
Abstract
The present case report describes isolation of the fungus Oxyporus corticola from multiple lymphocutaneous tissues of a Beagle dog. Until recently, this fungus had not been reported in the human or veterinary medical literature as a cause of animal disease. A single previous report also involved infection in a German Shepherd Dog, a breed with reported increased susceptibility to disseminated fungal infection and dysfunctional immune response. Isolates were non-sporulating and required molecular identification methods for prompt differentiation from other fungal pathogens. Risk factors for infection with O. corticola are unknown.
A 3-year-old, female spayed Beagle dog was referred to Leesburg Veterinary Internal Medicine at the LifeCentre (Leesburg, Virginia) for evaluation of persistently enlarged popliteal lymph nodes of approximately 10 weeks duration, which had occurred spontaneously with no other clinical signs. A fine-needle aspirate had previously been obtained from the left popliteal lymph node. Cytologic evaluation of the aspirate revealed abundant blood with focal collections of lymphocytes and occasional plasma cells interpreted as consistent with hyperplastic lymph node. Doxycycline a (50 mg orally once every 12 hr for 10 days) was prescribed with no change in lymph node size. Six weeks before presentation, the patient was clinically unchanged; complete blood cell count and serum chemistry panel with electrolytes were performed. All test values were within normal limits, with the exception of eosinopenia (0; reference [ref.] range: 100–1,250), hyperglobulinemia (6.0 g/dl; ref. range: 2.5–4.5 g/dl), and hyperproteinemia (8.7 g/dl; ref. range: 5.2–8.2 g/dl). Results of a point of care test b for antibodies to Ehrlichia canis and Borrelia burgdorferi and antigens of Dirofilaria immitis were negative, and no significant abnormalities were observed in thoracic and abdominal radiographs. Enrofloxacin c (22.7 mg orally once every 24 hr for 21 days) was prescribed, and the patient was referred for further assessment.
At presentation, the dog weighed 12.0 kg and had normal vital signs. Significant physical examination findings were those of enlarged, firm popliteal lymph nodes (left 4 cm, right 2 cm), firm and enlarged (1 cm) right caudal mammary nodule, and a left caudal thoracic, firm intradermal nodule (1 cm). Ultrasonography of the abdomen revealed marked enlargement of the inguinal lymph nodes (4.4 cm × 1.1 cm, 3.6 cm × 2.3 cm) with all other organs normal in appearance. Cytologic examination of aspirates from the left popliteal lymph node and mammary nodule revealed scattered branching, septate fungal hyphae, approximately 1–2 mm in width, with parallel, nonstaining cell walls, and basophilic internal structure.
A portion of each aspirate fluid was placed on a swab, submerged into the gel portion of a commercial culture transport system, d and then submitted by overnight courier to the Clinical Bacteriology and Mycology Laboratory at the University of Tennessee, College of Veterinary Medicine (Knoxville, Tennessee) for fungal culture. Primary culture media and incubation conditions included inhibitory mold agar e (IMA) incubated at 30°C aerobically, mycosel agar e (MYC) incubated at 30°C aerobically, and Columbia agar e containing 5% sterile defibrinated sheep blood f (BA) incubated at 35°C in an atmosphere containing 7% CO2. Each aspirate yielded growth of greater than 100 colonies of an identical appearing fungus, in apparent pure culture, after 3 days of incubation on BA and IMA. Colonies on BA were wet, gray, and adherent to the agar (Fig. 1). After several weeks, a few colonies on BA developed small white patches of aerial mycelia. On IMA, the colonies were white, velvety, and increased slowly in size with age, becoming more wooly and having a slight tan color (Fig. 2). There was no distinct reverse pigment. Growth on MYC was delayed (3 weeks) in primary cultures and negative on subculture. Subcultures grew poorly on potato dextrose agar. e
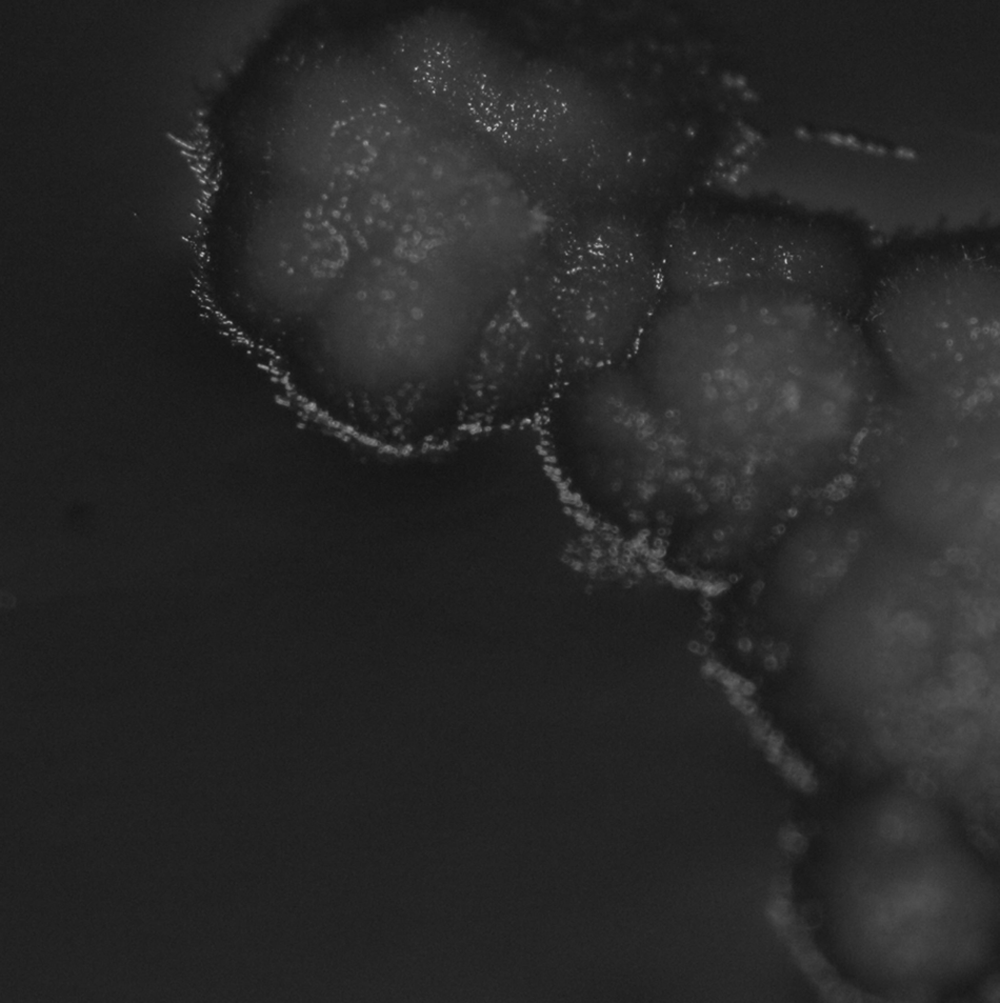
Oxyporus corticola isolate lacking aerial mycelia when grown on blood agar incubated at 35°C (7 days).
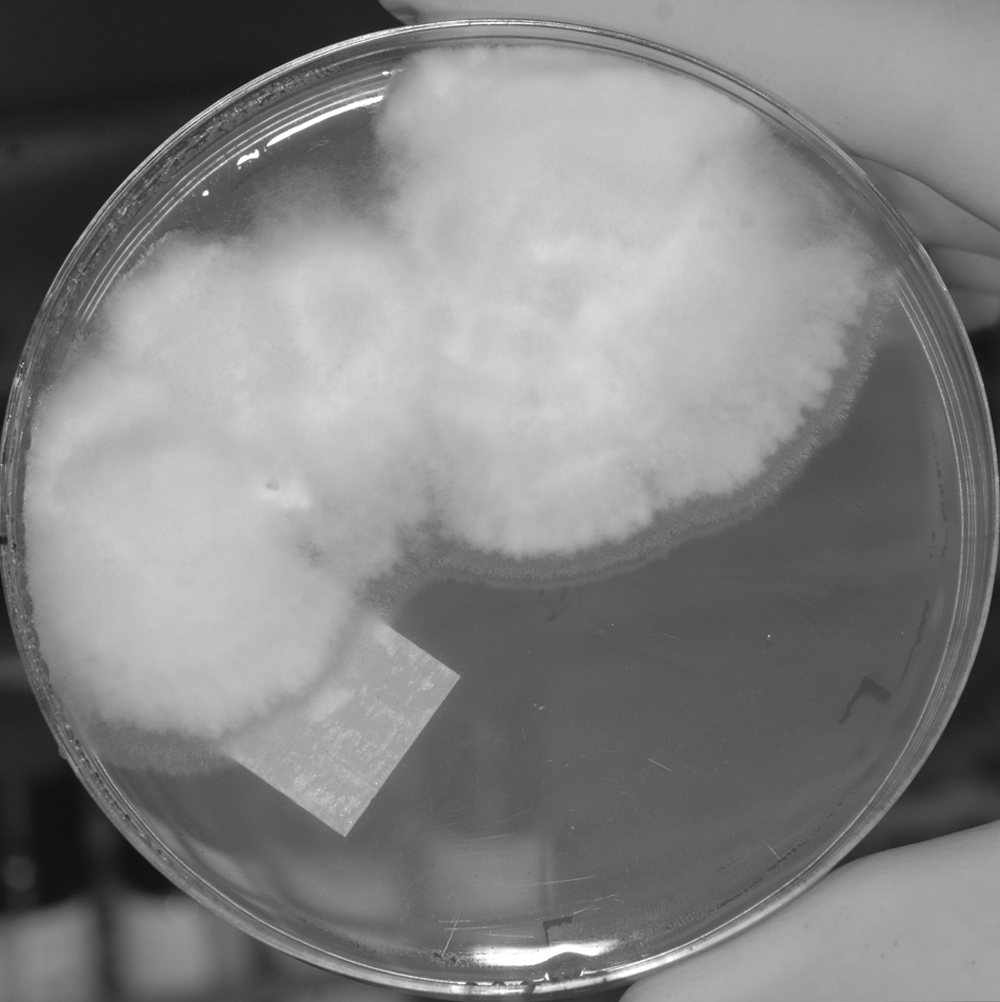
Oxyporus corticola isolate on inhibitory mold agar incubated at 30°C (31 days).
Microscopic appearance of the fungus was that of narrow, septate, parallel-walled, acute-angle–branching hyphae. Mature fruiting structures were not observed; however, terminal hyphal swellings resembling terminal vesicles or immature chlamydospores were occasionally observed in aged IMA cultures (Fig. 3). Antifungal susceptibility studies were not performed on this isolate because of the lack of standardized methods for performing and interpreting the results of such testing.
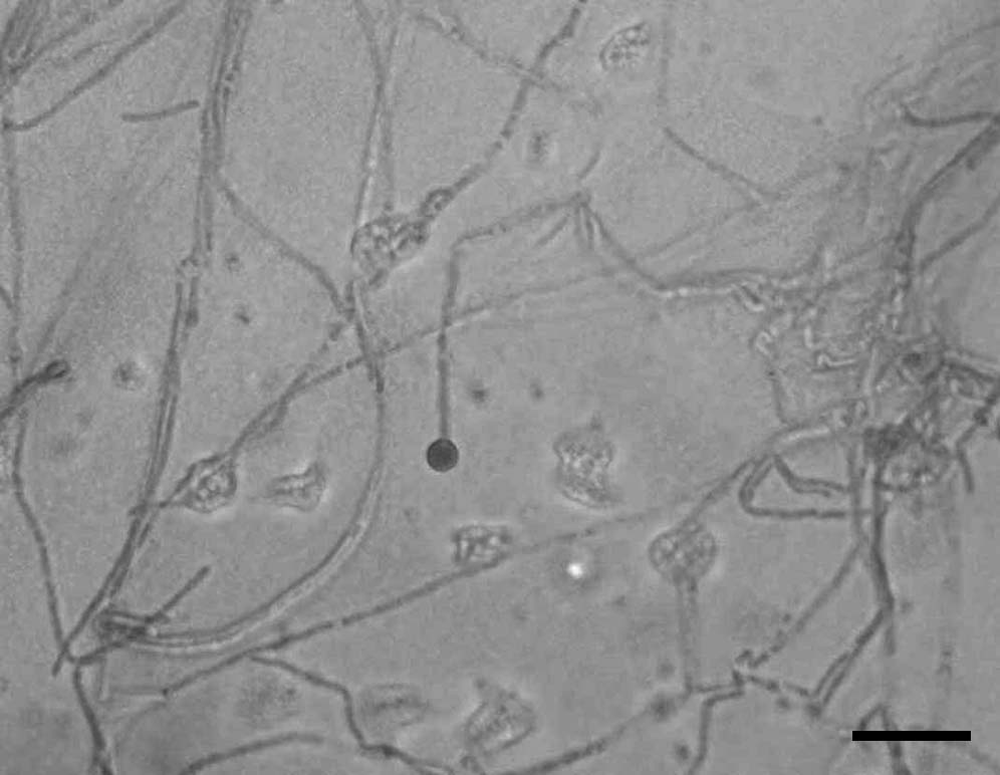
Microscopic appearance of Oxyporus corticola isolate from inhibitory mold agar incubated at 30°C (31 days) showing a rare spore-like structure. Lactophenol cotton blue. Bar = 37 µm.
Antifungal therapy was declined due to cost concerns. Empirical therapy of cephalexin g (250 mg orally once every 12 hr for 21 days) and metronidazole h (125 mg orally once every 12 hr for 21 days), in treatment of potential bacterial infection, was prescribed pending sample culture results. Results were finalized, and a definitive diagnosis was determined 6 weeks after sample submission. To alleviate patient discomfort due to the enlarged lymph nodes, tramadol i (25 mg orally once every 12 hr for 7 days) was prescribed. The left thoracic intradermal nodule ruptured and drained periodically, and transient decrease in appetence was reported.
Three weeks after presentation, therapy with amphotericin B was declined, and itraconazole j (40 mg orally every 12 hr for 18 days) was initiated with no change reported by the owner. Long-term administration was recommended, but the medication was not continued due to cost concerns. Periodic verbal reports from the owner indicated waxing and waning energy and appetite.
Ten weeks after presentation, tests for histoplasmosis were negative (Histoplasma capsulatum quantitative antigen enzyme immunoassay k on urine and agar gel immunodiffusion for Histoplasma antibodies of serum). The negative results did not preclude Histoplasma infection, but implied that infection with Histoplasma and Blastomyces (which is cross-reactive with Histoplasma in the above testing) were unlikely. Although the isolate exhibited rapid growth on IMA and was not likely to represent a typical thermodimorphic fungus, mold to yeast conversion procedures were attempted because of difficulty identifying the mold. Subculture of mycelia from mold grown on IMA at 30°C consistently produced predominantly gray colonies with substrate mycelia on BA at 35°C. Interestingly, the isolate failed to grow, after multiple subcultures, on brain heart infusion agar whether incubated at 35°C or 30°C.
Fourteen weeks after initial presentation, the patient was presented with complaints of lethargy, weight loss, and anorexia. At the owner’s request, euthanasia was performed. A minimally invasive postmortem assessment was performed. Muscle wasting, and enlarged popliteal, axillary, and prescapular lymph nodes, as well as enlargement of mesenteric and lumbar lymph nodes were present. Thoracic radiographs revealed caudal displacement of the heart and lungs by a 10 cm × 7 cm cranial mediastinal mass, most likely mediastinal lymph nodes. Abdominal radiographs showed an enlarged lumbar mass effect, again most likely reflecting an enlarged lymph node, and marked gastric distention by luminal contents. Mesenteric lymph nodes were markedly enlarged based upon palpation. Hepatosplenic enlargement was not visualized via radiography or appreciated via abdominal palpation. Tissue samples of the popliteal lymph nodes and the intradermal nodule were collected via sterile surgical technique and submitted for fungal culture and histopathologic examination as described above.
Two slides of formalin-fixed left lymph node tissues were assessed. The specimen consisted of tissue without natural surfaces. The tissue was slightly lobulated, but residual lymph node architecture, such as remnants of a capsule, subcapsular, and medullary sinuses, was not seen. The nodules consisted of aggregates of inflammatory cells. The inflammatory cell infiltrate consisted of many multinucleated cells and scattered macrophages with many plasma cells among them. Small lymphocytes, eosinophils, and neutrophils were also present in lower numbers. Some nodules had central areas of necrosis. The necrotic foci were stained dull pink and granular. There were occasional fragments of cellular debris. Branching, septate fungal hyphae were within multinucleated cells and macrophages (Fig. 4). The hyphae had parallel to slightly tapering walls. There were rare spores. The fungal organisms were visible on slides stained with hematoxylin and eosin, periodic acid–Schiff, and Gomori methenamine silver.
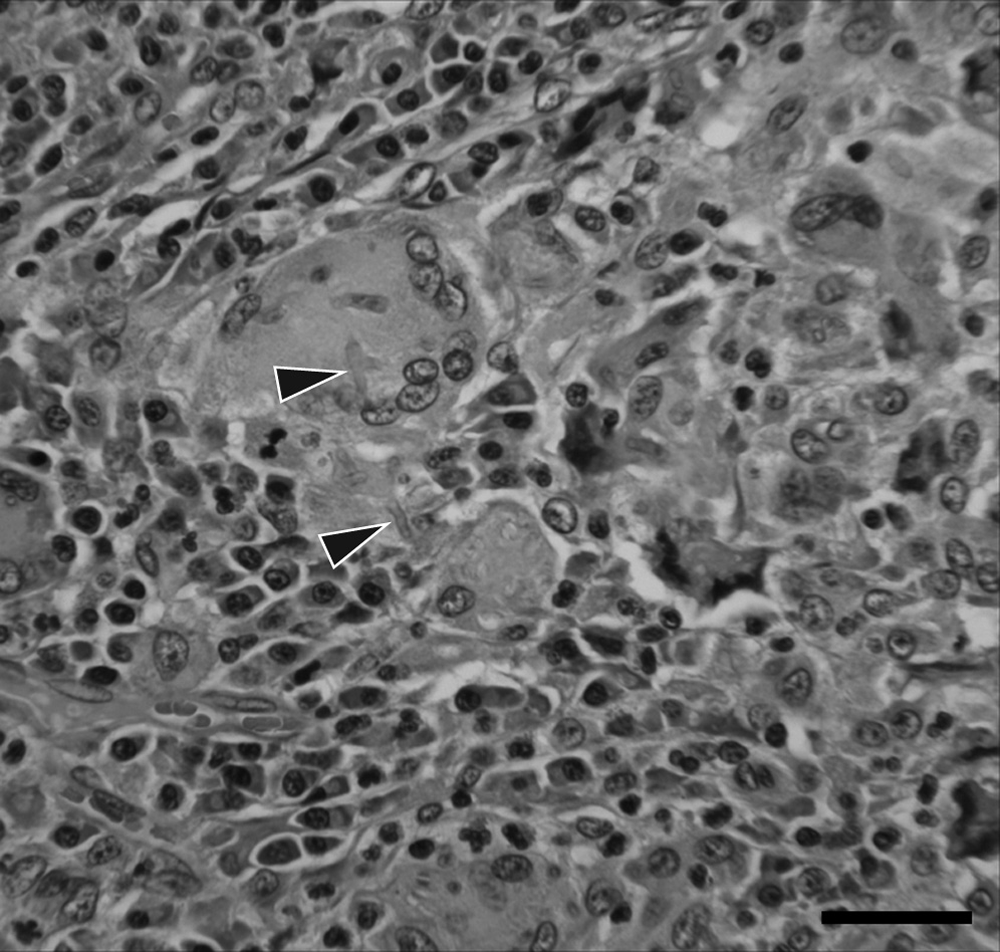
Hematoxylin and eosin–stained histopathology slide of lymph node biopsy showing macrophage with associated hyphal elements (arrows). Bar = 112 µm.
DNA extracted from the fungal isolates was used as template for polymerase chain reaction (PCR) using primers internal transcribed spacer (ITS)4 and ITS5 to amplify the entire ITS region, 5.8S ribosomal RNA gene, and portions of the 18S and 26S ribosomal RNA genes, as previously described. 11 DNA sequences (664 nt) obtained directly from the PCR products had 99% sequence similarities, as determined by BLAST 1 search of the GenBank database, to those of 5 Oxyporus corticola strains, including one previously isolated from a dog (GenBank accession no. EF011124). The next closest matches to other fungal genera and species lacked sufficient discrimination for identification. Subsequent PCR using primers ITS1 and NL4, as previously described, 9 amplified a fragment that encompassed both the ITS region and the D1/D2 region of the 25S ribosomal RNA gene. Individual analysis of sequences representing the ITS and D1/D2 regions within this fragment, using primer sets ITS1/ITS4 and NL1/NL4, respectively, as previously described, 9 revealed that sequences (605 nt and 648 nt, respectively) from both regions had 99% similarities to those of the previously reported canine isolate (GenBank EF011121 and EF011117, respectively).
Identical appearing isolates were obtained from biopsy samples taken from the right and left popliteal lymph nodes at the time of euthanasia. DNA sequences from the ITS region of these isolates were aligned with those of the initial isolates using commercial software. l The sequences of all 4 isolates were identical. Sequence from a representative isolate (from mammary nodule) obtained in the current study has been assigned GenBank accession number JF894098, and the isolate has been deposited into the University of Alberta Microfungus Collection and Herbarium (http://www.ales.ualberta.ca/devonian/uamh/) accession no. UAMH 11535.
Filamentous basidiomycetes or mushrooms and smuts are commonly found on decaying trees and woody plants and are considered to be emerging and unusual human pathogens.4,6 In addition to the present case, 2 reports of canine infections caused by filamentous basidiomycetes have appeared in the medical literature, one involving Schizophyllum commune in a mixed breed dog from Japan 5 and the other O. corticola in a German Shepherd Dog from the midwestern United States. 2 Dysfunctional immune response8,10 and genetic predisposition to disseminated Aspergillus terreus infection 3 is reported in the German Shepherd Dog. These factors may also result in increased susceptibility to disseminated O. corticola specifically in the German Shepherd Dog. The current case is noteworthy in that it describes disseminated O. corticola infection in a breed that is not reported to have increased susceptibility to disseminated fungal infection.
Since identification of O. corticola isolates from dogs requires molecular characterization, previous isolates may have been recognized simply as hyaline fungi producing sterile mycelia. To understand virulence properties and infection risk factors associated with these rare but emerging opportunistic pathogens, it is important to examine additional isolates. Genotyping techniques, such as multilocus microsatellite typing, 7 may reveal epidemiologically useful features that distinguish canine isolates from other environmental isolates of the species. The present report suggests that O. corticola infections in dogs, while rare, may be more prevalent than currently known and emphasizes the need to identify and collect additional isolates. Comparative studies on such isolates are needed to establish and standardize testing methods. Veterinary diagnosticians are encouraged to confirm and document the identification of unusual fungal isolates causing infection in dogs.
Footnotes
Acknowledgements
The authors thank Rebekah Jones, Brian Johnson, Rupal Brahmbhatt, and Jennifer Steinberg for technical assistance.
a.
Doxycycline, Par Pharmaceutical Inc., Woodcliff Lake, NJ.
b.
SNAP® 3Dx® Test, IDEXX Laboratories, Portland, ME.
c.
Enrofloxacin, Bayer Healthcare LLC, Shawnee Mission, KS.
d.
CultureSwab™ Plus with Amies, BD Diagnostic Systems, Sparks, MD.
e.
BBL™ Dehydrated Culture Media, BD Diagnostic Systems, Sparks, MD.
f.
Hemostat Laboratories, Dixon, CA.
g.
Cephalexin, Apothecon Inc., Princeton, NJ.
h.
Metronidazole, Akyma Pharmaceuticals LLC, Glasgow, KY.
i.
Tramadol, Amneal Pharmaceuticals, Glasgow, KY.
j.
Itraconazole, Janssen Pharmaceuticals Inc., Titusville, NJ.
k.
Histoplasma Antigen Enzyme Immuno Assay, MiraVista Diagnostics, Indianapolis, IN.
l.
DNA Lasergene®, version 7.2, DNASTAR Inc., Madison, WI.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.