
Abstract
Localized, myocardial toxoplasmosis contributed to the death of a female ring-tailed lemur (Lemur catta) 1 week after the delivery of 4 stillborn offspring with disseminated toxoplasmosis; the diagnosis was obtained by histopathology and immunohistochemistry in all 5 lemurs. Varying degrees of placentitis and placental edema with intralesional Toxoplasma gondii immunolabeling were observed in the 3 available placentas. The dam had severe myocarditis, and T. gondii antigen was only detected in the myocardial lesions. Disseminated toxoplasmosis with mild encephalitis was noted in all 4 fetuses, and 2 of the fetuses had mild acute multifocal hepatic necrosis. Fetal death was attributed to placental insufficiency with subsequent hypoxia and amniotic fluid aspiration.
Keywords
Toxoplasmosis is a worldwide-distributed protozoal disease caused by the coccidian Toxoplasma gondii. Felids serve as definitive hosts shedding oocysts in feces while a variety of vertebrates are intermediate hosts. 6 Disease presentations and mortality vary greatly depending on the susceptibility of the species affected and host-parasite relationship, and other factors including the immune response and the occurrence of disease after initial exposure or as a reactivation of latent infection. Disease after initial exposure is usually an acute disseminated process involving a variety of organs including the intestine, lymph nodes, liver, and lungs and causing mostly necrotizing and inflammatory lesions and interstitial pneumonia. Unlike acute disseminated toxoplasmosis, reactivation of latent infection usually is followed by inflammatory lesions localized in neural and muscular tissues. Such tissues are the most common targets for Toxoplasma tissue cysts, which are more commonly found in chronic latent toxoplasmosis.3,6 Fatal acute disseminated toxoplasmosis is a frequent epizootic disease of highly susceptible nonhuman primates (New World monkeys and lemurs), presenting typically with enteritis, necrotizing mesenteric lymphadenitis and hepatitis, interstitial pneumonia, and/or pulmonary edema.2,7,12
Localized toxoplasmosis involving usually the heart and central nervous system6,15,17 and transplacental infection5,8,16,18 can occur in a variety of animal species and human beings; however, this appears to be the first report of localized toxoplasmosis and transplacental transmission with placentitis, disseminated fetal infection, and stillbirths in ring-tailed lemurs (Lemur catta) and any other highly susceptible nonhuman primate in the literature reviewed by the authors.
A 3-kg, adult ring-tailed lemur was hospitalized because of severe cage mate trauma, distended abdomen, and decreased appetite. Radiographs revealed pregnancy with 4 fetuses. One week after presentation, the lemur delivered 2 stillbirths during hospitalization; a third fetus was extracted manually because of abnormal position, and the fourth stillbirth was delivered after oxytocin injection. Hospitalization with antibiotic and supportive treatment was continued for 1 week until the dam recovered fully from trauma and started to feed on its own. The lemur was returned to the zoo and housed in the quarantine area with 2 other lemurs before reintroduction into the group, but it presented 12 days later with anorexia and died within 2 days despite intensive care. Three weeks before the death of this lemur dam, another breeding female suffered cage mate aggression and delivered a dead fetus the same day; this female died 3 days later. Acute disseminated toxoplasmosis as previously described in lemurs 7 was diagnosed by histopathology. The fetus was not necropsied, and therefore tissues were not available for histopathology. For these reasons, the second female and stillborn fetus were not included in the current study. These lemur dams had been housed in a group of 23 ring-tailed lemurs (19 males and 4 females). To date, 2 females have bred uneventfully in 2010. Their diet consists of primate pellets, fruits, and vegetables, and less frequently boiled rice and corn; bamboo and other plants are used for environmental enrichment. Lemurs have contact with people (children offering small quantities of the lemur diet for photography). Sanitary footbaths and antimicrobial hand-washing products are available for staff and visitors. Feral cats are numerous at the zoo but they cannot enter the lemurs’ enclosure; however, the top of the enclosure consists of wire fence and cats have been known to sit on the fencing. Arthropods that can serve as transport hosts of Toxoplasma oocysts may be present even though plagues were controlled in the recent past. No clinicopathologic evidence of additional cases of toxoplasmosis was found in the available medical records.
Necropsy was performed on all 5 lemurs (1 female and 4 fetuses) by the referring veterinarians, and tissues were fixed in 10% formalin. Stillbirths were opened by the ventral midline and fixed whole in formalin together with 3 placentas. Tissues from the dam (heart, spleen, skeletal muscle, stomach, skin, trachea, ovary, intestine, lungs, adipose tissue, lymph node, pancreas, brain, salivary gland, liver, kidney, urinary bladder), the 4 stillborn lemurs (heart, esophagus, lymph nodes, elastic arteries, trachea, liver, lungs, adrenal, stomach, spleen, kidney, pancreas, intestine, skeletal muscle, spinal cord, brain, skin, and/or bone marrow), and placentas were embedded in paraffin, sectioned at 5 µm, and stained with hematoxylin and eosin. Immunohistochemical staining for T. gondii on all tissues was performed with minor modifications to a previously used protocol. 12 Briefly, an avidin–biotin–peroxidase complex method a was used. Tissue slides were incubated overnight with a rabbit polyclonal primary antibody b at a dilution of 1:500 and a biotinylated goat anti-rabbit immunoglobulin G (1:200 dilution, 1 hr). Peroxidase reaction was visualized with 0.05% diaminobenzidine c and 0.01% hydrogen peroxide. Sections were counterstained with Harris hematoxylin. Positive controls were from a dog with toxoplasmosis. Sections incubated without the primary antibody served as negative controls.
Grossly, the dam had a pale, yellowish liver. All placentas had varying degrees of diffuse edema. Moderate pectus excavatum was observed in 1 fetus. Microscopically, the dam had severe myocarditis characterized by infiltrates of lymphocytes and rare macrophages, plasma cells, and neutrophils randomly distributed in the interstitium (Figs. 1, 2). Very low numbers of round to oval protozoal organisms 2 µm in diameter with an eccentric nucleus (tachyzoites) and clusters of these organisms (aggregates of tachyzoites and tissue cysts of bradyzoites) were observed in the cytoplasm of cardiomyocytes and macrophages or extracellularly within or close to inflammatory foci (Fig. 2). Additional major lesions included acute interstitial pneumonia with atelectasis and thrombosis, hepatic lipidosis, islet hyperplasia, and granulomatous steatitis and panniculitis with steatonecrosis (fat necrosis). Additional, low-grade, but relevant lesions included mild focal lymphocytic and neutrophilic encephalitis, and mild multifocal and perivascular gastrointestinal leiomyositis. Placentas had moderate or severe diffuse mucin-rich edema and multifocal infiltrates of lymphocytes, macrophages, and rare neutrophils with leukocytic margination and pavementing in vessels in the chorionic villi (Figs. 3, 4); possible tachyzoites were found in some of the infiltrates. All 4 fetuses had diffuse atelectasis and moderate to severe aspiration of amniotic fluid. Mild multifocal and perivascular infiltrates of lymphocytes, neutrophils, and glial cells were scattered randomly in the neuropil in the brain of all 4 fetuses; 1 focus in one of the fetuses had 2 aggregates of tachyzoites (Fig. 5). Mild multifocal hepatocellular necrosis with possible intralesional tachyzoites was observed in 2 fetuses. Two fetuses had mild multifocal or perivascular lymphoplasmacytic myocarditis.
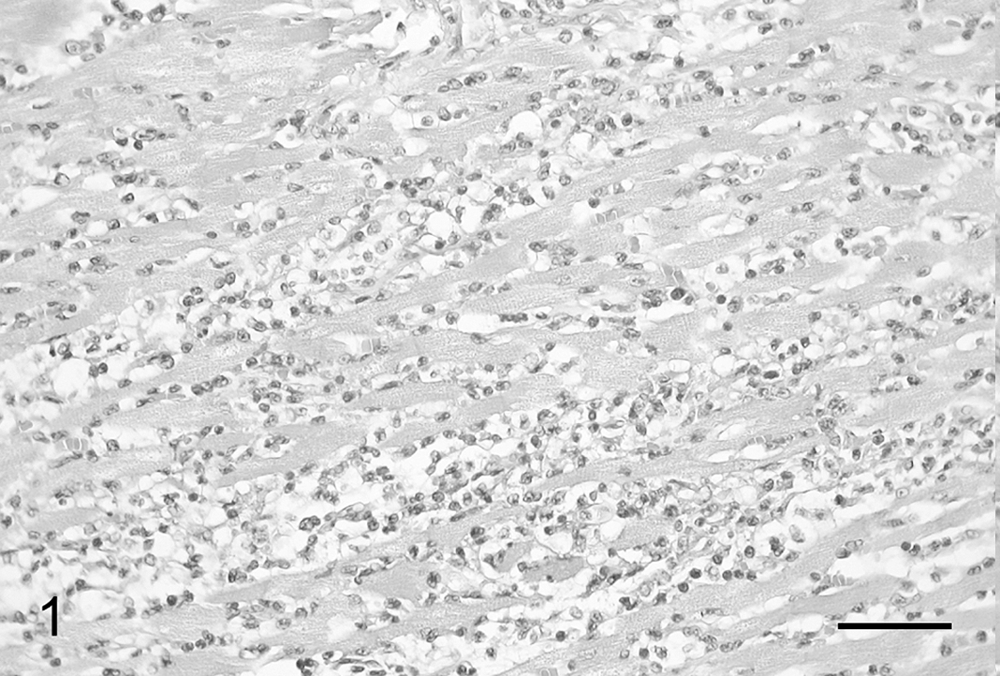
Heart; dam, lemur (Lemur catta). Note severe interstitial infiltration of lymphocytes and rare plasma cells, macrophages, and neutrophils in the myocardium. Hematoxylin and eosin. Bar = 70 µm.
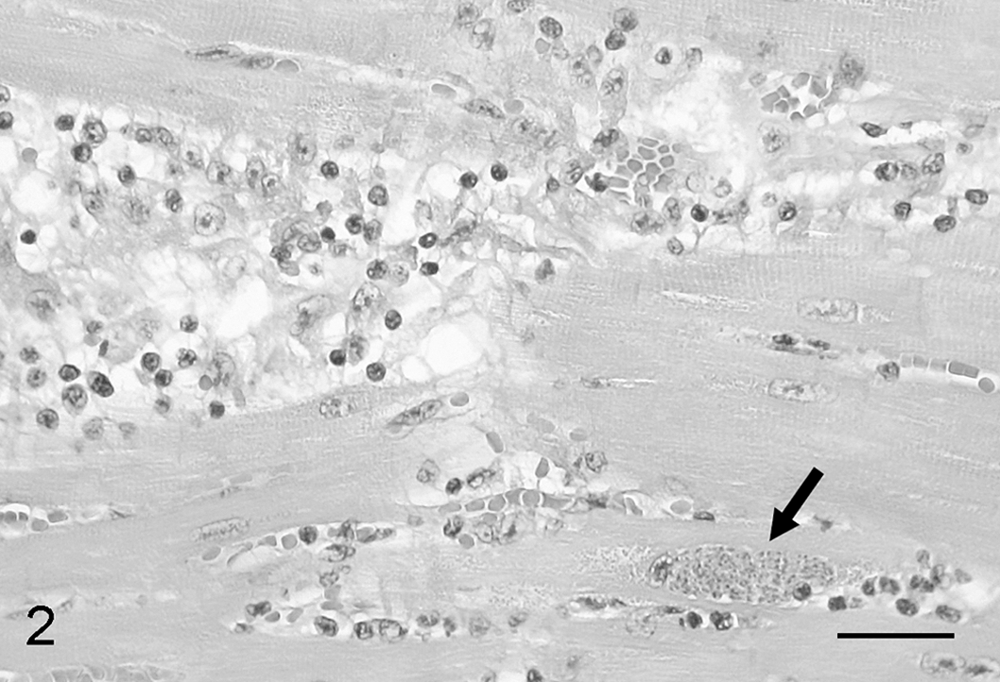
Heart; dam, lemur (Lemur catta). Note the presence of a tissue cyst of bradyzoites (arrow) adjacent to a focus of interstitial inflammation in the myocardium. Hematoxylin and eosin. Bar = 50 µm.
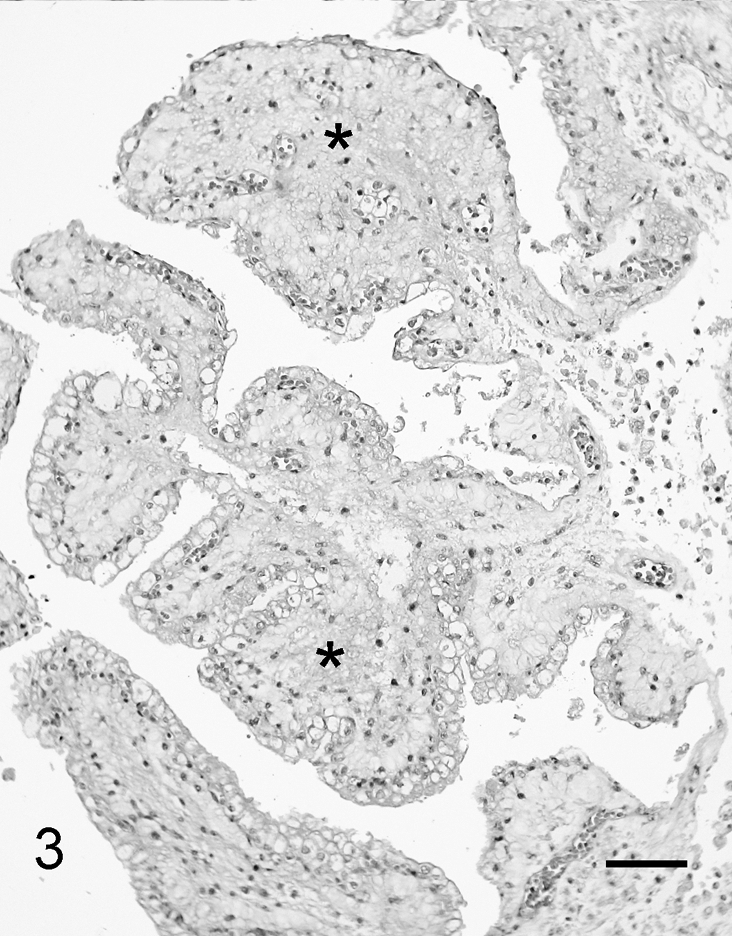
Placenta; lemur (Lemur catta). Prominent edema (asterisks) with mild infiltration of lymphocytes and macrophages in the chorionic villi is present. Hematoxylin and eosin. Bar = 125 µm.
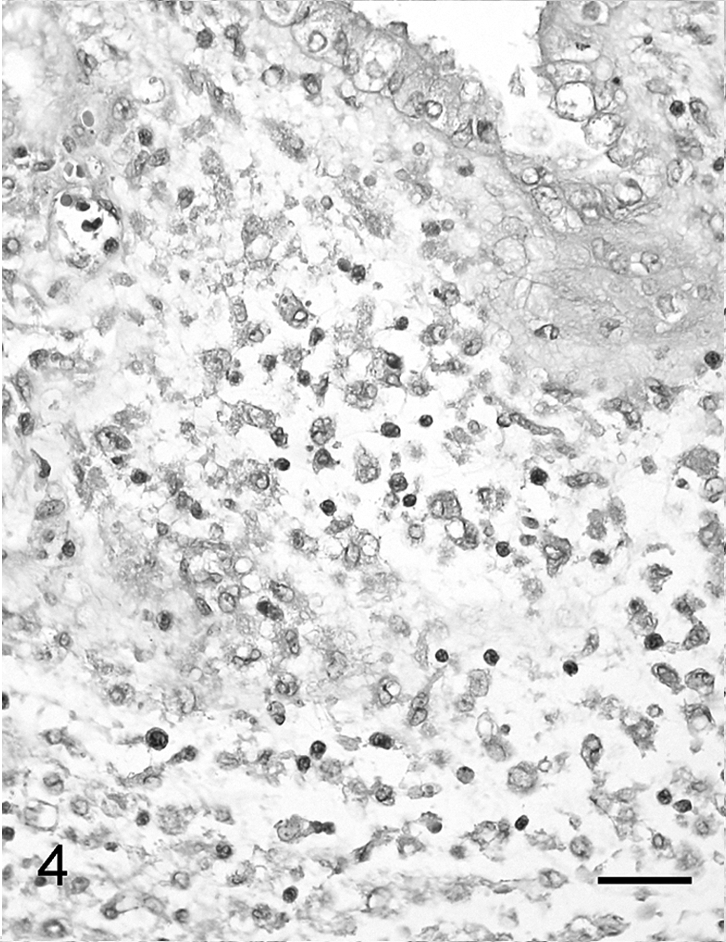
Placenta; lemur (Lemur catta). Infiltration of lymphocytes, macrophages, and plasma cells with edema in a chorionic villus is noted. Hematoxylin and eosin. Bar = 55 µm.
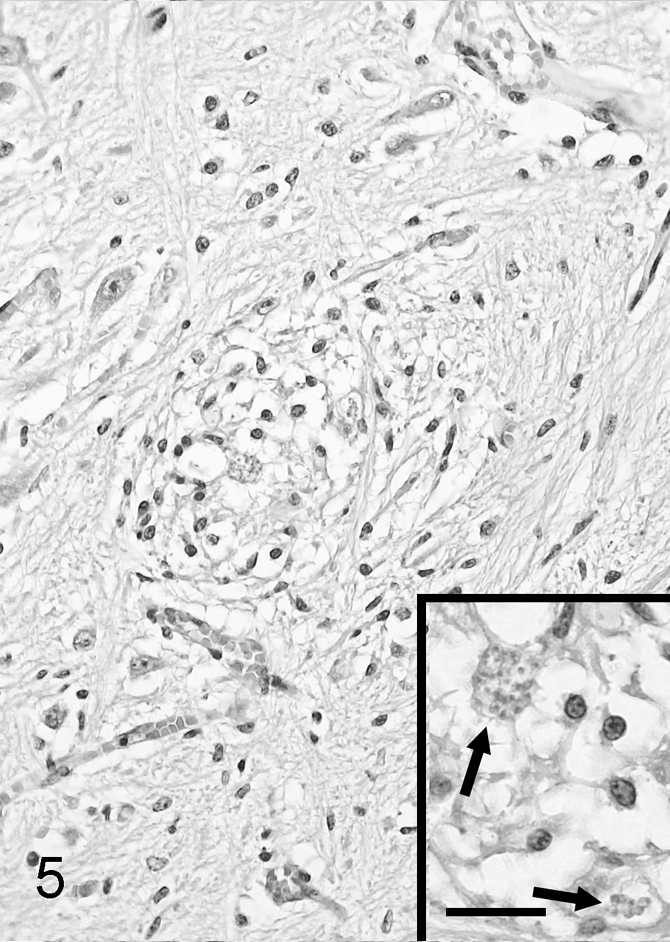
Brain; fetus, lemur (Lemur catta). Note the presence of a small focus of mild encephalitis with gliosis. Hematoxylin and eosin. Bar = 65 µm. Inset: 2 intralesional clusters of tachyzoites (arrows) are present. Hematoxylin and eosin. Bar = 30 µm.
Protozoan organisms stained positively by immunohistochemistry in all lemurs and placentas (Figs. 6–8) and were more numerous and/or readily visible than with hematoxylin and eosin stain. Toxoplasma gondii antigen consisting of ill-defined staining was also observed. In the dam, positive immunolabeling was found only in the heart in very small amounts within and adjacent or distant to foci of myocarditis (Fig. 6). No T. gondii antigen was identified within encephalitic or gastrointestinal lesions. Toxoplasma gondii antigen was found in the cytoplasm of macrophages and chorionic epithelial cells of all examined placentas (Fig. 7); antigen was also found in medial cells of few arteries in 1 placenta. Slight or mild T. gondii immunolabeling was observed in all fetuses, particularly in the heart, liver, kidney (Fig. 8), adrenal, spleen, brain, lung, lymph nodes, and intestine.
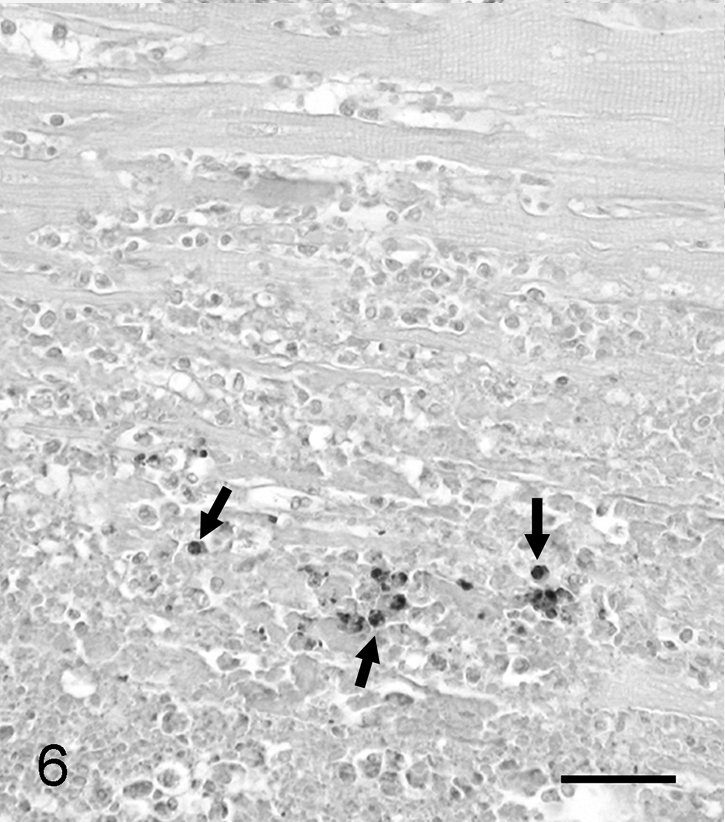
Heart; fetus, lemur (Lemur catta). A focus of myocarditis with intralesional Toxoplasma gondii immunolabeling (arrows) is observed. Avidin–biotin–peroxidase complex method, hematoxylin counterstain. Bar = 20 µm.
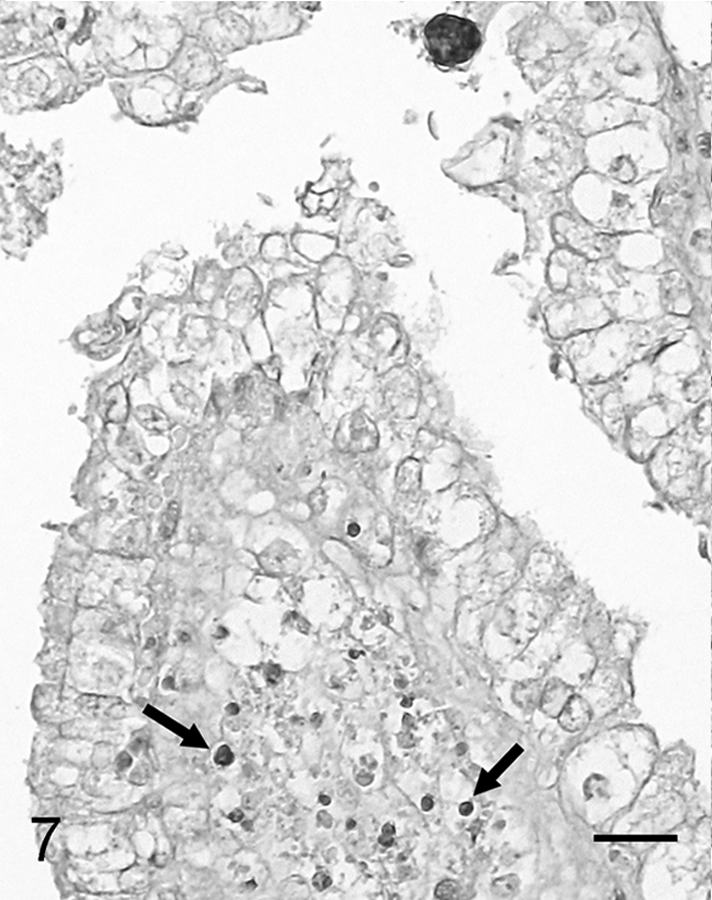
Placenta; fetus, lemur (Lemur catta). Toxoplasma gondii immunolabeling is present in the cytoplasm of macrophages in a focus of placentitis (arrows); also note 1 intact cluster of protozoa in the chorionic epithelium (top). Avidin–biotin–peroxidase complex method, hematoxylin counterstain. Bar = 15 µm.
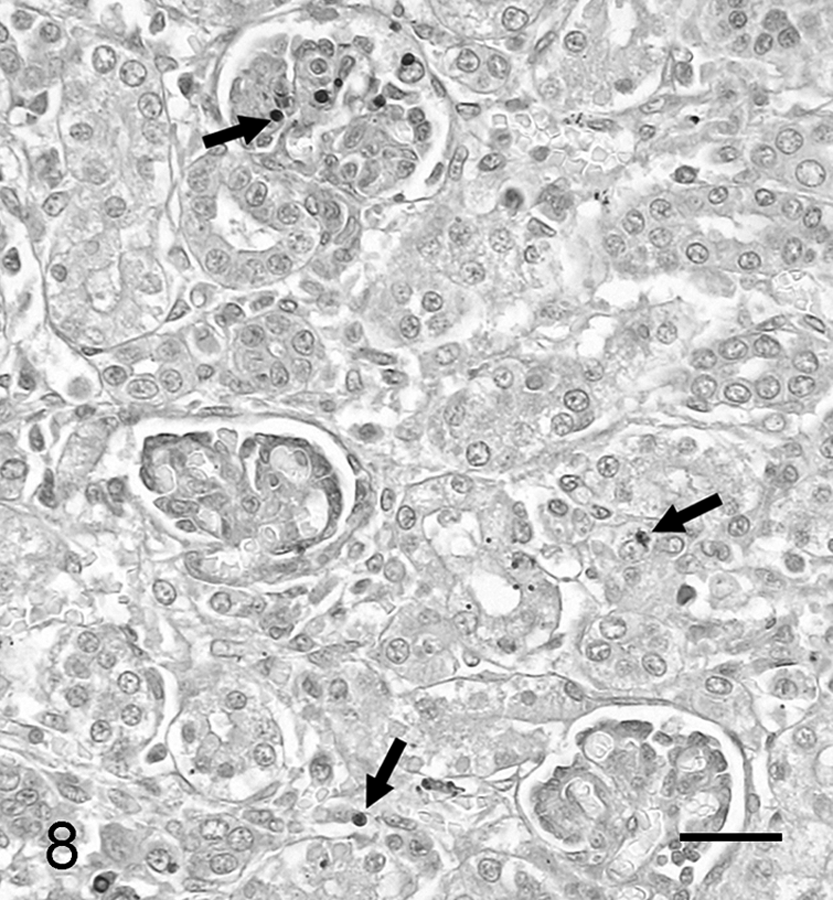
Kidney; fetus, lemur (Lemur catta). Note the presence of Toxoplasma gondii immunolabeling in the cytoplasm of mesangial cells of a glomerulus and epithelial cells of tubules (arrows). Avidin–biotin–peroxidase complex method, hematoxylin counterstain. Bar = 20 µm.
Localized myocardial toxoplasmosis was diagnosed in a ring-tailed lemur approximately 3 weeks after delivery of 4 stillbirths with disseminated toxoplasmosis based on histopathology and specific immunohistochemistry; all 3 available placentas had placentitis and edema with intralesional T. gondii antigen, which was considered the cause of fetal hypoxia with severe amniotic fluid aspiration and death. According to the literature reviewed by the authors, the current case seems to be the first description of localized toxoplasmosis and placentitis with subsequent disseminated fetal infection caused by T. gondii in lemurs and any other highly susceptible nonhuman primate species. Infection in the dam was localized in the heart based on the presence of T. gondii antigen only in the myocardial lesions; encephalitis and gastrointestinal leiomyositis may have also been caused by toxoplasmosis but antigen was not found in these tissues by immunohistochemistry. Although the dam presented with interstitial pneumonia, which is a frequent lesion of acute disseminated toxoplasmosis in lemurs and other highly susceptible nonhuman primate species, T. gondii antigen was not found in this lesion, which may have been caused by endotoxemia or bacteremia based on concurrent thrombosis.
Localized toxoplasmosis usually involves the muscular and nervous tissues6,15,17 and result from reactivation of latent infection, unlike acute disseminated toxoplasmosis, which typically results from a primary exposure (usually by the oral or transplacental route) to T. gondii. 3 Reactivation of toxoplasmosis was suspected in the dam based on the finding of localized infection in the heart. There is serological evidence indicating some lemurs can survive T. gondii infection and this supports the possibility of latency in these species despite their high susceptibility to T. gondii. Antibodies to T. gondii have been found in captive and rarely free-ranging lemurs4,13,21; however, this appears to be rare in the wild, and several field studies of several lemur species in Madagascar have failed to demonstrate T. gondii antibodies,9,10,14 which is in agreement with the assumed lack of or minimal opportunity of lemurs for contact with T. gondii in Madagascar during evolution.2,7
Several stressors including cage mate aggression in a lemur group with a sex ratio of approximately 5:1, a 2-week hospitalization (with the first week before delivery of stillbirths), and concurrent pregnancy may have facilitated reactivation of latent toxoplasmosis in this animal with subsequent transplacental infection. Pregnancy can increase the susceptibility to T. gondii infection. 19 In women, congenital toxoplasmosis usually results from acquired infection in non-immune pregnant patients, 1 but reactivation of latent infections can also occur in both immunocompetent and immunocompromised pregnant women.1,11 In the lemur dam of the current report, severe localized (myocardial) toxoplasmosis suggests reactivation of latent infection, which may have been facilitated by stress resulting from cage mate aggression, hospitalization, and/or pregnancy.
Placentitis was followed by disseminated fetal infection. This demonstrates that vertical transmission of T. gondii can occur even in highly susceptible nonhuman primates and raises the possibility of involvement of vertical infection in the transmission and maintenance of toxoplasmosis in some captive populations of these species if infected fetuses survived. The death of all fetuses was attributed to hypoxia from placentitis and placental edema with subsequent severe amniotic fluid aspiration; lesions attributable to disseminated toxoplasmosis in the stillbirths, mostly hepatic necrosis and encephalitis, were of low histologic grade and thus considered minor contributors to their demise. Reports of congenital toxoplasmosis in nonhuman primates are rare and consist of experimental infections in resistant species (macaques).18,20
In conclusion, localized (myocardial) toxoplasmosis with placentitis, placental edema, and transplacental infection with subsequent fetal disseminated infection and death is described in a pregnant ring-tailed lemur; congenital toxoplasmosis in the present case may have occurred due to reactivation of maternal latent infection. Although uncommon, toxoplasmosis should be considered as a differential for placentitis and reproductive failure in lemurs.
Footnotes
Acknowledgements
The authors thank Mundomar, Parque de animales marinos y exóticos, Alicante, Spain, for case submission and permission for this study; Blanca Pérez and Aida Neira (Departament de Sanitat i Anatomia Animal, Facultat de Veterinària, Barcelona, Spain) for excellent technical assistance with immunohistochemistry; Dr. Myriam Tomás (Centro Veterinario La Marina, La Marina, Elche, Spain) for medical assistance with the lemurs of this report; and Dr. Pilar Galipienso and lemur keepers at Mundomar, Alicante, Spain.
a.
Dako Denmark A/S, Glostrup, Denmark.
b.
From Dr. Bjerkås, Norwegian School of Veterinary Science, Oslo, Norway.
c.
Sigma Chemical Co., St. Louis, MO.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.