid appeared hypoechoic. No fetal movements were visualized by transrectal or transabdominal ultrasonography, and viability of the fetus could not be determined. A thickened band of tissue was evident adjacent to the fetus and was suspected to be the amnion. The amniotic fluid surrounding the fetus showed slightly increased echogenicity beyond what would be expected for this stage of gestation. Conservative treatment for placentitis was initiated based on the clinical signs and the thickened placental tissues. The mare was prescribed altrenogest (0.088 mg/kg orally, once daily), trimethoprim sulfadiazine (20 mg/kg orally, twice daily for 10 days), and flunixin meglumine (1.1 mg/kg intravenously, twice daily for 3 days).
Two days later, the mare aborted a single, nonviable male fetus and intact fetal membranes without complications. The fetus was stillborn with no movement or attempts to breathe following delivery. The placenta and fetus were submitted entire for necropsy. A uterine biopsy, culture, and cytology were obtained from the mare 5 days following the abortion.
The fetus had a crown rump length of 42 cm and weight of 2.1 kg (Fig. 1). The abdomen was distended by ascites, and the liver was yellow, friable, and adhered to the ventral abdominal wall (Fig. 2). The chorioallantois weighed 2.45 kg and had focally extensive thickening and brown discoloration in the right (gravid) horn and multifocal brown discoloration in the adjacent body. The left (non-gravid) horn appeared normal. The cervical star area was thickened by edema but lacked brown discoloration. The allantoic surface of the chorioallantois had diffuse perivascular fluid accumulation that often resulted in fluid-filled saculations up to 5 cm in diameter. These sacculations were largest at vessel bifurcations and were most numerous opposite the gravid horn (Fig. 3). Five areas of the chorioallantois were sampled, labeled (right pregnant horn, body adjacent to the right horn with brown exudate, left nonpregnant horn, body adjacent to the left horn, and cervical star), and submitted for microscopic examination in separate cassettes.

American Quarter Horse. Fetus and allantoic surface of the complete placenta (chorioallantois, allantoamnion, and umbilical cord) demonstrating fetal ascites, umbilical cord sacculations, amniotic edema, and perivascular sacculations on the allantoic surface of allantoamnion and chorioallantois.
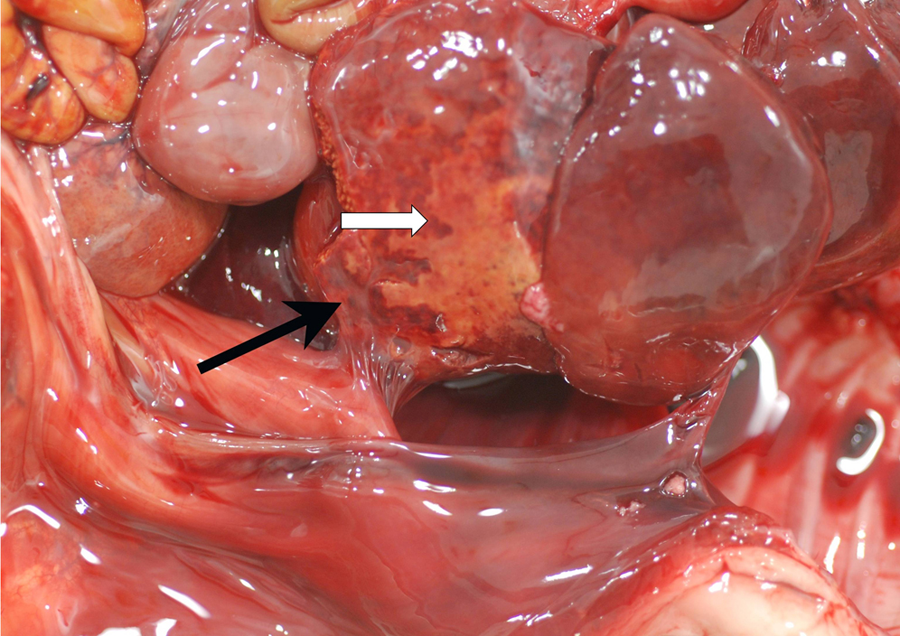
American Quarter Horse. Fetal liver demonstrating a yellow friable area of necrotizing hepatitis (white arrow) and abdominal adhesions (black arrow).
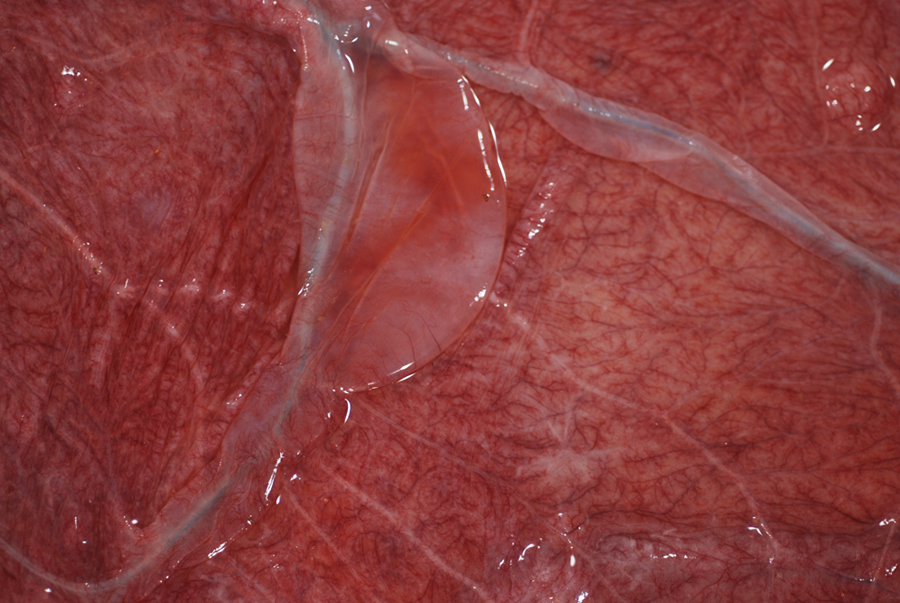
American Quarter Horse. Allantoic surface of the chorioallantois demonstrating clear fluid accumulation around vessels and fluid sacculation at a vessel bifurcation (mega allantoic vesicles).
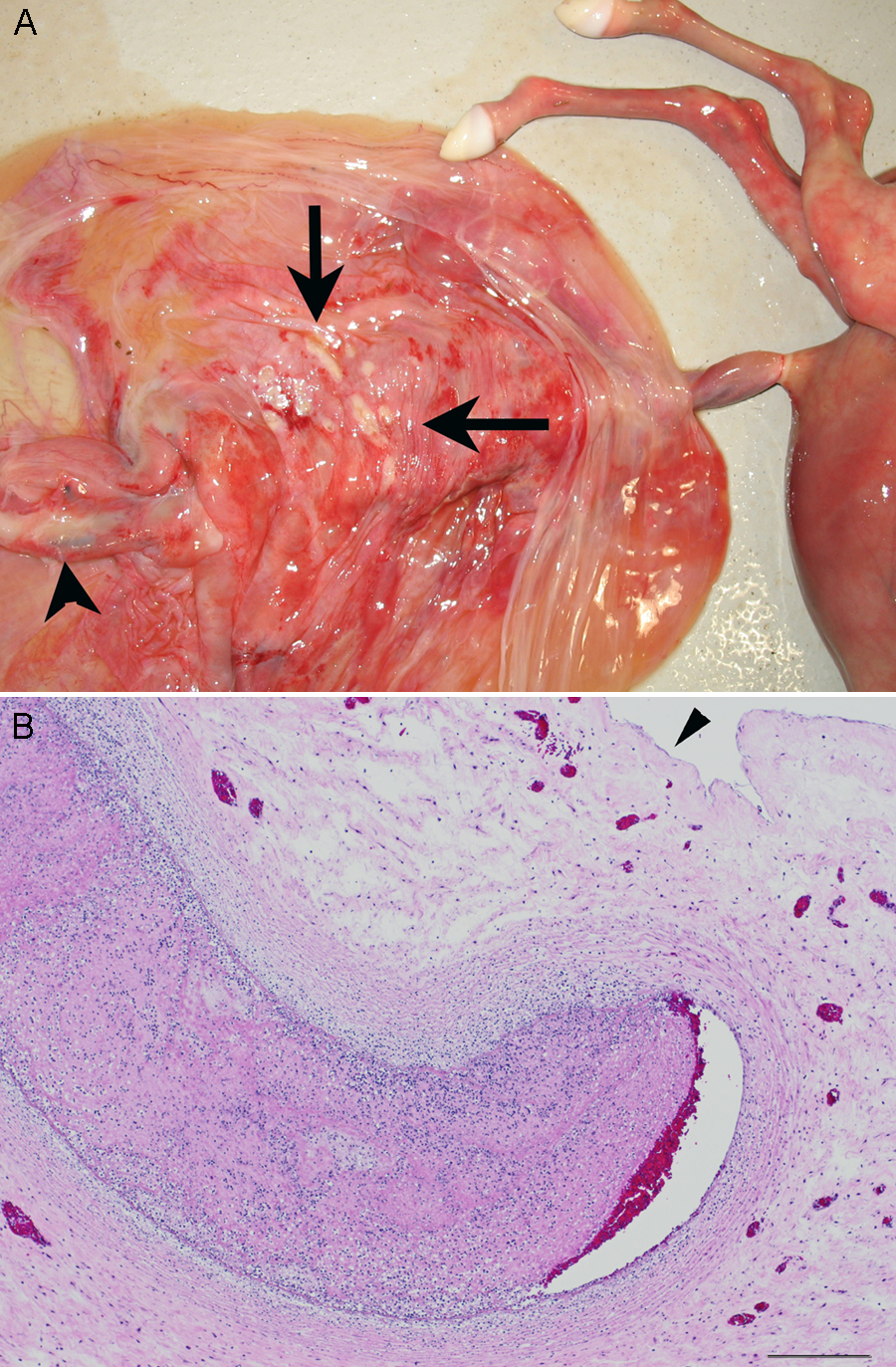
The allantoamnion and umbilical cord had a combined weight of 0.64 kg, and the total umbilical cord length was 37 cm. The umbilical cord had similar fluid-filled sacculations associated with vessels in the allantois. The allantoamnion was diffusely thickened by edema, had decreased transparency, and contained central areas of hemorrhage. The allantoic surface of the allantoamnion adjacent to the allantoic umbilical cord attachment had multifocal, irregular, 0.5–1.5 cm, white areas that were confirmed microscopically to be infarctions secondary to thrombosis (Fig. 4A, 4B).
American Quarter Horse.
The fetal liver had diffuse centrilobular hepatocellular degeneration that progressed to centrilobular necrosis in some areas. The liver also showed diffuse congestion of portal venules, disassociation of periportal hepatocytes, and moderate periportal extramedullary hematopoiesis. The area of the liver corresponding to the grossly observed abdominal adhesions had areas of necrosis with focal infiltration by neutrophils. Distended veins throughout the liver contained moderately dense aggregations of fibrillar material mixed with mature and immature red blood cells. The fetal lung was noninflated and did not have significant inflammatory exudate in air spaces. The trachea had submucosal edema. The spleen was expanded by cells indicating extramedullary hematopoiesis. Thyroid follicles near the center of the organ were distended by colloid. The adrenal gland and kidney had congestion at the corticomedullary junction. No lesions were observed in the fetal heart.
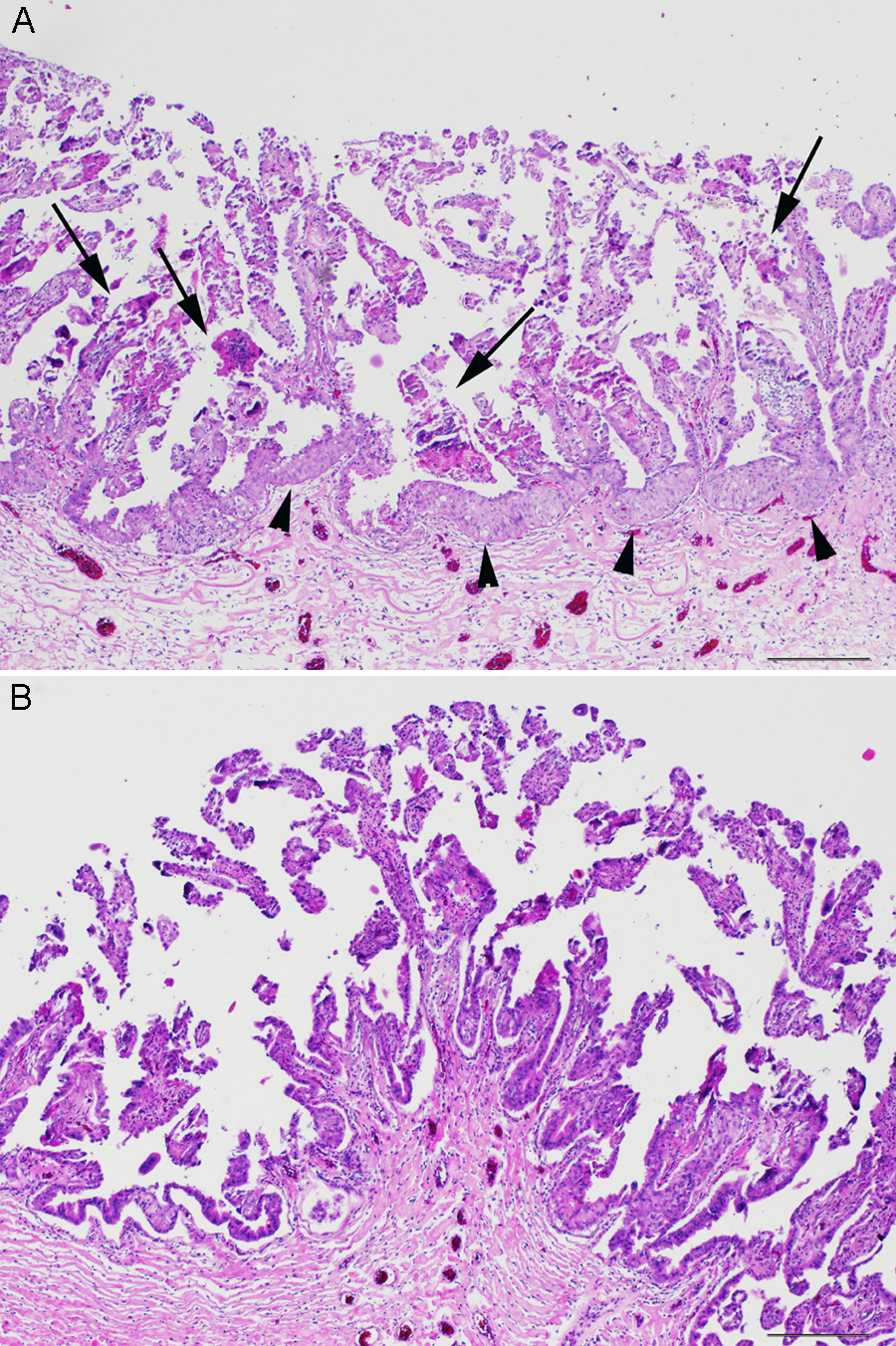
Microscopically, the chorioallantois of the gravid horn had blunted, shortened, and often necrotic villi with variable hyperplasia and syncytia formation in the trophoblast later. The chorionic surface had minimal exudate, and, when present, the exudate consisted of exfoliated trophoblasts and detached villi (Fig. 5A). The chorioallantoic stroma had diffuse congestion. In selected sections, vessels in the chorion contained marginated neutrophils or foci of dystrophic calcification. The chorioallantois from the non-gravid horn was slightly autolyzed but had morphology consistent with a normal placenta and lacked hyperplasia of the trophoblast layer and villar necrosis (Fig. 5B).
American Quarter Horse.
Histologic sections of the allantoamnion had diffuse edema and congestion. Areas most distant from the umbilical cord attachment had mild inflammation around allantoic vessels. Sections adjacent to the umbilical cord and corresponding to infarctions were cuffed primarily by neutrophils and fewer mononuclear cells. Many vessels in this area were densely cuffed by inflammatory cells and contained intraluminal thrombi composed of degenerate inflammatory cells and amorphous eosinophilic debris (Fig. 4B).
Ziehl–Neelsen acid-fast staining was conducted on all tissue blocks associated with the current case. Intracellular acid-fast bacilli were abundant in trophoblasts from the gravid horn and the cervical star of the chorioallantois. Intracellular bacteria were often directly associated with areas of villar necrosis, and in these areas, mild neutrophil infiltration was present. Intratrophoblastic acid-fast bacteria were observed in the cervical star chorion without villar necrosis, inflammation, and hyperplasia of trophoblasts (Fig. 6A, 6B). The non-gravid horn had a few intracellular acid-fast bacteria, but these bacteria were present in free-floating detached trophoblasts. No intracellular acid-fast bacteria were observed in the umbilical cord, allantoamnion, liver, lung, adrenal gland, spleen, kidney, or heart.
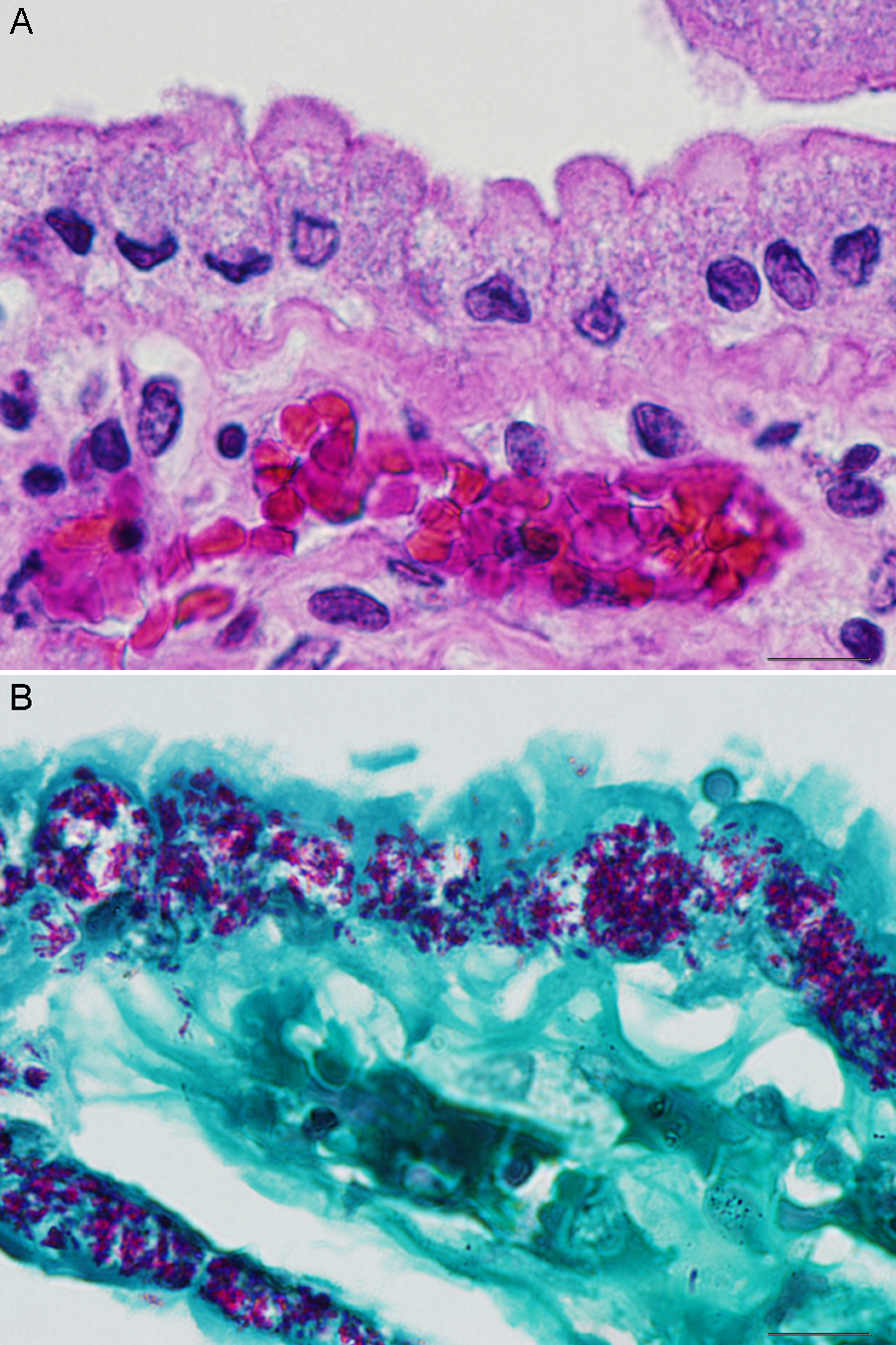
American Quarter Horse.
A pure growth of Mycobacterium Runyon group IV was isolated from the chorioallantois. Other pathogenic bacteria or fungi were not isolated from the amnion, vaginal discharge, fetal lung, fetal liver, and fetal stomach contents. Polymerase chain reaction for Equid herpesvirus 1 was negative.
Runyon group IV mycobacteria are comprised of fast-growing, saprophytic, acid-fast bacilli that usually infect as a transient colonizer without pathogenicity and is a nontuberculous mycobacterium grouping that encompasses all mycobacteria outside of the Mycobacterium tuberculosis complex. 10 Mycobacteria are well known for their intracellular multiplication but may also multiply extracellularly. 10 The use of Ziehl–Neelsen acid-fast stain was vital to microscopic pathogen detection because the lipid-rich cellular wall of these bacteria made it nondetectable by hematoxylin and eosin and Gram stains. 10
Sequence analysis of the 16S ribosomal RNA gene and the rpoβ gene, the latter encoding the β subunit of RNA polymerase, at Veterinary Diagnostic Laboratory, College of Agriculture, University of Kentucky (Lexington, Kentucky) was used to attempt species-level identification of the culture. This sequencing strategy was developed to improve the recognition of numerous bacterial genera including Mycobacterium.1,14,16 The rpoβ gene, made up of 723 base pairs, is linked with each established species of Mycobacterium. The bacteria isolated in the current case contained 5% difference in base pairs of the rpoβ gene from all currently known species and therefore was considered a novel species.
Five days following the abortion, a transrectal palpation and ultrasound of the mare revealed a normally contracting uterus with 3 cm of hyperechoic free fluid within the body of the uterus. The cervix was open, and a moderate amount of purulent discharge was present within the vaginal canal. No further treatment was performed, and the mare was retired from breeding due to multiple failures to produce a live foal. Her owners declined further treatment. The vaginal discharge resolved within 10 days of the abortion, and the mare remains systemically healthy.
Five other cases of Mycobacterium spp. abortion are reported by abstract from Kentucky mares between 2002 and 2006 (Bryant U, Giles R, Tramontin R, et al: 2007, Mycobacterial abortion in 5 thoroughbred mares. Vet Pathol 44:742. Abstract). The causative agent in each case was an unspecified species of mycobacteria. This prior abstract report does not supply the age of gestation or the specific microscopic findings present in each case. In addition to this abstract report, 3 other single-case reports have confirmed Mycobacterium species (M. avium and M. terrae) as the causative organism in an equine abortion.4,9,22 In 2 of these cases, systemic mycobacteriosis was confirmed or suspected in the mare.4,9 Including the current case, 5 out of 9 mares with confirmed mycobacterial abortion have reported abortions or stillbirths in the preceding years, but the cause of these abortions was undetermined.9,22
The current case is unique in that mycobacteria, primarily identified in the cytoplasm of chorionic trophoblasts, did not initiate a significant inflammatory response unless villar necrosis had occurred. The prominent area of brown discoloration observed grossly in the gravid horn of the chorion corresponded to villar necrosis rather than inflammatory exudate, as was originally assumed at necropsy. It is hypothesized that regionally diffuse colonization of trophoblasts by intracellular bacteria along with extensive villar necrosis and trophoblastic hyperplasia impaired oxygen exchange. This led to venous hypoxia in the umbilical cord and anaerobic centrilobular degeneration and necrosis in the liver. Areas of regional necrotizing hepatitis with adhesion were most likely secondary to hypoxia. No bacteria were observed in areas of hepatic necrosis. Disruption of fetal circulation caused by hepatic necrosis most likely contributed to thrombosis of allantoic vessels in the allantoamnion. It is also believed that allantoic thrombosis and hepatic necrosis blocked return of blood from the chorioallantois and increased venous pressure in allantoic veins. Increased venous pressure resulted in fluid leakage from vessels and may have caused development of prominent perivascular fluid accumulation and eventual allantoic fluid saculations. A 2009 publication refers to these structures as “mega allantoic vesicles” and discusses the possible cause and debates the clinical significance. 20
Although mycobacteria are uncommon causes of placentitis and abortion, mycobacteriosis should be suspected in cases of chronic placentitis where more common bacteria are not isolated. In order to increase the likelihood of diagnosing a mycobacterial abortion, the placenta from any mare exhibiting atypical lesions of placentitis should be microscopically examined with an acid-fast stain. The current case illustrates that gross lesions of mycobacterial placentitis may be misinterpreted as nocardioform placentitis. Classic nocardioform placentitis typically occurs later in gestation and has a more copious mucoid exudate on the chorionic surface. 3 Mycobacteria are ubiquitous in the environment and may be isolated from the soil. With detection of intratrophoblastic mycobacteria at the cervical star, the cervical route of infection was considered in this case. The cervical star, however, lacked villar necrosis and trophoblastic hyperplasia observed in the gravid horn. Thus, it was believed that the infection initiated in the chorion of the gravid horn because the microscopic lesion at this location was more chronic. Although intratrophoblastic mycobacteria have not been previously reported from the horse, mycobacteria have been documented to infect trophoblasts in other species. 12 Intratrophoblastic infection of other infectious organisms has been documented in horses and these include Encephalitozoon cuniculi and Chlamydophila psittaci.17,21 Other bacteria such as Brucella spp. and Listeria monocytogenes are also documented to cause intratrophoblastic infection in other species.7,19 Because mycobacteriosis is usually chronic and the bacteria elude the immune system through intracellular multiplication, it is possible that this mare was infected at the time of breeding or had a chronic infection over several years. It should be noted that other reported cases of mycobacterial abortion have been accompanied by confirmed chronic systemic infection in the mare. 4 Other theories to explain the route of infection are the same theories implicated for nocardioform placentitis and include hematogenous spread and direct inoculation via foreign body through the colon wall. None of these theories for nocardioform placentitis have specific scientific data to support them and the route of infection for “atypical placentitis” is still unknown.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.